
Abstract
Background:
Persons with disabilities who reside in rural areas experience challenges accessing and utilising health services and rehabilitation. Due to the high prevalence of diabetes mellitus in rural regions, the risk of having a lower-limb amputation is increasing. Comprehensive rehabilitation is vital to mitigate the negative impact that a lower-limb amputation has on a person.
Objective:
To explore the barriers and facilitators to accessing rehabilitation experienced by persons with lower-limb amputations in a rural setting.
Study Design:
A qualitative descriptive approach was used to collect and analyse data.
Methods:
Data were collected from 11 conveniently sampled participants from three sub-district hospitals in the rural iLembe district, Kwa-Zulu Natal, South Africa. Data were collected using semi-structured interviews to explore the barriers and facilitators perceived by persons with lower-limb amputations in a rural region.
Results:
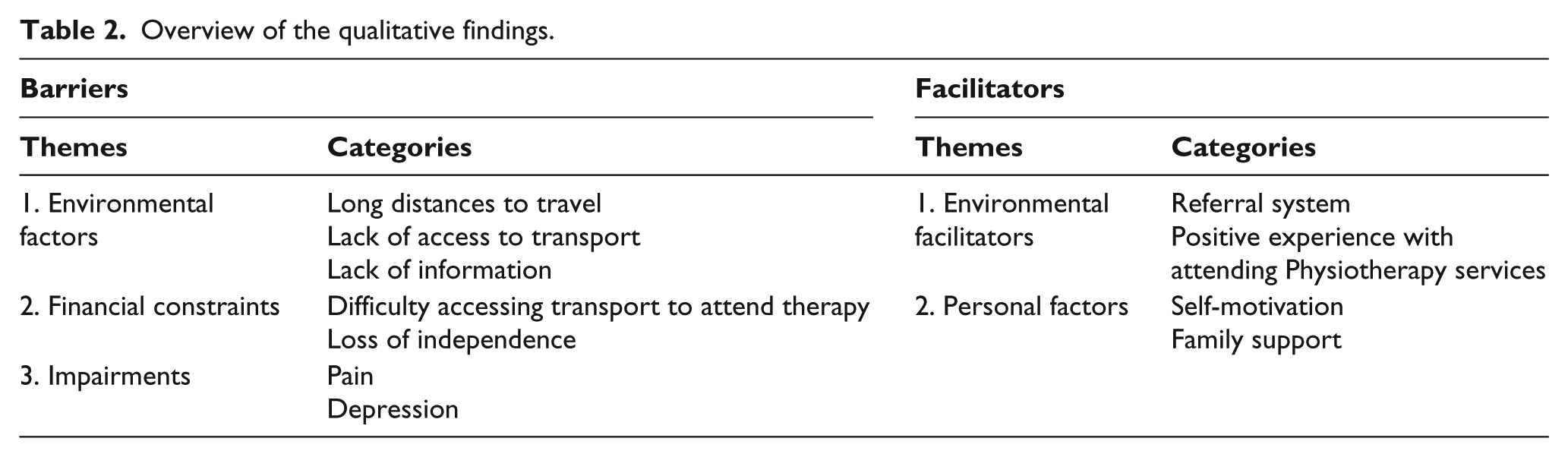
The three main barriers identified in this study were environmental factors, financial constraints and impairments. These barriers negatively impacted the participant’s utilisation of rehabilitation. The two main facilitators identified were environmental facilitators and personal factors which aided participant’s utilisation of rehabilitation.
Conclusion:
Access to rehabilitation was mainly hindered by the challenges utilising transport to the hospital, while self-motivation to improve was the strongest facilitator to utilising rehabilitation.
Clinical relevance
Rehabilitation is essential in preparation for prosthetic fitting. If a person cannot access rehabilitation services, they will remain dependent on caregivers. Highlighting the challenges to utilisation of rehabilitation in rural areas can assist to reduce these barriers and improve the functional status of persons with lower-limb amputations.
Background
The KwaZulu-Natal (KZN) province in South Africa has an estimated population of 10.5 million people, with 53% residing in rural areas and 8.4% of the population living with at least one disability. 1 There is a marked increase in the incidence of diabetes mellitus in rural areas in South Africa, 2 which is a known predisposing risk factor for lower-limb amputations. There are approximately 1.4 million diabetics in state healthcare in KZN alone, and approximately 2400 amputations are performed annually in the province. 3
Rehabilitation can assist to mitigate the negative impact of a lower-limb amputation by retraining physical and functional abilities, as well as facilitating social and community integration. 4 The ultimate aim of rehabilitation of a person with a lower-limb amputation is to mobilise independently with a prosthesis. However, in rural KZN, many patients wait more than 5 years for a prosthetic limb due to long waiting lists.
The right to access healthcare services in South Africa is guaranteed by Section 27 of the constitution. 5 However, in order to be fitted with a prosthetic limb, a person with a lower-limb amputation requires pre-prosthetic rehabilitation. Rehabilitation services for persons with an amputation are poorly managed and often not provided in Africa 6 and South Africa. 7 Several studies have shown that a multi-disciplinary approach to the diabetic foot can reduce amputations by up to 85%.8,9
People with disabilities in South Africa have difficulty accessing rehabilitation services. 10 In a recent study, the challenges experienced from the healthcare providers’ perspective in providing pre-prosthetic rehabilitation in a rural setting were highlighted. 11 However, in South Africa, little information exists from the perspective of people with disabilities about the healthcare barriers they face, while even less is known about what barriers people with specific impairments encounter.11,12
Barriers to the utilisation of healthcare services documented in the literature include inadequate policies and standards, negative attitudes, lack of provision of services, inadequate funding, lack of accessibility, lack of consultation and patient involvement and lack of data. 13 Even though challenges with accessing healthcare in a rural setting, such as transport, travel distances, high travel costs, out-of-pocket expenditure and disempowered patients, are well-documented,14–16 it is often not voicing the personal experiences of the people involved.
The objective of this study was therefore to explore the barriers and facilitators perceived by persons with lower-limb amputations to utilisation of rehabilitation services in a rural setting in KZN, South Africa.
Methods
A descriptive qualitative study design was utilised to collect data using a self-developed semi-structured interview guide with 11 participants. The interview guide consisted of open-ended questions that were developed based on the possible known barriers and facilitators to rehabilitation derived from the literature. The interview guide was piloted on two persons with lower-limb amputations. The guide was also sent to an expert to review for clarity. The semi-structured interview involved a set of predetermined, open-ended questions which initiated the discussion, followed by further prompting questions. Open-ended questions were asked to allow the participants to freely explore different avenues regarding the topic. This allowed the researcher an in-depth understanding into the participants’ experiences from their point of view. Five of the interviews were conducted at hospital-based therapy departments and six of the interviews were conducted at participants’ homes. A translator was present for those interviews where the participant’s first language was isiZulu. Each participant was given an explanation of the study prior to obtaining written informed consent and consented to be audio-recorded. Once consent was obtained, participants completed a demographic survey and the interview commenced. Semi-structured interviews aimed to explore the participants’ perceived barriers and facilitators in accessing rehabilitation services.
Non-probability convenient population sampling was adopted at three rural sub-district hospitals in the iLembe district in the KZN province in South Africa. Participants were identified by physiotherapists at each of the three sub-district hospitals and contacted telephonically to participate in the study. Participants were included if they had undergone a lower-limb amputation, if they were within the ages of 18–80 years and if they were able to understand the study and provide written consent. Those participants with co-morbidities that interfered with their function beyond that of the lower-limb amputation were excluded.
A general inductive approach to content analysis was followed to analyse the qualitative data, even though the open-ended questions in the interview were deduced from barriers and facilitators in the literature.17,18 Themes that arose were then organised into either barriers or facilitators. These themes emerged from a process of inductive analysis of the raw data, and the researcher used the international language of the ICF (International Classification of Functioning, Disability and Health) to describe the themes. Themes were not specifically deduced from the ICF categories. The analysis was performed by following Creswell’s steps for thematic analysis of qualitative data. 17 First, the researchers familiarised themselves with the verbatim transcripts of the raw data, and then similar words or phrases were classified into codes. These codes were then grouped together to form individual categories. Categories that overlapped were finally collapsed into the themes. Any differences that arose during the analysis were discussed until consensus could be reached.
Ethical clearance to conduct the research study was obtained from the University of the Western Cape’s Research Ethics Committee (Nr. 14/7/14) and permission was obtained from the relevant authorities to conduct the study.
Results
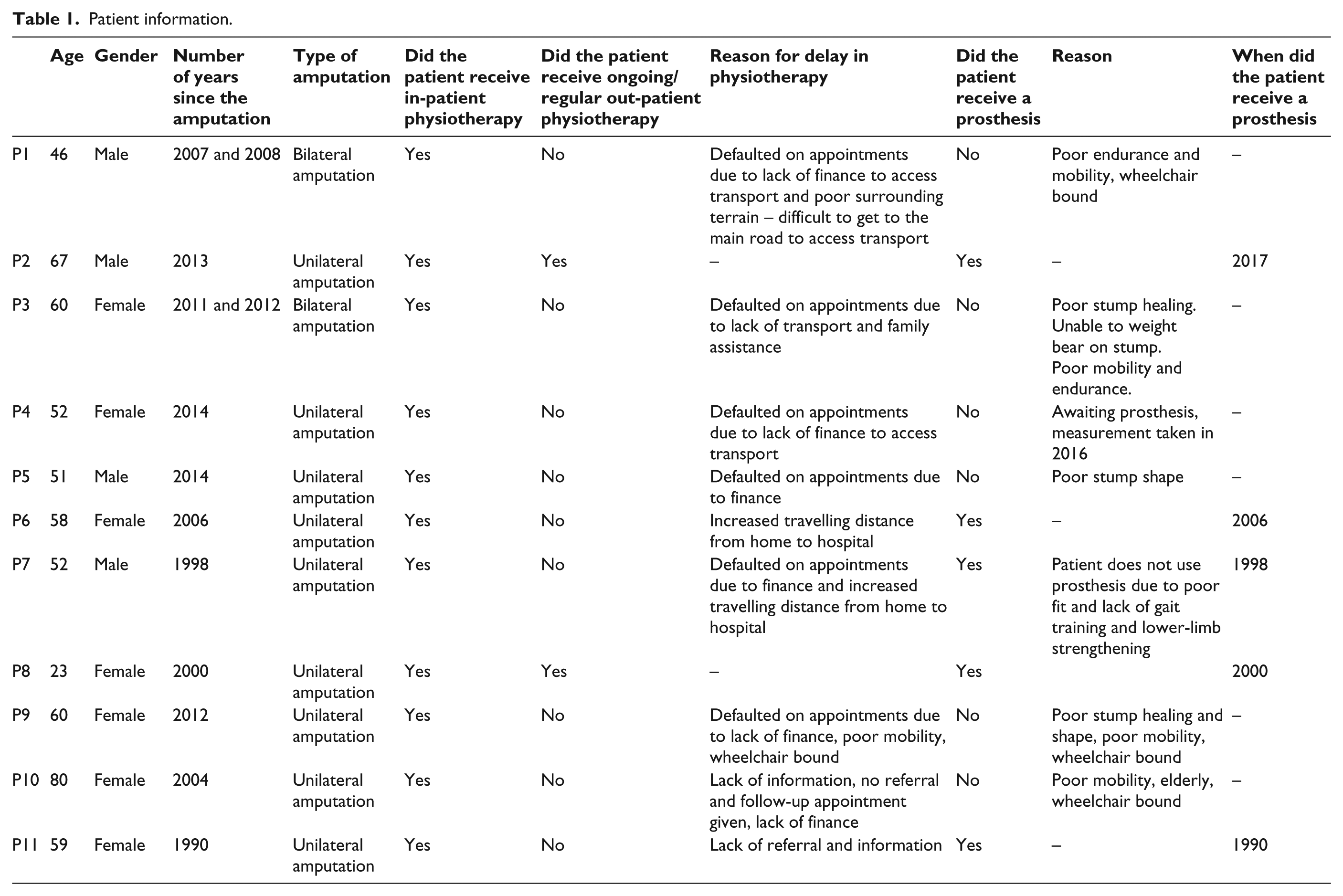
The average age of participants in this study was 55 years and ranged from 23 to 80 years of age, and the majority (64%; 7/11) were female and had unilateral limb (73%; 8/11) amputations (Table 1). Themes were classified as either a barrier or facilitator to accessing rehabilitation services. Three main themes emerged under ‘barriers’, namely, (1) environmental factors, (2) financial constraints and (3) impairments, while two themes, namely, (1) environmental facilitators and (2) personal factors emerged as ‘facilitators’. These themes and their related categories are listed in Table 2.
Patient information.
Overview of the qualitative findings.
Barriers
Environmental factors
Long distances to travel, a lack of access to transport, and a lack of information were frequently reported as barriers to accessing rehabilitation services.
Long distances to travel
Due to the nature of the surroundings, most participants reported that long distances challenged their access to rehabilitation. Some participants had to plan ahead and wake up early in order to reach the main road in time to seek transportation to the nearest rehabilitation facility: … I woke up at 4(am) trying to find transport because there are no cars in our area. We come from all the way down there by foot … There are no cars here; you only get cars when you get up there to the main road … it’s far indeed. (P7) It’s a 20-minute drive … I use public transport … I have to walk from home … it’s a 10-minute walk (to the main road to get the taxi). (P8)
Lack of access to transport
Others expressed their need for transportation to and from rehabilitation facilities, as there was no public transport available close to their home and private transportation was expensive. Participants further expressed their need to use more than one mode of transportation in order to access rehabilitation services. It was also noted that participants experienced difficulty when accessing transportation such as taxi services as they could only use the front seat: I went there (to physio) often then it became a problem when the car broke down. (P3) Exercising is hard because there is nothing (transport) to pick me up and take me there … it is too far there. It’s difficult. (P7)
Lack of information
Participants highlighted that they did not attend physiotherapy due to lack of information, no referral or no knowledge of physiotherapy services at the nearest hospital. Due to the lack of information, patients were left despondent and reluctant to attend physiotherapy: … they’re the ones who were supposed to explain to me that ‘come to the physio, continue with the physio … (P7) – referring to the doctors … they did not tell me to see the physiotherapist … No one has told me about what the physiotherapist does … I have not been told to go to see the physiotherapist … since I was discharged from the hospital, nobody told me anything. (P11)
Financial constraints
Financial constraints limited participants’ ability to attend rehabilitation at hospitals and also reinforced the loss of independence that participants experienced following a lower-limb amputation.
Difficulty accessing transport to attend therapy
Participants expressed their difficulty accessing rehabilitation services due to financial constraints. Participants relied solely on their monthly disability grant (US$93) as a source of income which, in some instances, was the only source of income for the household. The disability grant was used not only to support the family but also to attend rehabilitation services: … it is expensive to go there. There isn’t money … (P5) – referring to the physiotherapy gym. They said I must come back in September so they can check it (the stump) … I didn’t go because I didn’t have money … (P5) There are three of us. There isn’t anyone [working]. I get a pension. It is difficult because there are a lot of things that need money but at least it is something because I can’t make money myself. (P7)
Participants expressed difficulties affording transportation to the hospital to access rehabilitation. Those participants who mobilised with wheelchairs needed to use private transport which was more costly than public transport: The transport is a problem. The transport is R300 [20 USD] from here [home] … I use private cars … I use a wheelchair. If there is no private transport to take me, I do not go to the hospital. (P9) I take whatever transport here at Mthombeni using the wheelchair … I would say it is R400 [27 USD]. (P10)
Loss of independence
Participants were dependent on family or paid caregivers to assist them in activities of daily living and participating in their communities. Due to poverty and high rates of unemployment, caregivers considered assisting a person with a disability as an opportunity to earn money and would not assist unless the patient could pay for their services. Participants required someone to push them in their wheelchair on uneven or rough terrain but could not afford to pay them which further hindered their utilisation of rehabilitation services. Financial constraints thus also reinforced the loss of independence that participants experienced following a lower-limb amputation: I can’t go alone … I need someone to push me … I pay for my brother … He push me in the wheelchair. (P2) I don’t have money. The pension money I get is the money I use to feed myself … I can’t find someone to help me. At times when I have found someone you find that it hurts me financially when the person wants their money. (P6)
Impairments
Under the theme of impairments, the two most commonly reported impairments were pain and depression.
For some participants, rehabilitation was painful. Some participants experienced stump pain as well as lower-limb pain during rehabilitation due to fatigue and decreased muscle strength. Although the participants had tried to exercise and attend rehabilitation, experiencing pain during the rehabilitation session made them unwilling to attend rehabilitation: It was still painful, I was still injured … They made me exercise inside (in the ward), I still had stitches, it was still very painful … that was the last time I exercised … (P4) I’d be trying to exercise and feel pain and sit down … (P9)
Some participants expressed their discouragement to attend rehabilitation due to being ridiculed and excluded in society and by hospital staff. Some participants were excluded and asked not to join certain groups of friends due to having a ‘disability’ or rather an ‘artificial leg’. Another patient was ridiculed by hospital staff for placing traditional strings (bands) around his amputated limb.
These stigmatisations lead to feelings of depression and being excluded resulting in a lack of motivation to attend rehabilitation or participate in society as they felt they did not belong: Even at the hospital they used to make fun of me when I’d take off my clothes and they’d see the strings that the healer put on me. They’d laugh at me … (P1) … in the community, some friends, you’ll meet some people who are saying ‘ah that girl has an artificial leg’ so I can’t roll with them. (P8)
Facilitators
The two themes that emerged from the interviews that facilitated utilisation of rehabilitation services were environmental facilitators and personal factors.
Environmental facilitators
Even though the environment posed many challenges to accessing services, in some instances, participants reported environmental facilitators such as a good referral system and positive experiences with attending physiotherapy services.
Referral system
Many participants were unaware of the services provided at the hospitals. Those who were aware of the services were more likely to attend and receive further rehabilitation: They cut the leg at Stanger and then said I should get further treatment at my local hospital. (P3) … they put me in touch with a physio so that I could get a new leg after they had cut my leg. (P6)
Positive experiences with attending physiotherapy services
Participants were more likely to attend rehabilitation if there was a shorter waiting period to access a physiotherapist: No, not wait long. (P2) If there other wheelchairs in front of me, I join the queue, if not, they escort me in. (P3)
Some participants perceived the physiotherapist as someone who was helping them and became motivated to attend rehabilitation due to the good relationship between the therapist and the participants: I saw the physio as someone who was going to help me. (P4) … it was very good because we understood each other and I was able to listen to her (the therapist) although sometimes it got very hard … we had a good relationship. (P8) It was the best thing for me (attending physio) ‘cause that lady, who I was talking with, told me that in life I’ll have to meet different people. Some will understand me, some won’t understand me. So as I grew up, there were those people in which made me feel bad about myself – lose confidence, ya. But then whenever it happened I just remembered that oh, that lady told me that I will meet such people so … (P8)
Personal factors
Personal factors that were reported as facilitators to utilising rehabilitation services included self-motivation and family support.
Self-motivation
Self-motivation and motivation given by the physiotherapist encouraged participants to continue with rehabilitation. Participants had different insights to what motivated them to attend rehabilitation. Some believed exercising in order to get a prosthesis would allow them to walk independently again. Others were motivated by the attitude of the physiotherapist and some wanted to regain independence by working again. One participant was encouraged by the counselling and information given by the physiotherapist who motivated her to attend rehabilitation: I could see that I was getting help because I could see that I was flexible. I was comfortable walking in crutches even when I hadn’t put in the prosthesis. (P6) I think because I went for counselling that really changed me like it made me realise that even though I have to like wear an artificial, it doesn’t mean that my life was like changing completely. It made me realise that ya I can still live my life fully even though I have an artificial leg. (P8)
Some participants were motivated by the hope to receive a prosthesis: … to stand up and walk is difficult. But I am able to get up into the wheelchair but the walking is hard … If I can just get the leg I know that I’ll be able to stand and maybe be able to walk. I need to get the leg. (P3) … I am looking forward to the shoe … (P9)
Family support
All participants expressed their need for help and assistance in their daily lives. Most participants, who had family members present, explained how their families assist them in attending rehabilitation and also help them at home: … it’s good because I have my family to help me. (P2) She (wife) is a great help to me. I wouldn’t be able to do it myself if she wasn’t there. She’s a great help … (P7)
Discussion
The ICF is the universal language for describing and contextualising disability and function. 19 It has also been established as appropriate for the description of function in persons with lower-limb amputation.20,21 In line with the World Health Organization (WHO) definition, environmental factors were identified as both barriers and facilitators to accessing rehabilitation services. Impairments in bodily function were identified as an additional barrier, while personal factors facilitated access to rehabilitation.
Impairments in bodily function
Due to the lack of accessibility to rehabilitation and the multi-disciplinary team, many participants were not appropriately re-integrated into society. Early intervention and continuous rehabilitation can improve functionality, mobility and adaptability for persons with lower-limb amputations, thereby decreasing the challenges faced with accessibility. In addition, rehabilitation also assists to manage and alleviate pain. 22 However, due to the lack of knowledge regarding the role of physiotherapy, pain during exercise and phantom pain was perceived as a barrier to the continuation of rehabilitation in this study. Participants were not aware that therapy could actually assist to decrease their phantom limb pain, and that the acute pain in the stump could be treated by therapy as well, which limited their utilisation of therapy services.
Due to healthcare professional staff shortages in rural settings, all the members of the multi-disciplinary team are often not available to be involved in the rehabilitation of a person with an amputation. Professional prosthetists, for example, are not employed by all hospitals, and prosthetists from the main tertiary hospital generally run monthly clinics at the rural district hospitals with enormous patient loads, limiting their availability to be part of the team. Staff shortages in rural settings are well-documented in the literature, but the problem seems to persist. 8 The National Department of Health has created an initiative to try and address the staff shortages specifically in rural areas by creating a compulsory ‘community service year’ for all graduating health professionals. During this year, young health professionals are employed in the public health system (as opposed to the private sector) in often rural and remote settings in order to service the community. Unfortunately, the Provincial Department of Health in this province is not creating enough posts for these professionals to continue working in these settings once their year is completed.
In this study, stigmatisation, mockery and discrimination by the community lead to participants being excluded and home-bound. Participants in some cases felt that they were not accepted by their friends anymore. These findings are resonated by a study exploring therapists’ perspectives on challenges to accessing rehabilitation services conducted in a different rural community in the same province. 23 In this earlier study, therapists reported that strong traditional and cultural beliefs regarding the cause of disability resulted in stigmatisation. In some rural communities in South Africa, disabilities are still attributed to punishment from the ‘ancestors’ or someone being ‘bewitched’.23,24 Some taxi drivers believe that they will also be ‘cursed’ if they pick up and transport persons with disabilities, which limits the available transport opportunities, and access to rehabilitation.
Some participants also reported experiencing negative attitudes and stigmatisation by hospital and rehabilitation staff, which contributed to feelings of depression. Even though depression is commonly associated with limb loss, the underlying reason given for depression in this study was more related to stigmatisation as opposed to the frequently reported sense of depression due to the loss of function and changes in body image. 25 These physical and psychological impairments were both expressed as barriers to accessing rehabilitation in this setting.
Environmental factors
The non-utilisation and inaccessibility to healthcare services and particularly rehabilitation services by persons living with disabilities in South Africa is well-documented.10,26 In this study, persons with lower-limb amputations were deterred from utilising rehabilitation services mainly due to the burden of environmental barriers and financial constraints.
Financial challenges added to the burden posed to participants’ mobility by the physical environment. In this study, all participants were unemployed and relied on a government social support grant. Participants in this study who had a prosthesis paid for it with their disability grant. However, since 2017, all prostheses are now free of charge. For some participants, prosthetic fitting was a part of early rehabilitation which yielded a better outcome as well as early independent ambulation. However, for most participants, prosthetic fitting was not an option (Table 1).
The lack of early rehabilitation and prosthetic fitting in turn limited participants’ mobility and increased their expenditure on healthcare and services. Due to the uneven terrain, and gravel roads, participants were required to pay a person to assist them if they wanted to leave their homes. In order to go to the hospital, participants often had to cover long distances just to get to the road where they could access public transport. Wheelchair users then had to hire a private car to transport them as they cannot use the local taxis due to space limitations, mobilising in and out the taxi (accessibility) or cultural beliefs regarding their disability.4,27,28 One round trip to the hospital for one rehabilitation session could easily cost a person with an amputation half of their monthly income. Social grants were found to be inadequate to sustain their daily living expenses for a household as well as to provide regular rehabilitation visits. These findings were supported by several studies in the literature.29–31
Environmental factors were in some instances also considered as facilitators in accessing rehabilitation services. Satisfaction with physiotherapy services, motivation and good relationships with healthcare providers plays a huge role in the adherence of patients with amputations to attending rehabilitation. 32 Participants, in this study, were more likely to attend rehabilitation when provided with information, motivation, involvement in decision-making, progression of functionality and easy accessibility. Congruently, the literature emphasises patients’ distaste for technical language, poor feedback and depersonalized care when communicating with their practitioner. 33
Knowledge of the environmental barriers and facilitators to accessing rehabilitation should be used to advocate for a community-based approach to rehabilitation services for persons with mobility impairments. Rehabilitation staff working in rural settings should also incorporate interventions aimed at raising awareness of the benefits and availability of rehabilitation services as part of their work.
Personal factors
Personal factors reflect on the individual’s experience of their disability. 21 In this study, two personal factors were identified as facilitators to accessing and utilising rehabilitation services. These were self-motivation and family support. Participants who were not depressed, and reported being intrinsically driven to be more functional, were more likely to attend therapy services. Some participants also reported that they attend therapy as they hoped that it would assist them to receive a prosthetic limb.
Family support was frequently reported as a facilitator because it reduced participants’ travel costs to access therapy. Participants preferred having a family member taking care of them as they would not have to pay extra for hiring a caregiver. Participants not only relied on family and friends for their day-to-day activities but also to assist with mobilization and transportation to and from the hospital where they would receive rehabilitation.
Active problem-solving influences psychological adaptation with the same reports of higher levels of adjustment and acceptance of disability and acknowledgment, with lower levels of depression and internalized anger. 34
In this study, some participants showed a positive mentality and positive attitude towards recovery and it may therefore be anticipated that some had employed a positive approach to problem-solving. Generally, participants in this study were looking forward to facing their challenges although at times they expressed concern or inhibitions that were not related to acceptance, for example, financial limitation.
Even though facilitators identified in this study were limited, the rehabilitation community should incorporate these facilitators into their rehabilitation to facilitate improved adherence to rehabilitation. Therapists should foster good relationships with their patients, educate them on the rehabilitation and prosthetic options available and motivate and encourage them. Early involvement and education of caregivers could also potentially assist to foster a more supportive environment for the person with an amputation. If these facilitators can be utilised to improve access to rehabilitation services in the absence of a community-based approach to rehabilitation, it might enable more persons with an amputation to qualify for prosthetic fitting.
Limitations
The available sample size for this study was reduced by a number of potential participants not consenting to participate in this study. Convenient sampling might have biased the study findings but due to the available sample size, random sampling was not feasible. The study findings are not generalisable to all rural settings in South Africa, as data were only collected in one rural district in South Africa.
Conclusion
The numbers of persons with lower-limb amputations are constantly increasing in rural areas, and people are not qualifying for prosthetic fittings mainly due to the lack of rehabilitation. This study provides preliminary evidence on rehabilitation accessibility and utilisation by people with lower-limb amputations in the rural iLembe district of KZN.
In this study, environmental factors such as the physical environment, challenges accessing transport, lack of information or referral and financial constraints continue to limit people with lower-limb amputations’ mobility and access to rehabilitation. These factors ensnare people in this rural community into a vicious cycle of immobility, disability and poverty. There are, however, some facilitators to accessing rehabilitation that were identified in this study. The main facilitators were environmental factors, such as positive experiences with therapy, and family support.
It was found that people with lower-limb amputations viewed rehabilitation and the physiotherapist as someone who would assist them in receiving a prosthetic limb and regain function. However, numerous barriers limited their access to these services. This led to a decrease in function, poor mobility and overall a poor quality of life for some participants.
Rehabilitation personnel working in these rural settings should be more aware of the possible facilitators, and it is vital that the barriers identified in this study are reduced in order to increase accessibility to rehabilitation and improve quality of life for persons with amputations.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical statement
Special ethical clearance obtained from the University of the Western Cape’s Research Ethics Committee (Nr. 14/7/14).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received financial support from the National Research Foundation of South Africa for this research.