
Abstract
Background:
The microprocessor-controlled foot Meridium is a prosthetic component with adjustable stance-phase characteristics.
Objectives:
To investigate subjects’ and prosthetists’ perception of safety, walking, and satisfaction during first routine fittings.
Study design:
Multicenter, prospective, observational cohort study.
Methods:
Data regarding demographics, fitting process, safety, daily life activities, and satisfaction were obtained through questionnaires. The follow-up period was 7 months.
Results:
In all, 89% of 70 users were satisfactorily fitted within the first two visits. Compared to previous feet, users reported improvements in walking on level ground (54% of subjects), uneven ground (82%), ascending (97%), and descending ramps (91%). More than 45% of the users perceived an improvement in safety and stability while standing and walking. No difference was observed in concentration, exertion, and pain. Overall user satisfaction with Meridium was 50% and the foot was preferred by 40% of users. Amputation level, age and mobility grade did not influence subjects’ preference. Prosthetists recommended Meridium for 59% of subjects. A correlation analysis revealed that transfemoral amputees fitted with Genium and/or having a long residual limb strongly preferred Meridium (p < 0.05).
Conclusion:
Meridium was appreciated by amputees with a preference for natural walking and requirement to safely and comfortably negotiate uneven terrain and slopes.
Clinical relevance
Amputees preferring Meridium perceive benefits with safe, comfortable, and natural walking. While the perception of benefits regarding the negotiation of uneven terrain and slopes is very high, the correlation to product preference is moderate. Individual assessment and trial fitting might be essential to identify patients who benefit greatly.
Background
Microprocessor-controlled feet (MPF) became available for lower limb amputees over a decade ago. MPF may be divided into two main categories: MPF that control the dorsi- and plantar flexion position of the foot and MPF where the ankle moves through a controlled range of motion with every step. Different algorithms support sequential or real-time adaptation. This study refers to non-powered systems. MPF are associated with some biomechanical and clinical advantages. The adaptation to a dorsiflexion position during swing is associated with increase in toe clearance and implies a reduction in stumbles and falls.1,2 The controlled range of motion during stance is associated with improvement in loading response due to a decrease in rollover resistance, increase in self-selected walking speed and reduction in peak socket pressures associated with a more steady loading of the soft tissue.3–5 Prominent improvements are associated with amputee ambulation on uneven terrain, ramps, and stairs. The ability of the foot to adapt to inclines may improve gait symmetry and reduce compensation strategies.6,7 Reduction of energy consumption and perceived exertion have also been reported.8,9 This is remarkable as MPF are associated with increased weight and - compromise on energy return. It is noteworthy that differences to rigid ankle feet are often derived from biomechanical investigations, while clinical measures do not seem to detect substantial differences. 10
This work describes an innovative MPF Meridium (Otto Bock Healthcare Products GmbH, Austria, Figure 1). The hydraulic plantar flexion and dorsiflexion resistances are controlled using sensor information on ankle angle and ankle angular velocity, ankle torque, and the position and movement of the foot in space. Energy storage and return is supported by an ankle spring, 11 while a carbon heel spring determines heel strike dampening. A four-axes geometry and articulating toe plate supports energy return, reduction of rollover resistance and increases the symmetry of the center of mass movement (Lang M, personal communication, 2016). Depending on the user’s individual dorsiflexion resistance settings, Meridium provides an extended dorsiflexion of up to 10° for rollover. In late stance, the four-axes geometry causes a 5° plantar flexion supporting push-off. The systems remain in up to 5° of dorsiflexion in swing that enhances toe clearance and dampens the following heel contact. The total range of motion is 36°. A heel height adaptation of up to 50 mm is claimed by the manufacturer for use with different shoes. 12 The foot weight is specified as 1.5 kg. Altenburg et al. 13 and Ernst et al. 14 report a normalization of vertical ground reaction force distribution of the prosthetic and unaffected side during standing on inclines with Meridium and minimized posture compensations. Altenburg et al. 15 reported on the reduction of knee torque immediately following a change of the slope in the investigated obstacle course indicating the favorable influence of real-time adaptation.

Meridium.
The objective of this observational study was to investigate subjects’ and prosthetists’ perception of safety, walking, and satisfaction with Meridium during first trial fittings performed in clinical routine. A further objective of this study was to investigate how such perceived performance was related to subjects’ preference of Meridium. A characterization of subjects preferring Meridium, related to clinical factors, such as age, mobility grade, amputation level, and others, was attempted. The influence of usage duration on preference for Meridium was investigated. The investigation and subsequent analysis were exploratory.
Methods
Data from first routine trial fittings in a convenience sample of 86 subjects were retrieved in a prospective cohort design. Control was intra-individual comparative assessment with the existing prosthetic foot of the participants. First trial fittings began in November 2014 and all trials were completed by May 2015. Data were retrieved from 44 international prosthetic clinics. The use of the data followed respective national requirements including Institutional Review Board (IRB) approval according to 45 CFR 46.116(d) issued by the Western IRB for the United States.
Meridium is indicated for unilateral or bilateral transtibial, unilateral knee disarticulation and unilateral transfemoral amputees, classified as limited community ambulators (K2), unlimited community ambulators (K3), or highly active adult/athletes (K4) according to the Medicare Functional Classification Levels (MFCL). Users can have a maximum weight of 100 kg and a foot size between 24 and 29 cm. Users must fulfill the physical and mental requirements for perceiving optical/acoustic signals and/or mechanical vibrations. No contraindications are given by the manufacturer. 12
Data retrieved included information on baseline assessments, an interim follow-up (planned after 60 days of Meridium use), and at the end of the trial period (planned after 100 days of Meridium use):
Initial practitioner questionnaire—requesting information on user characteristics, current status of the subject, and the fitting process including the evaluation of adaptation time, the alignment, and the use of the control software.
Subject questionnaire—addressing and comparing usage of previous and Meridium fitting in daily life situations, including the evaluation of level ground, uneven ground ambulation and the rating of comfort, concentration needed when walking, exertion, safety, stability, and pain. Subjects were asked to which extent they were satisfied with Meridium and whether or not they would prefer Meridium.
Practitioner questionnaire—to provide information about the prosthetist’s satisfaction with Meridium and its fitting process including the prosthetists recommendation to the subject.
Subject and practitioner questionnaires were filled at interim and final participant’s visit. In the subject’s questionnaire, level ground ambulation at different walking speeds, uneven terrain ambulation, and ascend and descend of stairs and ramps were rated. Comfort was evaluated during walking, standing, and sitting. Pain was rated with respect to back pain and pain in the sound and in the residual limbs. Concentration and perceived exertion were rated during walking. Safety and stability were evaluated during standing and walking. Fear of falling and number of falls and stumbles during the observation period were recorded. Comparative evaluations were recorded on 5-point Likert scales indicating “much better with Meridium,” “better with Meridium,” “no difference with Meridium,” “worse with Meridium,” and “much worse with Meridium.” Questions regarding pain, concentration, and exertion used the terms “more” and “less.” Responders are classified as subjects who experienced “better” or “much better” performance with Meridium.
Descriptive analysis was performed with Microsoft WinSTAT and EXCEL on a de-identified data set. Missing entries were classified “n/a” and not used in the analysis.
A correlation analysis (Kendall’s tau) investigated the influence of perceived performance on subject’s satisfaction and preference with Meridium. Furthermore, correlation analysis was used to understand how factors such as age, etiology, mobility grade, amputation level, prosthetic knee, time since amputation, amputation level, accommodation time, time of daily use, walking capacity, number of falls or stumbles, and fear of falling influenced subjects’ preference. Correlation analyses were performed in SPSS. To analyze the influence of usage duration (hypothesized effects on performance (H1)) Wilcoxon–Mann–Whitney test was performed in SPSS. A usage duration of more or less than 70 days was chosen retrospectively to balance the user groups.
Results
Data on 86 subjects were retrieved: 56% (48 participants) interim at 54 ± 25 days; 62% (53 participants) at the final follow-up after 113 ± 51 days. A total of 31 data sets (36%) were complete. For 70 participants (81%), at least one patient questionnaire was completed. Therefore, data on 70 participants were used for analysis. No statistically significant differences were detected between interim and follow-up data for gender (p = 0.35), age (p = 0.42), weight (p = 0.95), mobility grade (p = 0.7), amputation side (p = 0.63), amputation level (p = 0.61), time since amputation (p = 0.98), or reason for amputation (p = 0.63). Average Meridium use was 106.3 ± 57.04 days. To investigate effects related to trial duration, stratification for time of use differentiated between those having worn Meridium for less than 70 (46 ± 15 days; 51% participants) and for more than 70 (136 ± 35 days; 49% participants).
Users were mostly male (77%) with a mean age of 45.6 ± 13.7 years. Mean time since amputation was 13.9 ± 13.6 years. Amputation levels were transtibial (64%) and transfemoral or knee disarticulation (36%). Mobility grades were K3 in 63% and K4 in 37%. Amputation etiology included trauma (66%), tumor (13%), vascular disease (13%), infection (5%), and congenital (3%). Prosthetic knees used were C-Leg (44%) and Genium (44%). Three subjects used other microprocessor knee joints (MPKs). Previous feet included carbon fiber feet (85%), MPF (7%), Solid Ankle Cushion Heel (SACH) feet (4%), Solid Ankle Flexible Endoskeletal (SAFE) feet (2%), and single-axis feet (2%). Distribution of the affected side was left in 60% and right in 40% of the subjects.
Satisfactory alignment was achieved for 55% of subjects during the first and for 34% during the second visit. For 11% of the subjects, a third visit was required. One-day acclimation period was reported by 37%, 2 days by 15%, 3–7 days by 31% and >7 days by 18% of the participants. The prosthetists rated the use of the adjustment software as “very easy” (32%), “easy” (47%), and “neutral” (20%). In 51% of the subjects, further parameter adjustments were performed after the initial fitting process. When Meridium was fitted in combination with an MPK, for 48% of the subjects, the parameters of the knee were also adjusted. Prosthetists commented that the fitting requires experience, but has not been judged as exceedingly challenging.
The results of subjects’ perception on task categories as indicated on in the Likert scales are displayed in Table 1.
Likert scale rating (%) for total population indicating comparison of Meridium to standard foot.
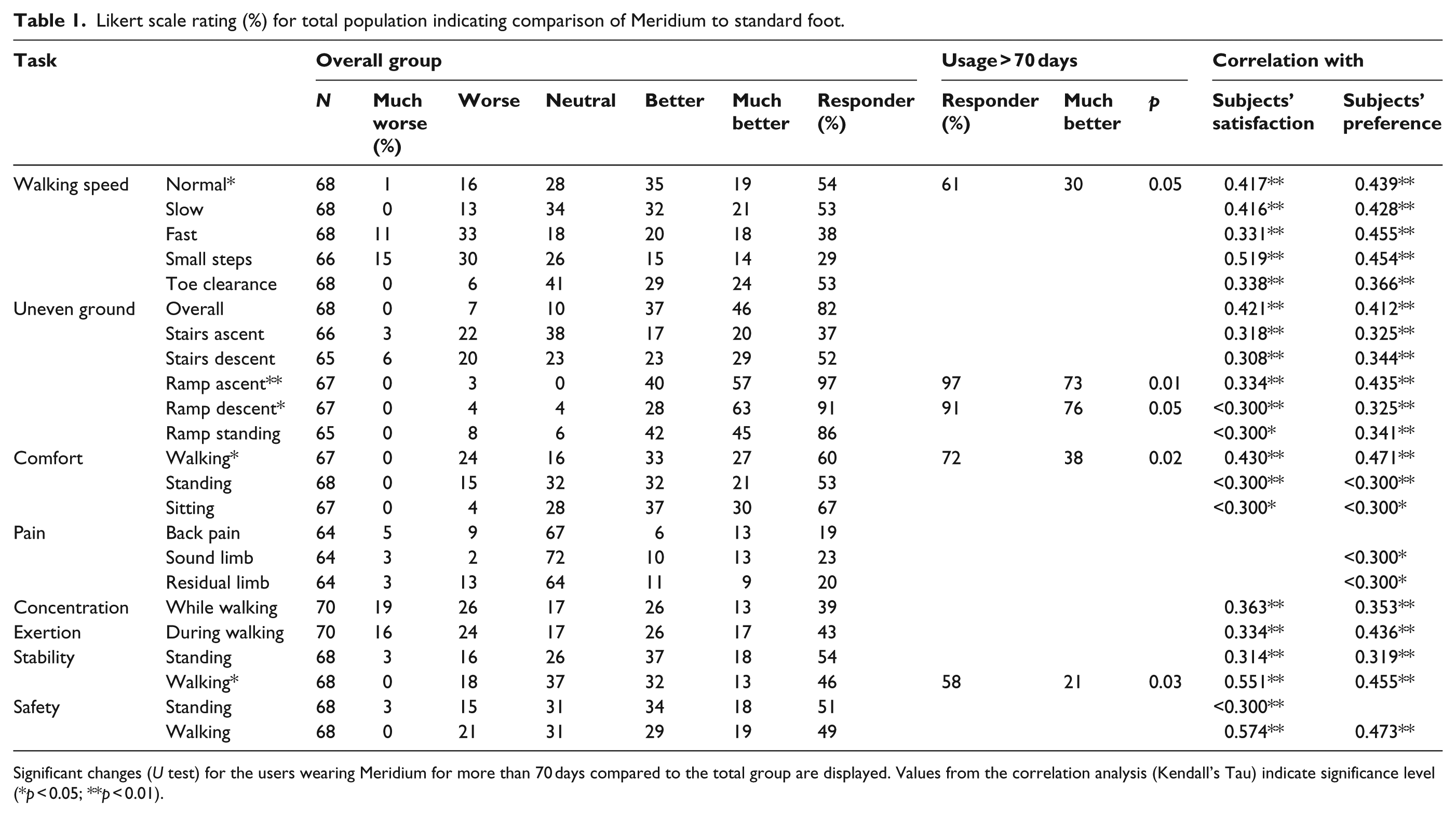
Significant changes (U test) for the users wearing Meridium for more than 70 days compared to the total group are displayed. Values from the correlation analysis (Kendall’s Tau) indicate significance level (*p < 0.05; **p < 0.01).
Improvements were reported in level walking (by 54% of subjects; Table 1), walking on uneven terrain (82%), ascending (97%), descending (91%), and standing on ramps (86%; Figure 2). Of the subjects, 53% preferred the toe clearance offered by Meridium. Ascending stairs with Meridium was favored by 37%, while descending stairs by 52% of users.
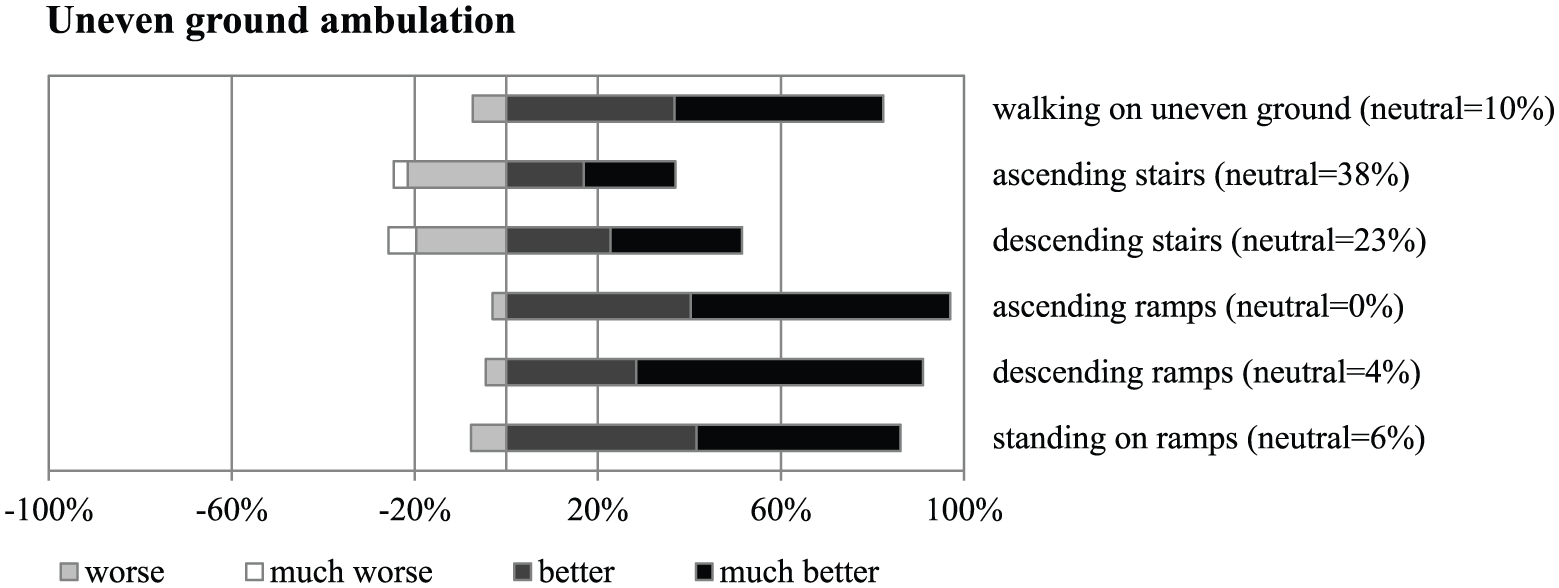
The Likert scale rating indicates the beneficial function of the real-time ankle flexion control of Meridium.
Walking, standing, and sitting were rated to be more comfortable with Meridium by 60%, 53%, and 67% of users, respectively. More than 45% of users perceived an increase in safety and stability during walking and standing (Table 1). No difference was observed regarding pain in either the residual or sound limb. There was also no difference in concentration and exertion during walking between the two prosthetic foot conditions (Figure 3).
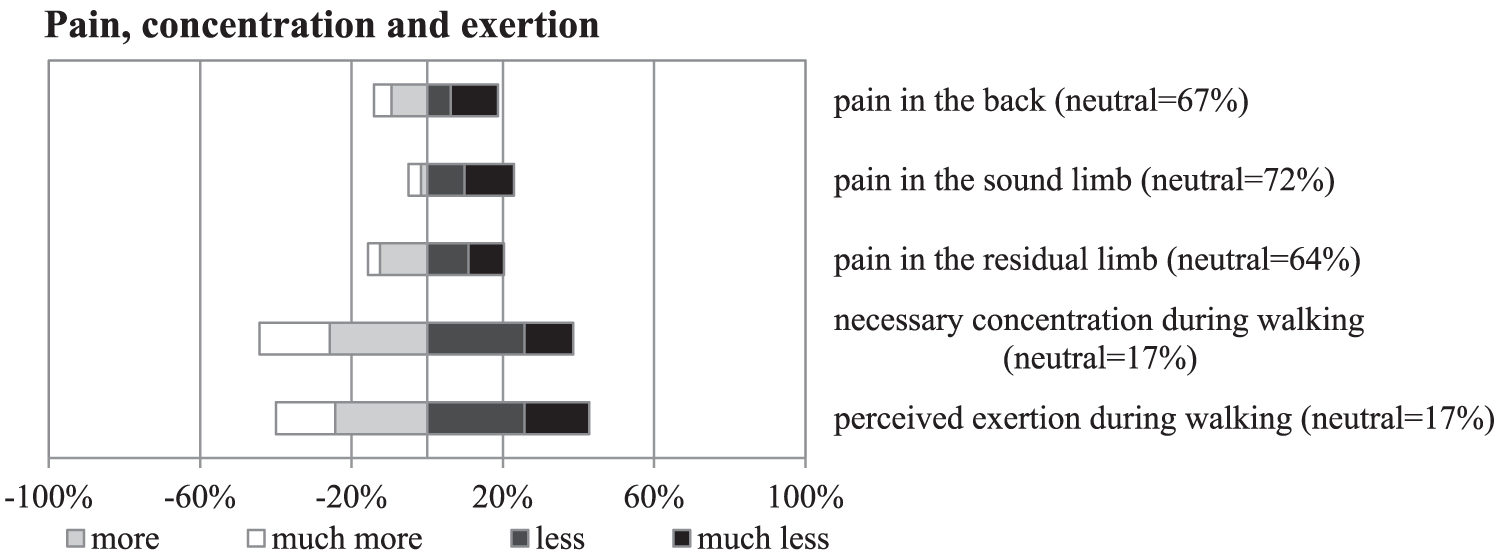
The Likert scale ratings for the categories “concentration” and “exertion” illustrate a polarized reaction to the trial, with very few neutral responses. Instead the subjects rather tend to have a clear perception. No difference was observed regarding pain in either the residual or sound limb or in back.
Of the subjects, 35% reported fewer stumbles, 32% reported no change, and 33% reported an increase in the number of stumbles with Meridium. While using Meridium, 23% of the participants reported fewer falls, 72% reported no difference, and 5% reported more falls.
In some categories, performance ratings are more positive for subjects using the Meridium for more than 70 days: when walking on level ground with normal walking speed, comfort while walking (p < 0.05), and ascending (p < 0.01) and descending ramps (p < 0.05, Table 1).
Overall user satisfaction with Meridium was 50%, and 40% would prefer Meridium over their previous foot. Prosthetists recommended the use of Meridium for 59% of subjects.
Dependence of user satisfaction and preference on task perception was investigated using correlation analysis. Moderate and higher correlations (τ > 0.3) are displayed. Subjects’ preference was strongly correlated to perceived safety during walking (τ = 0.473**), walking comfort (τ = 0.471**), walking stability (τ = 0.455**), fast walking speed (τ = 0.455**), walking with small steps (τ = 0.454**), walking on level ground (τ = 0.439**), and exertion during walking (τ = 0.436**). Statistical significance was high (**p < 0.01; *p < 0.05). Days of using Meridium during the trial were moderately correlated with preference (τ = 0.330**). The ratio of those preferring Meridium in the group using the device for more than 70 days was 50%.
Subjects’ preference was also investigated regarding the epidemiologic characteristics of the cohort using Meridium for longer than 70 days. Subjects’ preference strongly correlated with their overall satisfaction (τ = 0.653**). In this group, preference correlates with walking on level ground (0.570**), perceived safety during walking (0.513**), perceived exertion during walking (0.484**), stability during walking (0.442**), and toe clearance in swing phase (0.404*). Participants having longer residual limbs showed a higher preference toward Meridium (τ = 0.453**).
The preference in the group of above-knee (36%, 25 participants) amputees was 50%. Preference in those using Meridium for longer than 70 days was strongly correlated to the use of Genium (τ = 0.617*).
No correlation with users’ preference could be found for age, body mass index (BMI), mobility grade, time since amputation, amputation level (transtibial/transfemoral), accommodation time, time of daily use, walking capacity, number of falls or stumbles, and fear of falling.
Discussion
We analyzed first results concerning the practical use of the new MPF Meridium. Fitting process, alignment, and accommodation have been rated to suit the requirements of clinical routine by prosthetists and users. Responders perceive benefits compared to their previous foot when walking on level ground, uneven terrain, ramps, and stairs (Table 1). Specifically negotiating ramps is rated as being improved. This may be interpreted as a function of real-time adaptation as well as a wide range of motion. Also noteworthy is a favorable rating of standing on ramps, standing comfort, and standing stability. This is consistent with the report of biomechanical benefits of MPF compared to standard feet during stair ascent and ramp descent (but not stair descent and ramp ascent).6,7
Comfort during walking, standing, and sitting as well as stability during walking and standing are positively perceived. We attribute this to the real-time adaptation capability of the rotation resistances as well as the availability of a dorsiflexion stop to support the standing functions. We interpret these findings to be in agreement with results found by De Asha and colleagues3,4 and Wolf et al. 5
The influence of the foot on pain is marginal. A majority of subjects report “no change.” The ratings of perception of concentration and exertion were highly polarized, with only very few neutral ratings. The perception of exertion may be influenced by the tolerance of the foot weight. The observation may also indicate that energy return perhaps requires optimization. The perception of concentration may be influenced by the acceptance of adaptation of the gait pattern to real-time adaptation and by acclimation needs
A reduction in stumbles (33%) and falls (23%) was reported with Meridium. In all, 18% of amputees reported a decrease in the number of falls. A partial explanation for this may be the improvement in toe clearance that 53% of the subjects reported. These results are consistent with the work of Altenburg et al. 15 Rosenblatt et al. 16 related an increase in toe clearance with a decrease in likelihood of tripping over an unseen obstacle. Prosthetic-side minimum toe clearance was more than 50% lower for participants who had reported one or more trip-related stumbles on that side compared to participants who had reported no trip-related stumbles on the prosthetic side. 16
Correlation analysis reveals that subjects’ preference and satisfaction may mainly be influenced by the perception of safety and stability, level ground walking, and exertion. The correlation with the negotiation of ramps and stairs is of lesser magnitude. Meridium is constructed and perceived to prominently support the negotiation of ramps and uneven ground. Still, it seems that other factors may be more important when it comes to actually choosing the component. Interestingly enough, while the perception of exertion with Meridium exhibits very few neutral ratings, its correlation with preference is moderate.
Significant changes in improvements of the responder rate or responder distribution with time were found for normal walking, ramp ascent and descent, and walking stability. No reduction in rating was observed with time. We infer that while acclimation was rated by the prosthetists to be completed within a week, the above aspects may still improve over time. However, it is also to be noted that most perceptions did not change.
In the group of subjects with above-knee amputations, a strong correlation with use of the Genium knee was found. It seems that this specific combination is perceived as beneficial by the subjects. Swing-phase control and hydraulic friction are advanced in Genium. Furthermore, a pre-flexed position of 4° in the late swing phase further dampens the heel strike. The auto-adaptive control of stance flexion of the Genium knee may also contribute to this favorable finding. 17
No correlation with preference could be found for age, etiology, mobility grade, amputation level, and other epidemiologic factors. This compares well to other research with microprocessor-controlled components.18,19
Subjects’ preference strongly correlates with satisfaction. A clear responder profile could not be identified. Individual trial fittings will remain necessary. The perceived benefits in those who did prefer Meridium may justify the additional effort.
This observation of routine use spans a large number of prosthetic clinics. The responses were captured on Likert scales in clinical practice. The fact that the full range of rating scales offered was used indicates a high sensitivity with respect to the subjects studied. No ceiling or floor effects could be detected. While Likert scales themselves are validated instruments to measure perception, no instruments specifically validated for measuring clinical effects in exo-prosthetics were applied. The use of Likert scales only limits the applicability of this work to subjects’ perception. The use of other validated instruments would facilitate the interpretation of the clinical effects.
Routine assessments were conducted in a commercial environment. Therefore, we do have to consider bias. In a recent publication, bias in trial fittings was found not to exceed 10% and more likely to be significantly smaller. 18 Nevertheless, conducting a randomized controlled trial would minimize the bias associated with a cohort study.
Conclusion
First fittings with Meridium showed that users perceived benefits and prosthetist recommended the device. Alignment and the use of the software were rated appropriate for routine use. Meridium seems to be preferred by amputees with a preference for natural walking and the requirement of safely and comfortably negotiating uneven terrain and slopes. Subject’s preferences do not correlate with amputation level, age, and mobility grade. In transfemoral amputees, the use of Genium seems to significantly increase the perception of walking-related benefits offered by Meridium. Individual assessment and trial fittings seem to be essential to identify responders to the new foot.
Footnotes
Author contribution
Andreas Hahn contributed to the study design, described, interpreted, compared the study findings and contrasted them with the existing literature.
Ivana Sreckovic collected, analyzed and described the study findings.
Sebastian Reiter contributed to the study design and coordinated the study conduct.
Milana Mileusnic contributed to the study design and critically reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.