
Abstract
Background: Stair ascent is a very demanding task for transfemoral amputees (TFAs). The purpose of this study was to investigate the lower extremity joint kinematics of TFAs who can climb stairs using a step-over-step gait pattern without an active artificial prosthetic knee joint or handrail use.
Case Description and Methods: Case series. Participants were two traumatic TFAs and 10 control participants. Both TFAs used a single-axis prosthetic knee joint in daily living. Sagittal plane joint kinematics were recorded at 60 Hz using an eight-camera motion analysis system and digital video camera.
Findings and Outcomes: From the instant of touchdown, the prosthetic knee joint was rapidly extended and remained fully extended until toe-off. In the latter half of the stance phase, the knee and ankle joints of the sound limb simultaneously showed rapid joint flexion during continuous extension. Further, the ankle joint of the sound limb showed greater plantarflexion at the end of the stance phase.
Conclusion: These results suggest that the TFA in the present study would (1) extend the prosthetic knee joint to prevent the knee flexion generated by the bodyweight (plus ground reaction force and/or joint moment), and (2) lift the whole body in an upward direction using strong counter-movements and greater joint extension during the stance phase.
Clinical relevance
The data describing the lower extremity joint kinematics of TFAs who can climb stairs in a step-over-step manner provides us with a basis for better understanding of adaptive prosthetic control and would be expected to aid in the development of more effective gait rehabilitation programme.
Introduction
In daily living, stair ascent is a very demanding task for transfemoral amputees (TFAs). In a step-over-step gait pattern during stair ascent, knee and ankle joints must continuously extend during the stance phase to overcome the joint flexion moment generated by the body’s weight. After that, both hip and knee must flex to clear the stairs to avoid tripping. Although some studies have been conducted to examine bilateral lower limb mechanics during alternating stair ascent in transtibial amputees,1-3 no study has yet quantified these in TFAs. Moreover, some studies clearly reported that TFAs could not climb stairs in a step-over-step manner.3-5
However, though less common than non-reciprocal stair climbing, there are TFAs who can climb stairs using a step-over-step gait pattern without an active artificial prosthetic knee joint or handrail use. Analysing such TFAs could aid in the development of a prosthetic knee unit and more effective gait rehabilitation; however, no study has yet reported such data. The aim of the present study was to describe the lower extremity joint kinematics in TFAs who can climb stairs in a step-over-step manner.
Methods
Subjects
Two male traumatic TFAs (TF1 and TF2) and ten able-bodied subjects (ABs) volunteered for the investigation conducted at the National Rehabilitation Center for Persons with Disabilities in Japan (Table 1). Both amputees routinely performed stair ascent in a step-over step manner in their daily lives. The stair assessment index (SAI) 6 was 13 for both amputees (‘without rail or assistive device, step-over-step pattern’). Our amputated subjects had no vascular disease, skin problems or any other balance limitations. The protocol was approved by the local ethical committee in accordance with the guidelines set out in the Declaration of Helsinki (1983).
Subjects characteristics.
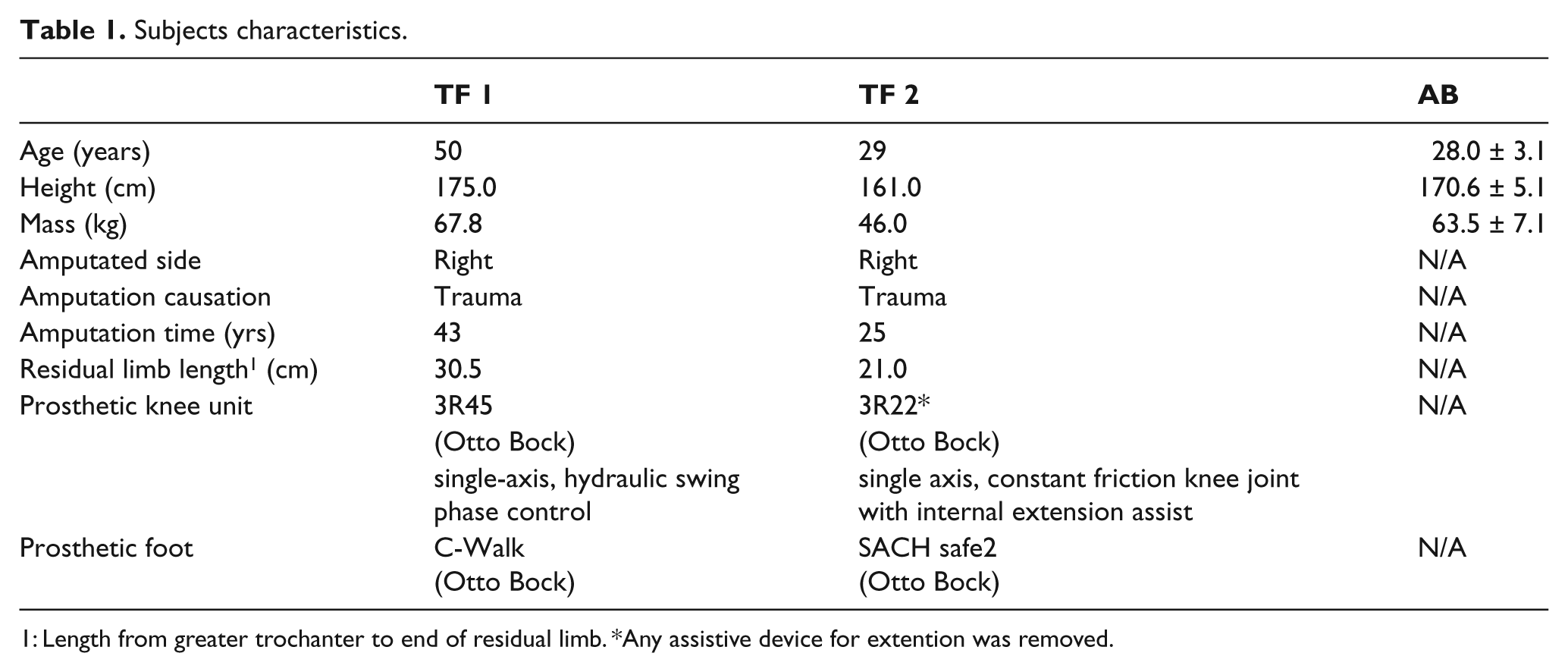
Length from greater trochanter to end of residual limb
Any assistive device for extention was removed.
Task
The subjects were asked to perform step-over-step stair ascent (normal reciprocal stepping pattern) at their preferred speed (Figure 1A and B). From the lowest step, the subjects climbed a custom-built staircase of five steps (height 16 cm, width 80 cm, tread 30 cm).
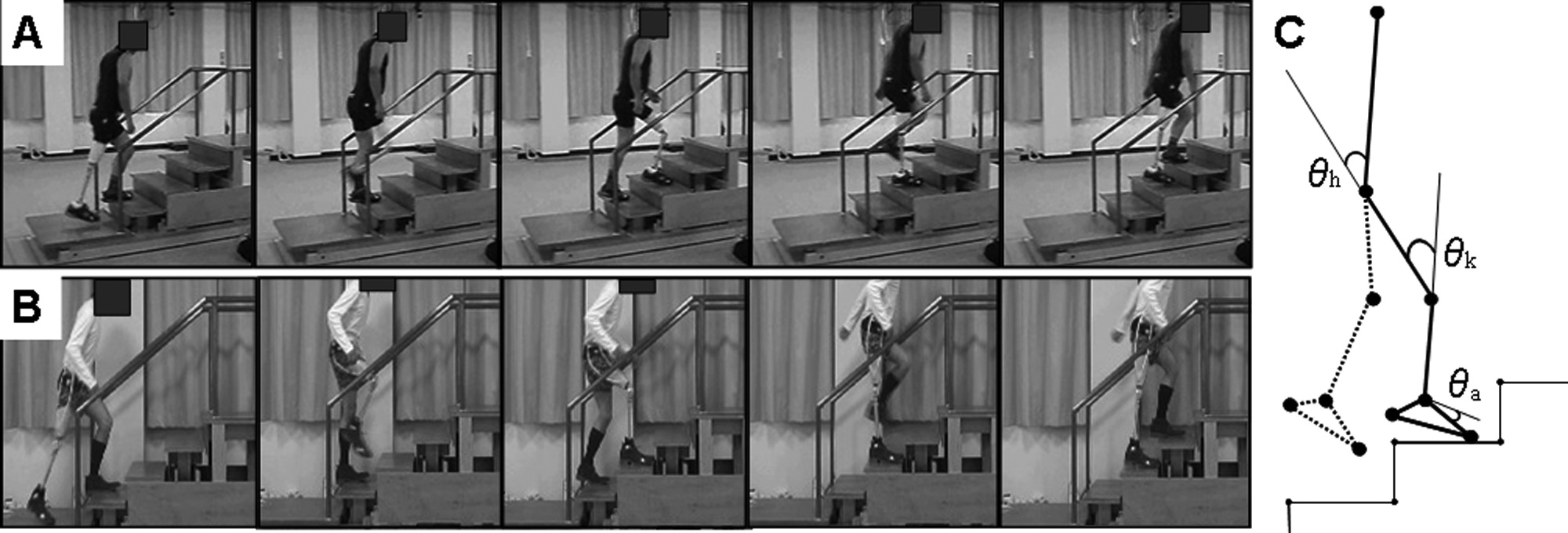
A-B; Successive picture of step-over-step stair ascent in TF 1 and TF 2, respectively. C; A schematic diagram of the linked segment model used to calculate sagittal-plane joint angles (θ) of hip (h), knee (k) and ankle (a). The solid leg is the analyzed side, and the dotted leg is the non-analyzed side.
Procedure
Although our TFAs had mastered step-over-step stair ascent, they practised the task for as much time as was needed before data collection. Then, three trials beginning with the left leg were performed.
For TF1 and the AB group, kinematic data were sampled at 60 Hz using an eight-camera motion analysis system (VICON 512, Oxford Metrics, UK). Kinematic data for TF2 was recorded from the right side using a 60 Hz video camera (DCR-SR-100, SONY, Japan). To calculate joint angular kinematics, raw marker coordinates were determined using Siliconcoach Pro 7 (Siliconcoach Ltd., Dunedin, New Zealand). Twelve 25 mm retro-reflective markers were placed at the following locations: the fifth metatarsophalangeal joint (or similar location of the prosthetic foot), heel (similar location of the prosthetic foot), lateral malleolus (ankle joint of prosthetic foot), lateral epicondyle of the femur (pivot of prosthetic knee joint), greater trochanter, and acromion scapulae. The positional data of the reflective markers were low-pass filtered by a fourth-order zero-lag Butterworth filter with a cut-off frequency of 6 Hz, from which sagittal plane joint angles for both the prosthetic (PST) and sound limb (SND) of the amputee were determined (Figure 1C). During swing phase, we further calculated average hip and knee flexion velocity (ωhip and ωknee), which was defined as the difference between the joint angle at toe-off and maximum joint flexion divided by the movement time. For SND and PST limbs, a stride cycle was defined starting with foot contact on the second step (third step for PST) and ending at the next foot contact on the fourth step (fifth step for PST). From video images, we measured stance (from foot contact to toe-off) and swing time (from toe-off to foot contact), respectively. For comparison, the kinematic data recorded from left and right legs (as dominant leg; preferred leg for kicking a ball) in AB were averaged for five trials in each leg.
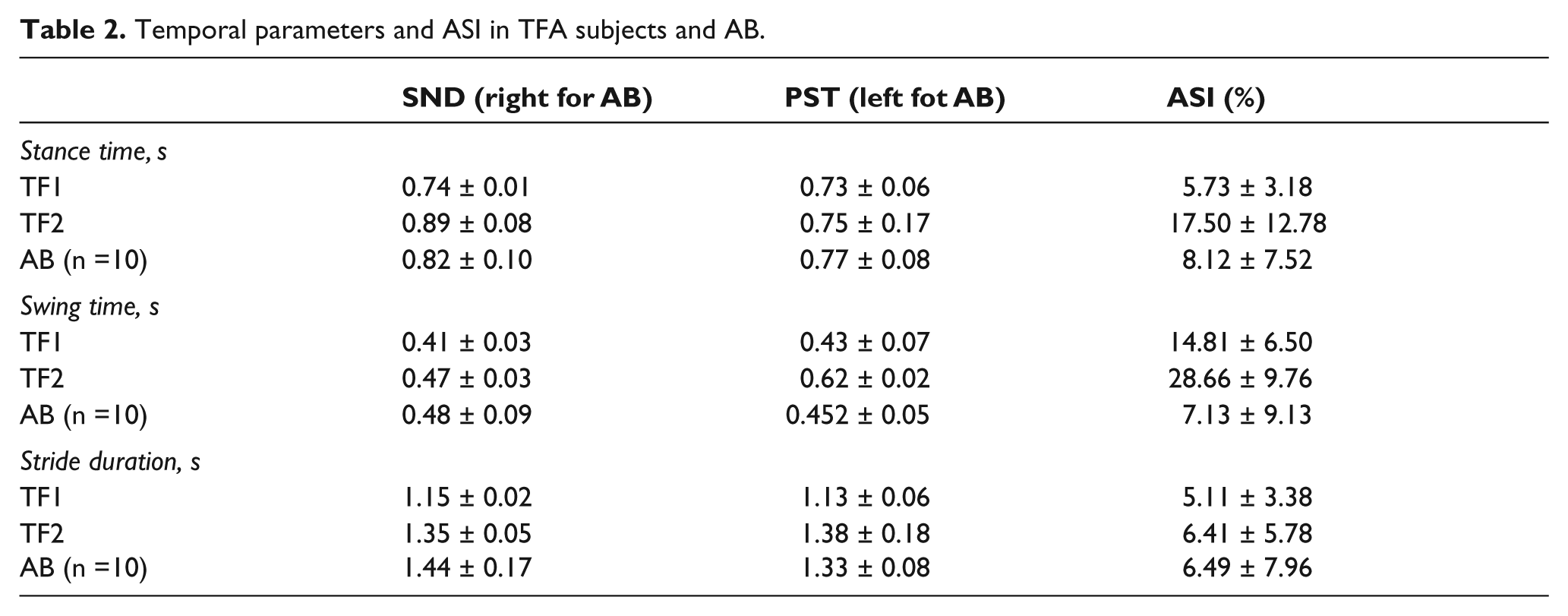
In accordance with a previous study, 7 the absolute symmetry index (ASI) of stance, swing time and stride duration for TFAs was calculated as follows:

where SND is the parameter recorded from the sound limb and PST is the corresponding parameter from the prosthetic limb. A value of zero for the ASI indicates that the variables SND and PST are identical and, therefore, that there is perfect symmetry as measured by that particular gait parameter.
Results
On average, stance time, swing time and stride duration in both TFAs were similar to those of ABs (Table 2). The ASI of the temporal parameters is summarized in Table 2.
Temporal parameters and ASI in TFA subjects and AB.
Kinematic data showed that the hip joints of ABs were extended from the instant of touchdown (Figure 2A). Hip extension peaked at the end of the stance phase, and the hip joint subsequently flexed during swing phase. These trends were similar for both legs in TF1 and for the PST in TF2.
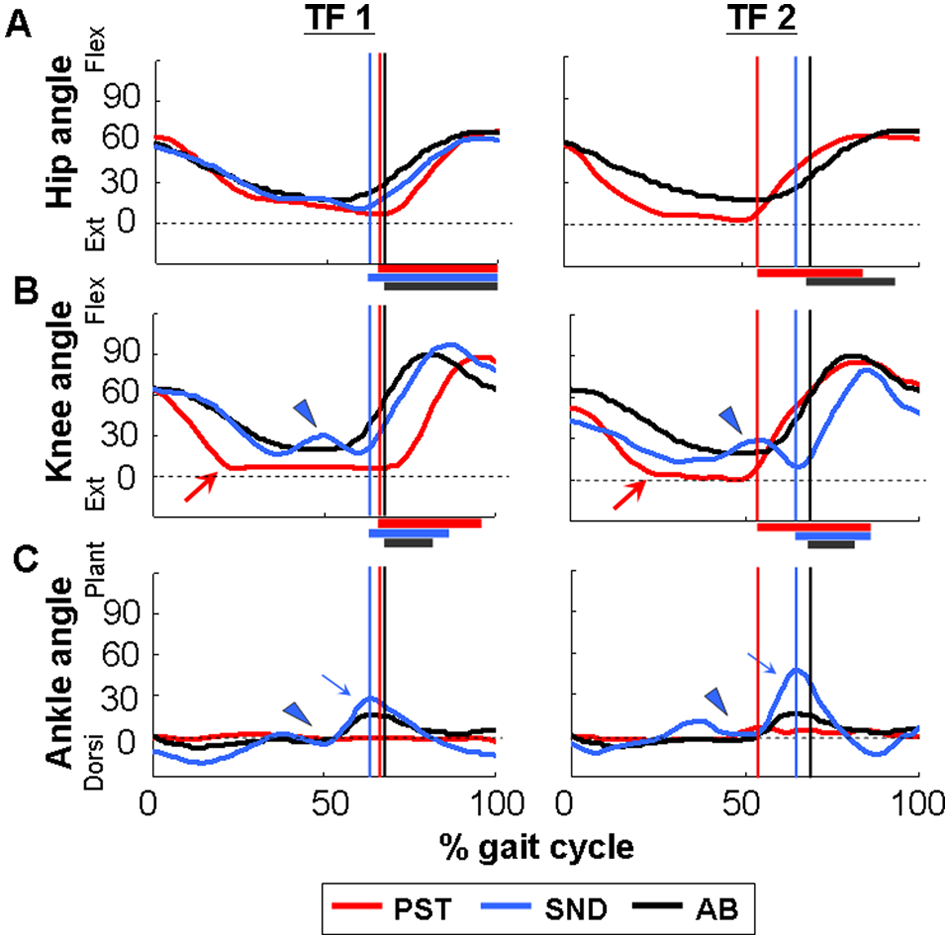
Typical example of sagittal-plane joint angles of hip (A), knee (B) and ankle (C) for each subject. Red, blue and black lines indicate the PST, SND and AB (n = 10), respectively. The timing of toe-off is indicated by vertical lines in the figure. Dotted lines represent the joint angle when the subjects performed quiet standing. Arrows indicate a full-extension of knee (B) and plantarflexion (C). Arrowheads indicate a temporary knee flexion and plantarflexion during the stance (B and C). Note that hip angle in SND of TF 2 is missing due to the blind angle from the video image. Bars along the X-axis represent time widows for calculating average hip and knee flexion velocity during swing phase.
The knee joint of ABs demonstrated continuous extension during stance phase, and subsequently, the knee joint flexed during swing phase (Figure 2B). However, we found distinct differences in knee joint kinematics between ABs and both TFAs. During stance phase, the knee angle of the PST was rapidly extended and remained at the full-extension angle until toe-off (Figure 2B). The peak knee extension angle in the PST was greater than in ABs. For the SND, the knee joint demonstrated continuous extension during the stance phase. However, the joint motion was interrupted by a temporary knee flexion in the latter half of the stance phase (arrowhead in Figure 2B).
The AB ankle joint remained at about 0 degrees for most of the stance phase, and began to plantarflex late in the stance phase (Figure 2C). The PST ankle joint was steady at around 0 degrees during the gait cycle (Figure 2C). During the stance phase, however, ankle joints in the SND demonstrated continuous ankle plantarflexion, which was interrupted by a temporary ankle dorsiflexion during the latter half of the stance phase (Figure 2C). Further, at the end of the stance phase, the ankle joint of the SND showed greater plantarflexion than those of the PST and ABs (arrowhead in Figure 2C).
Absolute and normalized data of both the ωhip and ωknee in the PST limb for both TF subjects are shown in Figure 3A and B. Although the ωknee in PSTs was similar to those of ABs, ωhip in PSTs it was about 1.5 times greater than in ABs.
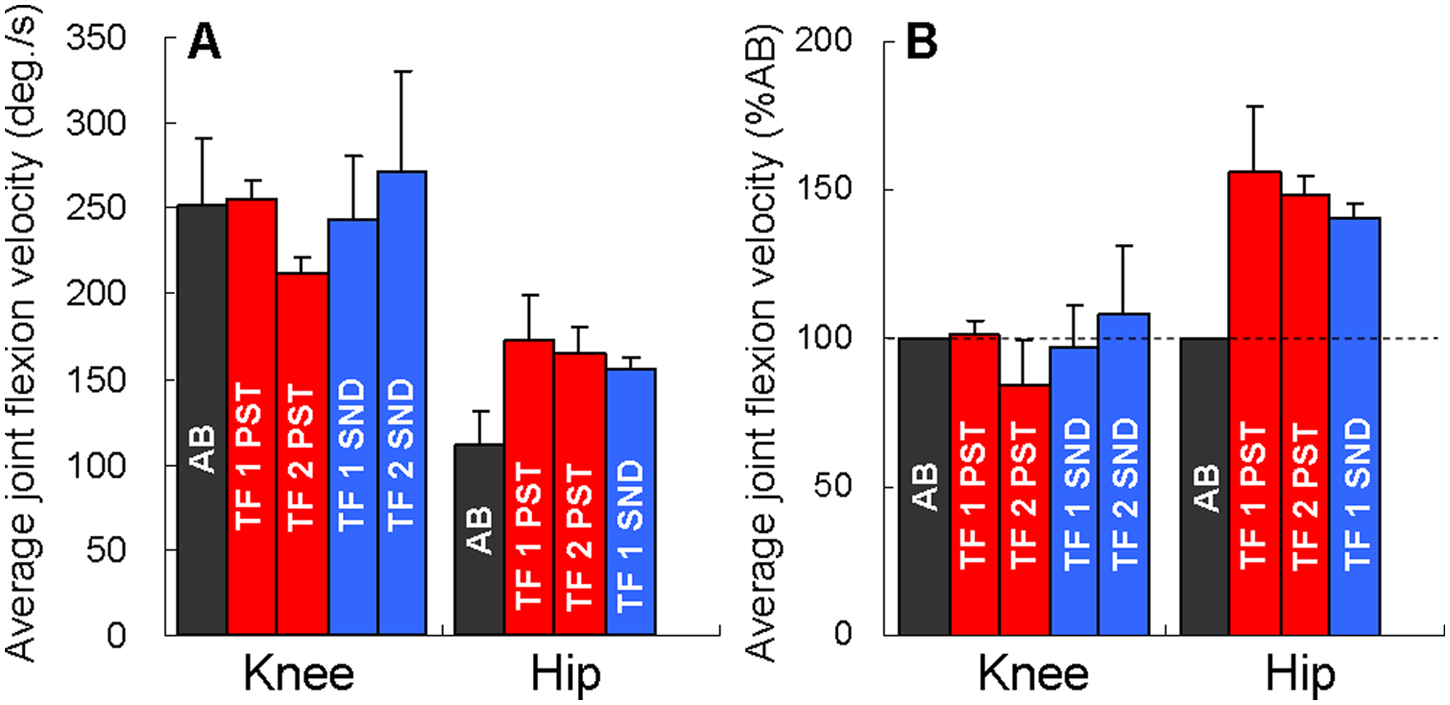
Average hip and knee flexion velocity during the swing phase. The data was shown in absolute values (A) and normalized to AB value (B).
Discussion
Although the amputees in our study differed in physical characteristics, they had one important thing in common in our study: stair ascent ability as measured by the SAI was 13 for both. Their scores are considerably greater than those of TFAs in a previous study, where the mean SAI score in TFAs was approximately 5 (‘without rail or assistive device, step-to pattern’). 6 These results suggest that stair ambulation ability in both TF1 and TF2 was relatively better than those of other TFAs. Furthermore, it is interesting to note that both amputees lost their leg at quite a young age. On the other hand, residual limb length, which was thought to affect ambulatory ability in amputees, differed between these two subjects (Table 1). These results agree with a previous finding demonstrating that residual limb length did not significantly correlate with any spatiotemporal, kinematic and kinetic gait parameters. 8
Both TF1 and TF2 used a single-axis prosthetic knee joint (Table 1). These results indicate that a single-axis prosthetic knee joint may be important for ascending stairs using the step-over-step pattern. The reason is unknown, however. It may increase voluntary control or reaction of the knee when the body is moved a certain way relative to the knee axis. Indeed, a patient preferred to use a non-microprocessor knee mechanism rather than a C-Leg, because it gave more voluntary knee control. 9 However, this is opposed to the more passive input required from microprocessor knees or the rapidly changing instantaneous centre of rotation in polycentric units. Also, when climbing stairs, the knee needs to be able to flex rapidly, and non-powered models obviously drop more readily into flexion in accordance with gravity than many microprocessor knees do. Therefore, a non-microprocessor single-axis prosthetic knee joint would be a reasonable mechanism for our TFAs during stair climbing in a step-over-step manner.
Past studies have reported that TFAs have a gait pattern in which the foot of the PST limb is pulled up only after the foot of the SND limb climbing the step is placed firmly on the step.4,5 This climbing strategy is called the ‘step-to-step pattern’, and is frequently seen in TFAs.6,10 Thus, to our knowledge, this is the first study describing the lower extremity joint kinematics of TFAs who can climb stairs using a step-over-step gait pattern without external aids.
In both TFAs, the range of stride duration was similar to those of past findings in healthy individuals, with a stride duration during stair ascent of 1.03 to 1.42 s. 11 Further, the observed asymmetry in temporal parameters were distinctly lower than those of level walking in TFAs, 7 where the ASI of stance and swing time ranged from 23.42 to 33.49% and 37.38 to 64.56%, respectively. This may be attributable to the knee unit features used, because some knees require force and time to actually pull open into extension. 12 Or maybe both TFAs have potential resistance for the stability of the knees in yielding. 13 Whatever the case, these results suggest that observed stair climbing performances in our TFAs were relatively symmetrical compared with the flat ground gait performed by other TFAs.
The most striking kinematic feature in our TFAs was the knee joint kinematics of the PST during the stance phase. At the instant of touchdown, the PST knee was rapidly extended and remained at the full-extension angle until toe-off (Figure 2B). Although no study has reported these kinematic features during step-over-step stair ascent in able-bodied subjects,11,14 similar knee kinematics in TFAs were observed not only during stair ascent using an above-knee prosthesis with a built-in hydraulic cylinder connected to an external source of power, 15 but also during running 16 and uphill walking. 17 These common joint movements may represent a singular posture in mechanics. That is, from the viewpoint of decreasing the degree of freedom of motion, such a posture might be an effective way to prevent knee flexion generated by the body’s weight (plus ground reaction force and/or joint moment).
It is worth noting that both knee and ankle joints of the SND limb simultaneously demonstrated rapid joint flexion during continuous extension in the latter half of the stance phase (Figure 2B and C). The joint extension preceded by joint flexion was called ‘counter-movement’, which could enhance mechanical power output utilizing the elasticity of the muscle-tendon complex (MTC). 18 Thus, our TFAs might compensate for the power production in the PST limb by using counter-movement in the SND, because it could utilize the elastic energy in the quadriceps and triceps MTC. Further, at the end of the stance phase, the ankle joint of the SNDs showed greater plantarflexion than those of the PSTs (Figure 2C). A similar trend was observed in the stair ascent of transtibial amputees, 3 suggesting that a necessary lift for the vertical centre of mass position is achieved by strong plantarflexion of the SND limb. Further, previous studies reported similar compensatory strategies during uphill walking and an obstacle avoidance task in TFAs. 19 Therefore, the TFAs in the present study would lift the whole body in an upward direction using both counter-movements and greater plantarflexion during the stance phase.
Despite both TFAs having no external source of power in their prosthetic knee units, they could flex their PST knee joint during the swing phase (Figure 2B). A possible explanation for the knee flexion would be the hip flexion in their PST limbs. We found that ω hip during swing phase in the PST limb was apparently greater than those of ABs (Figure 3). Given that the hip joint in the PST limb is the only joint controllable for TFAs, they would intentionally flex the hip joint rapidly to replicate the knee joint in conjunction with the hip flexion in the same manner as ABs.
Limitations
There are several concerns regarding the interpretation of the findings. First, due to the limited number of transfemoral amputees who can climb stairs in a step-over-step manner without an external aid, only two TFAs were available for the present study. To verify the effectiveness of the compensatory strategies observed in this study and establish practical gait rehabilitation by the therapist, there should be multiple subjects in future research. Secondly, we could not determine the ground reaction force and joint kinetics due to the experimental setting. Thirdly, in the present study, we could not identify how these TFAs acquired the compensatory movement over the past decade or so. Clearly, additional work is necessary to determine the mechanisms responsible for the step-over-step stair ascent pattern in TFAs.
Conclusion
The results of the present study suggest that the key to performing step-over-step stair ascent in transfemoral amputees could be (1) a fully extended prosthetic knee joint in the early stance phase, and (2) strong counter-movements and greater joint extension motion in the SND limb during the late stance phase. Further, both TFAs used a single-axis prosthetic knee joint in daily living. Current results indicate that reciprocal stair ascent is possible in TFAs. Such a possibility accompanied by biomechanical analyses would contribute to an increase in training options for stair ascent in TFAs.
Footnotes
Acknowledgements
The authors thank Dr Andrew Lavender for careful reviews of this and earlier drafts.
Funding
This work was supported by Grant-in-Aid for Young Scientists (B; No. 21700569) from the Japanese Ministry of Education, Culture, Sports, Science and Technology.