
Abstract
The value of gait analysis for research and product development/evaluation in prosthetics is well understood. However, in the rehabilitation of amputees, the application of gait analysis beyond observation in the clinical setting is not routinely practiced, largely due to the cost and time taken to complete a fully instrumented data collection and analysis. To address the time issue, a weekly clinical gait service for primary amputees, based around a reduced data set from video and video vector technology, has been developed. In this clinic primary amputees are seen twice in the Gait Laboratory during their rehabilitation period, with the clinic time for each patient being no more than 15 minutes, which covers both data collection and review.
A questionnaire was developed to evaluate the patients' perceptions of the clinic. The questionnaire was completed anonymously by 48 primary amputees over a 6-month period. The results from the questionnaire demonstrate that the clinic was perceived positively by the patients, and suggested areas of future development, e.g. the education of junior staff, and the need to include the patient's physiotherapist in the data collection and review process.
Introduction and background
One of the aims of the rehabilitation for primary lower limb amputees attending the physiotherapy led ‘Walking School’ at Queen Mary's Hospital (QMH), is to achieve a safe and long term functional gait. This usually requires that the deviations in walking and standing from a ‘normal’ pattern are minimized (Sanderson and Martin 1997). The presence of deviations, e.g. limited weight bearing through the prosthetic limb, excessive circumduction and differences in step length during walking, is common at the start of rehabilitation. There are two main reasons for this. Firstly, amputees can experience some degree of discomfort when initially fitted with a prosthesis as a result of the condition of the stump, and also as a consequence of the prosthetic fit (Barsby et al. 1995). Secondly, an amputee's gait can be compromised according to the level of amputation, proprioceptive and sensory loss, muscle strength imbalance, the presence of co-existing pathologies, psychological or social reasons, or as a result of habit (Engstrom and Van de Ven 1999).
Following observation and assessment, primary amputees receive feedback from their physiotherapist regarding their walking (gait) and standing, whilst manual facilitation also aims to improve the gait patterns seen. However, although verbal feedback is important, it can be difficult for patients to apply this when they cannot view their own gait. Even when this is possible, e.g. with mirrors, it can be difficult for some patients to appreciate the information in real-time, and this approach does not provide a direct method of determining symmetry in weight bearing. An alternative would be to make use of gait analysis tools and techniques.
There is a broad definition of the term ‘gait analysis’. It has been applied to the use of a number of data collection tools through which, in parallel with other measures, e.g. joint range of movement, muscle strength and patient self-assessment questionnaires, one can assess a subject's walking (and standing) pattern and plan a treatment programme. Without commenting on the validity or appropriateness of these tools, they range from visual observations made by a skilled clinician (Little 1981; Saleh and Murdoch 1985), the use of video, stop watch and measured distances (Stillman and McKeeken 1996), systematic review through the use of observational gait analysis tools (Brunnekreef et al. 2005; Pathokinesiology Service and the Physical Therapy Department 2001; Read et al. 2003), to instrumented kinematic, kinetic, electromyography and energy consumption measures (Harris and Wertsch 1994; Schmalz et al. 2002).
The concept that gait analysis can be a useful objective method of evaluating amputee progress was discussed by Baker and Hewison (1990). However, in a busy amputee rehabilitation clinic it can be very difficult to undertake any type of formal gait analysis, even at the basic level of measuring speed and cadence. Therefore, for the most part, gait assessments tend to be undertaken as part of the development and evaluation of prosthetic componentry, or in developing basic understanding of amputee movement (Czerniecki and Gitter 1996; Mulder et al. 1998; Rietman et al. 2002), for which the data can take time to collect and convert into a meaningful form.
The Walking School felt that their greatest problem was not in identifying how a given patient needed to improve their gait, but in conveying this information in a meaningful form to the patient. This has led to a video-kinetic data collection approach (gait clinic), which could be readily incorporated into routine clinical time. In this clinic, video images and ground reaction force (GRF) data are collected whilst the patient walks and stands on the force plates in the Gait Laboratory. The GRF data is superimposed as white lines onto the video image. This technique is known as force line visualisation (Wilson et al. 1979) or video vector (Tait and Rose 1979), with the equipment used in this setup following the method described by Rowe (1996). The force plates used are parallel 3.3 m platforms (Hynd et al. 2000), enabling multiple contacts to be recorded in one traverse of the laboratory, making them particularly suitable for primary amputees, whose walking may be limited through fatigue or discomfort. Both sagittal and coronal views are recorded.
Figure 1 illustrates typical screen shots of the video and the video vector lines. Figure 1a shows coronal data recorded at an instant in time during standing. The white lines give the resultant of the vertical and medial-lateral forces for each plate. In this case, however, as the right plate is loaded by both the leg and stick, the line for the right plate is the single point resultant of the load through the stick and the leg. Figure 1b shows sagittal data recorded during the walking cycle, just after right toe-off, so the only loading through the right plate is through the stick. In this figure, the white lines are the resultant of the vertical and anterior-posterior forces for each plate. For both figures, the numbers in the left hand corner are the vertical force in Newtons.
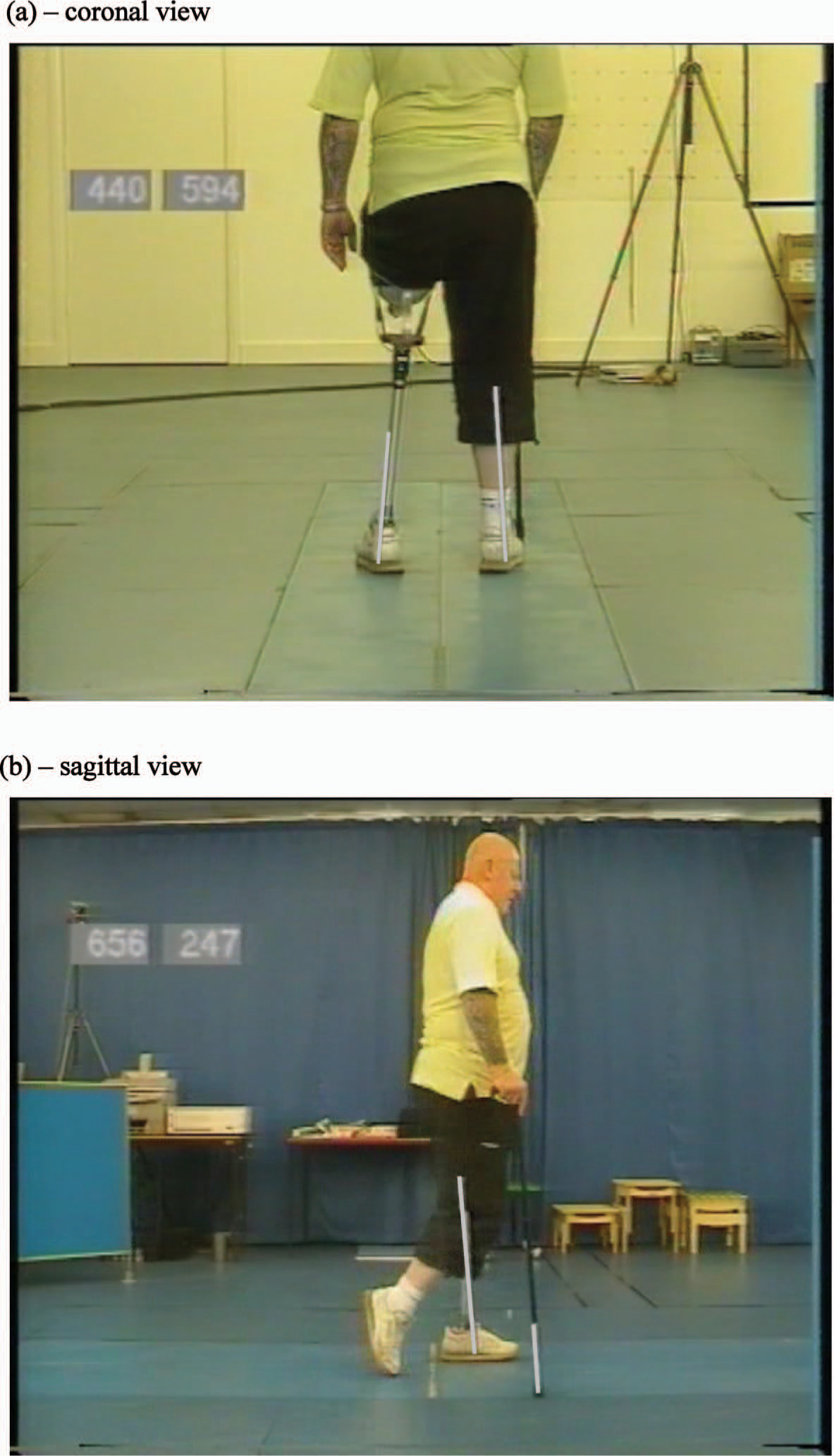
Screen shot illustrating video vector lines: (a) coronal view during standing and (b) sagittal view during walking, just after right toe-off.
Most primary amputees attending the Walking School now attend this clinic within the first or second week following the fitting of a prosthesis, and one to two weeks later to evaluate progress. At the end of each recording, the patient and the physiotherapist view and discuss the video with Gait Laboratory staff, focusing on asymmetry in posture and weight bearing during standing, and asymmetries in weight bearing, posture and gait deviations in walking. Care is taken to present the information as feedback only and not as the result of a ‘test’, and to provide the patient with clinically realistic expectations/targets of symmetry. The process from each patient entering to leaving the Laboratory takes up to fifteen minutes. Findings are then related to the patient's goal setting and treatment planning in the Walking School.
The introduction of routine visits to the Gait Laboratory is recent and innovative. The informal feedback from both patients and physiotherapists has been positive. However, it has not been followed up in a systematic manner to establish the benefits to the patients or the improvements/changes they would like to see in the approach taken. The clinicians involved in this recent innovation felt that there was a need to optimise the experience of the patient within the confines of manageable clinical practice. The opinions of NHS users have been encouraged by several UK government papers in recent years, e.g. Department of Health (1997), and consequently there is currently a strong emphasis for patient involvement in assessing the quality of healthcare. Holman (1993), in his commentary into medical research, discusses the need for enquiry and investigation into patients' perceptions and attitudes towards their rehabilitation. Therefore a study to evaluate this new practice was undertaken.
Aims of the study
The study was designed to address four important areas of the patients' perceptions of
attendance in the gait laboratory: Whether the information and instructions provided were felt to be adequate If they found the process of being observed unsettling in any way Were the sessions useful and if so what was useful Did the sessions highlight information that would be relevant to their
rehabilitation
Method
A questionnaire was developed in conjunction with the Clinical Governance Department at the Hospital. Section 1 comprised of questions to elicit general background information on the patients who were completing the questionnaire (age, sex, level of amputation and time since limb fitting) and a check question to determine if patients had previously been to the Gait Laboratory. The questions in Section 2 aimed to provide feedback on the patient's perception of why they were attending the gait session, how they felt about the background information provided to them by the clinical staff, and their preliminary feelings about being ‘recorded’. Section 3 questions were written to identify the patients' perceived benefits of the gait laboratory sessions. Sections 2 and 3 are based upon Likert scales (Oppenheim 1992), with the respondents asked to provide a score on a 1 to 10 range, except for one multi-part question in Section 3, for which a 5 point scale was used, and another for which a (Yes, No, Do Not Know) category scale was used. A final open-ended question gave the patients an opportunity to provide any additional comments that they felt would be helpful. The questionnaire was intended to be straight forward and completion was expected to take no more than ten minutes.
The inclusion criteria were that the patients should be primary lower limb amputees, attending the QMH Walking School, and aged over 18. The exclusion criteria were patients with impaired vision, non-English speaking patients, and patients with cognitive impairment.
The questionnaire was piloted to test the appropriateness of the content (content validity). The first version was sent to clinical specialists working within the field of lower limb amputee rehabilitation at Queen Mary's Hospital to get their feedback on whether the questions were understandable, unambiguous, relevant and addressed the aims of the project. Following feedback from these colleagues and the Hospital's clinical governance team, the revised questionnaire was then piloted on ten patients, chosen at random from those patients meeting the inclusion criteria. Once completed, the questionnaire was discussed with each subject individually to identify any ambiguity and misunderstanding. As a result of the pilot study minor changes to the questionnaire were made.
Over a period of 6 months, 48 patients completed the questionnaire the day after their first visit to the Gait Laboratory and the day after their second visit to the Laboratory. These were patients who had not attended the Gait Laboratory for any reason prior to the first visit, and who also were new patients to the Walking School. On both occasions the questionnaire was completed anonymously, and once all data collection had been completed, the questionnaires were forwarded to the Clinical Governance Department for preliminary analysis. To enable the anonymous data to be collected into pairs for each patient, the personal data of sex, age, level of amputation and time since limb fitting were used. To minimise bias in responses from the patients based on the prior association of the senior therapists in the Walking School with the Gait Laboratory staff, the task of accompanying patients to the Gait Laboratory and asking them to complete the questionnaires was undertaken by the junior physiotherapists who were working in the Walking School as part of their rotational training.
Results
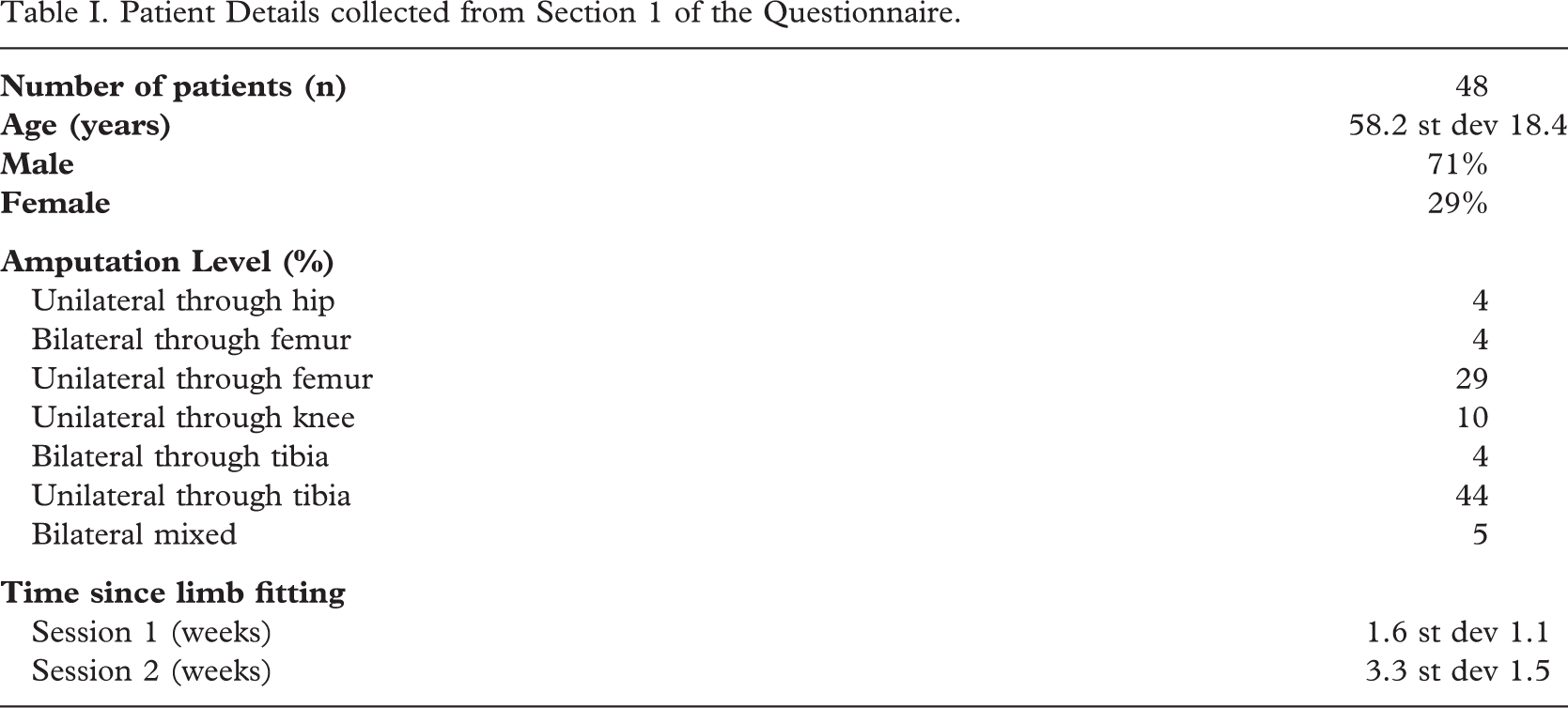
Table I shows the (self-reported) details of the patients included in the study and reports the time since limb fitting at each session.
Patient Details collected from Section 1 of the Questionnaire
The results from the patient feedback are summarized below. For the Likert questions, the summary indicates the percentage of responses indicating a neutral response or better. For some of these questions where the data is quite spread, figures have been included.
A 10 point (1 – 10) scale was used with the three Section 2 questions to assess the quality of the background information and instructions patients were provided with, and their feelings about being recorded at the 1st and 2nd visits - Aims (i) and (ii) - with a score of 6 or above to represent a neutral response or better. From this, no patients reported problems with following the instructions, 77% of patients reported the experience to be as they expected at session 1, rising to 98% at session 2, Figure 2a, and only 10% at session 1 and 6% at session 2 felt self-conscious about walking in the Gait Laboratory, Figure 2b.
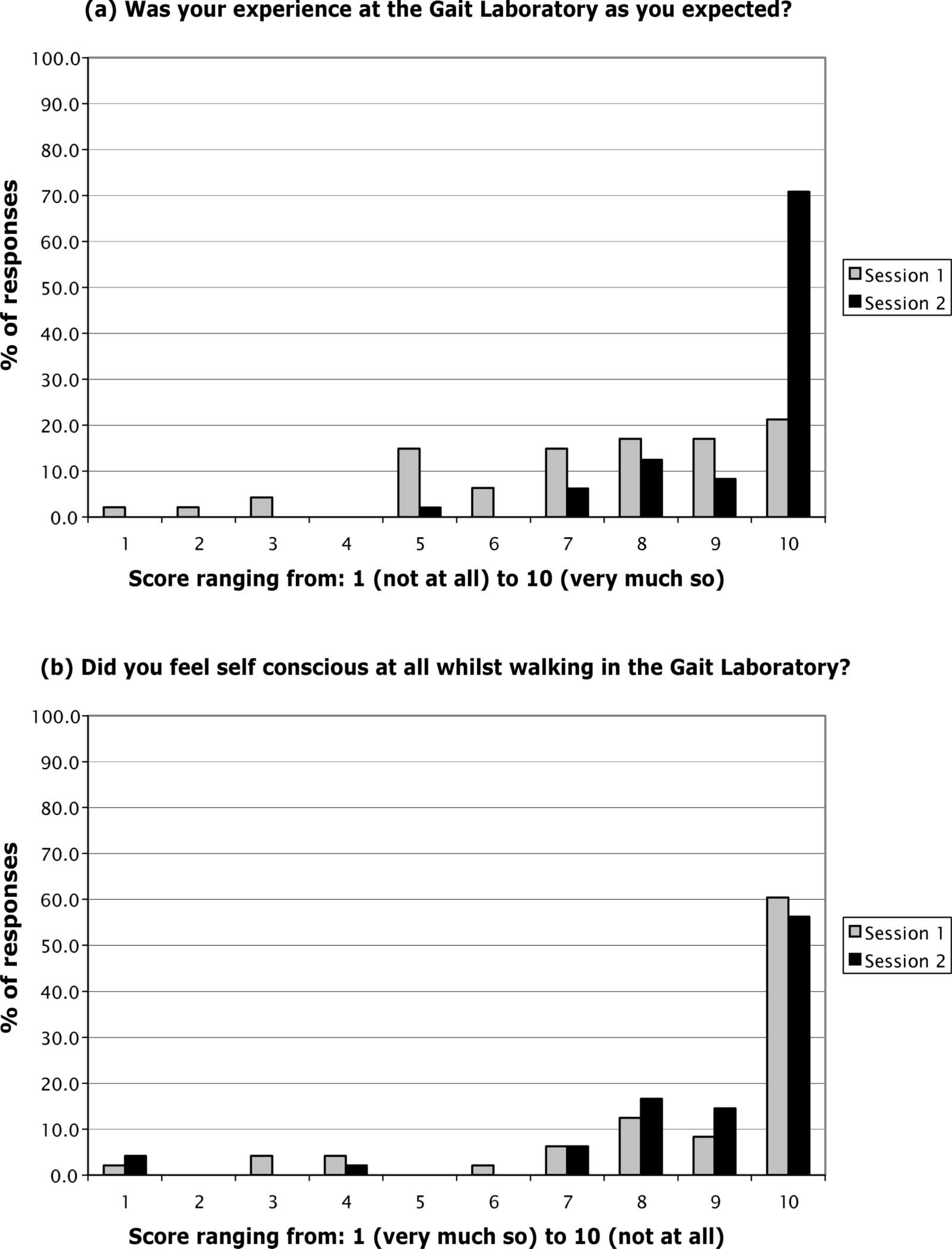
– b. Patients' responses to Section 2 of the Questionnaire.
Seven questions were used in Section 3 to determine the perceptions of the patients to the usefulness of the gait laboratory sessions - Aims (iii) and (iv). The first four of these concentrated on specific elements of the review sessions and a 5 point scale was used, with a score of 4 or higher being used to indicate a neutral or better response. For the more general questions, a 10 point scale was used for two questions, with a score of 6 or above taken as a neutral response or better, and a simple Yes/No/Do Not Know for the final question.
For the specific questions, 100% of patients at session 1 and 98% at session 2 were positive about being able to review their standing and walking posture. For evaluating their gait deviations the figures were 94% and 100%. At session 1, 96% of patients found the video vector lines to be useful, with this figure rising to 98% at session 2. In terms of what to concentrate on in the future, 96% of patients at session 1 and 100% at session 2, found the video to be useful.
For the general questions, Figure 3a shows that 76% of patients at session 1 and 100% at session 2 found the video to confirm their own thoughts on their gait. For Figure 3b, 43% of patients at session 1 and 38% patients at session 2 reported that the video did identify problems not previously noted by their physiotherapist. For the final general question, at both sessions 96% of patients thought other visits to the Gait Laboratory would be useful, with 2% saying No and 2% Do Not Know.
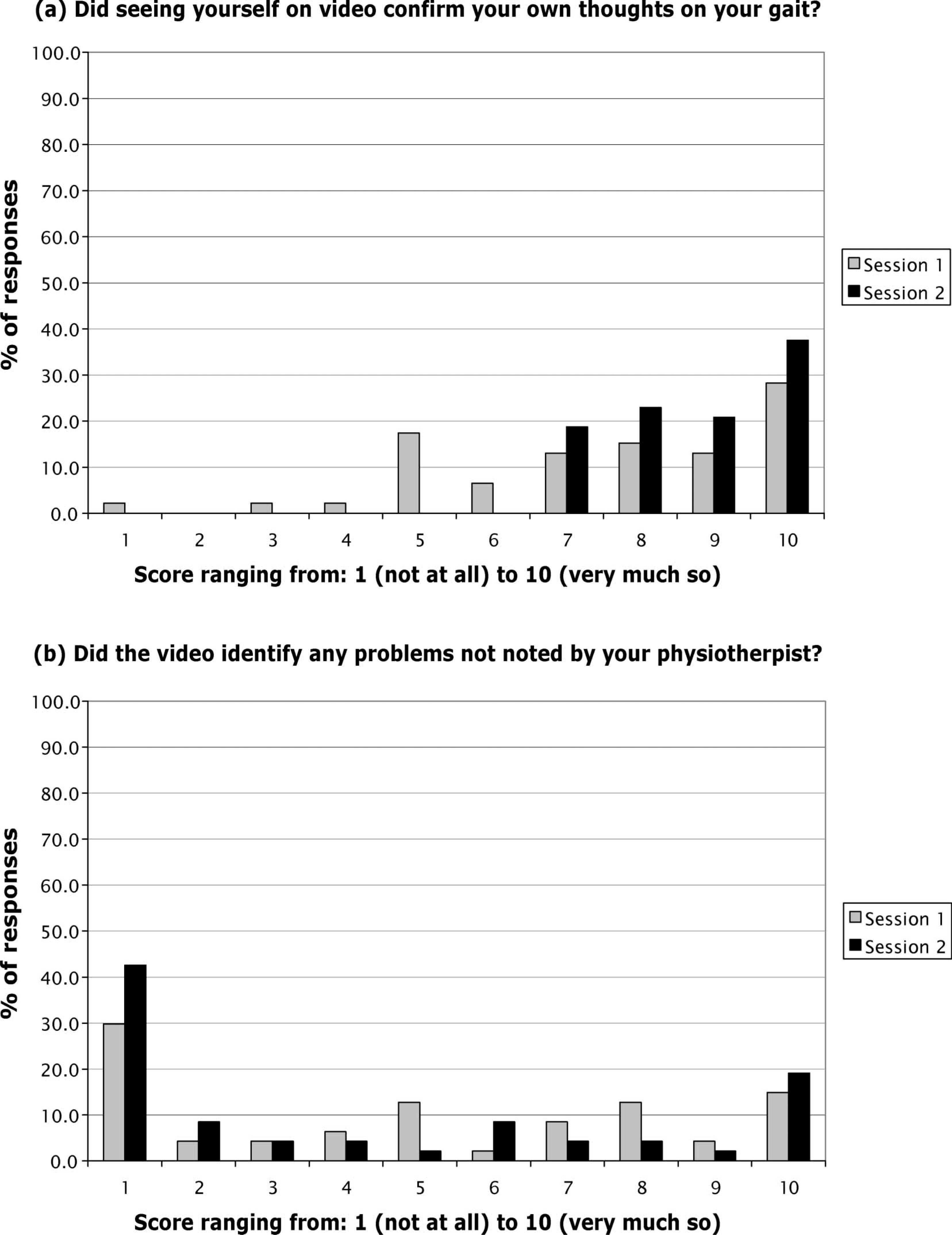
– b. Patients' responses to Section 3 of the Questionnaire – general questions on the information presented.
For the open-ended question asking patients for any further comments or suggestions about the whole process, of 96 possible replies, 26 patients responded, 17 in session 1 and 9 in session 2, with 7 responding in both sessions. All of these responses were very positive, apart from one patient who commented that the lab should be used after the 2nd week only, but did not expand upon this. A common theme in these responses was that patients felt that being shown (through the video) is better than being told, and how it is much easier to see the relevance of their therapy ‘targets’ once they have been in the gait lab. Three patients commented that it would be helpful if the (2.5 m) parallel bars in the Gait Laboratory were of a similar length to those in the Walking School, so that they could walk as they do in the Walking School, and one patient commented that it would have been helpful if the explanation and review of the video could have been slower. One patient whilst being positive about being able to review herself walking, noted that she was a little self-conscious about walking in the laboratory, but was “well supported” by the physiotherapist. A further patient, who was not accompanied by his own physiotherapist, commented that the large room was a little impersonal, but still found the review helpful.
Discussion
A record of which patients were involved in this study was not made; however, the clinical team felt that they were representative of the general population seen in the Walking School. The authors were therefore surprised by the high number of (self-reported) through knee amputees in Table I. It is believed that this is most likely due to the errors by the patients in completing the form or a misunderstanding of the formal wording used for their level of amputation. It is much more likely that the majority of these patients are unilateral trans-femoral amputees and given this, the figures for amputation level, together with those for age and male/prevalence would be in-line with those published for the Hospital in NASDAB (2004).
The authors goal was to see primary amputees within the first or second week of fitting and then one to two weeks later. The mean figures for time since limb fitting in Table I would suggest that this goal was met, though the standard deviation is relatively high. However, given the problems that often need to be overcome to achieve a ‘good’ prasthetic fit, the values of the standard deviation are not unexpected.
The results from Section 2 suggest that the patients were very content with the instructions given by the staff and that only a small minority felt self-conscious about the recording process itself. However, the results would suggest there appears to be some inconsistency between the expectations and experience of the first session, which is (unsurprisingly) resolved by the 2nd session. This could reflect the fact that some of the Walking School physiotherapists were junior staff on 4 monthly rotations and therefore did not always know themselves what happens in the gait laboratory sessions. This highlights the importance of effective communication between the Gait Laboratory and the Walking School, and may also suggest that it would be helpful to run in-service training on clinical gait analysis for the physiotherapists on rotation, and this needs further investigation.
In terms of the perceived benefits of coming to the Gait Laboratory (Section 3 of the questionnaire), the results are very encouraging. The results from the specific questions demonstrate clearly the perceived usefulness of the video vector and video in showing asymmetries in weight bearing during standing and walking, identifying concerns over posture and gait patterns, and what to think about in future walking school sessions. Video alone could be used to identify gait deviations such as step length, however, the video vector is necessary to show directly the weight that is taken through each leg (or leg and stick, if both are in contact with the plates simultaneously) during standing and walking. The session 1 results from Figure 3a do support the idea that some patients have difficulties in visualising their gait. Figure 3b is interesting in that at both sessions, less than half the patients said that the video reported problems not noted by their physiotherapist. This may suggest that a key benefit of attending the gait sessions, is not to be given new information, but to be able to visualise the comments being made by their physiotherapist. This supports the inference drawn from Figure 3a. The fact that 96% of patients thought further visits would be useful demonstrates the very positive interest that the patients have in the use of the Gait Laboratory.
The responses made in the open-ended question reflect the summary above and suggest that for some patients at least, the sessions would be more helpful if their own physiotherapist attends with them. The comments also show that there is a clear need to provide longer parallel bars to enable the patients to be able to walk as they do in the Walking School. A further observation by the clinical team was that it would be helpful in a number of cases if the patients' prosthetist could be involved in the data collection, or at least time be set aside to allow them to view the video.
Although the results are positive the authors are aware that the questionnaire approach taken to evaluate perceptions is not without its limitations. Oppenheim (1992) states that with predominantly closed questions there is a loss of spontaneity and expressiveness, and the potential for bias by forcing respondents down particular paths. However, Fitzpatrick (1991) does suggest that a well piloted and self-completed questionnaire need not be such a poor second choice to the interview based approach.
For the purpose of this study and given the expected large number of participants, it was considered more appropriate to use a descriptive, self-administered and anonymous questionnaire, to be used longitudinally, i.e. to coincide with the two visits to the gait laboratory. It was anticipated that the one open question would produce comments that in themselves might indicate a pattern or trend, and possibly areas for further investigation.
Conclusions
A key aim of this investigation was to establish whether patients found this method of visual feedback on their symmetry of weight bearing and analysis of walking patterns useful and informative. Clearly what has not been done in this study is to objectively measure relevant outcomes, e.g. changes in gait or posture and weight bearing, or determine if there has been a decrease in rehabilitation time as a result of the introduction of the gait laboratory sessions. This remains an interesting area of further work. However, the patients who participated in this study perceived an improvement in their quality of care and an understanding of what to work on in their rehabilitation programmes through these gait sessions. The review by May (2001) suggests that patient satisfaction can have a significant effect on important outcomes of healthcare, e.g. compliance with medical advice and improvements in health status.
The results suggest that patients perceive the use of real time video vector superimposed on sagittal and coronal plane video, to give visual feedback on weight distribution and symmetry in standing and walking to be an acceptable and helpful adjunct in their rehabilitation. With the gait facility available, this video/video-vector analysis of standing and walking is relatively inexpensive and quick. The authors believe it offers the type of novel (gait) assessment encouraged by Mulder et al. (1998), in that it informs the clinician about the more functional aspects of gait rather than focusing in on a detailed analysis of forces, joint angles and muscle activations, and goes some way to addressing the concern raised by Gard (2006), who proposes that “greater attention must be paid to gait training for new amputees, and retraining for more experienced users to break their bad habits and to instill proper form.”
This questionnaire evaluation suggests that the approach presented in this work offers benefits to patients and may be used as a teaching tool for clinical staff involved in amputee rehabilitation.
Footnotes
Acknowledgements
The authors would like to thank the junior physiotherapy staff in the Walking School for collating the questionnaires and the patients for completing them. They would also like to acknowledge the Clinical Governance Department at Queen Mary's Hospital, for its support in the development of the questionnaire and preliminary data processing.