
Abstract
Background:
Stair negotiation is biomechanically more challenging than level gait. There are few biomechanical assessments of transtibial amputees descending stairs and none specifically related to falls. Stair descent may elicit more differences than level gait in amputees with and without a previous falls history.
Objectives:
The aim of this study was to compare the gait kinematics of fallers and non-fallers during downwards step transitioning in transtibial amputees.
Study design:
Cross-sectional study.
Methods:
Six fallers and five non-fallers completed step transition trials on a three-step staircase at their self-selected pace.
Results:
Nine participants exhibited a clear preference to lead with the affected limb, while two had no preference. Four participants self-selected a step-to rather than a reciprocal stair descent strategy. The fallers who used a reciprocal strategy walked 44% more quickly than the non-fallers. To compensate for the lack of active plantar flexion of the prosthetic foot, exaggerated range of motion occurred proximally at the pelvis during swing. The step-to group was more reliant on the handrails than the reciprocal group and walked more slowly.
Conclusion:
As anticipated, the fallers walked faster than the non-fallers despite employing the more difficult ‘roll-over’ technique. Handrail use could help to improve dynamic control during downwards step transitions.
Clinical relevance
Transtibial amputees are advised to descend steps using external support, such as handrails, for enhanced dynamic control. Hip abductor and knee extensor eccentric strength should be improved through targeted exercise. Prosthetic socket fit should be checked to allow adequate knee range of motion on the affected side.
Background
Like stair ascent, walking down stairs involves the rhythmic shift of body weight in the vertical and horizontal directions. Stair descent is characterised by eccentric forces from the ankle plantar flexors and knee extensors during the weight acceptance (loading) and controlled lowering (pre-swing) phases.1,2 The controlled lowering phase is accomplished through large eccentric muscle forces, particularly about the knee, and corresponds to a phase in the gait cycle when failure could result in a fall. 3 Falls that occur during stair negotiation are more likely to happen during stair descent than ascent, and the consequences are often more severe.4,5 Difficulties descending stairs have been linked with poor balance and gait abnormalities in non-disabled older adults. 6 Reeves et al. 4 have shown that older adults function close to their biomechanical limits during stair descent.
Compared to able-bodied individuals, transtibial amputees exhibit altered lower limb mechanics as a result of reduced joint mobility, muscle weakness, postural instability 7 and gait modifications that predispose them to falling. 8 Previous research found that 52% of lower limb amputees fall annually and that 75% are recurrent fallers. 9 These numbers are significantly higher than among age-matched, able-bodied individuals. Moreover, these values may be underestimated as not all falls are reported.
There are few studies that have conducted biomechanical investigations of transtibial amputees transitioning downwards on steps, and the mechanical adaptations they make during this complex task are not as well understood. Previous reports demonstrated that transtibial amputees maintain the knee extended on the affected side for a longer period of time to compensate for the loss of the dorsiflexor and plantar flexor muscle groups during stair descent.10,11 They also noted that the amputees ‘fall’ onto the intact leg, which was considered a compensatory movement related to the excessive loading at the ankle and knee joints of this limb. 10
There is a paucity of research into downwards step transitioning in transtibial amputees and specifically in relation to falls. Such evidence-based findings would have important implications for rehabilitation programmes by making recommendations for targeted exercises to improve musculoskeletal function. The aim of this study was to compare the gait kinematics of transtibial amputee fallers and non-fallers transitioning downwards on steps. We predicted that amputee fallers would step downwards more quickly than the non-fallers. This was based on our previous observations that the fallers walked more quickly over level ground and during stair ascent.8,12 It was also anticipated the fallers would exhibit increased joint mobility, compared to the non-fallers and that this would be especially evident at the lower limb joints on the affected side. This was expected because the fallers demonstrated greater joint range of motion (ROM) on the affected side during stair ascent. 12
Methods
Participants
A total of 11 transtibial amputees were recruited from the local Artificial Limb Unit (Table 1). Participant inclusion criteria specified participants must have worn their prosthesis on a daily basis without experiencing pain and were able to ascend and descend a three-step staircase independently without walking aids, although the use of handrails was permitted. Participants were classified as either fallers (n = 6) or non-fallers (n = 5) based on their falls history in the 9-month period leading up to testing. As described previously, 12 one participant fell during stair descent specifically, two participants fell during stair ascent, and three fell during level and/or slope walking in the 9-month period preceding testing. Moreover, no significant differences were found between the two groups for physical characteristics as reported in our earlier studies.8,12 This study was approved by the National Health Service (NHS) Local Research Ethics Committee (REC number: 05/Q1105/68). All participants gave written informed consent to take part in this research.
Mean (SD) participant characteristics and stair descent strategies.
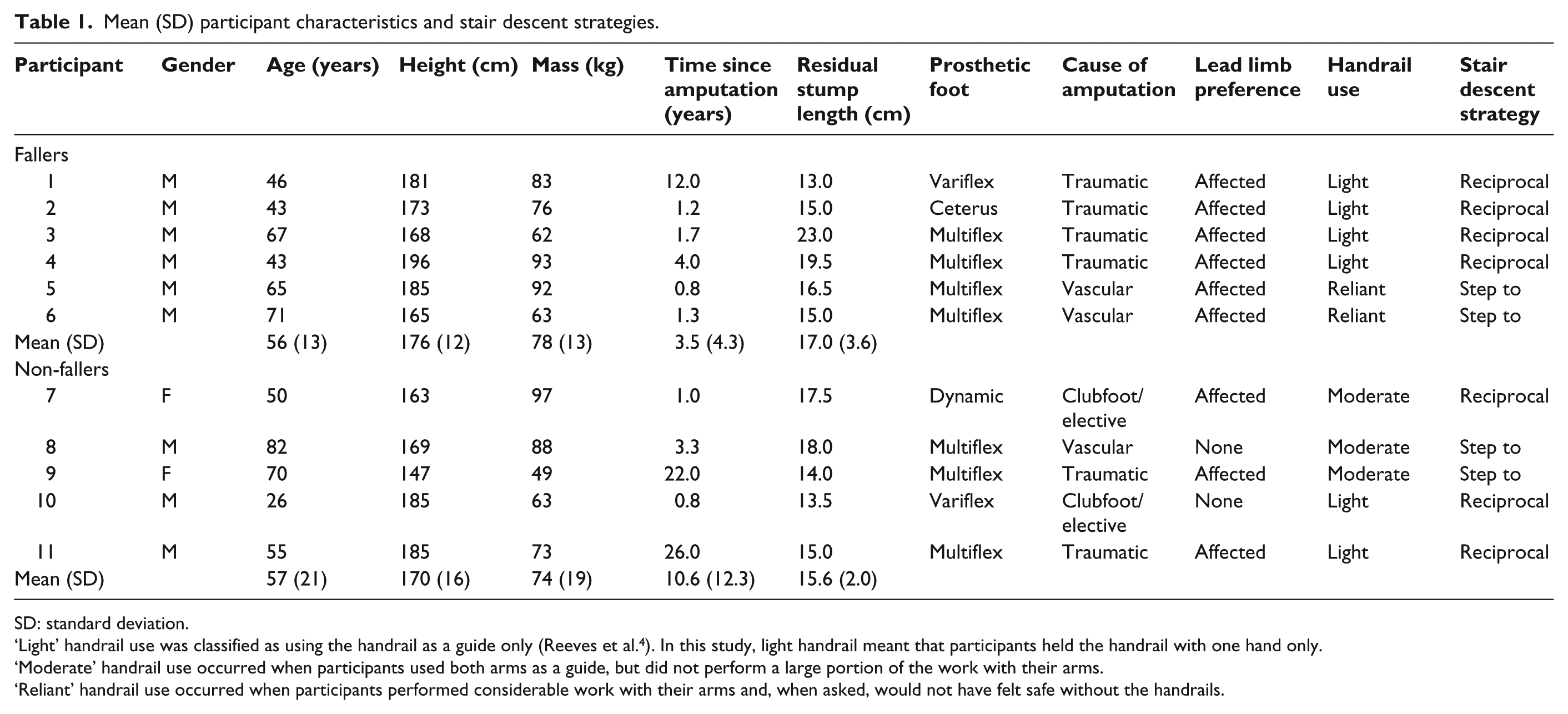
SD: standard deviation.
‘Light’ handrail use was classified as using the handrail as a guide only (Reeves et al. 4 ). In this study, light handrail meant that participants held the handrail with one hand only.
‘Moderate’ handrail use occurred when participants used both arms as a guide, but did not perform a large portion of the work with their arms.
‘Reliant’ handrail use occurred when participants performed considerable work with their arms and, when asked, would not have felt safe without the handrails.
Staircase
A three-step wooden staircase was built for this study. The steps were 80 cm wide, with a rise of 20 cm, a tread of 25 cm and a final tread of 80 cm. These dimensions conformed to Building Regulations 2010 for England. Wooden handrails were 50 cm high and attached to the main structure 12 (Figure 1).
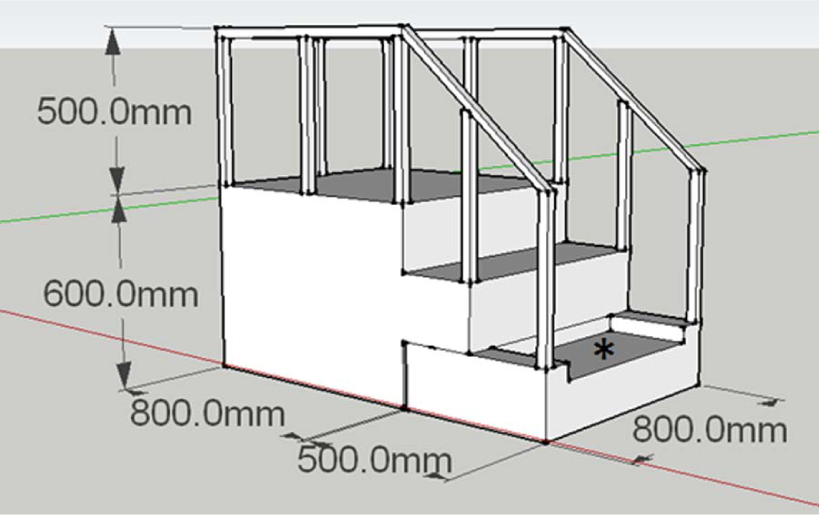
Illustration of the 3-step staircase used for stair descent and the step dimensions.
Protocol
Three-dimensional (3D) kinematic data were obtained from 10 ProReflex MCU1000 cameras sampling at 100 Hz using Qualisys Track Manager software (Qualisys, Sweden). The calibration details have been reported previously. 12 All participants completed the test wearing their own comfortable walking shoes. A six-degrees-of-freedom marker set-up for static and dynamic trials was used.8,12 Participants first climbed the three-step staircase at their own pace. After turning around and a self-selected rest period on the top landing, participants took up to two steps on the landing before descending the three steps, and kinematic data were captured for a total of 12 trials involving downwards step transitions at the top and bottom of the staircase.
Data analysis
Kinematic data were processed and analysed as before 8 and normalised to the gait cycle starting with toe off. 1 As participants were instructed to descend the steps naturally, the data were first inspected to determine their lead limb preference. This revealed that 9 of 11 participants displayed a preference for leading with the affected limb, while two had no clear limb preference. Therefore, the affected limb was selected as the lead limb for all participants. With a reciprocal strategy and descending two vertical step heights, the affected (lead) limb transitioned from the first step to the floor; the unaffected (trail) limb transitioned from the top landing to the second step. As the gait cycle was initiated and terminated with toe off, 1 the stance phase for the affected limb occurred on the floor. Two fallers and two non-fallers used a ‘step-to’ strategy meaning that they descended one step at a time. Under these circumstances, the total vertical distance covered by each limb was only one step (Table 1). Thus, the gait cycle from the first to the second step was analysed for the step-to participants. Given that the participants displayed rather unique stair descent strategies, each group was separated into those who used reciprocal versus step-to descent strategies and group numbers were reduced. Thus, it was not deemed appropriate to conduct statistical analysis as the sample size was reduced. The following ‘Results’ section uses descriptive statistics to compare the groups according to falls history and strategy.
Variables
The gait variables that were selected for analysis included (1) temporal–spatial parameters: average resultant walking speed (m/s) and support times (as % of gait cycle); along with (2) joint kinematics at specific time points (°) and ROM across the full gait cycle for the hip, knee and ankle bilaterally. Data were analysed in the sagittal plane, but hip and pelvic kinematics were also analysed in the frontal plane.
Results
The data are presented for fallers versus non-fallers who used a reciprocal and step-to downwards step transition strategy according to affected (lead) and intact (trail) limbs.
Temporal–spatial variables
Of the participants using a reciprocal strategy, the fallers walked 44% more quickly compared to the non-fallers. There were no meaningful differences between fallers versus non-fallers for stance phase duration.
The step-to groups were markedly slower overall, with the fallers walking 29% more slowly compared to the non-fallers. The step-to fallers walked 66% more slowly than the fallers who used a reciprocal strategy. The step-to fallers also exhibited a 15% longer affected stance phase and 5% longer intact stance phase compared to the non-fallers (Table 2).
Mean (SD) temporal–spatial and sagittal plane peak joint kinematics according to falls history and stair descent strategies.
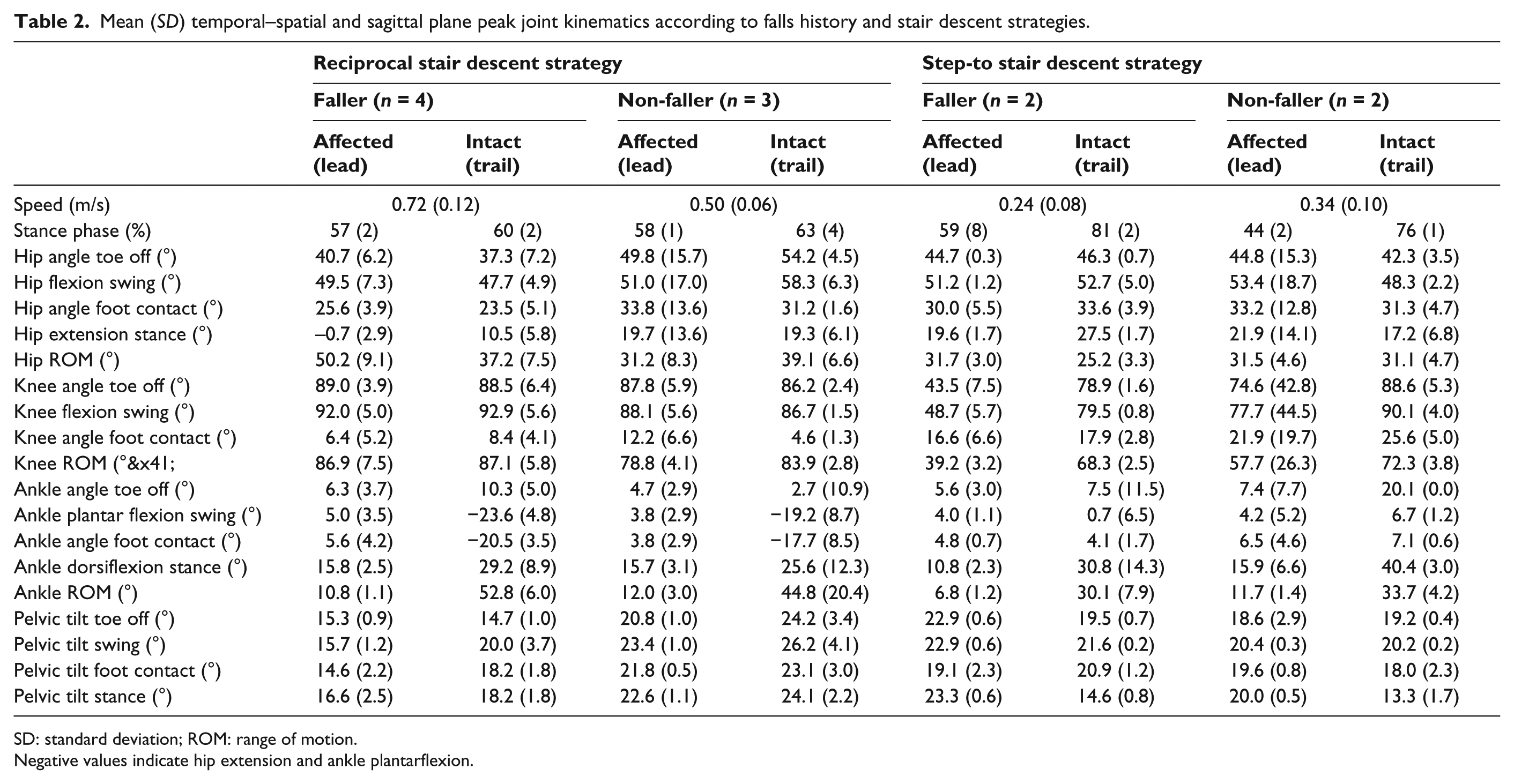
SD: standard deviation; ROM: range of motion.
Negative values indicate hip extension and ankle plantarflexion.
Sagittal and frontal kinematic variables – reciprocal downwards step transition strategy
Peak sagittal and frontal plane joint and pelvic kinematics are presented in Tables 2 and 3 and illustrated in Figures 2 and 3, respectively.
Mean (SD) frontal plane peak joint kinematics according to falls history and stair descent strategies.
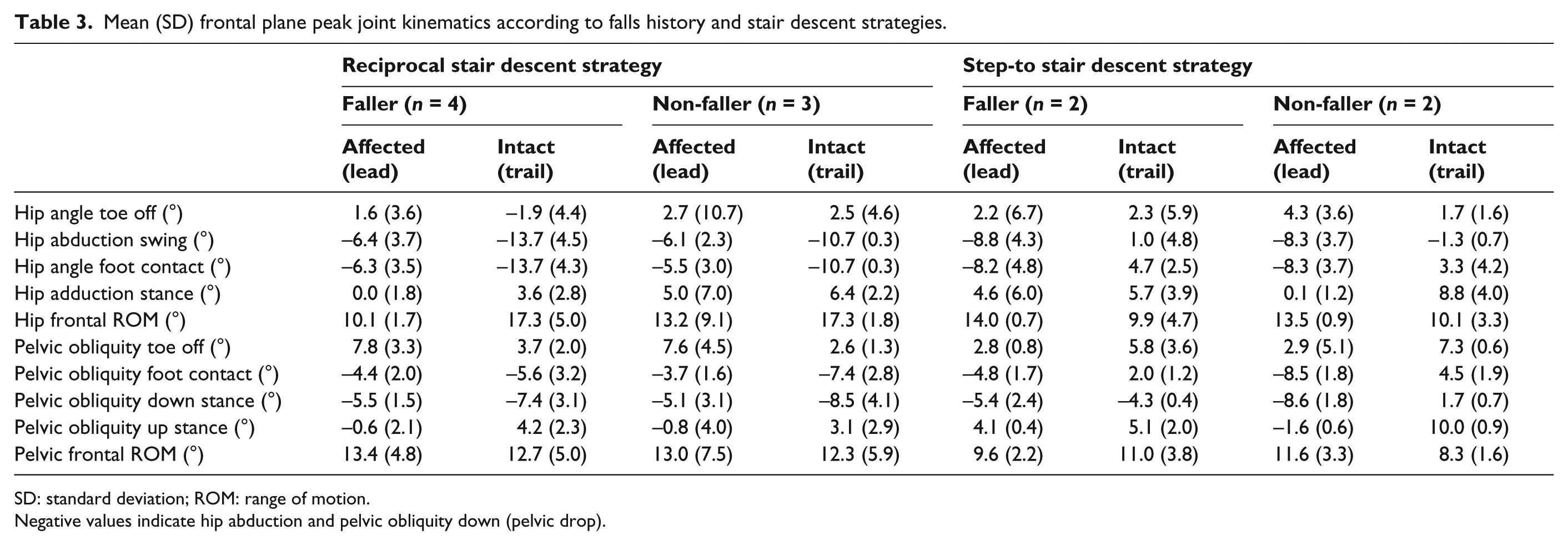
SD: standard deviation; ROM: range of motion.
Negative values indicate hip abduction and pelvic obliquity down (pelvic drop).
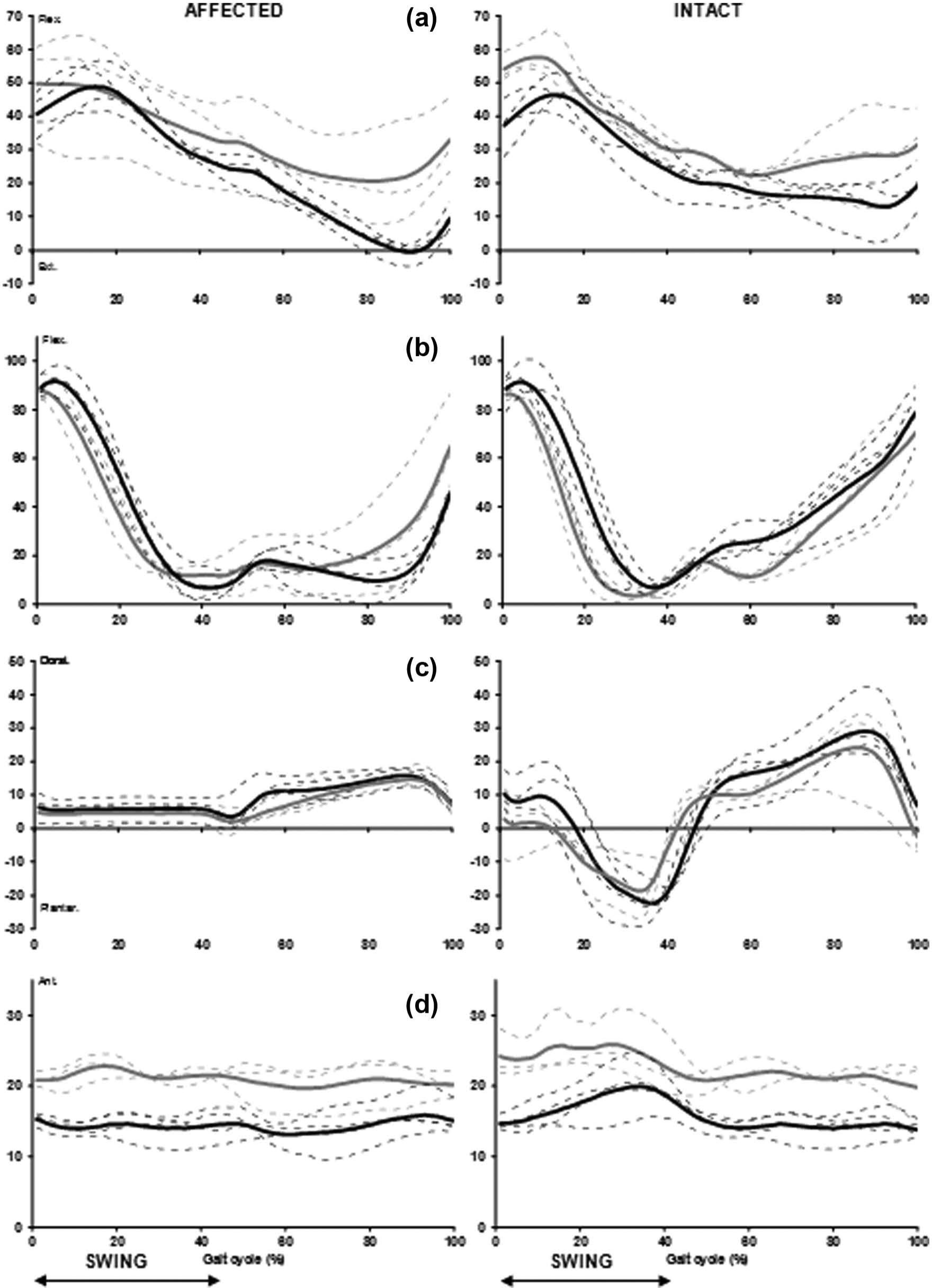
Average sagittal plane joint kinematics of the (a) hip, (b) knee, (c) ankle and (d) pelvis for the fallers (bold black line) and non-fallers (bold grey line) using a reciprocal stair descent strategy.
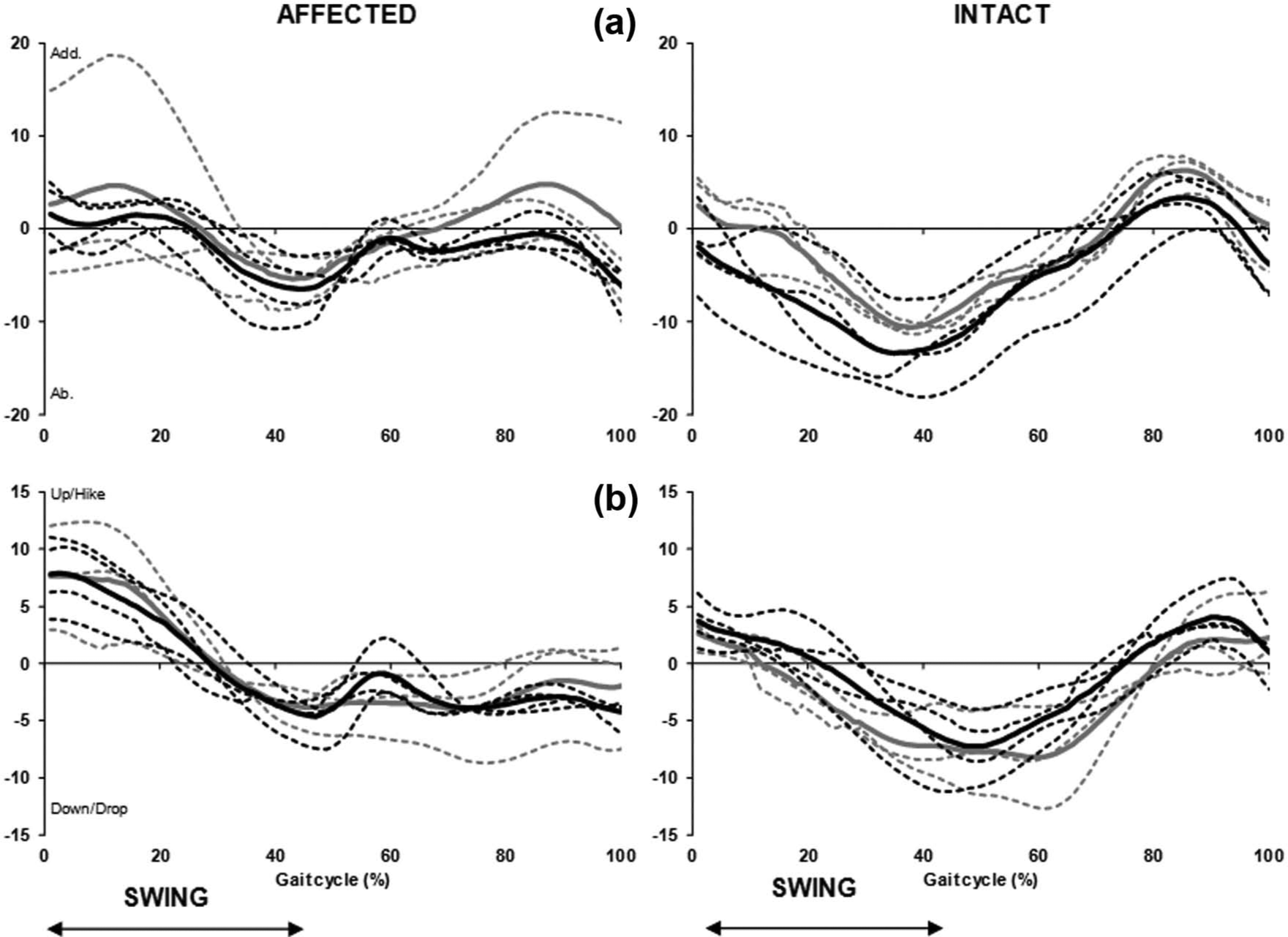
Average frontal plane joint kinematics of the (a) hip and (b) pelvis for the fallers (bold black line) and non-fallers (bold grey line) using a reciprocal stair descent strategy.
Notable differences were found for peak hip extension during late stance (pre-swing) on the affected side when the foot was on the floor. While the fallers displayed full hip extension (−0.7 ± 2.9°), the non-fallers showed almost 20° of flexion (Table 2). The hip on the affected side revealed almost 61% greater ROM in the fallers compared to the non-fallers.
Less obvious kinematic differences were found at the knee joint. The fallers displayed less knee flexion at foot contact on the affected side compared to the non-fallers. Overall knee ROM was not too dissimilar across both groups and between limbs.
Compared to the non-fallers, the fallers exhibited more ankle dorsiflexion (7.6°) at toe off on the intact side (Table 2). As expected, a between-limb difference occurred at the ankle joint where the prosthetic ROM remained in dorsiflexion and was almost a quarter of that observed on the intact side. On the affected side, foot contact occurred with the ankle almost neutral, whereas on the intact side, the ankle was plantar flexed at approximately 20° and 18° (fallers and non-fallers, respectively).
Peak anterior pelvic tilt tended to occur during mid-swing. The fallers exhibited on average at least 5° less anterior pelvic tilt compared to the non-fallers (Figure 2).
Participants displayed minimal hip adduction at toe off, followed by increasing hip abduction of the affected limb during swing in preparation for foot placement. The most noteworthy difference occurred during mid-stance, where the fallers exhibited a neutral angle on average, whereas the non-fallers exhibited 5° more hip adduction on the affected side (Table 3, Figure 3).
Both groups showed very similar frontal plane pelvic ROM and initiated toe off with the pelvis up (pelvic hike). From toe off through swing, pelvic hike changed to pelvic drop as the swing leg was preparing to make foot contact with the step below (Figure 3).
Sagittal and frontal kinematic variables – step-to downwards step transition strategy
The step-to fallers maintained the hip approximately 20° and 17° more flexed on the affected and intact sides, respectively, during stance compared to the reciprocal group (Table 2). They also had a smaller hip ROM (31.7 ± 3.0°) compared to the fallers with a reciprocal strategy (50.2 ± 9.1°).
The most noteworthy difference at the knee joint was that the fallers maintained the knee on the affected side less flexed at toe off and during swing and exhibited almost 19° reduced ROM compared to the non-fallers (Table 2). Moreover, ROM on the affected side was less than half the ROM for the fallers using a reciprocal strategy.
For both step-to groups, the intact ankle remained dorsiflexed throughout the entire gait cycle and was dorsiflexed greatly (over 40°) for the non-fallers during late stance (Table 2).
Hip adduction profiles were varied with little difference between the fallers and non-fallers. The hip was abducted on the affected side in swing. For both groups, hip ROM in the frontal plane was larger on the affected side compared to the intact side (Table 3). Pelvic obliquity was very similar.
Discussion
The aim of this study was to contrast the gait patterns of fallers and non-fallers during downwards step transitioning, as multiple stair descent cycles could not be achieved with a three-step staircase. All of the participants were able to complete the task successfully, although four amputees (two fallers and two non-fallers) self-selected a step-to rather than a reciprocal stair strategy.
Reciprocal downwards step transition strategy group
Temporal–spatial
Our predictions related to walking speed and the results indicated that walking speed was reduced during downwards step transitioning, supporting the notion that it was a more mechanically complex task than level walking 8 and similar to stair ascent. 12 As walking speed is considered a good indicator of physical mobility, the mechanical challenge of descending steps is emphasised by a slowing down. 13
Few published studies report speed during stair descent in lower limb amputees. Torburn et al. 14 reported that transtibial amputees descended stairs at a rate of 1.6 stairs/s. Powers et al. 13 and Ramstrand and Nilsson 15 reported average velocities of 29.6 m/min (0.49 m/s) and 0.48 m/s, respectively, for their transtibial amputees. More recently, Wolf et al. 16 reported stair descent speeds of 0.42 and 0.45 m/s for transfemoral amputees using a Power Knee and C-Leg, respectively. In this study, the amputee fallers walked more than 0.2 m/s faster than in these previous studies,13,15 whereas the non-fallers’ speeds were virtually the same as reported for other transtibial amputees.13,15
In accordance with our expectations, the fallers descended more quickly than the non-fallers. The current findings suggest the fallers may have put themselves at risk of falling by descending at higher speeds. Walking speed has been used as an overall indicator of function. 17 Descending more quickly may imply higher functioning, as faster speeds often require sufficient joint ROM and eccentric muscle strength. However, in the absence of adequate lower limb musculoskeletal strength and flexibility, amputees may in fact be placing themselves at risk of a prospective fall. It is surprising that the fallers descended steps at speeds faster than those reported for other transtibial amputees given that some of their previous falls in the 9-month period before testing actually occurred during stair negotiation. It is possible that the fallers had high self-efficacy beliefs and perceived their locomotor ability to be sufficient to ambulate quickly under familiar circumstances, such as descending a short staircase. Consequently, they evaluated this task as relatively low-risk. Conversely, the weaker or more cautious amputees were likely to have altered perceptions of risk and negotiated uncertain situations more slowly in an attempt to avoid a fall. Thus, fear of falling is an important consideration when addressing falls-related issues. It is possible the non-fallers were actually more fearful of a prospective fall than the previous fallers, as fear of falling has been associated with slower speeds. 18 Moreover, two of the five non-fallers were women, which may have influenced fear of falling, as women report greater fear than men. 19 Future work investigating biomechanical differences in fallers versus non-fallers should include information about participants’ fear of falling to provide a more holistic overview.
One strategy for improved dynamic stability during stair negotiation is handrail use, as has been advocated in other stair studies with older (able-bodied) adults. 20 Reeves et al. 20 demonstrated that handrail use could redistribute some of the work onto the arms and partially unload the legs, thereby reducing the demands on the knee extensors. In this study, the fallers only used the handrails ‘lightly’, as a guide for one hand. Given their faster walking speed, using the handrail on both sides (if available) would enhance dynamic control of balance on the affected and intact sides. Handrail use would also benefit amputees using the more complex ‘roll-over’ technique. This technique involves placing the midfoot over the nose of the step and rolling over the edge while in single support (also known as controlled lowering). It is useful with reduced joint mobility at the ankle and knee on the affected side. In this study, the fallers tended to use a ‘roll-over’ technique, similar to that reported in transfemoral amputees. 10 In any case, we advocate handrail use at all times for better dynamic control.
Joint kinematics
We predicted that joint mobility reflected in the lower limb joint angles at specific instances, and overall ROM would be different between the fallers and non-fallers for the affected limb. The ankle joint plays a crucial role during weight acceptance, demanding eccentric control by the ankle plantar flexors when initial contact is made, typically with the forefoot. Ankle plantar flexion assists in lengthening the leg in preparation for contact with the step below. This facilitates smoother movement of the centre of mass (CoM) in the vertical and horizontal directions. In the absence of active plantar flexion with the prosthetic foot, compensations are likely to occur proximally at the hip and pelvis. Previous studies investigating stair descent in amputees have not specifically examined pelvic hike or drop.10,11,13,14 In this study, both fallers and non-fallers showed exaggerated pelvic ROM in the frontal plane when compared to young and older able-bodied adults completing the same task. 21 Increased frontal plane hip and pelvic motion has been related to lack of neuromuscular control in able-bodied older adults and weakness in the hip abductor musculature. A large internal hip abductor moment is required to control the amount of hip adduction in late stance. 21 Increased frontal plane motion around the hip suggests proximal compensations were not solely due to insufficiencies of the prosthetic foot and ankle, but also muscle weakness around the hip. Therefore, increased strength of the hip abductors could also help to improve dynamic control when descending steps.
Peak ankle joint kinematics were similar to those reported by Powers et al. 13 for transtibial amputees. Peak dorsiflexion in stance was limited by the prosthetic ankle. Knee flexion could have been inhibited as socket fit tends to be high posteriorly. 22 The non-fallers showed a tendency to ‘throw’ their prosthetic foot down onto the next step compared to the fallers. This was evident with more hip flexion at toe off and throughout swing, thus lifting the whole leg into the air for stair clearance. Similar observations were reported in transtibial amputees when crossing obstacles with their prosthesis as the lead limb. 22
At the knee, the only noteworthy kinematic difference between the groups was smaller knee ROM on the affected side in the non-fallers (78.8 ± 4.1°) compared to the fallers (86.9 ± 7.5°). This reflected a combination of greater knee flexion at initial contact (because the limb was being ‘thrown’ over the step) and possibly differences in prosthetic socket fit restricting peak flexion.
There were larger differences when hip kinematics were examined. The hip joint on the affected side was fully extended in stance (−0.7 ± 2.9°) for the fallers and displayed larger ROM compared to the non-fallers. This was related to the fact that the affected limb was measured from the first (middle) step to the floor. Initiating and terminating the gait cycle with toe off meant that the stance phase of the affected limb was analysed when the foot was already on the ground and about to start level walking. Peak hip extension has been linked with walking speed, with greater hip extension observed at faster speeds. 23 As the fallers stepped more quickly downwards and also during level walking, 8 it is likely they would have extended their hip more in pre-swing prior to toe off.
Step-to group
To date, no studies have revealed a step-to gait strategy in lower limb amputees descending stairs. Our previous work has shown that this strategy is not unique to stair descent, as two of the same participants who used a step-to strategy during descent also exhibited the same strategies during ascent. 12 The step-to groups most likely adopted this gait strategy because of functional and strength limitations at the knee of both limbs. The time spent in single support on the affected limb was reduced and the knee was maintained almost completely extended. The controlled lowering phase, the most vulnerable phase during stair descent, was substantially shorter for the intact (trail) limb and virtually absent for the affected (lead) limb as the knee was maintained in an extended position.
In this study, 9 out of 11 amputees led with their affected limb on all occasions, while 2 participants showed no clear preference. It is plausible that the reduced space on the top landing, which limited the number of steps that could be taken prior to descending, prompted participants to lead with their affected limb. This may have introduced a limb preference bias. However, transtibial amputees frequently are taught to lead with their prosthesis/affected limb during stair descent, and so, we believe the limb preference was representative of typical stair walking. This is because the trail limb must flex at the knee to ensure safe lowering during the controlled lowering phase (lead limb swing phase, trial limb single support phase) and move through a greater knee ROM. Depending on prosthetic fit, the height of the prosthetic socket behind the knee could limit joint flexion. Although modifiable, if prosthetic socket fit was limiting knee ROM, particularly flexion, then that could have had a detrimental effect on stair locomotion.
The main distinguishing characteristics between the fallers and non-fallers was reduced ROM at the ankle and knee joints. Although reduced joint mobility was a characteristic of the step-to gait strategy, a certain ROM would still be necessary to negotiate stair descent and transition downwards on steps safely. The inability to achieve this may be considered a risk factor for falling. Exercise programmes aimed at improving knee extensor eccentric strength and knee joint mobility on the affected side, in those individuals adopting the step-to gait strategy, would be encouraged.
Some limitations of this study must be acknowledged. By using a three-step staircase, as has been done previously, 24 the gait cycle inevitably involves a component of level walking and thus represents more of a step transition. However, this is representative of real life, and the transition from steps to level walking warrants study as it may present an increased falls risk compared to level or continuous stair walking. 25 As the participants chose to lead with their affected limb, it meant this limb was the first to reach the ground. We did not deem it safe enough to ask participants to lead with their intact limb expressly, given their affected limb preference and falls history on stairs. Thus, no true controlled lowering phase on the affected side could be analysed. Although speed has been shown to influence kinematic parameters, such as ROM and peak joint angles, 23 it was not controlled for in this study. This was to allow participants to descend stairs using their most natural gait pattern, but also to ensure their safety during a more complex task. The small participant numbers also made it difficult to generalise the findings to the wider amputee population, while the reduced sample size made statistical analyses problematic. Achieving adequate participant numbers, while accounting for the variability that amputee fallers and non-fallers can present with, is a complex task. Finally, it was not possible to differentiate between cause and effect, and it remains unclear whether the fallers’ gait patterns contributed to their falls history or whether the consequence of falling resulted in modified gait patterns.
Conclusion
This biomechanical analysis in amputee fallers versus non-fallers provided some initial evidence that these two groups adopted different strategies during downwards step transitioning. In agreement with our predictions, the fallers walked faster than the non-fallers and exhibited larger ROM in the lower limb joints on the affected leg in the reciprocal groups. Notably, the non-fallers appeared to ‘throw’ their prosthesis over the edge of the step, while the fallers employed the more difficult ‘roll-over’ technique, requiring adequate strength and control of the knee extensor musculature. More participants adopted a step-to gait strategy in stair descent than ascent and this reduced the demands on joint mobility and muscle strength. The vulnerable controlled lowering phase was missing on the affected limb for the step-to group.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Conflict of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit.