
Abstract
Background:
There are currently no national competency standards upon which to develop educational objectives for prosthetist/orthotists in Sweden. While standards have been developed in other countries, they cannot be applied without confirming their relevance in a Swedish context.
Objectives:
To describe and obtain consensus on core competencies required for newly graduated prosthetist/orthotists in Sweden.
Study design:
Modified Delphi process.
Methods:
A modified Delphi technique was carried out. Focus groups were initially used to identify core competency domains. Two consecutive questionnaires, containing a list of potential competency items, were sent to a group of stakeholders with ties to the prosthetic and orthotic profession. Stakeholders were requested to rate their level of agreement with each competency item and provide written comments. Finally, two focus groups were conducted to obtain feedback on the draft competency standards.
Results:
Forty-four competency items, listed under five key domains of practice, were identified as essential for newly graduated prosthetist/orthotists in Sweden.
Conclusions:
Many similarities exist in core competency descriptions for prosthetist/orthotists in Sweden when compared to other countries. Regional differences do however exist, and it is important to confirm the relevance of core competency items at a national level before they are applied.
Clinical relevance
Competency standards developed in this study can be used to guide development of learning objectives within an undergraduate prosthetic and orthotic program, provide a framework for workforce development, assist professional organizations in understanding the needs of their members, and prepare for international accreditation.
Background
Clinical competence is a dynamic concept which requires much more than just knowledge. It also requires an understanding of concepts, clinical skills, interpersonal skills, technical skills, problem-solving abilities, and clinical judgment. 1 Competency-based education serves as a framework for focusing learning on the competencies required of health professionals to deliver high-quality care. Within a competency-based framework, performance characteristics are defined by stakeholders and competencies that reflect stakeholder needs are used to guide curriculum development and assessment. 2 One of the recurring concepts in competency-based education is the need to predefine the competency standards required of graduates and to ensure that they are aligned to the outcomes of the training program. 3
Traditionally, objectives for prosthetics and orthotics education programs have tended to focus on a legacy curriculum, modified over time by faculty “experts.” 4 A risk of this approach is that the emphasis of programs becomes knowledge acquisition and assessment of curricula content without regard to the current core competencies that are required to work in the professional environment. While knowledge is an important component of competence for prosthetist/orthotists, so too are the skills, attitudes, and judgment required to work in professional practice. 2
An international comparison of prosthetic and orthotic education programs has identified many course objectives which are common across institutions. 4 Common objectives generally relate to the need for knowledge in the fields of medical and engineering sciences. Several regional differences in course objective have, however, been identified. Examples include objectives related to clinical reasoning, integration of theory into practice, and critical thinking. 4 Regional differences also exist in the priorities given to various teaching methods by prosthetic and orthotic educational institutions. 5
It is possible that international differences in course objective and teaching methods within prosthetic and orthotic programs are a consequence of regional work practices, cultural variations, and national healthcare systems. Recognition of these regional variations is subsequently essential for development of educational programs which are relevant in meeting the needs of clients within a specific region and suggest that it may be necessary to confirm the relevance of professional competencies at a national level.
A number of national associations have published professional profiles6,7 or core competencies8,9 required for entry into the prosthetic and orthotic profession. Unfortunately, in many cases, details regarding the process by which they were developed are not readily available in the published material. In an evidence-based approach to generate core competencies of prosthetist/orthotists, Ash et al. 10 utilized a mixed-methods research design to develop and perform a content validation of professional competency standards for Australian prosthetist/orthotists. Based upon this work, the Australian Orthotics and Prosthetics Association (AOPA) has subsequently published its competency standards with six overarching domains. 9
Prosthetist/orthotists in Sweden are licensed to practice by the National Board of Health and Welfare. The education of clinicians is also accredited by the Swedish Higher Education Authority. The 3-year bachelor-level education for prosthetist/orthotists is the largest in Scandinavia and, in addition to Swedish students, educates students from Denmark and Iceland. At the time this study was initiated, the prosthetics and orthotics program was undergoing a full re-structure and re-development of its curriculum. Given that there were no national competency standards available, it was decided that these would need to be developed to ensure that the new prosthetics and orthotics program was relevant and would meet the future needs of the profession.
The aim of the present study was to describe and obtain consensus on core competencies required of prosthetic and orthotic graduates in Sweden. These competencies will be used to guide development of learning outcomes for the education of prosthetist/orthotists within the region.
Method
A modified Delphi technique, comprising of four stages, was used to obtain opinions from stakeholders with a professional interest in prosthetics and orthotics. The Delphi technique utilizes an iterative multistage process to draw upon the collective knowledge and opinions of experts and to arrive at a collective decision regarding subject matter of interest. 11
In stage 1, questionnaire development, we undertook a literature review to identify available professional profile and competency descriptions related to prosthetics and orthotics. These documents were distributed for review, and then discussed, by participants in two face-to-face focus groups. Purposive sampling was used to identify participants for each focus group. Focus group 1 (n = 7) included clinical prosthetist/orthotists (n = 3), a manager of a prosthetic and orthotic clinic (n = 1), students from the final year of the Swedish prosthetics and orthotics program (n = 2), and a physiotherapist with extensive experience working alongside prosthetist/orthotists (n = 1). Focus group 2 comprised of prosthetist/orthotists working within research and/or education (n = 6). During focus group sessions, existing competency and professional profile descriptions of prosthetist/orthotists were discussed and key competency domains were identified and agreed upon.
Following focus group sessions, an initial questionnaire was developed listing 73 potential competency items relevant to each of the domains generated by focus group participants. A small pilot study of the questionnaire was conducted with five certified prosthetist/orthotists and minor modifications were made.
Stage 2 involved seeking the opinion of a larger group of stakeholders. Once again, purposive sampling was used. An e-mail was sent to 45 possible participants, informing them of the study, how much time would be required, and what the results would be used for. An attempt was made to ensure that individuals invited to participate in the study represented the demographic of the profession. As no data were available to ensure this was the case, the selection of individuals was based upon the opinion of the authors who have detailed knowledge of the prosthetics and orthotics profession in Sweden. Forty-one individuals agreed to participate. Included in the sample were prosthetist/orthotists representing clinical practice, sales, manufacturing and research, employers of prosthetist/orthotists, and individuals from other professional groups with an intimate knowledge of the profession (physiotherapist, occupational therapy, engineering). The decision to include individuals representing other professional groups was made to identify competencies that individuals from related field considered desirable in prosthetist/orthotists. Participants represented both private and public facilities, four different countries typically serviced by graduates from the Swedish educational program, and two individuals who were educated as prosthetist/orthotists but who have since left the profession.
The questionnaire was distributed electronically using EsMaker software (Entergate AB) accessed via a personal link which was sent to the participants’ e-mail address. When completing the questionnaire, participants were requested to consider the competencies required of newly graduated prosthetist/orthotists and to indicate their level of agreement with each competency item on a 5-point Likert-type scale (1 = completely disagree; 5 = completely agree). Within the context of this study, the term “newly graduated” was used to refer to individuals who had completed their bachelor’s level education in prosthetics and orthotics and are subsequently eligible, by law, to practice independently as a prosthetist/orthotist. Questions related to each domain were included on separate pages and an open-ended question was included after each domain requesting that participants document their thoughts and/or indicate any items that were unclear. A reminder to complete the survey was sent after 2 weeks.
In the absence of a universally agreed proportion to determine the level of consensus in Delphi studies, 11 consensus was considered to be reached if 75% of participants rated a competency item as 4 or 5 on the Likert-type scale.
For stage 3, results from stage 2 were compiled and modifications made to the questionnaire on the basis of comments provided by participants. Participants who responded to the initial questionnaire were requested to complete the modified version via a personal e-mail containing a link to the survey. Once again, a reminder to complete the questionnaire was sent after 2 weeks.
In the final stage of the study, stage 4, competency items that achieved consensus were presented in face-to-face sessions with members of the original two focus groups. Five individuals participated in focus group 1 while four individuals participated in focus group 2. During these focus group sessions, comment was sought, and recommendations made to improve clarity of the competency items and presentation of results.
This study does not fall under Swedish law for ethical approval. Questionnaires were sent to each participant separately to protect their anonymity. Consent was considered to be granted when participants actively chose to return the survey.
Results
Figure 1 presents a flowchart representing stages of the Delphi process. Six competency domains describing the general areas of practice for prosthetist/orthotists were identified during the initial focus groups and the 73 competency items rated in this stage were distributed across all six domains (see Table 1).
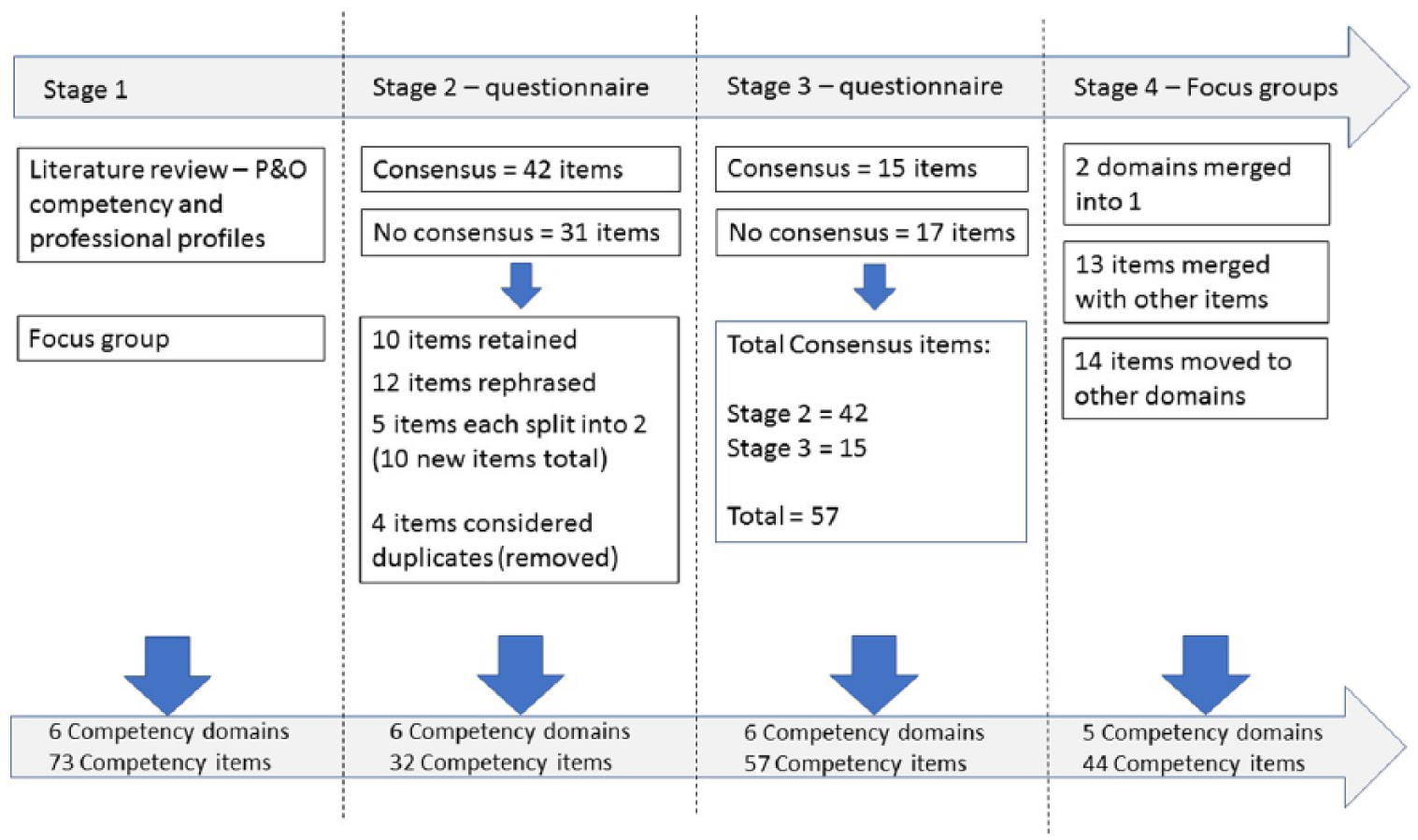
Flowchart of Delphi process.
Initial competency domains, number of items included in each domain, and number of items in which an agreement level of 75% or more was reached.
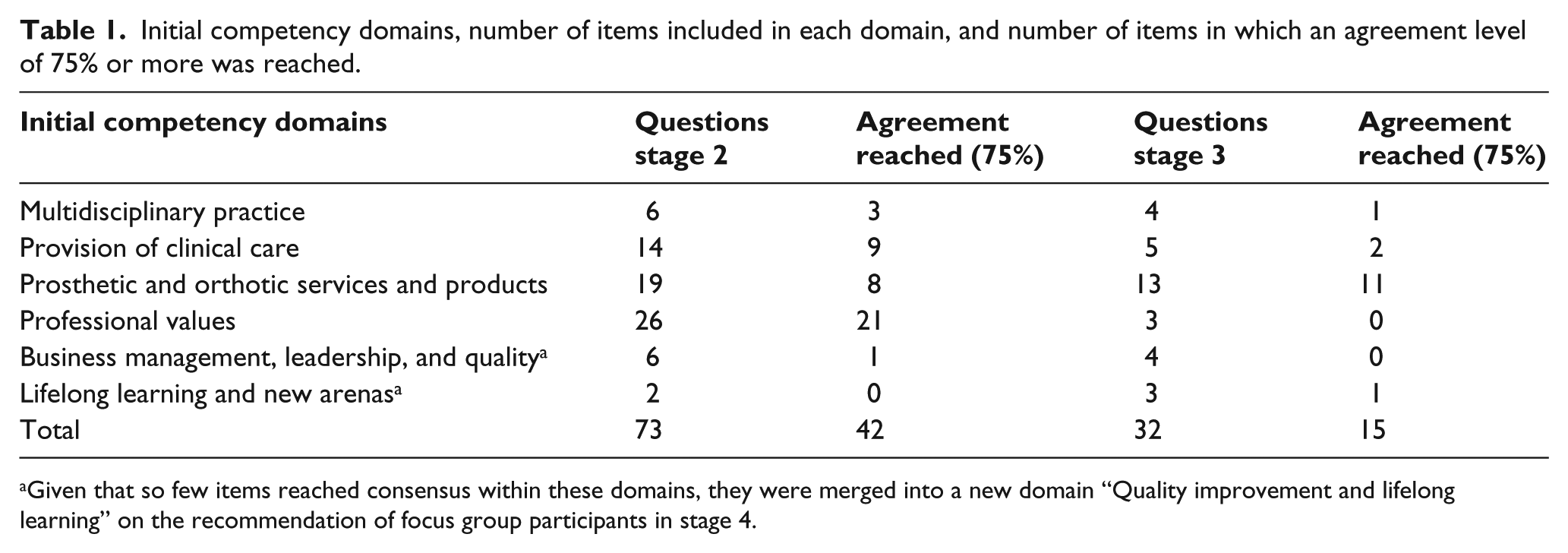
Given that so few items reached consensus within these domains, they were merged into a new domain “Quality improvement and lifelong learning” on the recommendation of focus group participants in stage 4.
Stage 2 was conducted in May 2017. Thirty-five persons responded (response rate 85%) and consensus was achieved on 42 competency items.
The questionnaire was modified for stage 3. The modified questionnaire only included competency items that did not reach consensus during stage 2. Several items were re-phrased or divided into two new items on the basis of written comments received during stage 2, while other items were considered as duplicates and subsequently removed (see Figure 1). The modified questionnaire contained 32 competency items to be rated. The same Likert-type scale was used. Prior to completing the modified questionnaire, participants received a summary of all results from stage 2, including all competencies in which agreement was reached. They were also made aware that the competency items they were about to rate had not achieved consensus during the initial phase of the study.
The modified questionnaire (stage 3) was distributed in August 2017 to all persons who responded in stage 2 (n = 35). A total of 28 individuals responded (response rate 80%). Consensus was reached on an additional 15 items.
Competency items that achieved consensus during stages 2 and 3 were presented to members of the original two focus groups for discussion in stage 4 (October 2017). Based upon these discussions, a recommendation was made to merge the two domains, “Business management, leadership, and quality” and “Lifelong learning and new arenas,” and create a new domain titled “Quality improvement and lifelong learning.” Participants also indicated that the results would be easier to communicate by reducing the total number of items and combining items with a similar focus. They also recommended that some items be moved to another domain and that a footnote be added to indicate the expectation that evidence-based practice is applied to all relevant competencies. Table 2 presents an overview of all consensus items following edits made on the recommendation of focus groups in stage 4.
Competency items reaching agreement of 75% or more.
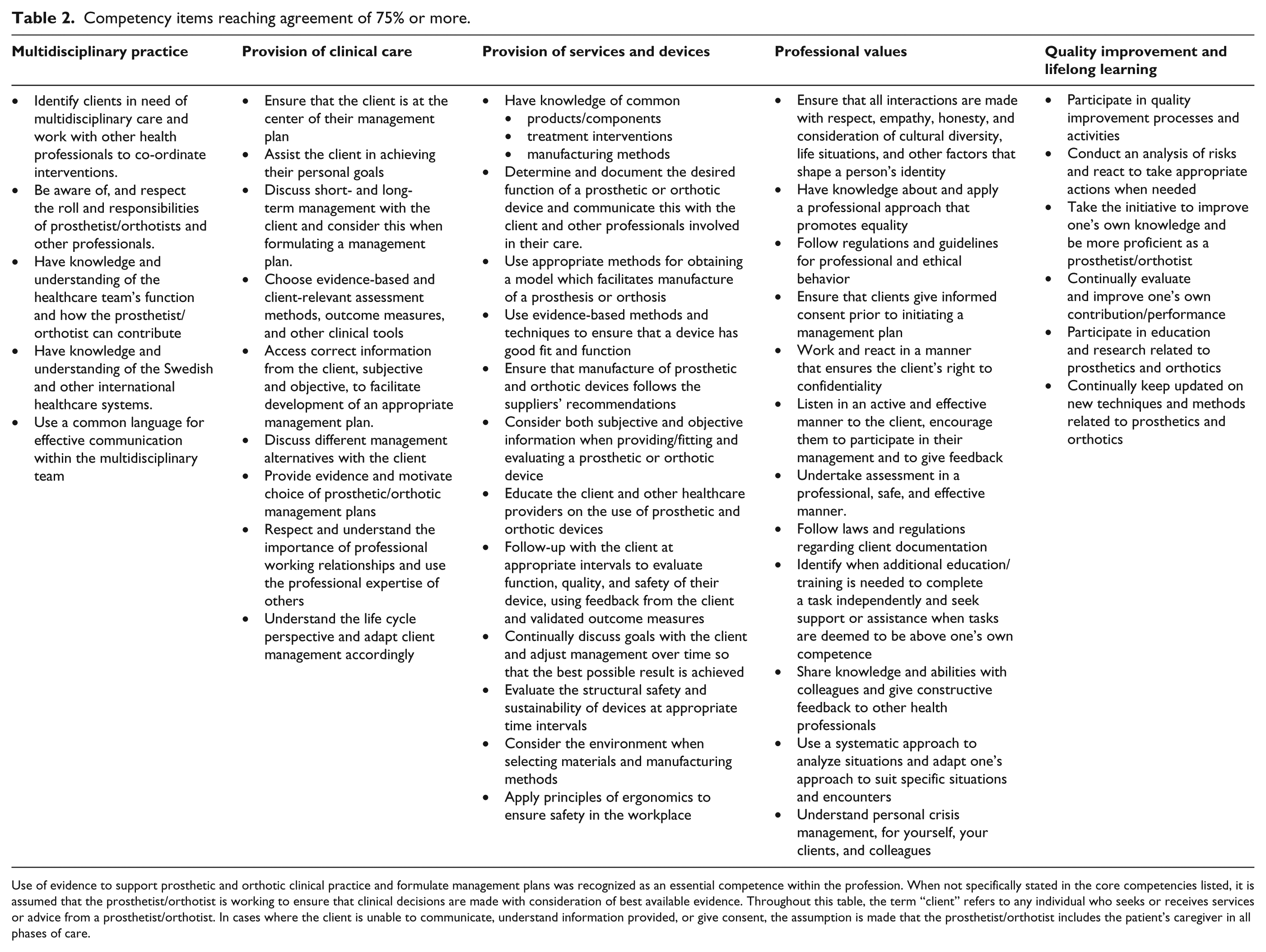
Use of evidence to support prosthetic and orthotic clinical practice and formulate management plans was recognized as an essential competence within the profession. When not specifically stated in the core competencies listed, it is assumed that the prosthetist/orthotist is working to ensure that clinical decisions are made with consideration of best available evidence. Throughout this table, the term “client” refers to any individual who seeks or receives services or advice from a prosthetist/orthotist. In cases where the client is unable to communicate, understand information provided, or give consent, the assumption is made that the prosthetist/orthotist includes the patient’s caregiver in all phases of care.
Discussion
Forty-four competency items, listed under five key domains of practice, have been identified as essential for newly graduated prosthetist/orthotists in Sweden. These competencies incorporate not just the knowledge required to work as a clinical prosthetist/orthotist but also the performance characteristics, attitudes, and judgments necessary to provide quality care. While the primary purpose of this study was to develop core competencies to guide development of learning objectives within an undergraduate prosthetic and orthotic program, results can be considered as a profession validated list of competencies and can also be used to provide a framework for workforce development, to assist professional organizations to better understand the needs of their members and to prepare for accreditation.
As expected, there were many similarities between the competency items generated in this study and those published by other groups.6–9,12 Close similarities can be attributed to common clinical practices that are not specific to a particular region, but also to the fact that these existing documents were identified as part of the literature review in the beginning of this study and subsequently used by focus groups to determine competency domains relevant in the Swedish context. Interestingly, there were a number of items that appear in competency and scope of practice documents from other countries that were not considered as essential for newly graduated prosthetist/orthotist in Sweden. These related specifically to service management, promoting the profession and supervision of others. Competencies related to quality improvement and evidence-based practice were considered essential in the Swedish context but the extent to which they are lifted in other competency or scope of practice documents varies considerably.
Competencies related to service management and promoting the profession were not prioritized by participants included in this study. Written comments in the questionnaire suggested that management skills were considered as post-graduate competencies, while competencies related to promotion of the profession were simply not considered as essential. Promotion of the profession as a competency item is prevalent in many of the international documents that were reviewed.6,7,12 The fact that this is not prioritized in Sweden is likely due to the structure of the healthcare system. In Sweden, fixed term contracts are awarded for the provision of prosthetic and orthotic services and, in most regions, beyond the contract tender process, there is little competition for service delivery.
The International Society for Prosthetics and Orthotics (ISPO) education standards describe one of the roles of professional prosthetist/orthotists as supervision or mentoring of associate professionals and technicians. 13 The British standards for best practice indicate that prosthetist/orthotists should delegate and supervise the activity of others, and stipulate that this is dependent upon career position. 6 The supervisory role of clinicians is not included in the Canadian scope of practice 7 or the Australian competency standards, 9 while the American board of Certification makes reference to “supervision of the provision of care” with no mention of who or what should be supervised. 12 While items related to leadership, allocation of work tasks to others, and coordination of manufacturing were included in the present questionnaire, these items did not reach consensus. As implied by the British standards, it is likely that the level to which prosthetist/orthotists in Sweden supervise and delegate work to others is dependent upon experience. As such, results from this study suggest that learning outcomes to facilitate these competencies should not form part of the undergraduate prosthetics and orthotics curriculum and it would be more appropriately dealt with at the post-graduate level.
Agreement on competencies related to evidence-based practice was evident throughout the questionnaire, so much so that the focus group members participating in stage 4 suggested that it should be lifted in a separate body of text. This suggests a positive cultural change that has occurred within the profession. 14 Use of evidence is given varied levels of attention in other competency and scope of practice documents. A high level of attention is provided in British and Australian documents6,9 while it is mentioned but briefly in the American and Canadian documentation.7,12
Participation in quality improvement processes and activities, as well as risk analysis were competency items that were considered important in the Swedish context. Similar items are mentioned under the domain “Service management and improvement” in the Australian competency standards and under “professional roles” in the British Association of Prosthetists and Orthotists (BAPO) standards for practice. No mention of competencies related to quality improvement processes or risk management are made in the American Board of Certification Scope of practice, 12 Canadian scope of practice, 7 or in the new ISPO professional profile. 13
Limitations
One of the criticisms of the Delphi technique is that participants are heavily influenced by their own experiences and working situation and may not be able to see the vision or the big picture. Although efforts were made in this study to include diversity of thought related to prosthetic and orthotic practice, it should be recognized that the core competencies presented in this study are based upon current thinking and practice within prosthetics and orthotics in Sweden. It is also important to note that there is only one educational institution offering a prosthetics and orthotics program in Sweden and that most participants in this study are graduates from this school. While an educational program designed to meet the needs of the profession must address competencies presented in this study, it is important for educational institutions to also identify and address future needs and opportunities which may not have been identified using the Delphi method.
This study was conducted with a primary focus on the Swedish prosthetic and orthotic profession. As the educational institution in Sweden also educates clinicians for Denmark and Iceland, participants from these two countries were included and results are likely to be generalisible to these regions. Additional research is however required to determine generalizability of results to other regions. It should also be recognized that the opinions of clients and care givers were not specifically sought in this study and the results cannot not be assumed to include the views of these groups.
Conclusion
This Delphi study has allowed stakeholders in prosthetics and orthotics to define and agree upon a set of competencies for the prosthetics and orthotics profession in Sweden. It represents an initial step toward developing a prosthetics and orthotics curriculum designed to meet the needs of stakeholders. While many core competencies were similar to competency descriptions and scope of practice documents produced in other countries, regional differences were also identified suggesting the importance of confirming core competency documents at a national level.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.