
Abstract
Background:
The two passive vacuum suspension systems currently available in total surface-bearing sockets are the hypobaric Iceross Seal-In® and the suction suspension system.
Objectives:
The purpose of this study was to compare the effect of the hypobaric Iceross Seal-In® liner with that of the suction suspension system for quality of life, pistoning, and prosthesis efficiency in unilateral transtibial amputees.
Study design:
Single-group repeated measures.
Methods:
Ten amputees were enrolled. The pistoning test, used to compare vertical movement of the stump within the socket, and the energy cost of walking test were carried out when the amputees were wearing the suction suspension system and after 2, 5, and 7 weeks of Seal-In® X5 use. The Prosthesis Evaluation Questionnaire and the Houghton Scale Questionnaire of perceived mobility and quality of life with the prosthesis, and the Timed Up&Go Test and the Locomotor Capability Index for functional mobility were also administered at the beginning and end of the study.
Results:
The hypobaric Iceross Seal-In® X5 led to significant pistoning reduction and improvement on the Houghton Scale Questionnaire and 3 of 9 domains of the Prosthesis Evaluation Questionnaire. No statistical changes were observed in functional mobility or the energy cost of walking tests.
Conclusion:
Replacing the suction suspension system with the hypobaric Iceross Seal-In® X5 improves quality of life in transtibial amputees.
Clinical relevance
The main indicator of suspension system efficiency in lower-limb prostheses is pistoning in the socket. Reduced pistoning of the hypobaric Iceross Seal-In® X5 may contribute to amputees’ rehabilitation.
Background
The efficiency of the prosthesis is mainly guaranteed by its suspension method for securing the socket to the stump. 1 A proper method of prosthetic suspension ensures a well-functioning and safe prosthesis. 2 Transtibial amputees (TTA) reduce their activity and limit prosthetic use because of residual limb problems and discomfort experienced at the socket interface. 3 In fact, the socket is the critical interface between the stump and the prosthesis. 4 Residual limb volume and shape changes lead to gait instability, which causes poor adaptation to the socket by altering limb–socket interface pressure and increasing shear stress. 5 These events occur even in a “mature” residual limb (defined by Berke 6 as >18 months post amputation); in fact, unpredictable individual daily fluctuations of residual limbs were observed in transtibial prosthetic users. 7 Board et al. 8 reported an average 6.5% residual limb volume reduction after only 30 min of walking with a standard Total Surface Bearing (TSB) socket with a one-way valve.
Residual limb volume loss due to prosthetic use leads to increased vertical movement of the stump in the socket, called “pistoning.”9,10 This phenomenon is minimized by a good suspension system that secures the socket to the amputee’s stump, guaranteeing prosthesis efficiency.1,11 As pistoning increases, fit deteriorates, interface pressure and shear stresses increase, and skin ulcerations may appear and limit the amputee’s mobility and autonomy.8,11
The range of pistoning in the TSB socket of TTA has been studied using various methods. Board et al. 8 adopted a roentgen approach and applied different loads and found a mean tibia bone displacement relative to the end of the socket of 4 and 3.3 cm for the socket with electric vacuum pump and suction suspension system (SSS), respectively. With the static photographic method, a mean displacement of 0.9 and 1.3 cm was found in the shuttle lock prosthesis during non-weight-bearing and when 30 N was applied, respectively. 12 Using a motion analysis system to investigate the Seal-In® X5 liners, Gholizadeh et al. reported 0.0, 0.1, 0.1, and 0.2 cm of pistoning in non-weight-bearing, 30, 60, and 90 N conditions, respectively. 1
Many studies have compared different suspension systems.1,7,8,13–17 As far as we know, however, no articles have been published to date that compare the two passive vacuum suspension systems currently available in TSB sockets, that is, the hypobaric Iceross Seal-In® (HIS) and the SSS. TSB suction sockets are widely used in clinical practice because of their better fit and suspension. The passive vacuum system is obtained in both systems by means of a one-way valve positioned in the distal part of the socket. This valve creates negative pressure between the liner and the socket. In Össur’s hypobaric Iceross Seal-In® (HIS) prosthetic liner, the liner holds five silicone hypobaric seals that are able to adapt to the internal surface of the socket, guaranteeing vacuum socket suspension without an external sleeve (Figure 1). 1 In the SSS, the vacuum is obtained by placing a urethane knee sleeve over the proximal one-half of the exterior socket wall and the distal three-quarters of the thigh (Figure 1). 8

Transtibial suspension systems used in the study. Suction suspension system socket components are on the left and hypobaric Iceross Seal-In® X5 membrane components are on the right.
This study aimed to evaluate the influence of the HIS suction system on pistoning, quality of life, and efficiency compared with SSS in unilateral TTA. To achieve our goals, we used the following tests and questionnaires: the pistoning test (PT) to compare vertical movement of the stump within the socket, energy cost of walking (ECW) to check prosthesis efficiency, the Prosthesis Evaluation Questionnaire (PEQ) and the Houghton Scale Questionnaire (HSQ) to evaluate perceived mobility and quality of life with the prosthesis, and the Timed Up&Go Test (TUGT) and the Locomotor Capability Index (LCI) for functional mobility.
We were also interested in determining the time needed by a new HIS Seal-In X5 user to reach or surpass the same suspension stability and ECW they had obtained using the SSS.
We hypothesized that the vacuum obtained with the hypobaric seals would provide better socket suspension than that obtained with the external sleeve, and that this would result in less pistoning, and better user satisfaction and performance with the prosthesis.
Materials and methods
To participate in the study, subjects had to meet the following inclusion criteria: (a) unilateral amputation of lower limb at below-knee level, (b) age 20–65 years, (c) body mass <116 kg and stump at least 11 cm long (to allow using Seal-In), (d) TSB SSS prosthesis user for at least 18 months and for a minimum of 4 h per day, (e) K-level of 3 or 4, 18 (f) ability to walk and perform ramp descending and ascending without aids, and (g) absence of significant clinical disorders.
We enrolled 10 TTAs to participate in the study. They were selected from those who were already SSS and carbon fiber foot users in our database; they had never used a Seal-In liner and wore a prosthesis that was made in the last 18 months by the same expert prosthetist on our team.
The enrolled TTAs gave their informed consent to participate in the study, according to the guidelines of the local ethics committee that approved the study. Each participant was fully informed about the research and understood that participation in the study was voluntary. No fee was paid to participants in the research.
PT
To measure differences between the SSS and the HIS, several PTs were carried out in each evaluation session as follows: first, to obtain a baseline measure, the patient was requested to stand only on the prosthetic limb and second, two measures were obtained when 0 and 30 N forces were applied to the prosthesis in the longitudinal direction while the TTA held the prosthetic leg straight in the air. We calculated the displacements (in mm) of the markers located on the greater trochanter (GT), proximal lateral end of the liner (PL), proximal lateral end of the socket (PS), and distal end of the socket (DS), as in the procedure described by Gholizadeh et al. 12 To minimize measurement errors, we calculated the means of the following displacements in each measure: GT-PS, GT-DS, and PL-DS. The amount of displacement from the baseline identifies the pistoning movement: lesser the displacement, lesser is the pistoning. Data were collected by photos acquired by high-resolution camera (Figure 2).

The three conditions of the pistoning test on the hypobaric Iceross Seal-In® X5: The baseline evaluation is on the left, 0 N applied to the prosthesis is in the middle, and 30 N applied is on the right. Note the markers on the tight and on the socket.
Due to the presence of the sleeve in the SSS, the PS and the PL markers were positioned at the same level as the HIS but above the sleeve. (Figure 3).

Position of markers on suction suspension system.
Compared with Gholizadeh et al.’s procedure, we did not test pistoning by adding 60 and 90 N because we noticed excessive knee flexion on the prosthetic side due to a load reflex of the knee muscles, which affected the pistoning measurements.
ECW tests
ECW tests were performed on the floor (floor walking test (FWT) and on a treadmill (treadmill walking test (TWT)). During the walking tests, metabolic data were collected using a portable metabolimeter K4b2 (Cosmed, Italy). This device guarantees breath-by-breath collection of oxygen consumption data.
TWT were performed with ascendant slope (12%), descendent slope (5%), and without slope (0%). Slopes used in a treadmill test in amputees were reported by Göktepe et al. 19 and Huang et al. 20 In previous studies, TWTs were widely used to compare the effect of different prosthetic components on energy expenditure during ambulation.21,22 FWT is also widely used in amputee ECW evaluation.23–25 In both TWT and FWT, amputees were requested to walk at their own self-selected speed wearing the portable metabolimeter.
ECW at steady state was calculated using the formula: “oxygen consumption/speed” (mL/kg/m). Trials were performed in a random sequence. The interval time between each trial was 30 min for recovery to baseline, as used by Schmalz et al. 22
PEQ
The PEQ is a self-report questionnaire that measures prosthesis-related quality of life and functional outcomes. It consists of nine independent functional domain scales: appearance, ambulation, frustration, perceived response, residual limb health, social burden, sounds, utility, and well-being. 26
Houghton Scale Questionnaire
The HSQ was used to measures time spent wearing the prosthesis and its functional use. 27 It consists of four items: amount of time the prosthesis is used, manner in which it is used, individual’s perception of stability, and whether walking aids are used while walking outside on a variety of terrains. Each item is scored on a 4-point ordinal scale, and the perception of stability questions are binary yes/no answers. The maximum score is 12.
TUGT
We used the TUGT to assess participants’ motor ability when they were wearing the prosthesis. 28 The test measures the time (in seconds) needed to stand up from a standard arm chair, walk 3 m, turn, walk back to the chair, and sit down again.
LCI-5
The LCI-5 was used to evaluate lower-limb amputees’ ambulatory skills with the prosthesis. 29 The LCI tests the ability to perform a number of motor tasks. It provides an aggregated score for 14 items. The maximum total score of the index was 56.
Timing
In a pretest morning session, the same prosthetist on our team who had previously designed the SSS, checked the alignment and adequacy of each participant’s prosthesis. Then each participant was administered the PEQ and the HSQ. Anthropometric (body mass, height) and anamnestic data were also collected. In the afternoon, the participants performed the PT with SSS. Preliminary walking tests on the treadmill (at three different slopes) were also conducted to allow TTAs to become familiar with the equipment and to avoid a learning effect. Two days later, TTAs were administered the ECW tests, LCI-5, and TUGT.
Meanwhile, the same experienced prosthetist began to construct the HIS starting from the plaster cast of the new socket, which is necessary for the Seal-In system. During the 2 weeks or so required to manufacture the HIS, the amputees met with the prosthetist three times. All other prosthesis components remained unchanged.
After 2, 5, and 7 weeks of HIS use, the participants performed the ECW tests and the PT at the same time as the SSS tests and wearing the same shoes. Before each session, body mass was measured to avoid erroneous comparisons between tests. The length of the acclimation periods was established on the basis of Datta et al.’s 21 results. These authors reported that TTAs needed a minimum of 6 weeks to become accustomed to a new socket. LCI-5, TUGT, PEQ, and HSQ were administered after 7 weeks of HIS use. Figure 4 presents a flow chart of the study.
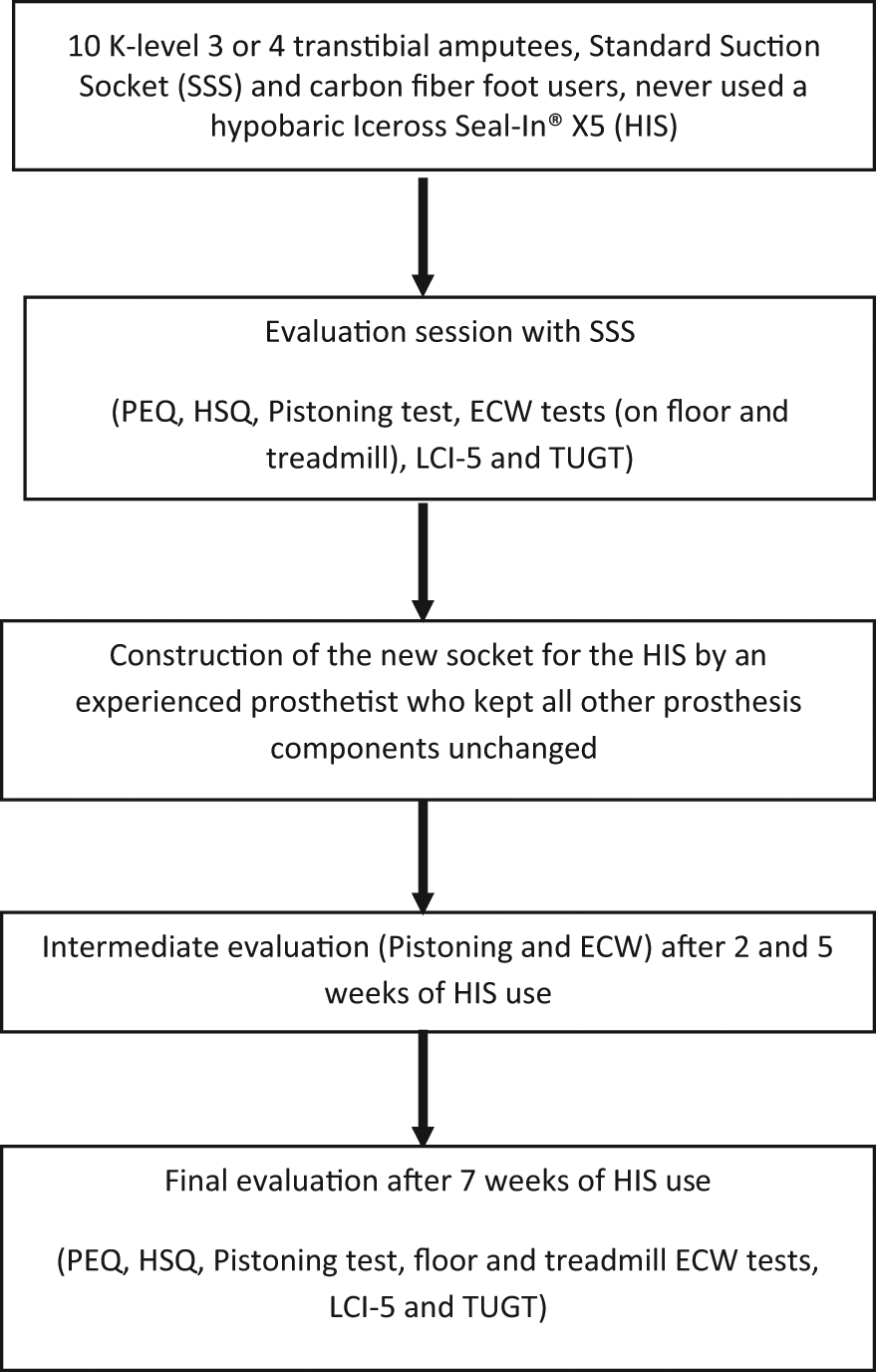
Study flow chart diagram.
Statistical analysis
Statistical analyses were performed using Statistical Package for Social Sciences (SPSS) version 17.0 for Windows. All data were reported as means and standard deviations (SDs).
A repeated-measures analysis of variance (ANOVA) was performed on continuous measures (TUGT, PT, and ECW tests) as within-subject factor along the observation period. Where ANOVAs were significant at a p = 0.05 level, a post hoc analysis was performed, setting the critical adjusted α value by using Bonferroni’s inequality. For nonparametric variables (PEQ, HSQ, and LCI), the Wilcoxon signed-rank test analysis was performed.
Results
Ten male TTAs were recruited to participate in the trial. Their mean age was 44.9 years (SD = 9.5 years). All had been using a SSS prosthesis daily for at least 18 months and continuously for at least 6 h a day. All participants were able to walk without aids, and were active and employed. Demographic data are summarized in Table 1. All participants completed the trial. The results of the PEQ are summarized in Table 2.
Participants’ demographic information and components of their standard suction socket.
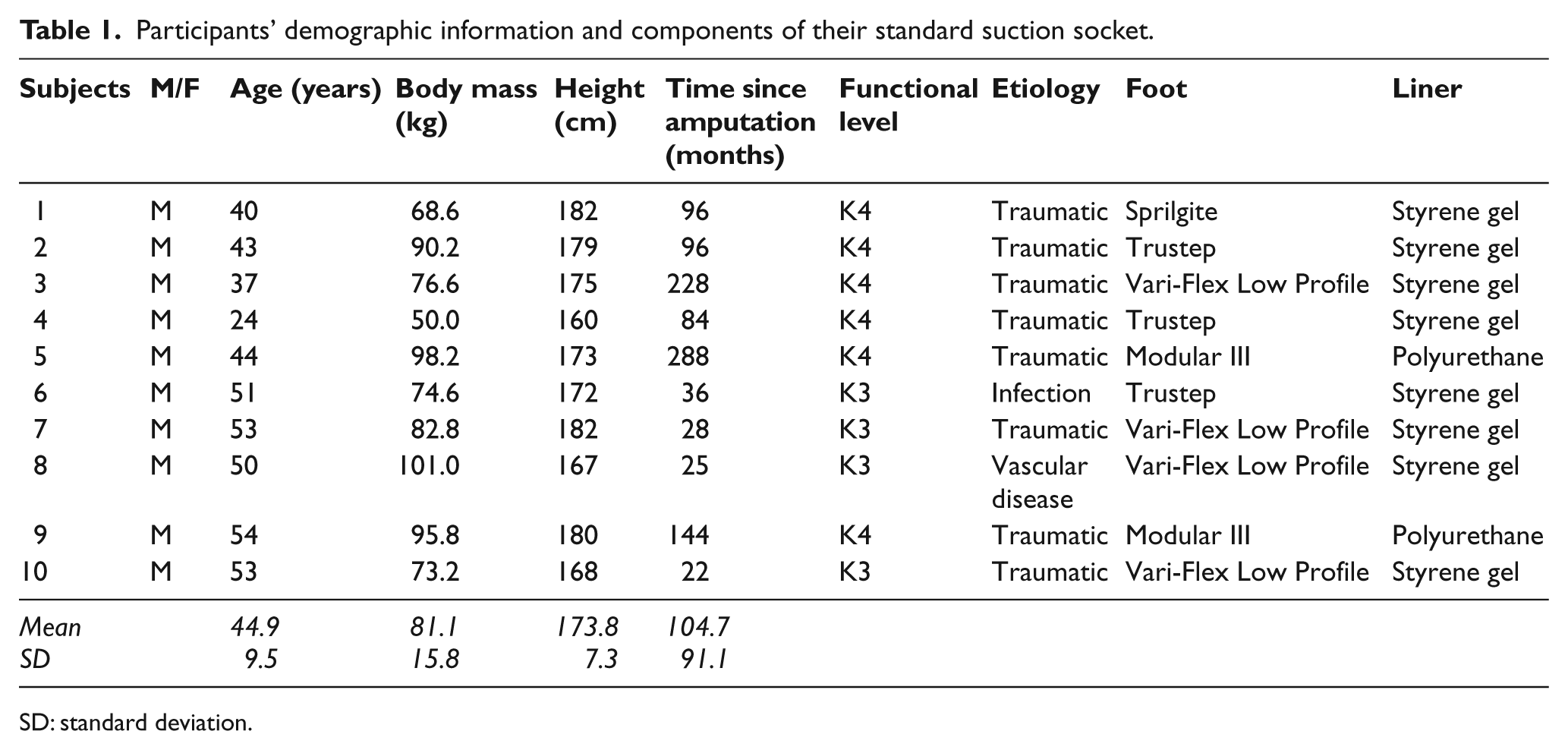
SD: standard deviation.
Results of the PEQ (means ± SDs) administered with the SSS and after 7 weeks of HIS use.
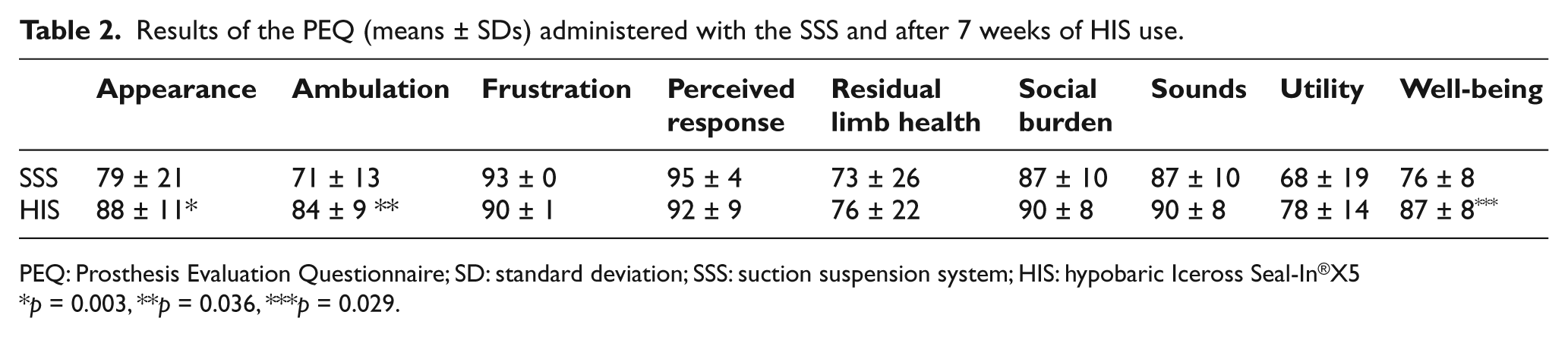
PEQ: Prosthesis Evaluation Questionnaire; SD: standard deviation; SSS: suction suspension system; HIS: hypobaric Iceross Seal-In®X5
p = 0.003, **p = 0.036, ***p = 0.029.
Significant improvement can be observed in the “Appearance,” “Ambulation,” and “Well-being” domains, as reported by participants when utilizing the HIS compared to their answers when they were using SSS.
Pistoning
With no additional weight, the vertical mean displacement with SSS was 7.5 ± 4.7 mm; with HIS, it was 4.7 ± 3.1, 4.6 ± 2.9, and 3.6 ± 3.1 mm after 2, 5, and 7 weeks of HIS use, respectively. As can be seen in Figure 5, use of the HIS led to reduced pistoning, with a statistically significant difference between the first and the last assessment (p = 0.016), in which the mean difference between SSS and HIS displacement was 3.9 mm.
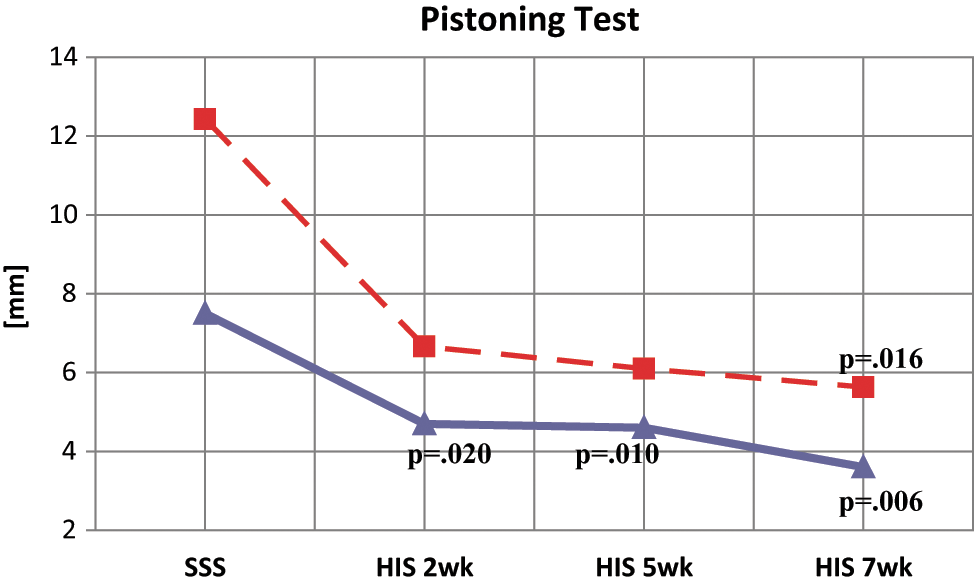
Prosthesis displacement with no weight on the prosthesis (continuous line) and with 30 N applied (dotted line).
When an additional 30 N weight was applied to the prosthesis prior to the PT, HIS use produced a significant improvement after only 2 weeks (p = 0.025); and after 5 and 7 weeks of HIS use, the statistical difference could still be observed, with p values of 0.010 and 0.006, respectively (Figure 4). The mean vertical displacement with SSS was 12.4 ± 5.6 mm; with HIS, it was 6.7 ± 4.1, 6.1 ± 3.1, and 5.6 ± 3.1 mm after 2, 5, and 7 weeks of HIS use, respectively. In this test, the difference between the displacements with SSS and after 7 weeks of HIS was 6.8 mm.
In both pistoning conditions (i.e. no weight and 30 N applied), no statistical differences were found in the data at 2 versus 5 weeks, 2 versus 7 weeks, and 5 versus 7 weeks of HIS use.
ECW tests
As shown in Figure 6, use of the HIS produced a reduction in ECW, which was more marked on the treadmill with the +12% slope. Improvement (mL/kg/m) in the evaluation with SSS and after 7 weeks of HIS use ranged from 0.20 ± 0.21 to 0.18 ± 0.03 (+10%) in FWT, from 0.35 ± 0.1 to 0.31 ± 0.04 (+11.5%) in TWT 0%, from 0.55 ± 0.1 to 0.44 ± 0.13 (+20%) in TWT +12%, and from 0.33 ± 0.11 to 0.28 ± 0.01 (+14.8%) in TWT −5%.
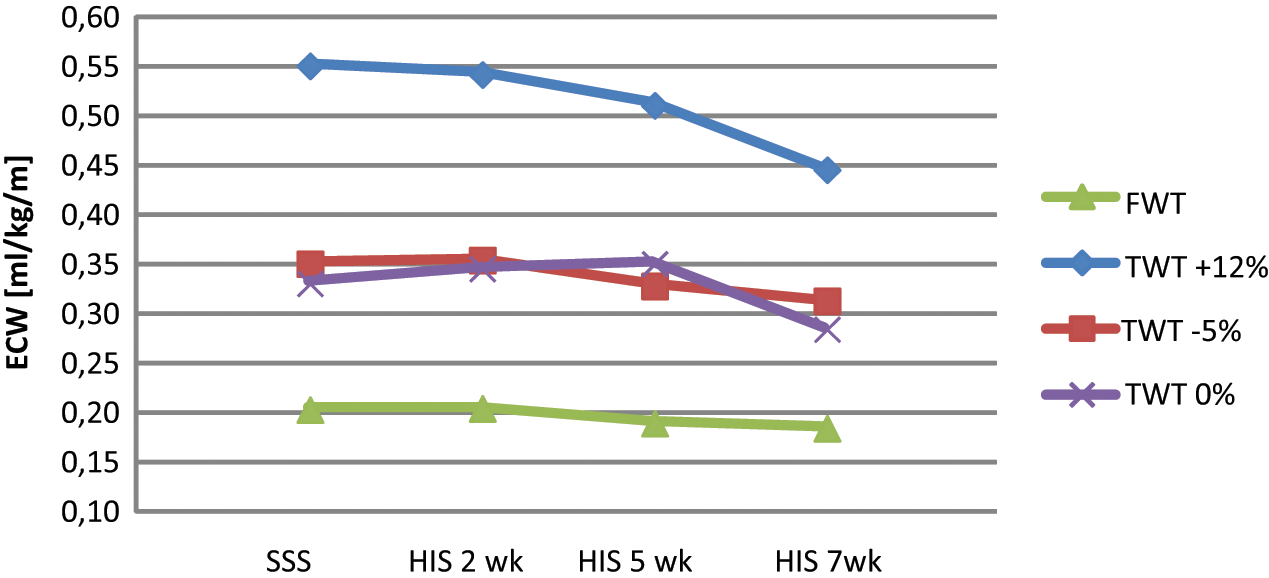
ECW in the four evaluation sessions on floor and on treadmill at different slopes.
Nevertheless, no statistical significance was observed between the two systems in the four conditions. Although walking speed showed a trend toward improvement, it did not reach statistical significance. When evaluated with the SSS, the mean FWT speed was 70.34 ± 11.11 m/min, and after 7 weeks of HIS use the mean speed was 74.21 ± 5.9 m/min, thus showing an increase of 5.5%.
TUGT, HSQ, and LCI
LCI and TUGT data show a trend toward improvement using the HIS (Table 3). Statistically significant improvement was observed in HSQ (Table 3).
TUGT, HSQ, and LCI results (mean ± SD).
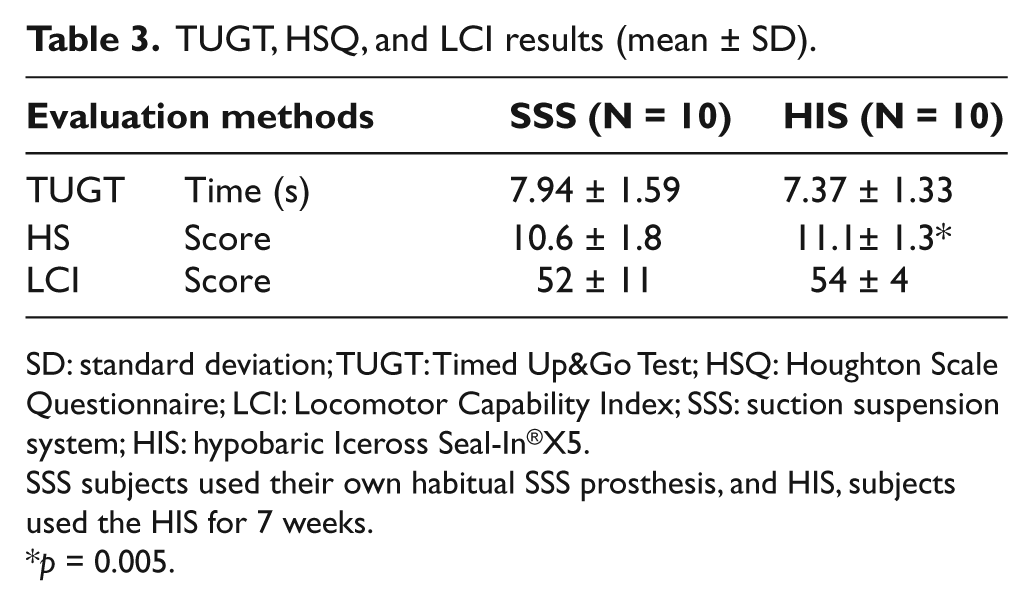
SD: standard deviation; TUGT: Timed Up&Go Test; HSQ: Houghton Scale Questionnaire; LCI: Locomotor Capability Index; SSS: suction suspension system; HIS: hypobaric Iceross Seal-In®X5.
SSS subjects used their own habitual SSS prosthesis, and HIS, subjects used the HIS for 7 weeks.
p = 0.005.
Discussion
This study investigated two of the most used passive vacuum suspension systems: the HIS system and the SSS. To ensure suspension of the prosthesis, both systems have a one-way valve that creates a vacuum between the liner and the socket, but the HIS needs a seal that adheres to the liner, not a sleeve. Gholizadeh et al. 1 investigated the HIS and reported a 71% pistoning decrease with its use compared with a Dermo® liner (shuttle lock system), but their study was limited to the PT. In this study, we used a wide range of evaluations (PEQ, PT, HSQ, ECW, TUGT, and LCI) to explore a wider range of prosthetic function.
The PEQ data showed a statistically significant improvement in the “Appearance” domain, that is, the amputees thought the HIS prosthesis had a more pleasing appearance than the SSS prosthesis. Moreover, participants rated their abilities to ambulate higher when wearing the HIS (“Ambulation” domain). After 7 weeks of HIS use, participants also reported significant improvement in the “Well Being” domain. The PEQ improvements may also explain the significant improvement in the HSQ. In fact, the HSQ asks amputees whether they feel unstable when walking outside on slopes with the prosthesis and for how long and when they wear the prosthesis. In light of these results, we also expected a significant improvement in “Utility,” but, despite an improvement of 12.8% the p level of significance in this domain was 0.057. Perhaps subjects were influenced by difficulty in donning the Seal-In X5 because it takes some effort to reverse the liner and roll it over the residual limb. The importance of a proper suspension system to guarantee amputees’ comfort and prosthetic function has been widely indicated in the literature, and vertical displacement or pistoning within the socket has been suggested to be one of the main indicators of suspension system efficacy in lower-limb prostheses.1,4,12,14,30 We found a statistically significant reduction of pistoning with HIS use. This effect may be related to the vacuum provided by the hypobaric seals of the Seal-In® X5. By contrast, in the SSS, the vacuum is provided by the sleeve. Moreover, the values recorded with the SSS may be underestimated because the proximal marker (PL), which should be fixed, is placed above the sleeve and may be slightly dragged down by gravity and applied weight. The vertical displacements found by Gholizadeh et al., 1 investigating the same Seal-In® X5 liner, were 0 mm in the non-weight-bearing (0 N) and 1 ± 0.8 mm in the 30 N applied condition after 4 weeks of HIS use. These values are lower than ours, that is, the mean displacement with HIS was 4.6 ± 2.9 mm in the 0 N condition and 6.1 ± 3.1 in the 30 N condition after 5 weeks of HIS use. These differences may be due to marker positioning and different measuring systems. Gholizadeh et al. used the Vicon motion system and the transparent socket to check vertical movement in the socket. Comparing our results with those of Gholizadeh et al. using the same PT methodology, we found that the displacement observed in the 0 N and 30 N condition with a shuttle lock system (10 ± 9.2 mm and 14 mm, respectively) was more than that obtained in our study with the SSS (7.5 ± 4.7 mm and 12.4 ± 5.6 mm). 12 Klute et al. 13 reported similar results in pin lock suspension pistoning at 0 N (6 ± 4 mm).
To our knowledge, there are no studies comparing ECW with two different suspension systems in the recent literature. 31 The energy cost on floor data with HIS (0.18 mL/kg/m) is similar to those reported in the literature for a comparable sample (0.16 mL/kg/m) and closer to those of healthy adults (0.15 mL/kg/m). 32 ECW was higher with SSS (0.20 mL/kg/m). The ECW data analysis showed that HIS may allow for more efficient gait, as reflected by the lower ECW and higher walking speed (not statistically significant) in all conditions.
The TUGT data show the high level of physical mobility of our sample. Time needed to perform the test was less than 8 s with both suspension systems. These data are similar to those reported in an analogous sample. 33
This study showed that HIS use decreases pistoning significantly, improves some aspects (appearance, ambulation, and well-being) of amputees’ perception of their prosthesis and prosthesis function, and increases prosthesis use when compared with a standard suction socket. Patients’ improved perception of mobility and functional outcome is not captured with objective functional tests (i.e. ECW and TUGT). The less pistoning experienced with HIS could be the main factor determining amputees’ satisfaction because they felt more stable in the socket. We must emphasize that the PEQ is sensitive to changes specific to prosthesis function and allows investigating important effects that probably would not be detected by any of the existing rehabilitation outcome measurements. 34
We found that despite a significant reduction of vertical displacement within the socket, neither motor capability test results nor ECW improved. However, we have to consider the high functional level of our sample (mean LCI score of 52; K-level of 3 and 4) whose efficiency was hard to improve. In particular, LCI is prone to ceiling effects that would limit its ability to detect improvement. 35 Moreover, the ECW test results showed a nonsignificant trend toward improvement while using HIS. Regarding our aim to determine the time needed to become acclimated to the HIS, we can speculate that 2 weeks are enough to reach the same performance as that with the SSS. In fact, the ECW and the PT with no additional weight remained statistically the same with the two suspension systems after 2 weeks of HIS use. Moreover, PT with 30 N significantly improved after 2 weeks, but no further significant improvements were observed in the values after 5 and 7 weeks of HIS use. Significant improvement in both conditions (PT with no additional weight and 30 N) was observed after 7 weeks of HIS use. We speculate that this is the time necessary for new HIS users to fully adapt their sensations and residual limb muscles to the new proprioception provided by the different suspension socket.
Study limitation
Our experimental sample was relatively small (10 subjects) because of difficulty in recruiting subjects willing to change their usual suspension system and take part in a study requiring many days of commitment. These difficulties have also been observed in previous studies: for example, Prince et al. 36 enrolled 5 TT amputees for a comparison between different prosthetic feet, and Klute et al. 13 analyzed the outcome of only 5 TT amputees when comparing PIN and a vacuum-assisted system because 15 patients dropped out. In fact, the study population included only amputees of a given functional status who were active and had defined prosthetic components. Therefore, the results cannot be generalized across a broader population. In fact, the HIS produced insignificant reduction on the floor and treadmill ECW and on TUGT time; this may have been due to the high functional level of our small sample. Future studies should recruit larger patient samples with broader functional levels.
Conclusion
Using the hypobaric Iceross Seal-In® X5, there were fewer pistoning movements in the socket. This was associated with a statistically significant improvement in quality of life, as reported by users. Moreover, HIS use led to improvement on the HSQ, which indicates more intensive and safe use of the prosthesis. In conclusion, this study shows that in unilateral TTAs, the HIS suction system (compared with that of the SSS) reduces pistoning and improves quality of life.
Footnotes
Conflict of interest
None declared.
Funding
This project was partially supported by grants from Össur, Reykjavík, Iceland.