
Abstract
Background:
Prosthetic services are inaccessible to people living in rural areas. Systems like the modular socket system have the potential to be fabricated outside of the prosthetic workshop.
Objectives:
This study aimed to evaluate the patient’s performance and satisfaction with the use of the modular socket system, and the technical feasibility of its implementation in a rural setting.
Study design:
A quantitative longitudinal descriptive study design was followed.
Methods:
A total of 15 persons with a lower limb amputation were fitted with the modular socket system and followed over 4–6 months. Performance was measured using a 2-min walk test, 10-m walk test and mobility and function questionnaire. Satisfaction was measured by the Socket Fit Comfort Score, Prosthesis Evaluation Questionnaire and EuroQoL 5 Dimensions 5 Levels. Notes on technical feasibility were taken at the moment of fitting (t0), at 1–3 months post fitting (t1) and at the end evaluation at 4–6 months post fitting (t2).
Results:
Performance did not change between t0 and t2. The comfort of the socket fit reduced between t0 and t2. Satisfaction with prosthesis and general health status stayed constant over time. The average fitting-time for the modular socket system was 6.4 h.
Conclusion:
The modular socket system can be considered a useful alternative for use in rural settings.
Clinical relevance
The use of the modular socket system is feasible and can improve accessibility to prosthetic technology in rural areas. Experienced prosthetic users were satisfied with the performance and the device. The shorter manufacturing time and use of only hand-held tools makes it an ideal alternative for use in remote and rural settings.
Background
According to the World Health Organization (WHO), 1 there are about 650 million people with disabilities worldwide, corresponding to about 10% of the world population; 80% of the people with disabilities is currently living in low-income countries. 2 One of the most important requirements for people with disabilities to participate well in society is their access to assistive technology. Prostheses and orthoses make up the majority of the devices which are required by people with physical disabilities. 3 However, in many low-income countries, only 5%–15% of the people who need assistive technology can afford it. 4
More than 30 years ago, Murdoch 5 wrote in an editorial article that one of the major problems in the provision of prosthetics and orthotics is a lack of instructors to train the required number of professionals needed to treat the millions of amputees worldwide. Plenty of prosthetists have been trained in the last decades, but many countries still have a reported shortage of rehabilitation professionals who are properly trained in manufacturing or adapting products or delivering prosthetic services. 4 Beside a lack of professionals who can provide prosthetic services, there are also other factors that limit access to prosthetics, for example, inaccessible transport, short supply of assistive technology services and far travel distances from the disabled persons’ home to the service delivery points. 4 To overcome those problems, there is a need for a different approach to be able to solve the problems with accessibility to assistive technology in rural areas.
Based on a global survey, it was concluded that about half of the responding countries do not have a programme regarding supply of assistive devices. 6 Non-governmental organisations often only have little geographical coverage due to limited financial resources, and their services often focus on specific types of assistive technology or disabilities. 4 A strategy that has been mentioned to provide assistive technology in less resourced settings is community-based rehabilitation (CBR). 4 The CBR model was developed in the 1960s, and it was promoted by the WHO as a way to reach up to 90% of the population in some lower income countries. 7 Intervention studies and case reports are, however, still scarce, 8 and although the CBR guidelines were updated in 2010, it is still unclear how provision of prosthetics and orthotics fit in this model. 7
Murdoch 5 suggested that automating manufacture of prostheses and use of modular components could help to diminish this problem. The most critical part of a prosthesis is the socket that is fitted to the residual limb of the patient as this has to be tailor made. In most of the current production methods, a prosthetist first needs to make a plaster cast negative and subsequently a plaster positive copy of the residual limb. Next, a specific material (typically a heated sheet of polypropylene) is moulded over the plaster positive. This fitting process is labour-intensive and patients sometimes have to wait 2 weeks from the intake until the prosthesis is finished. Since travel distances are often large, people usually stay close to the workshop during this period. Not all patients can afford to be away from home for such a long period.
The lengthy manufacturing process is a problem for amputees living in the area east of Bali (Indonesia), where one prosthetic workshop at Bali is serving the vast region east of the island. To make production of prosthetics suitable in a CBR setting, a first step may be a mobile production method. 9 Prerequisites for such a method is that the prosthesis can be produced low-cost within 1 day and only requires simple portable machinery.
An approach that targets the requirements to make a lower leg prosthesis within 1 day with limited required tools is the modular socket system (MSS), developed and delivered by Össur®. The MSS system is a further development of the ICEX® system 10 in which the socket is produced directly on the residual limb of the patient. Normann et al. 11 showed that the direct prosthetic costs of the MSS were higher compared to plaster casting with standard laminated socket, but also that the MSS could be delivered significantly faster with fewer visits and it does not require the use of any heavy machinery. This could make it suitable for application in a CBR setting. However, although the MSS has demonstrated its use in Western countries, 11 it is unknown whether it suits the lifestyle of people living in rural areas.
The aims of this study were therefore to evaluate (1) the patient’s performance when using the MSS, (2) the patient’s satisfaction regarding the use of the MSS in a rural setting and (3) the technical feasibility of the MSS for implementation in a CBR setting in terms of required tools, skills and required production time.
Methods
A quantitative longitudinal descriptive study design was followed.
Study setting
The study was performed by Exceed Jakarta by a team of four prosthetists, under the supervision of the head of Exceed Indonesia. A 3-day training in the application of the MSS was provided in Jakarta by an instructor of Össur. The head of Exceed Indonesia, who was already familiar with the MSS system, provided further instructions and supervision to the team that fitted participants in the study with the MSS. The team performed all measures together, to guarantee consistent outcome results during the study. There were no medical–ethical objections to the way in which the research was carried out (Politeknik Kesehatan Jakarta I), and the study was conducted according to the guidelines of the Helsinki protocol. All participants have given their written informed consent for participation in the research study.
Study participants
Initially, 5 persons were included in the region of Jakarta, and subsequently, 10 persons were included in the region of Bali. The initial study sample included 15 participants. However, after the initial fitting and completion of the prosthetic use questionnaire, one female participant withdrew due to pain and difficulty with mobility. The results reflect the final sample of 14 participants. These persons were conveniently selected by the prosthetists from the existing database of prosthetic users (Exceed Indonesia and Puspadi Bali). Inclusion criteria were persons having a unilateral trans-tibial amputation with a stump length of 10–30 cm, a distal circumference of less than 60 cm and bodyweight of under 160 kg according to the criteria of fitting for the MSS. Participants unable to independently keep their own stump and liner clean were excluded.
A total of 14 participants had a patellar tendon bearing (PTB) socket in combination with a pelite liner. One person had a thigh-corset (this person also had significant atrophy in the stump muscles). Participants needed to be able and willing to visit the prosthetic and orthotic centre for the follow-up measurements. Participation in the study was voluntary, and written informed consent was obtained from all volunteers. Participants were also informed that they were free to use their own prosthesis again at any time if they wanted to.
Materials
The MSS consist of fibre braid that is reinforced with resin. First, the residual limb is covered by a silicon casting liner with a distal connector and isolated with a layer of silicon sheath. Second, a glass fibre braid is then rolled on and a second layer of silicon sheath is applied. Finally, the Icecast bladder is connected to the distal connector, rolled on and pressurised by injection of air into the bladder. When the resin has cured, the proximal edge of the socket is trimmed and a pin locking system, pylon, foot and locking liner (i.e. the Össur Aspire kit) is assembled into a final prosthesis. The user’s previous devices were ICRC standardised PTB socket systems with supracondylar suspension and with either a Cambodian-made rubber SACH foot or an Otto Bock SACH foot. Since the MSS was not commercially available in Indonesia at the time, a direct cost comparison could not be done. The required material and equipment for the production of 15 MSS prostheses were sponsored by Össur.
Outcome measures
Outcomes were measured at the levels of performance, patient satisfaction and technical feasibility of the MSS (Table 1). The performance was measured using the standardised 2-min walk test (2MWT, 12 measures the distance walked in 2 min), the 10-m walk test (10MWT, 13 measures the comfortable walking speed) and a mobility and function questionnaire (self-made set of questions that measures the amount of hours the prosthesis is used and capability to perform certain activities).
Overview of measures used.
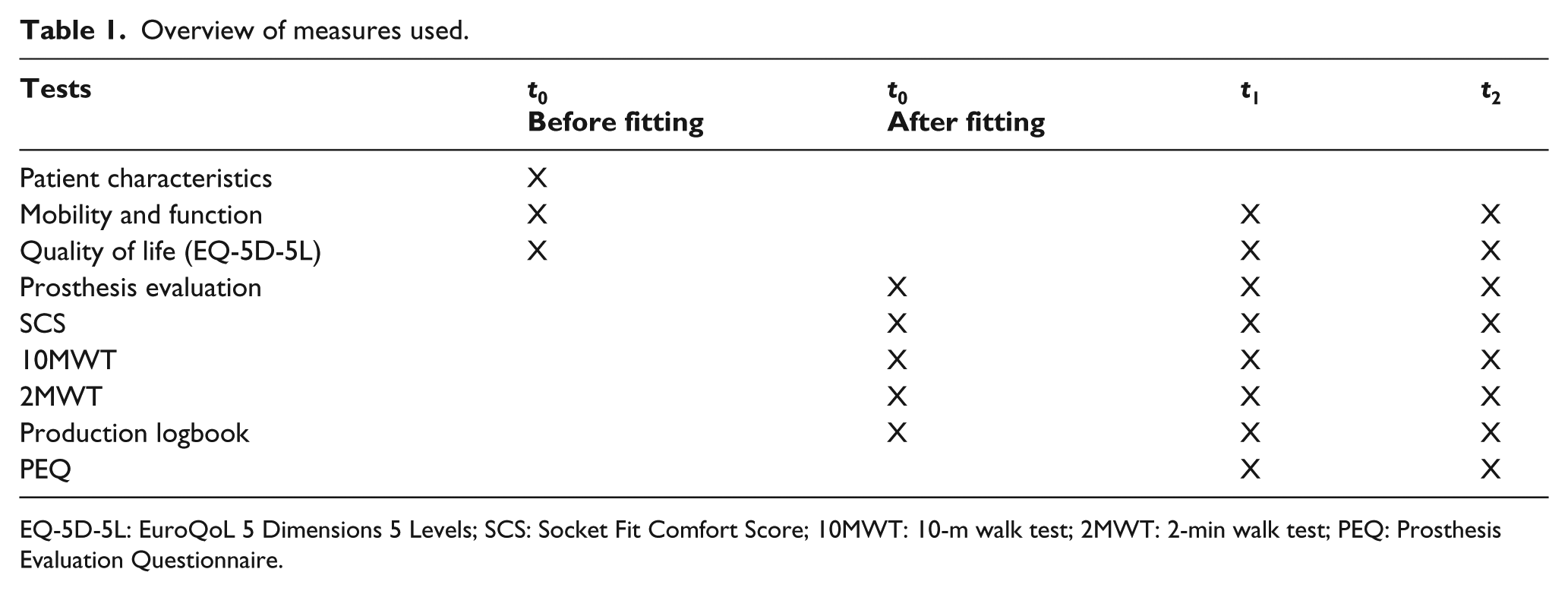
EQ-5D-5L: EuroQoL 5 Dimensions 5 Levels; SCS: Socket Fit Comfort Score; 10MWT: 10-m walk test; 2MWT: 2-min walk test; PEQ: Prosthesis Evaluation Questionnaire.
Patient satisfaction with the prosthesis was measured using the Socket Fit Comfort Score (SCS, 14 a numerical scale of 0–10, 0 = most uncomfortable socket fit you can imagine, 10 = most comfortable socket fit), an overall prosthesis evaluation score (a numerical scale of 0–10, 0 = not at all satisfied, 10 = very satisfied) and the Prosthesis Evaluation Questionnaire (PEQ). The PEQ consists of 83 questions comprising 9 validated independent subscales of which in this study 5 were included: ambulation, appearance of the prosthesis, residual limb health, prosthetic sounds and utility. 15
General health status was evaluated using the EQ-5D-5L (EQ-5D™ is a trade mark of the EuroQol Research Foundation 16 ). Health status is measured in terms of five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. The respondents rated their level of severity for each dimension using a five-level scale, and subsequently, the health state descriptions are converted into a single-index score (range: 0–1, the higher the index, the better the evaluated health status). The overall health status was evaluated using a visual analogue scale (EQ-VAS of 0–100, 0 = the worst health you can imagine, 100 = the best health you can imagine).
Technical feasibility was evaluated by having the prosthetists fill out production and maintenance logbooks. Those logbooks included a registration of the steps that were taken to produce and fit the prosthesis and the duration of each step. Prosthetists were also asked to report which tools they used. To prevent bias, the assessors did not have access to the initial assessment scores at the second assessment.
Procedure
The study was performed in three phases: fitting (t0), follow-up (t1) at 1–3 months post fitting and end evaluation (t2) at 4–6 months post fitting. The measurements taken at each time are presented in Table 1.
Because most subjects were non-English speaking, all questionnaires except the EQ-5D-5L were interviewer-administered by prosthetists who were fluent in both English and the local language that the participants were speaking. Answers were also translated back to English.
Data analysis
Shapiro–Wilk normality tests were performed and showed lack of normality only for the time needed for production. Therefore, mean and range were reported to describe the data. Differences between t0 and t2 were tested for significance with Student t-tests. Significance was set at p < 0.05 for all statistical tests.
Results
Study participants
In all 15 persons (n = 15) with a lower limb amputation participated in this study. The majority (n = 11) were male. The mean age was 37 ± 10 years and ranged between 23 and 5 years. Of the 15 participants, 13 suffered a traumatic amputation, while two participants had their leg amputated due to vascular problems. The two participants that were amputated due to vascular problems were relatively young (26 and 41 years of age at time of study), and community ambulatory, thus functionally comparable to the other participants with traumatic causes. All participants had previous experience with using a prosthesis. The average years of prior prosthetic use was 12 years (range 75 days–35 years). Measurements were taken directly after fitting with the MSS (t0) at 1.3 months (t1) and again after 4.6 months (t2). Detailed subject data can be found in Table 2.
Patient characteristics.
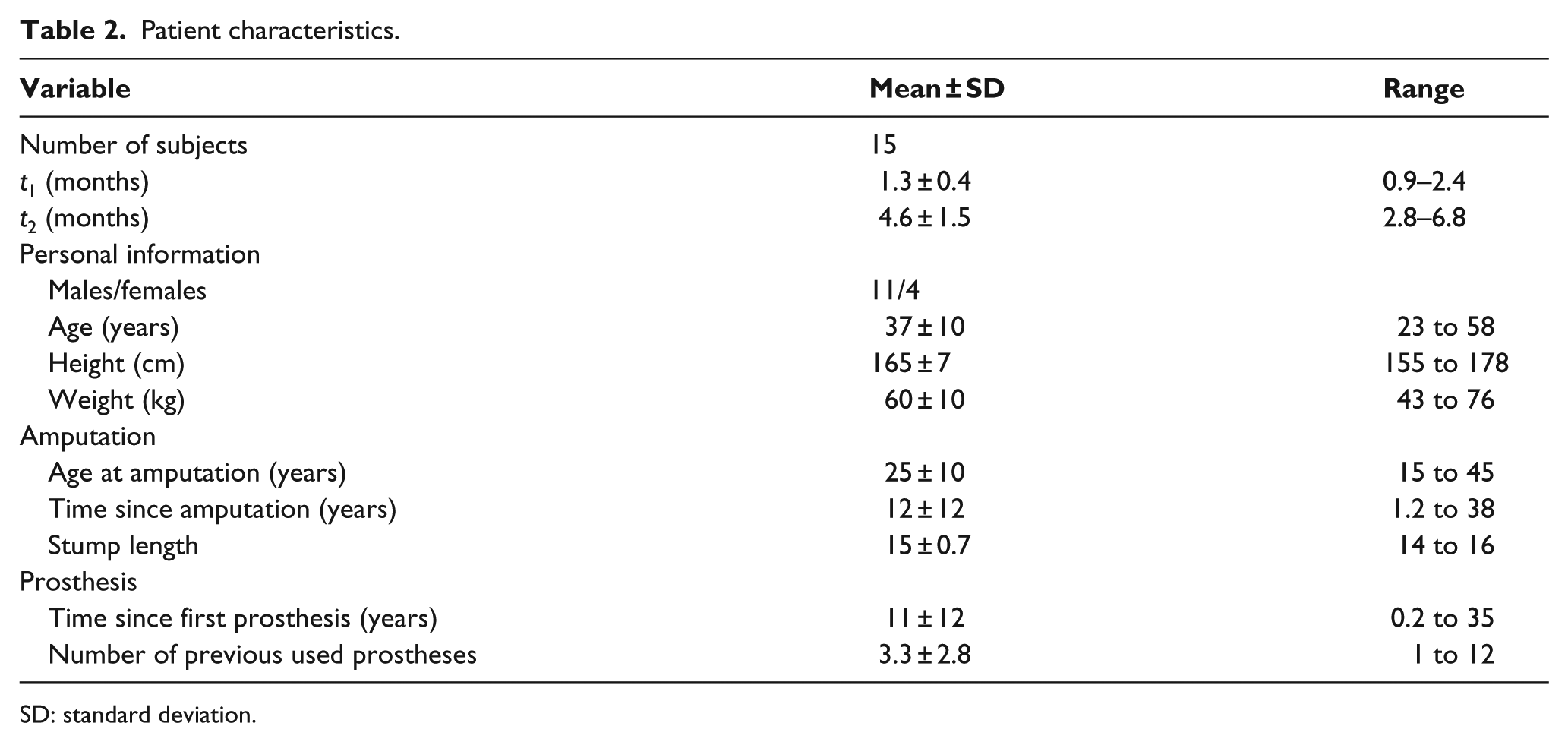
SD: standard deviation.
Performance
The mean distance walked in the 2MWT varied from 163.6 ± 30.1 m at t0 (after fitting), 157.8 ± 58.0 m at t1 and 162.0 ± 36.4 m at t2. The mean distance across all three measurements being 161 m. The mean walking speed measured in metres per second for the 10MWT varied from 1.17 ± 0.24 m/s at t0, 1.22 ± 0.27 m/s at t1 and 1.23 ± 0.19 m/s at t2 (Figure 1). When comparing the performance of patients using the MSS over time, no significant differences (p > 0.05) could be observed between t0 and t2.
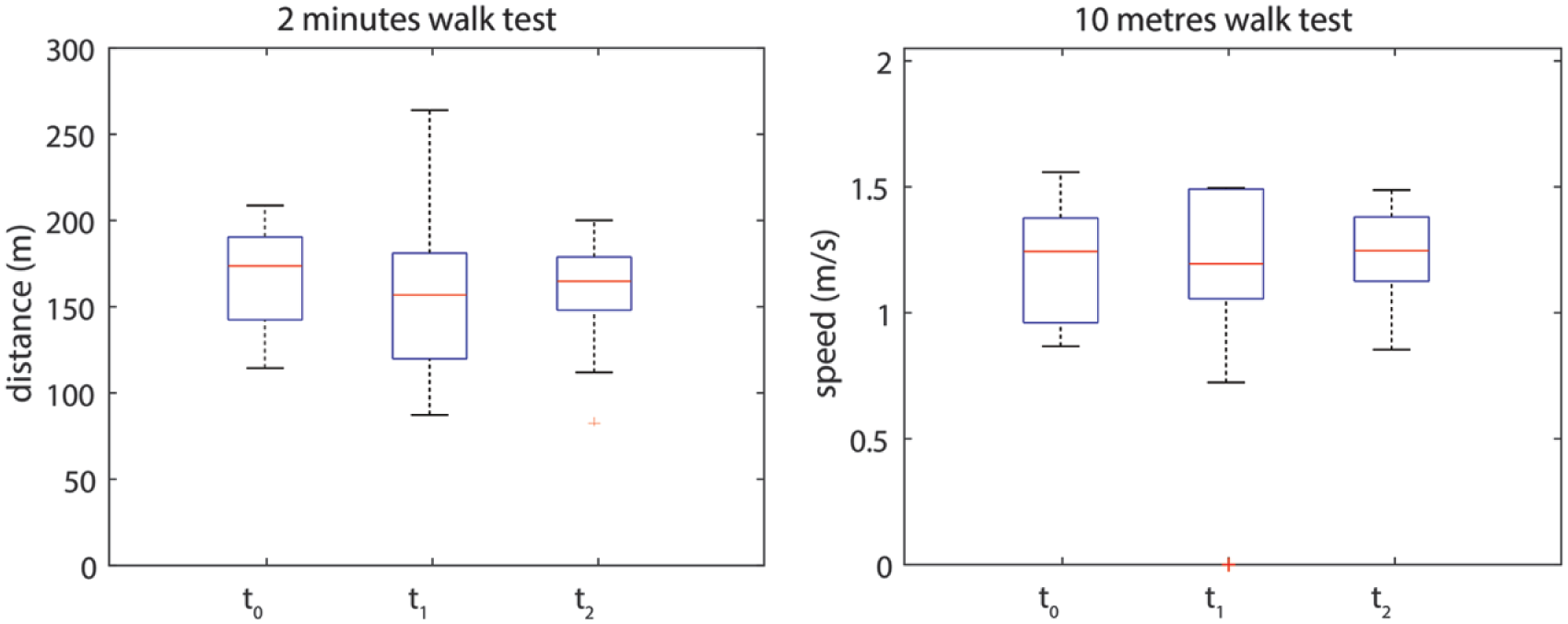
Results for the 2 min walk test (2MWT) and the 10 m walk test (10MWT).
The mean self-reported use of the prosthesis decreased significantly (p = 0.036) from 13.2 h at t0 with the previous prosthesis to 9.2 h at the first measurement (t1) with the MSS. It also decreased slightly between the first and second measurements with the MSS from 9.2 h at t1 to 8.1 h at t2 (Table 3). However, the self-reported ease of doing activities independently increased from 82% at t0 (previous prosthesis) to 89% at t1 (MSS), indicating that even though the prosthesis was used less, they felt more functionally independent while using it. This decreased back down to 81% at t2.
Results of prosthetic use questionnaire.
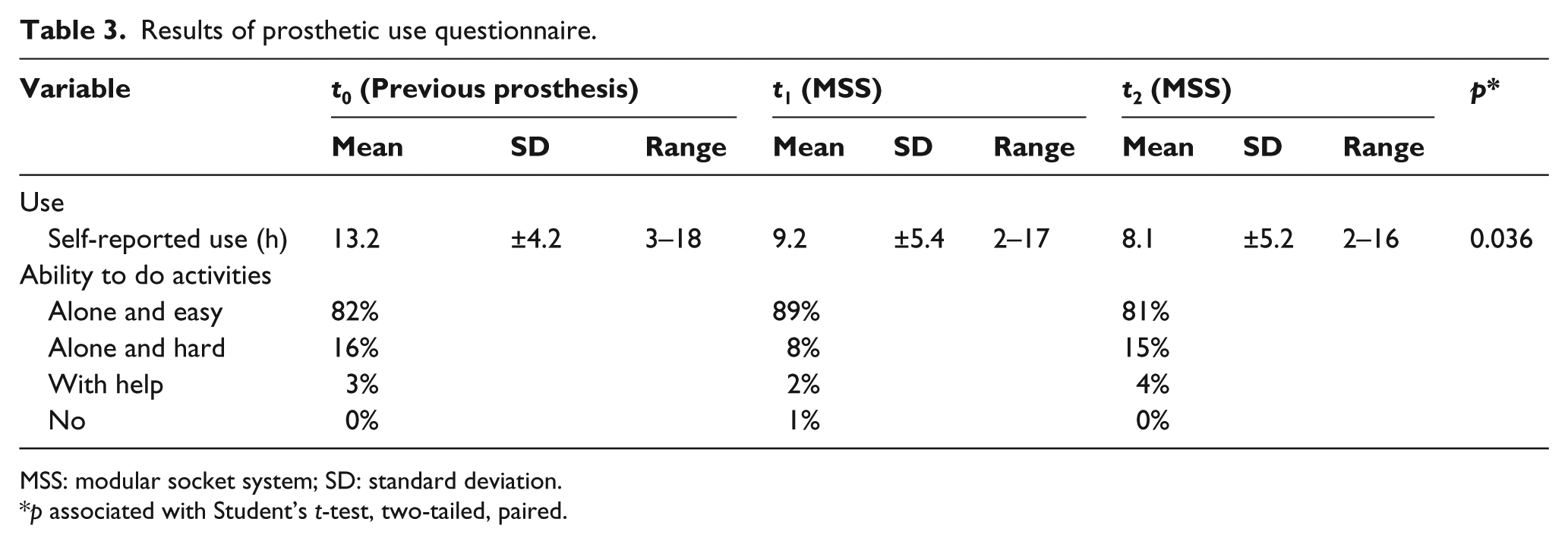
MSS: modular socket system; SD: standard deviation.
p associated with Student’s t-test, two-tailed, paired.
Patient satisfaction
The SCS decreased significantly (p = 0.027) from 8.1 ± 1.0 directly after fitting at t0 to 7.3 ± 1.5 at t1 and to 7.0 ± 1.3 at t2 (Table 4). When considering the EQ-5D-5L, the reported pain and discomfort frequency increased from 47% at t0 (previous prosthesis) to 60% at t1 (after fitting with MSS). This changed back to be comparable with the previous prosthesis score again at t2. This is also reflected in the increase from 13% to 27% in the frequency of reported problems with mobility at t1.
Results of evaluation of MSS prosthesis and quality of life.
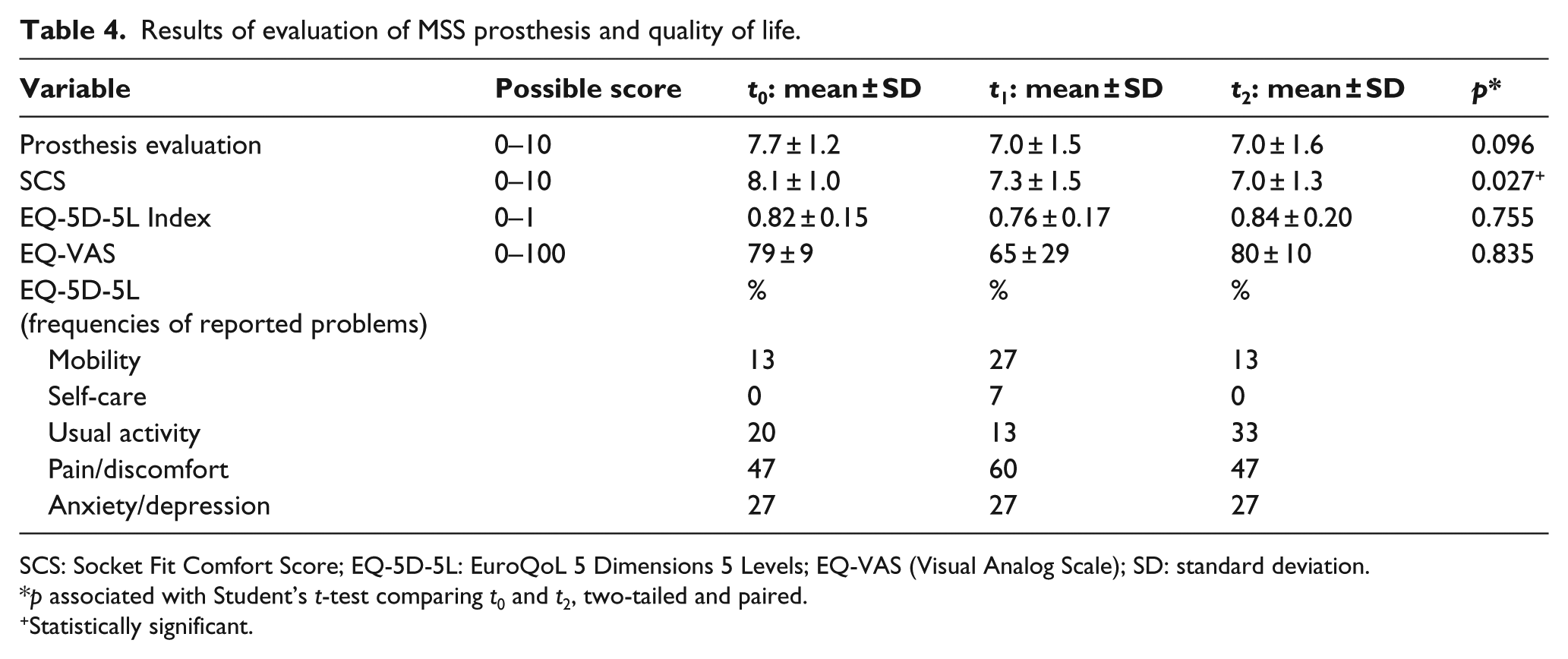
SCS: Socket Fit Comfort Score; EQ-5D-5L: EuroQoL 5 Dimensions 5 Levels; EQ-VAS (Visual Analog Scale); SD: standard deviation.
p associated with Student’s t-test comparing t0 and t2, two-tailed and paired.
Statistically significant.
From the PEQ, no significant differences in scores were found between follow-up (t1) and end evaluation (t2) for ambulation, appearance, residual limb health, sounds or utility (Figure 2).
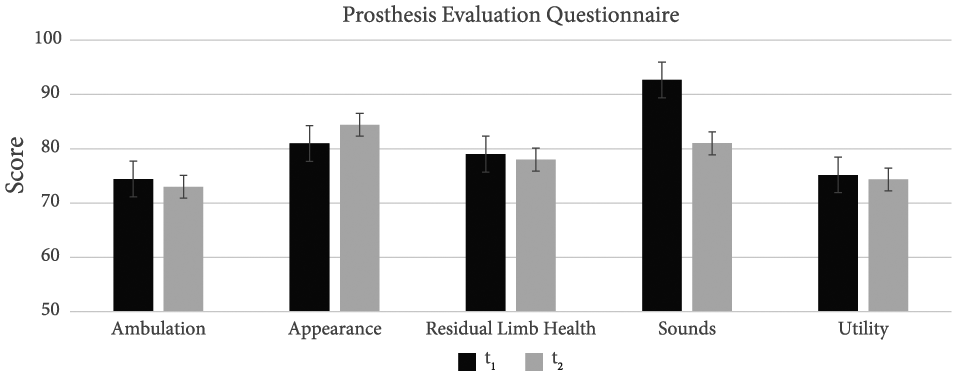
Prosthesis evaluation questionnaire.
Technical feasibility
Not all production logbooks were equally detailed, and identical production steps might have been documented under different names. The amount of time to fit an MSS to a patient took on average of 6.4 ± 2.6 h. Socket production 1.9 ± 0.5 h and prosthesis assembly and fitting 4.4 ± 2.6 h, with a range from 3.3 to 10.5 h. All sockets were completed in 1 day. In 10 out of the 15 cases, assembly of the complete prosthesis was finished that same day as well. The only nonportable machine needed for the production of the prosthesis was a grinding machine (router). Smaller portable machines that were used beside the Icecast® system were a cast cutter or jigsaw.
Discussion
The aims of this study were to evaluate the patient’s performance when using the MSS, the patient’s satisfaction regarding the use of the MSS in a rural setting, and the technical feasibility of the MSS for implementation in a CBR setting in terms of required tools, skills and required production time.
Patients’ performance
Considering the relatively young age, cause for amputation and experience with using a prosthesis, participants were expected to perform well with the use of the MSS. Walking speed and distance walked in 2 min were used as outcome measures to evaluate performance with the MSS. The average walking speed was comparable to the comfortable walking speed measured in other groups of persons with trans-tibial amputations (ranging from 1.0 17 to 1.2 m/s17–19) and slightly lower than the comfortable walking speed measured in healthy adults in a similar age group (1.2 vs 1.5 m/s18,20). The average distance of approximately 160 m recorded in this study during the 2MWT is much higher than the 69.9 m reported by Brooks et al. 12 and 114 m by Resnik et al. 21 However, age is considered as a strong effector on the walking distance, 22 and the participants in this study were much younger (37 vs 65 years).
The self-reported use of the MSS prosthesis was lower compared to the old prosthesis that people used (p = 0.036). It is not uncommon that the self-reported use of a prosthesis is overestimated. The possible reasons for this finding were not studied. One hypothesis is that the silicone liner used with the MSS could have caused sweating and discomfort in the hot and humid environment of Bali and might have been less comfortable on the skin than a pelite liner. Sweating and itching is a commonly reported complication of the use of a silicone liner, which could have been exacerbated by the heat. 23 An older study by Lake and Supan 24 also reported an increase in the incidence of sweating and irritation experienced when switching from a different liner to a silicone liner and in the younger population. This possibility is supported by the fact that the SCS in this study also decreased slightly over time. This is similar to the findings of Ennion et al., 25 who studied the use of a direct lamination application socket (a component of the MSS) in a similar sub-tropical setting in South-Africa. However, in an older study investigating correlations between body image, satisfaction with prosthesis and prosthesis wearing time, no significant correlation could be identified between satisfaction with prosthesis and wearing time. 26
Patients’ satisfaction
Participants in this study were generally satisfied with their prostheses. The reported health index was comparable to the norm values reported by people in Thailand. 27 In line with what was expected from this population of experienced prosthetic users, no decline in satisfaction was noted over time from the PEQ. The general health status as measured with the EQ-5D-5L did not change significantly over the duration of the study. The SCS decreased over time (t0 = 8.1 ± 1.0; t1 = 7.3 ± 1.5; t2 = 7.0 ± 1.3), but remained above the average threshold score of 5.7 for requiring adjustment of the socket. 14
Technical feasibility
Finally, the technical feasibility of providing the MSS in a rural setting was considered. The measurement, manufacturing and fitting of the socket could in most cases be performed within 1 day, (as opposed to several visits with the traditional socket) making it ideal for use in a rural setting. The clinical relevance of this finding is that patients who normally have to travel long distances to access prosthetic services were only required to make one visit to the health facility in order to receive a prosthesis, improving their access. The use of the MSS can also provide an alternative solution to deep rural areas where prosthetists only visit once every few months, such as in the rural settings of South Africa. 25
The biggest electric tool that was required during the manufacturing of the MSS was a router machine. All other tools were handheld. Although the use of a router machine may not be suitable in rural settings, it is plausible to assume that a handheld rotary tool can be used as an alternative; a portable generator could then be used in settings where electricity is not available.
There is a scarcity of professional prosthetists who can provide services to rural areas. 4 Although cases are known where local prosthetic service delivery is provided successfully, it requires a well-organized network of professionals to create sustainable individually tailored prosthetic and orthotic services. Even though according to the existing literature the MSS is more costly than the traditional PTB plaster casting technique to manufacture, it could optimise the productivity of the limited number of prosthetists servicing rural areas. 25
Provision of a prosthesis is a part of the rehabilitation process and after care and education can be considered equally important. Especially in a rural setting after care can be challenging, and who should provide this remains elusive. Despite the MSS being both technically and functionally feasible for mobile production, a strong organisation of health care is needed before implementation in a rural setting should be considered.
Limitations
The cause of amputation has a big influence on the recovery or function of the patient post operation. The most common cause for amputation for the participants in this study was related to trauma. This might have biased the performance scores in this study when compared to other studies where vascular problems are reported as main cause.18 –20
Since the participants were recruited from users who presented themselves at the clinic with discomfort in their prosthesis, determination of PEQ, SCS, 2MWT, 10MWT and prosthesis evaluation scores would have been meaningless. The fact that no comparison can be made between the MSS and the previous prosthesis can be considered a limitation.
A large variety of Indonesian dialects are spoken in Bali, but the language Bahasa was the closest to most. The questionnaires were translated from English and Bahasa and then adapted to the individual user’s specific dialect by the prosthetists (who were fluent in most dialects as well as English and Bahasa) when required. Subsequently, the prosthetists translated the user’s expression back towards English. Due to the multiple translations required, it was difficult to standardise terminology.
The interviews were administered by the same team that fitted the subjects with the MSS prostheses. This unblinds the research which might have influenced the judgements of both the researchers and the subjects. Supervision by the head of the department was supposed to have decreased, but not eliminated completely, the risk of bias.
Conclusion
The use of the MSS in a rural setting can be considered feasible in terms of performance, patient satisfaction and manufacturing time. It is worth noting that even though it cannot be directly correlated with prosthetic satisfaction, the self-reported use of the MSS prosthesis was lower compared to the old prosthesis that people used and the SCS decreased slightly over time. The measurement, manufacturing and fitting of the MSS socket could in most cases be performed within 1 day. Although the prosthetists reported that they used a non-portable router, there are adequate portable routers that can be used which would make the methodology technically feasible in a rural setting.
Footnotes
Acknowledgements
The authors thank I Nengah Latra from Puspadi Bali for providing the perfect case for this study, the involved prosthetists from Exceed Indonesia for their careful collection of data, Dr Jusuf Kristianto of the Indonesian Ministry of Health for support and guidance of the study and Eline Kolk for editing the manuscript.
Author contribution
Not all authors contributed equally in the preparation of this manuscript. Giesberts, Ennion and Bergsma worked together in writing the paper. Hjelmström, Karma, Lechler and Hekman reviewed the paper.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Össur sponsored the material for the manufacturing of 15 prostheses.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.