
Abstract
Background:
A transfemoral amputee’s functional level can be classified from K-level 0 (lowest) to K-level 4 (highest). Knowledge of the biomechanical differences between K3 and K4 transfemoral amputation could help inform clinical professionals and researchers in amputee care and gait assessment.
Objectives:
Explore gait differences between K3- and K4-level transfemoral amputation across different surface conditions.
Study design:
Cross-sectional study.
Methods:
Four K3 and six K4 transfemoral amputation and 10 matched able-bodied individuals walked in a virtual environment with simulated level and non-level surfaces on a self-paced treadmill. Stability measures included medial-lateral margin of stability, step parameters, and gait variability (standard deviations for speed, temporal-spatial parameters, root-mean-square of medial-lateral trunk acceleration).
Results:
K3 walked slower than K4 with wider steps, greater root-mean-square of medial-lateral trunk acceleration, and greater medial-lateral margin of stability standard deviations, indicating their stability was further challenged. K3 participants had greater asymmetry in double support time and trunk acceleration root-mean-square in the medial-lateral direction, but similar asymmetry overall. K3 participants had larger differences from AB and in more parameters than K4, although K4 differed from AB in trunk acceleration root-mean-square in the medial-lateral direction, walking speed, and double support time standard deviations.
Conclusion:
The findings improve our understanding of K3 and K4 transfemoral amputation gait on slopes and simulated uneven surfaces.
Clinical relevance
High performing and community ambulatory transfemoral amputees cannot match the ambulatory abilities of ablebodied individuals. Understanding gait differences between these groups under conditions that challenge balance is required to develop rehabilitation protocols and prosthetic componentry targeted at improving transfemoral amputee gait and overall mobility in their chosen environment.
Background
Forward ambulation challenges stability because the center of mass (CoM) is constantly moving. For people with transfemoral amputation (TFA), additional difficulties in maintaining dynamic stability are posed by the loss of sensory feedback mechanisms and force generation in their prosthetic knee and ankle. In comparison with able-bodied (AB) populations, TFA walk slower,1–6 with shorter, wider, and longer duration steps, 1 and more pelvic and trunk motion.2–4 A primary goal of rehabilitation following a lower limb amputation is restoring normal gait, achieved through a combination of prosthetic technology and specific gait training. While advances in both areas greatly improve the potential for “normal” gait, even individuals who are capable of advanced levels of prosthetic mobility still do not perform as well as their AB peers.
TFA limb asymmetries include smaller ankle and knee motion and pelvic drop on the prosthetic side compared to the intact side7–10 and increased lateral trunk bending over the prosthetic limb that can have multiple causes, such as weak hip abductor stabilizing muscles. 11 Double support time (DST) is also longer for the intact limb than the prosthetic limb. 11 Limb asymmetry evaluation is particularly important because greater joint moments and forces on the intact limb, compensating for prosthetic limb deficiencies, could lead to intact limb osteoarthritis.12–14
TFA also have greater medial-lateral margins of stability (ML-MoS) on their prosthetic side than both their intact side and AB participants, 5 which is considered a stability-enhancing strategy. 6 Increased gait variability has also been associated with greater instability,15–19 which could relate to risk of falls. In our previous study, 20 TFA differed from AB for root-mean-square of trunk acceleration in the medial-lateral direction (RMSML), walking speed, step width, ML-MoS, and gait variability.
Non-level conditions likely further exacerbate these differences in transfemoral prosthetic gait. TFA who have the ability to walk in the community are challenged on a daily basis to adapt to different walking terrains. Using K-level functional classification, 21 individuals at K3 are community ambulators with the ability to transverse most environmental barriers and may have vocational, therapeutic, or exercise activity that demands prosthetic use beyond simple locomotion. K4 level exceeds basic ambulation skills, exhibiting high impact, stress, or energy levels. Given the higher locomotion demands faced by these individuals, it is important to understand how gait mechanics differ from AB individuals. This information could help improve clinical treatment programs and further optimize prosthetic technologies to prevent long-term complications.
The purpose of this study was to determine differences in TFA (K3 or K4 level), and AB gait over level and non-level conditions. Given the greater physical demands on K3 and K4 TFA, more biomechanical research is needed on non-level, realistic walking conditions rather than only level walking. Based on previous TFA gait research between TFA and AB, the lower functional level K3 participants should walk slower than K4, with wider steps, greater ML-MoS, greater trunk acceleration RMSML, and more variable and asymmetric gait patterns. We also hypothesized that K3 differs from AB for more outcome measures and more walking conditions than K4. Normalizing gait is important to prevent future complications such as osteoarthritis, 22 and studying gait mechanics is an essential component. Since the literature comparing K3 and K4 populations is limited, walking biomechanical knowledge across surfaces other than level, such as up and down slopes, cross slopes, rocky, will inform practice for researchers, prosthetists, therapists, and physicians.
Methods
Participants
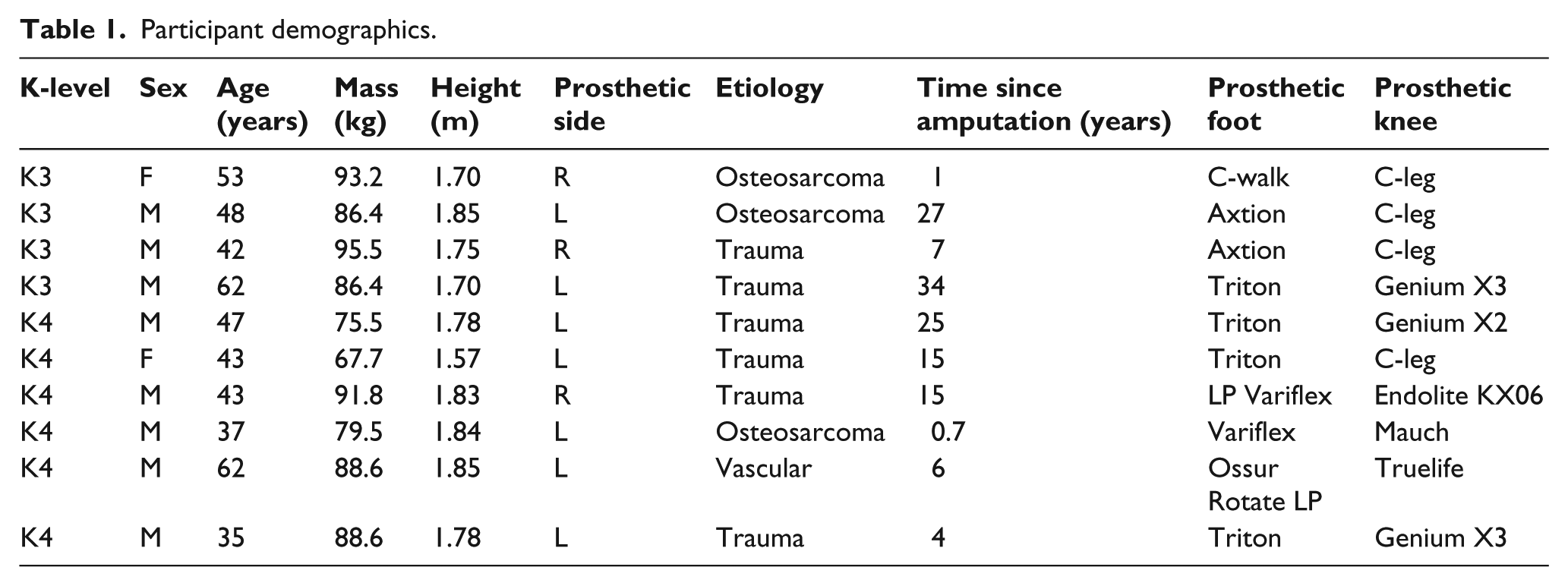
A convenience sample of 10 individuals with unilateral TFA (Table 1) and 10 age, sex, height, and mass-matched AB volunteers (8 males, 2 females; age = 43 ± 8.6 years; mass = 83.2 ± 10.1 kg; height = 1.78 ± 0.07 m) were recruited from The Ottawa Hospital Rehabilitation Centre, Canadian Forces Health Services, Glenrose Rehabilitation Hospital, or the community. Participant K-level was determined by clinical assessment prior to the study. All AB participants had a dominant right leg (preferred limb to kick a ball). The Ottawa Health Science Network Research Ethics Board and University of Alberta Research Ethics Board approved this study and written informed consent was obtained.
Participant demographics.
Data collection
The CAREN–Extended virtual reality system (Motekforce Link, Amsterdam, NL), which includes a 12-camera motion capture system (Vicon Inc., Oxford, UK), 180° projection screen, and 6 degree-of-freedom motion platform embedded with a dual belt instrumented treadmill (Bertec Corp., Columbus, OH, USA) was used for all trials (Figure 1). The system is capable of simulating real-world environments by matching platform motion to the programmed visual surround. Participants wore a safety harness that prevented ground contact in a fall, yet permitted movement along treadmill dimensions. Three markers tracked platform motion. A 57 marker set tracked full body kinematics 23 (Figure 2), and a digitizing pointer defined 20 additional anatomical landmarks (C-Motion Inc., Germantown, MD, USA). Marker data were sampled at 100 Hz.
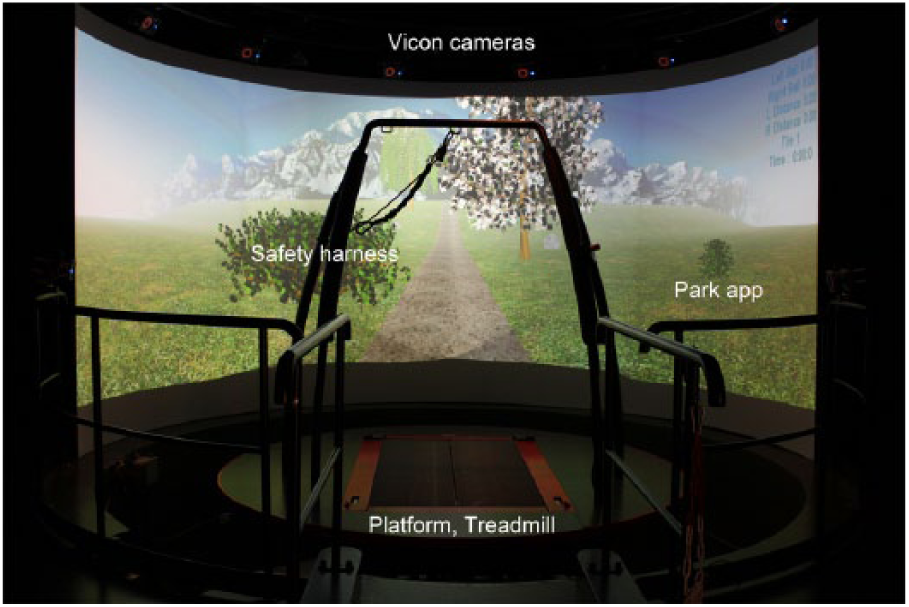
CAREN–Extended system with Park application.
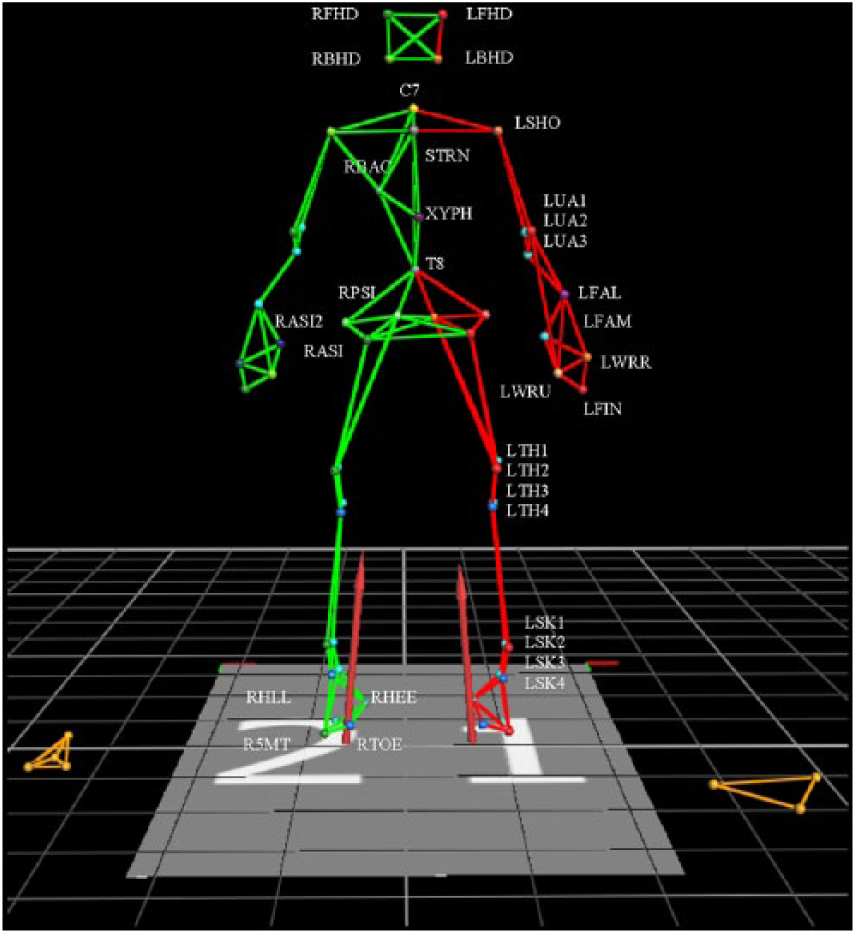
Full body marker set.
Participants completed a 10 to 15-min virtual environment acclimation period that included self-paced treadmill training and a warm-up trial. Self-paced control 24 automatically adjusted treadmill speed to match participant walking speed, with 0.7 sensitivity scaling, 1 m/s2 maximum treadmill acceleration, and equal visual scene speed (optic flow) and treadmill speed.
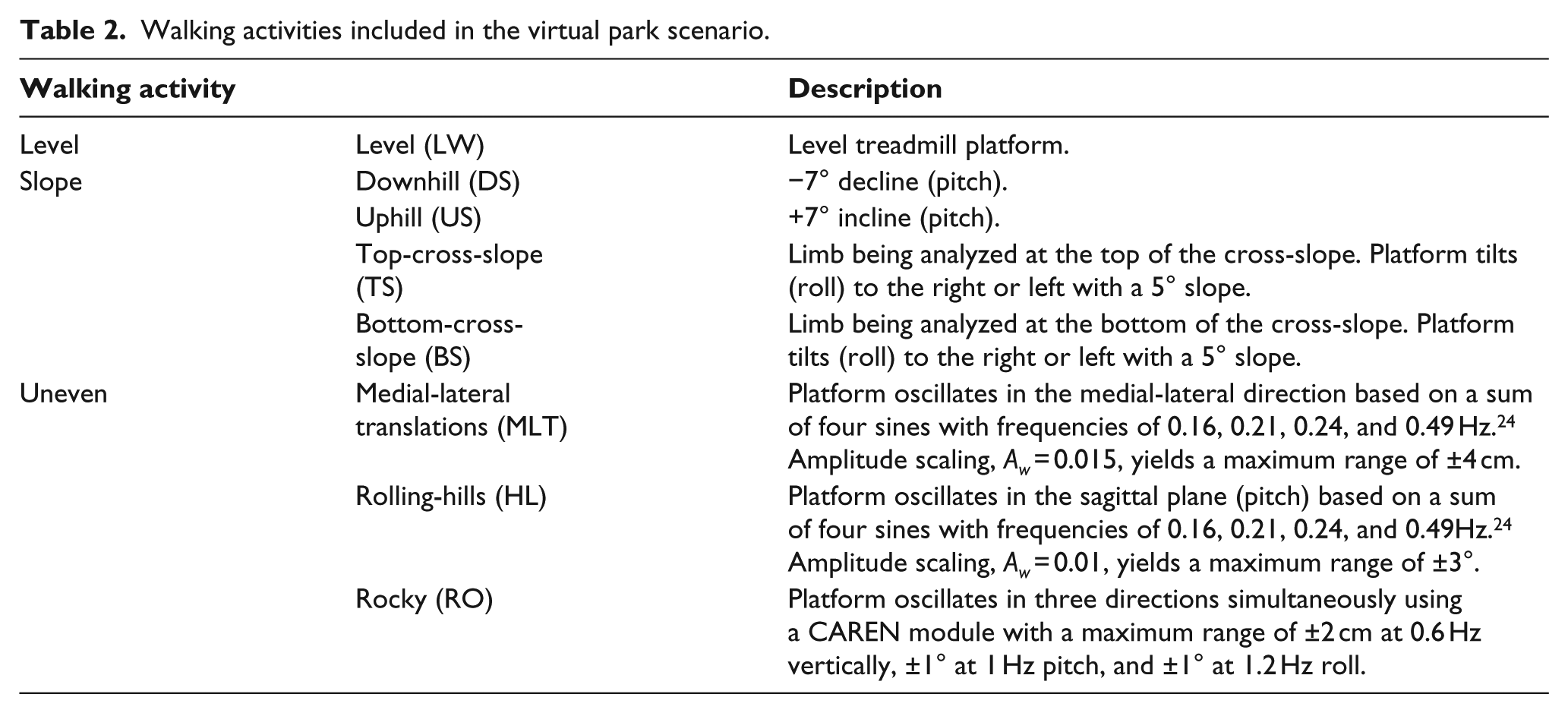
Using self-paced mode, participants completed two to three walking trials through a virtual park scene. Each walking condition was a 20-m section (LW: level walking, DS: downhill slope, US: uphill slope, TS: top-cross-slope, BS: bottom-cross-slope, HL: rolling-hills, MLT: medial-lateral translations, RO: simulated rocky; Table 2). These conditions represented real-world surfaces or continuous surface perturbations in different axes. Each trial started from standing, an initial level walking period, and ended with a level walking section. Intermediate sections were randomized and separated by level sections (340 m total per trial). Level walking at the beginning of the trial, after reaching steady state, was used for the level condition. Participants could take breaks between trials. Four TFA intermittently grasped one treadmill handrail; however, analyzed gait cycles were without handrail use.
Walking activities included in the virtual park scenario.
Data Analysis
Marker data were filtered using a fourth-order low-pass Butterworth filter (10 Hz). A 13-segment body model25,26 was created in Visual 3D 4.96.4 (C-Motion, Inc.). Gait events were identified from foot velocity relative to the pelvis. 27 Thirty gait cycles were selected for each walking condition. Anterior–posterior foot marker velocity during mid-stance was used to calculate treadmill velocity for each stride.
Mean and within-subject variability (standard deviations (SD)) of walking speed, step width, DST, and ML-MoS were calculated (Table 3). RMSML measures acceleration and gait pattern smoothness, 28 stability, and variability.29,30 SD represents within-subject variability 31 and has identified level and non-level surface differences between AB and balance-impaired groups.32–35
Measures examined to quantify stability: medial-lateral margin of stability (ML-MoS), step parameters, and gait variability.
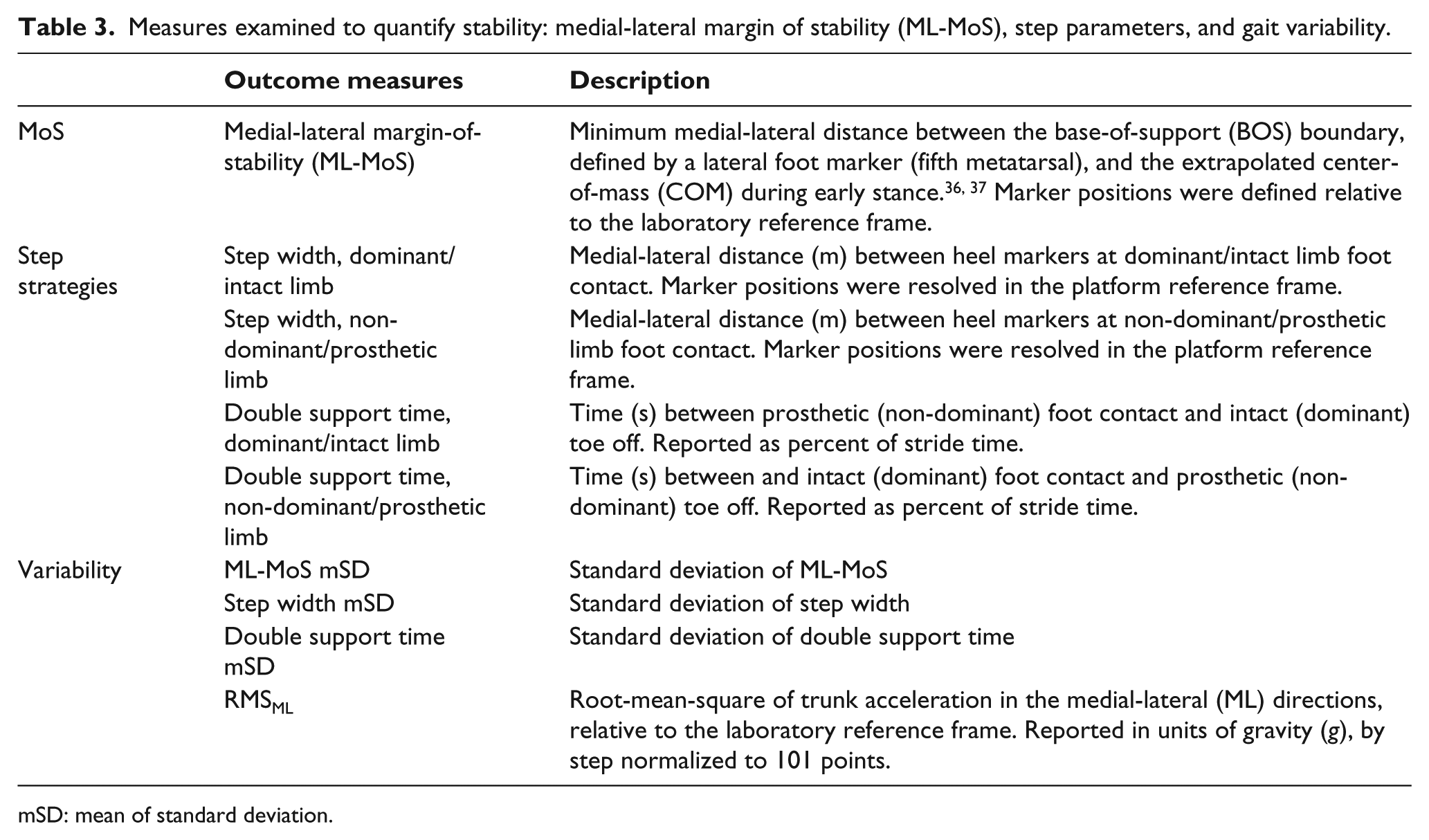
mSD: mean of standard deviation.
Outcome measures were calculated using custom MATLAB programs (2010a, Mathworks, Natick, MA, USA) and R v2.14 (R Foundation for Statistical Computing, Vienna, Austria) was used for all statistical analyses. Data were examined using separate linear mixed models (lmer4 package) to examine group and limb main effects and group × limb interactions, for each walking condition. Fixed factors were group (AB, K3, K4) and limb (dominant/intact and non-dominant/prosthetic), and participant was the random factor. Analyses were also performed with a treadmill speed covariate to understand how speed affected findings.
Significant main effects were examined using multcomp package post hoc tests (p < 0.05). To minimize between group comparisons, limb comparisons were intact versus dominant and prosthetic versus non-dominant. Step width effects on RMSML were examined since step width can influence trunk motion. 7 As an exploratory study with small sample size, results and discussion were reported without a statistical correction for multiple tests. All statistical results reported include speed as a covariate. The results report statistical comparisons after considering main effects and any interactions.
Results
K3 and K4 comparison
K3 participants walked slower than K4 for LW, TS, BS, and HL conditions (p < 0.031, Table 4). K3 walked with wider steps than K4 for BS and MLT (p < 0.046). K3 participants walked with wider steps than K4 when their prosthetic limb was on the TS (p < 0.003).
Mean of treadmill speed, temporal-spatial parameters, and margin-of-stability (ML-MoS).
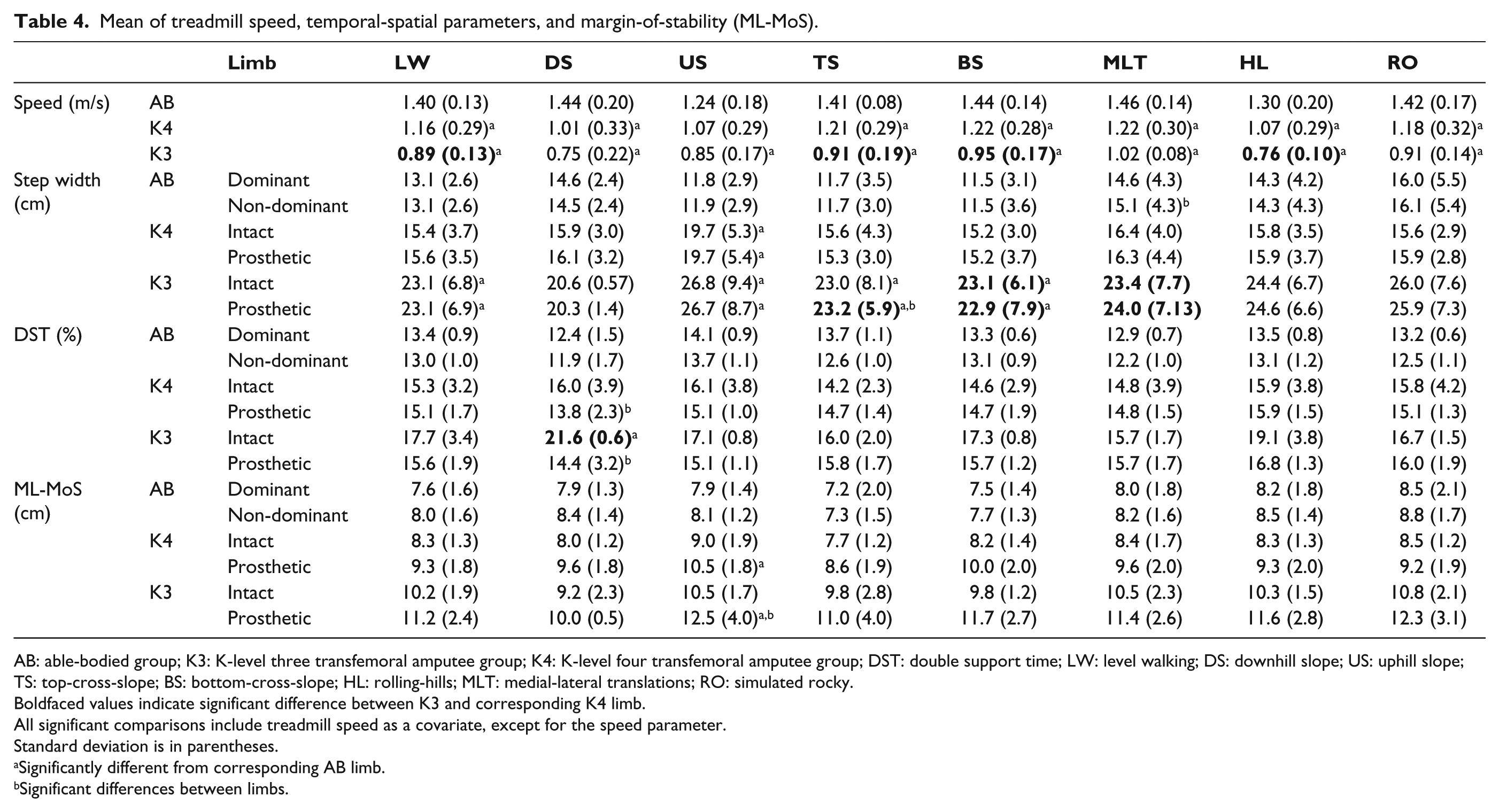
AB: able-bodied group; K3: K-level three transfemoral amputee group; K4: K-level four transfemoral amputee group; DST: double support time; LW: level walking; DS: downhill slope; US: uphill slope; TS: top-cross-slope; BS: bottom-cross-slope; HL: rolling-hills; MLT: medial-lateral translations; RO: simulated rocky.
Boldfaced values indicate significant difference between K3 and corresponding K4 limb.
All significant comparisons include treadmill speed as a covariate, except for the speed parameter.
Standard deviation is in parentheses.
Significantly different from corresponding AB limb.
Significant differences between limbs.
For downhill, K3 had significantly greater DST on the intact limb than the K4 intact limb (p < 0.010). However, DST SD was significantly smaller for K3 compared to K4 for US and MLT (p < 0.042; Table 5). DST SD was also smaller on the K3 prosthetic limb than on the K4 prosthetic limb for HL (p < 0.041), but was greater when walking downhill (p < 0.001).
Mean of the standard deviations (mSD) for treadmill speed, temporal-spatial parameters, margin-of-stability (ML-MoS), and root-mean-square for medial-lateral trunk acceleration (RMSML).
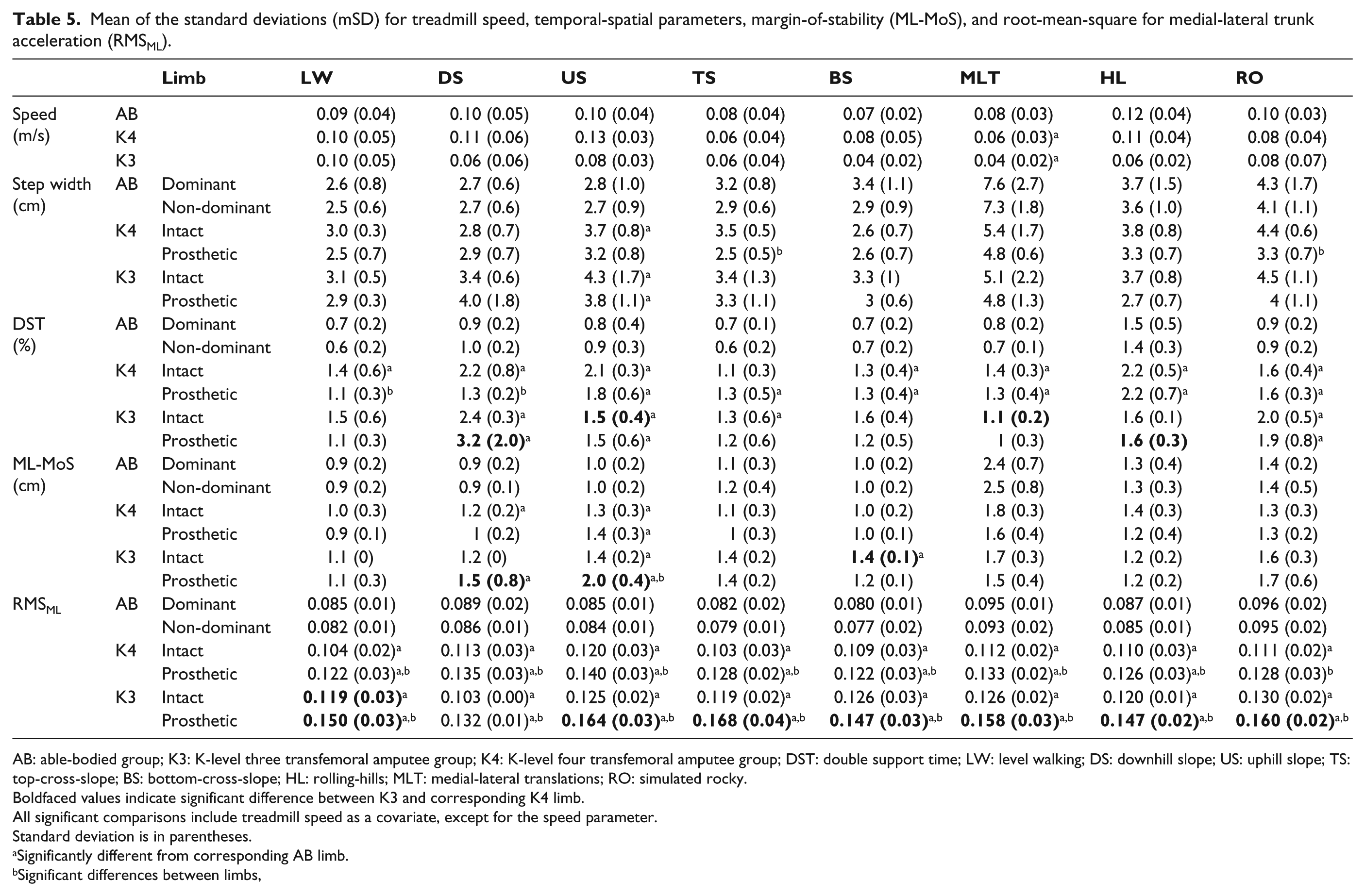
AB: able-bodied group; K3: K-level three transfemoral amputee group; K4: K-level four transfemoral amputee group; DST: double support time; LW: level walking; DS: downhill slope; US: uphill slope; TS: top-cross-slope; BS: bottom-cross-slope; HL: rolling-hills; MLT: medial-lateral translations; RO: simulated rocky.
Boldfaced values indicate significant difference between K3 and corresponding K4 limb.
All significant comparisons include treadmill speed as a covariate, except for the speed parameter.
Standard deviation is in parentheses.
Significantly different from corresponding AB limb.
Significant differences between limbs,
K3 prosthetic limb had a significantly greater ML-MoS SD than K4 prosthetic limb for DS and US (p < 0.008). K3 intact limb had significantly greater ML-MoS SD than K4 intact limb for BS (p < 0.002).
K3 had significantly greater trunk acceleration RMSML when stepping onto their prosthetic side than K4 for all conditions except DS (p < 0.021), where K4 had greater trunk acceleration RMSML than K3, but not significantly. K3 also had greater trunk acceleration RMSML on their intact side than K4, but only for LW (p < 0.027). When a step width covariate was included in addition to the speed covariate, differences in trunk acceleration RMSML were no longer significant between K3 and K4, with the exception of US where K3 and K4 prosthetic limbs were significantly different (p < 0.005).
Comparison to AB
K3 participants walked significantly slower than AB for all conditions (p < 0.002, Table 4) and K4 walked significantly slower than AB for all conditions except US (p < 0.046). Both K3 and K4 had smaller walking speed variability than AB for MLT (p < 0.05). K3 participants had significantly greater step width than AB for LW, US, TS, BS, and MLT (p < 0.042); K4 participants had significantly greater step width than AB for US (p < 0.033); and K3 (p < 0.009) and K4 intact limbs (p < 0.025) had significantly greater step width SD than AB for US.
For downhill, K3 had significantly greater DST on the intact limb compared to AB (p < 0.002). K3 had significantly greater DST SD than AB for DS, US, and RO (p < 0.027), and K4 had significantly greater DST SD on both limbs than AB for US, BS, MLT, HL, and RO (p < 0.008). K4 also had significantly greater prosthetic DST SD than AB for TS (p < 0.001), and significantly greater prosthetic DST SD than AB for LW and DS (p < 0.002).
For uphill, K3 and K4 had a significantly greater ML-MoS on the prosthetic limb than AB (p < 0.039) and greater ML-MoS SD on both limbs (p < 0.01). On the intact limb, K4 had significantly greater ML-MoS SD than AB when walking downhill (p < 0.024) and K3 had greater ML-MoS SD than AB for BS (p < 0.004). K3 also had greater ML-MoS SD than AB on the prosthetic limb for DS (p < 0.016).
K3 and K4 had significantly greater trunk acceleration RMSML than AB for all conditions (p < 0.025) except for RO where the K4 intact limb was not significantly different from AB.
Limb asymmetries
K3 had greater step width on their prosthetic limb for TS (p < 0.005; Table 4). Both groups had significantly greater DST on the intact limb for DS (p < 0.029). K3 and K4 also had greater trunk acceleration RMSML when on their prosthetic side, for all conditions (p < 0.001). AB had a larger step width on the non-dominant limb for MLT (p < 0.008).
K3 had significantly greater ML-MoS and ML-MoS SD on the prosthetic side than the intact side, for US (p < 0.034). K4 had significantly greater ML-MoS on the intact side than the prosthetic for DS (p < 0.022) and greater ML-MoS SD on the prosthetic side than the intact for BS (p < 0.022).
K4 had significantly greater step width SD on the intact limb than the prosthetic limb, for TS (p < 0.001) and RO (p < 0.001) and significantly greater DST SD on the intact limb than the prosthetic limb for DS. K3 did not exhibit limb asymmetries in step width SD or DST SD.
Discussion
This study investigated TFA gait differences between K3 and K4 functional levels over level and non-level conditions, as well as differences from an AB group. The use of non-level surfaces revealed between-group gait differences that were not apparent with level walking, such as wider step width on cross-slopes and medial-lateral translations; greater ML-MoS SD for downhill, uphill, and bottom cross-slope; and differences between K3 and K4 groups on uphill and downhill walking. As hypothesized, K3 participants generally walked slower than K4 participants with wider steps, greater trunk acceleration RMSML, and greater ML-MoS SD. Contrary to expectations, K3 had significantly shorter DST SD than K4 for several conditions, and no significant differences were observed between K3 and K4 for step width SD or ML-MoS. Most K3 and K4 limb asymmetries were similar, but K3 participants exhibited greater asymmetry for DST and trunk acceleration RMSML. The outcome measures highlighted in this study could be used to quantify gait differences between TFA functional levels, and as compared to AB populations.
Trunk acceleration RMSML was the most consistent parameter that differed between K3 and K4, with greater results for K3 across nearly all walking conditions. Greater trunk acceleration RMSML is an indicator of trunk movement instability. 38 TFA can have difficulty positioning their trunk over the prosthetic limb, possibly from poor femur stabilization in the socket that effectively weakens the moment arm. Similarly, K3 may have less trunk control and poorer socket stabilization than their K4 counterparts. This could relate to increased trunk muscle activity that increases spinal load,39,40 leading to low back pain41–43 that is prevalent within the lower limb amputation population. 44
K3 participants walked with wider steps than AB in five of the eight walking conditions, but differences from K4 were only significant for cross-slopes and medial-lateral translations. Wider steps increase the base of support and could enhance stability for those with compromised balance. 5 While step width could have been influenced by prosthetic fit or alignment, step width for level walking was similar to other results in the literature. 8 Our K4 group had smaller step width and K3 had wider step width than published results.
Since step width has been proposed to influence trunk motion, 7 a step width covariate was applied when analyzing trunk acceleration RMSML. Trunk acceleration RMSML differences between groups became insignificant when applying a step width covariate, suggesting that differences between K3 and K4 were related to the K3 group’s larger step width.
K3 did not differ from K4 for mean ML-MoS, but had greater ML-MoS SD for downhill, uphill, and bottom cross slope. This indicated that K3 gait was further challenged than the K4 group when walking on non-level surfaces, 45 highlighting the relevance of variability measures when assessing movement patterns.
K3 participants walked slower than K4 for all conditions, but were only significant for level, cross slope, and rolling-hills. Considering the well-documented differences in walking speed between AB and balance-impaired populations,1,11 slower walking for K3 participants than higher functioning K4 was expected, especially over less familiar conditions such as cross slopes. K3 was also 6.8 years older and 8.4 kg heavier than the K4 group, which could contribute to their slower walking speed and overall reduced walking performance. Alternatively, slower walking speed could be related to extra time requirements to plan movements or less gait confidence. 46 Although K3 walked slower than K4 for downhill and uphill, these differences were not significant. K3 participants might not have needed to reduce speed more than K4, since they were already walking slowly.
Contrary to downhill walking, K3 participants had significantly less DST SD than K4 for the uphill, medial-lateral translations, and rolling-hills. This was unexpected since K3 gait was predicted to be more variable based on their lower functional level. However, differences were less than 1% and may not be clinically significant.
Differences between K3 and K4 in step width, DST, DST SD, and ML-MoS SD were not significant for level walking, but were significantly differently for many other conditions. This demonstrated how the challenge of navigating non-level surfaces can magnify differences between groups, and the importance of training gait on a variety of surfaces. Cross slopes had the most differences between K3 and K4 participants. This could be because, unlike level and inclined surfaces, cross-slope walking requires an asymmetrical gait pattern to keep the body vertical while adapting to different ground heights and angles. 47 This may pose a greater challenge for maintaining balance and forward progression. Thus, cross slopes should be included in prosthetic gait training.
A functional status progression was observed from K3 to K4 to AB. Overall, differences between the K3 and AB groups were larger and occurred for more parameters than differences between the K4 and AB; however, the higher functioning K4 group still exhibited significant differences from AB participants. The largest differences between K4 and AB were for walking speed, DST SD, and trunk acceleration RMSML, for nearly all conditions. K3 and AB differences for nearly all conditions were for walking speed, step width, and trunk acceleration RMSML.
Unlike K3, K4 and AB groups had similar step width, with the exception of uphill, which was the only condition where K4 walked faster than AB. Therefore, increased step width was not used as a compensation mechanism by the K4 group. This differed from other studies where TFA walked with wider steps than AB over level ground.1,11
K4 participants had similar DST magnitudes to AB, but greater DST SD for all conditions. However, K3 only had greater DST SD than AB for four conditions. While walking speed SD and DST SD are strong fall predictors in older adults, 16 no participants indicated falling during the study period (i.e. verbal report to prosthetist during prosthesis status evaluation). Additionally, walking speed SD was only significantly greater in AB participants than K4 and K3 for medial-lateral translations, possibly related to greater AB gait confidence that permitted greater walking speed fluctuations.
Future research in this topic area could expand the number of participants in the K3 and K4 groups, examine other factors that can affect gait across surface conditions, such as prosthetic components and fatigue, and verify the results in non-virtual environments.
Limitations
This study had small groups; however, significant between-group differences were found. K-level was determined by clinical assessment and, while accepted, other models based on movement assessment could be considered. Differences between participant’s prosthetic components could have affected walking performance across activities. However, all participants used prosthetic feet designed for variable speeds and terrain and mechanical knee user outcomes were within the range from microprocessor controlled knee users (no outliers with prosthetic knee).
A CAREN virtual environment was used, with conditions representing real-world scenarios and participants walking at self-selected speeds. While comparable to overground walking for persons with transtibial amputation, 48 this research was not reproduced with TFA. Therefore, some uncertainty exists for outcome transferability to the real world. However, walking in this virtual environment was similar enough to improve our understanding of how people accommodate to non-level conditions. Use of knee stance phase flexion or yielding during downslope walking was not investigated in this study involving stability-related measures. Medial-lateral translations and rocky conditions only simulated real-world uneven surfaces, because the treadmill was flat, with medial-lateral translations being similar to walking along a crowded hallway and the rocky condition provided a continuous variable platform angle. Additionally, many variables and conditions were analyzed in this exploratory study and the chance of type-I errors was increased.
Conclusion
This study examined differences between K3- and K4-level persons with TFA over level and non-level walking conditions. The most prominent difference between groups was in trunk acceleration RMSML, highlighting the importance of including a trunk parameter in gait assessment. K3 participants also walked slower and with wider steps than K4. Even the higher functioning K4 participants differed significantly from AB for walking speed, DST SD, and trunk acceleration RMSML. Cross slopes and uphill and downhill walking evoked the most significantly different outcome measures between K3 and K4, and between TFA and AB. This could have been due to the challenging nature of these conditions and potentially less experience walking on cross slopes. Gait training on these surfaces is recommended to ensure optimal mobility in the community.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Canadian Forces, Surgeon General Health Research Project Fund.