
Abstract
Background:
Prosthetic services, including the provision of an appropriate prosthesis, are a crucial part of the rehabilitation process for individuals with lower limb amputations. However, globally there exist unique challenges in the delivery of prosthetic services that are limiting rehabilitation outcomes and consequently the well-being and socio-economic status of individuals with lower limb amputations.
Objectives:
The objective of this work was to explore the issues related to the provision of appropriate prosthetic technologies and to compare these across different economies of the world.
Study design:
Cross-sectional survey.
Methods:
An online survey was developed and distributed to prosthetic practitioners providing services in countries around the world. An open-coding thematic content analysis procedure was applied to extract key themes from the data.
Results:
The response codes defined three overall themes of lower limb prosthetic delivery, and several key differences between higher and lower income countries emerged. Namely, a higher emphasis on part/material availability, practitioner training and durability in lower income countries was found. High costs were an issue raised by practitioners in all countries.
Conclusion:
Practitioners around the world share many of the same concerns; however, some lower income countries face important and pressing issues that limit their ability to provide adequate prosthetic services.
Clinical relevance
This work highlights the most crucial service and technology-related needs, as perceived by trained prosthetic practitioners, of populations requiring lower limb prosthetic treatment around the world. Additionally, the results may be used to prioritize prosthetic-related health-care initiatives led by other researchers, governments and organizations working to improve services internationally.
Background
For individuals with lower limb amputations (LLAs), the provision of a functional prosthesis is an important part of the rehabilitation process, facilitating mobility and with it physical, recreational and occupational activity. However, around the world and especially in lower income countries (LICs), great challenges persist in the delivery of prostheses to those in need; based on recent estimates, there are globally 25 million people without access to basic prosthetic and orthotic services. 1 Without prostheses, individuals with LLAs experience major mobility limitations and thus are stripped of many basic rights including access to food, shelter, education, work and the ability to earn a living, as well as equal opportunities and citizenship within their communities. 1
As with other global health issues, three barriers can influence the availability of adequate prosthetic services. 2 The first barrier is where a solution to a health problem does not exist, and therefore, a scientific or technological advancement is needed. The second barrier is where a solution exists, but is not accessible, for example, due to high cost associated with its broad implementation. The final barrier is where a technology exists and is accessible, but is not adopted, for example, due to cultural resistance. Key elements associated with these barriers have been identified within the international prosthetic community, including the limited resources that are available to provide adequate prosthetic care and poor access to appropriate prosthetic technologies and trained personnel to ensure that devices are optimally set up and applied.1,3,4 This aspect of prosthetic care is effectively summarized in the well-accepted definition of ‘appropriate technology’, which is ‘a system providing proper fit and alignment based on sound biomechanical principles which suits the needs of the individual and can be sustained by the country at the most economical and affordable price’. 5
While the above definition provides an important starting point, a deeper and more complete understanding is needed to efficiently apply and prioritize efforts aimed at facilitating the delivery of more effective prosthetic services and technologies around the world, especially in severely under-resourced regions. The literature identifies important attributes of appropriate prosthetic technologies including function, cost, durability and others, but it is not clear which of these are the most important to address and therefore should be given priority.3,5 –8 Given the limited resources, it is necessary to target and combat the most critical barriers that are presently limiting the provision of appropriate prosthetic services and technologies around the world. In this way, it may be possible to most effectively improve prosthetic outcomes across a larger proportion of the population of individuals with LLAs.
Several initiatives have tried to assess the current state of prosthetic services and technologies through surveys or focus groups; however, these approaches have often been limited to a single country and therefore are unable to provide a global perspective.9–12 There have also been a number of literature and conference reviews which have investigated different aspects of prosthetic services, but these are limited to examinations of published literature or are based on small groups of experts including researchers, whose experiences and opinions may not necessarily reflect those working on the front lines.6,13,14 While these studies provide important information, it is likely that the scope of the problem has not yet been fully captured. In this regard, the overall objective of this study was to explore the issues related to the provision of appropriate prosthetic technologies and to compare these within different economies of the world. It was hypothesized that there would be both universal issues spanning the prosthetic industry as a whole and also issues that are highly dependent on regional economies. This work aims to provide a global perspective on the delivery of prosthetic services for individuals with LLAs and to direct future researchers on their efforts to deliver more effective prosthetic devices and treatments. Additionally, the goal is to identify priority areas for governments and organizations working to improve prosthetic-related health-care services around the world.
Methods
The survey
A cross-sectional survey on lower limb prosthetics was developed to be answered by practitioners working in the field of lower limb prosthetics. The reason for sampling practitioners rather than prosthetic users themselves was because it was felt that the former would be more consistently familiar with the technical and service-related issues. Intended survey participants included prosthetists, orthotists, technologists, technicians and others with experience in treating persons with LLAs. Ethical approval was obtained through the Research Ethics Board at the authors’ institution. Consent was considered implied by the submission of the survey responses.
The content for the survey was developed by reviewing literature dealing with issues pertaining to prosthetic technologies, including conference proceedings and journal articles 3,6,8,10 as well as input from certified prosthetists based at the researchers’ institution. Iterative refinement between the investigators and a pilot group of three prosthetists led to a version of the survey comprising six main sections representing the following categories: (1) Demographics, (2) Knees, (3) Feet, (4) Alignment, (5) Sockets & Suspension and (6) General. Section (1) identified the relevant information on the training and responsibilities of the respondents and the range of services currently provided to patients at their facility. Sections (2)–(5) were designed to identify service or technological issues relating to the lower limb prosthetic systems most commonly used at each respondent’s facility. Section (6) was designed to capture broader, or any remaining, issues with prosthetic treatment in general. The survey consisted of both closed- and open-ended questions. This article focuses on the results of the open-ended questions which included ‘If you feel there are any major problems or issues with existing prosthetic knees, please provide information here’; this question was repeated four times, replacing the word knees with feet, then alignment techniques or systems, sockets & suspension systems and finally systems as a whole. A final question, question 6, was ‘If you have any other final comments on any aspect of lower limb prosthetics, please provide this information here’. Once finalized, the survey was translated from English into Spanish and French, as these are the top three most influential languages. 15 The survey was provided electronically using an online survey tool (FluidSurveys).
Participants
To achieve a global scope, the survey was distributed to practitioners using the contact networks of the International Committee of the Red Cross (ICRC), the International Society for Prosthetics and Orthotics (ISPO), Handicap International (HI), Fédération Africaine des Techniciens Orthoprothésistes (FATO), the Canadian Board for Certification of Prosthetists and Orthotists (CBCPO), the Orthotics & Prosthetics Listserver (O&P-L) and other individuals working in the field of lower limb prosthetics. An invitation email with a link to the survey was initially sent out and the survey was made available for 3 months; after 6 weeks, email reminders were sent out to practitioners who had not yet completed the survey.
Data analysis
All open-ended responses were retyped verbatim for each participant and, where necessary, translated into English. Typos and spelling errors were corrected. We applied an open-coding thematic content analysis procedure to the data,16,17 whereby three investigators (two trained in rehabilitation engineering with specializations in prosthetics and one trained in health sociology and qualitative methods) independently reviewed each response, coding line by line while noting key themes and patterns. The research questions guided the analysis in the formation of key categories. The investigators compared and contrasted the themes and their relationships between each other. All codes were re-read and compared with each other in a constant comparative method. 17 Any discrepancies were resolved through discussion among all investigators. Using an iterative process, codes were then organized according to those with similar meanings.
Responses were categorized by country into a low- and lower-middle-income group and an upper-middle- and high-income group. Country income grouping was determined from the July 2012 World Bank list of economies, which allowed for a comparison of issues within each major category of lower limb prostheses (i.e. Knees, Feet, Alignment and Sockets & Suspension) based on an economic context. Additionally, responses from the questions on the general issues in lower limb prosthetic services were compared across each country income level. Representative direct quotes of each key theme were abstracted while considering the whole context of the participant’s response. An audit trail of key decisions made during the analysis was kept. This along with peer examination helped to establish the trustworthiness of the findings.16,17
Results
The survey was accessed by 400 individuals resulting in 192 fully completed surveys and 39 partially completed surveys, which were all used in the analysis. The total number of professionals invited to complete the survey is impossible to know because respondents were encouraged to further distribute the survey to colleagues or other working professionals. However, of the subset of 512 individuals who were emailed directly, 143 completed the survey marking a 28% completion rate among those directly mailed. In the responses, 64 different countries were represented. The demographic data of the respondents are summarized in Table 1. Response rates ranged from 13% for the section on alignment to 91% for the section on feet.
Respondent characteristics.
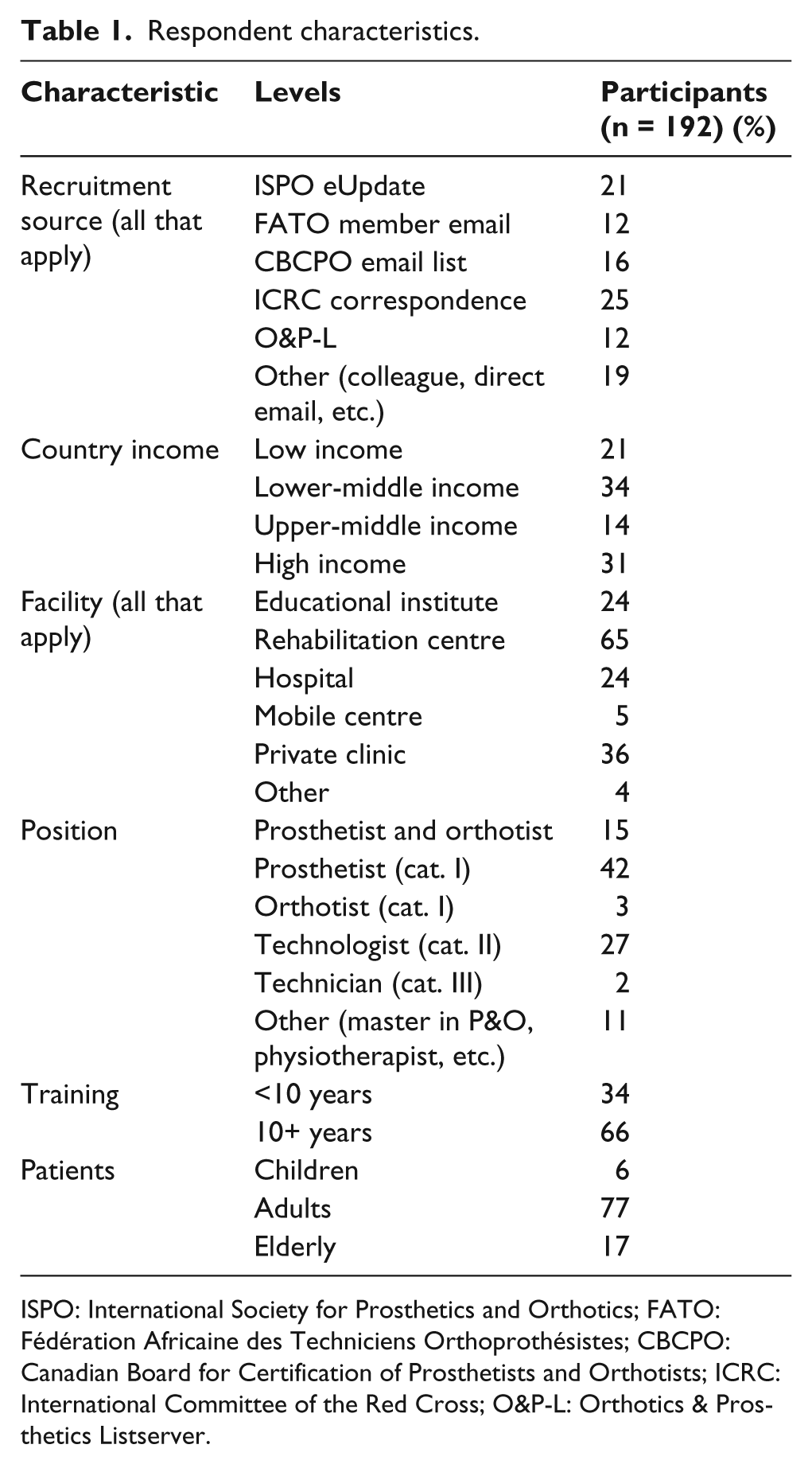
ISPO: International Society for Prosthetics and Orthotics; FATO: Fédération Africaine des Techniciens Orthoprothésistes; CBCPO: Canadian Board for Certification of Prosthetists and Orthotists; ICRC: International Committee of the Red Cross; O&P-L: Orthotics & Prosthetics Listserver.
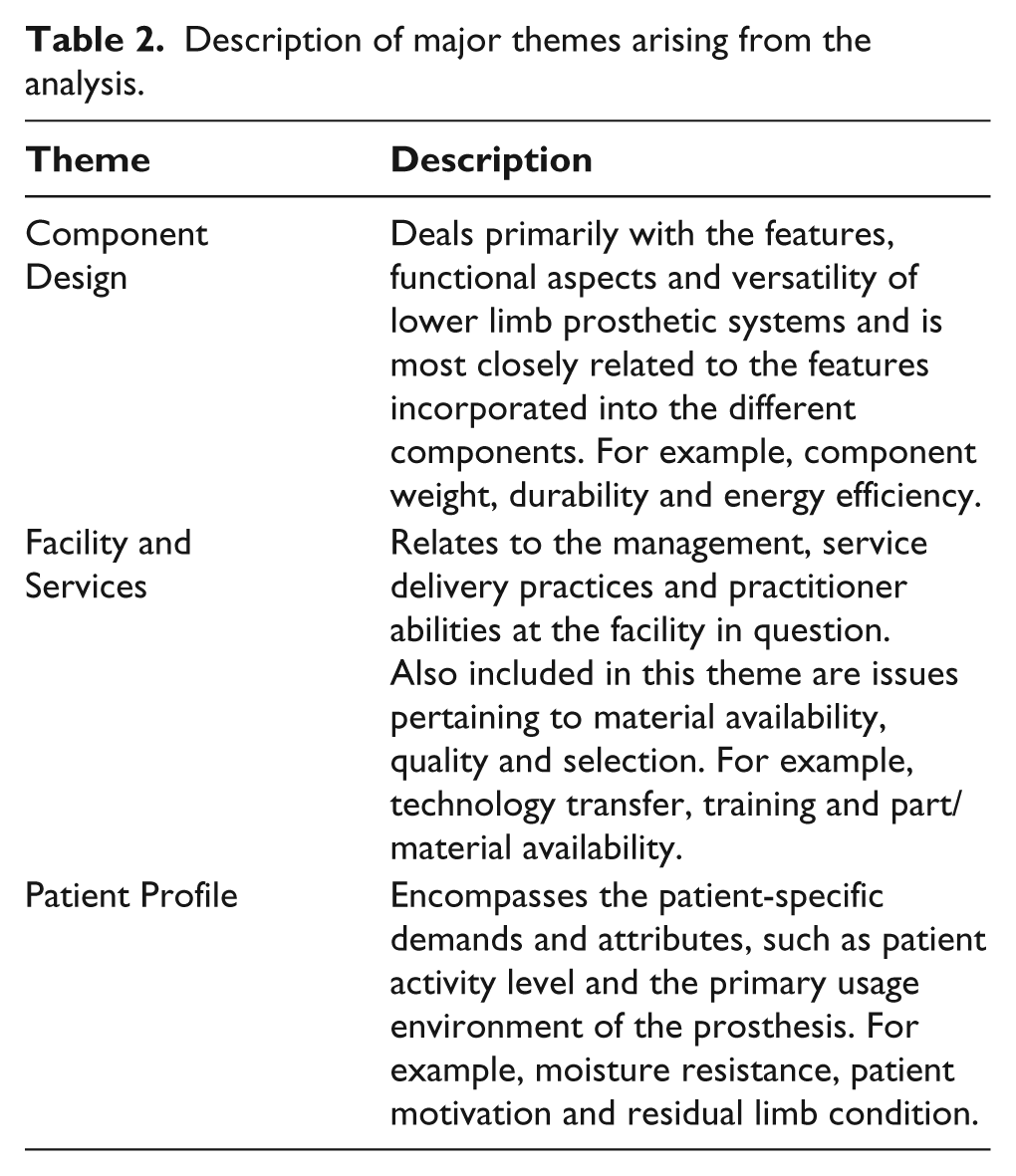
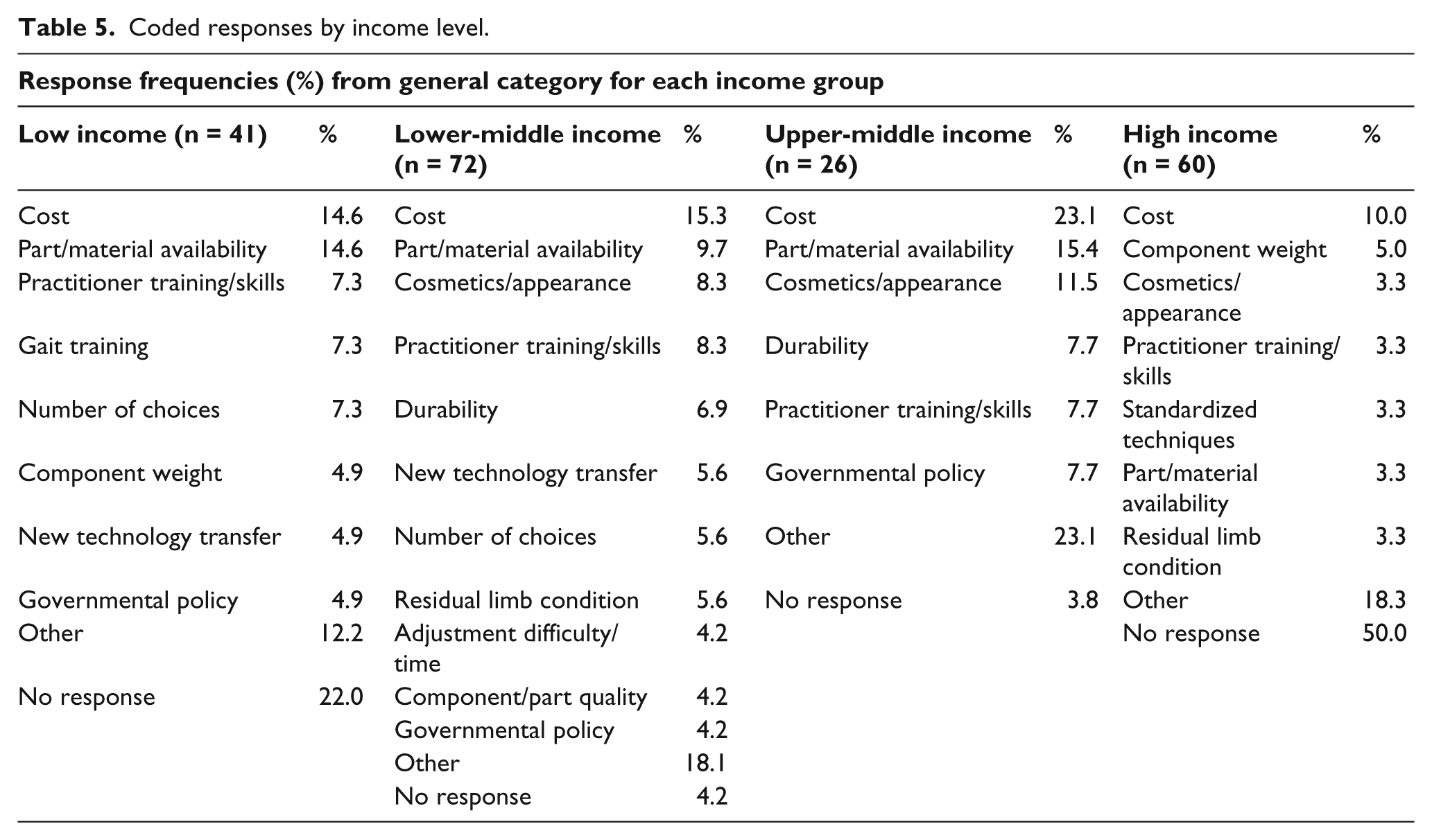
Three themes emerged from the analysis of these written responses: Component Function, Facility & Services and Patient Profile; these are each described in more detail in Table 2. The coded responses were then organized according to the four prosthetic categories (Knees, Feet, Alignment and Sockets & Suspension) and country income level (low/lower-middle income and upper-middle/high income) and then ordered by percentage of responses, as shown in Tables 3 and 4. In Table 5, the combined responses to the question on prosthetic systems as a whole and question 6 on general issues from respondents working in each country income group are presented. Finally, some representative responses from each section are shown in Table 6 where respondents are described by their respondent number, country (income level), job title, years of experience and type of clinic.
Description of major themes arising from the analysis.
Coded prosthetic category responses from low- and lower-middle-income countries.
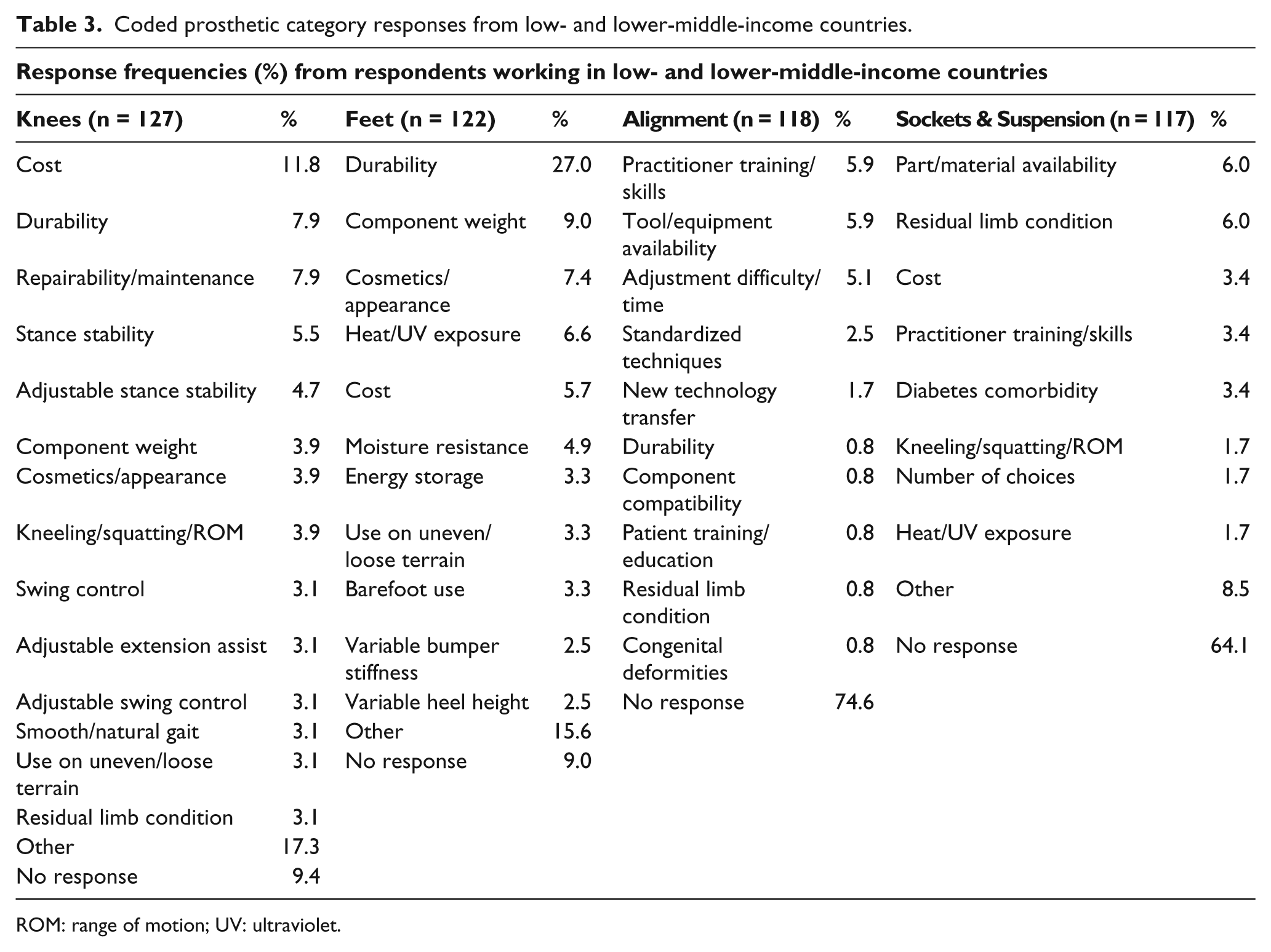
ROM: range of motion; UV: ultraviolet.
Coded prosthetic category responses from upper-middle- and high-income countries.
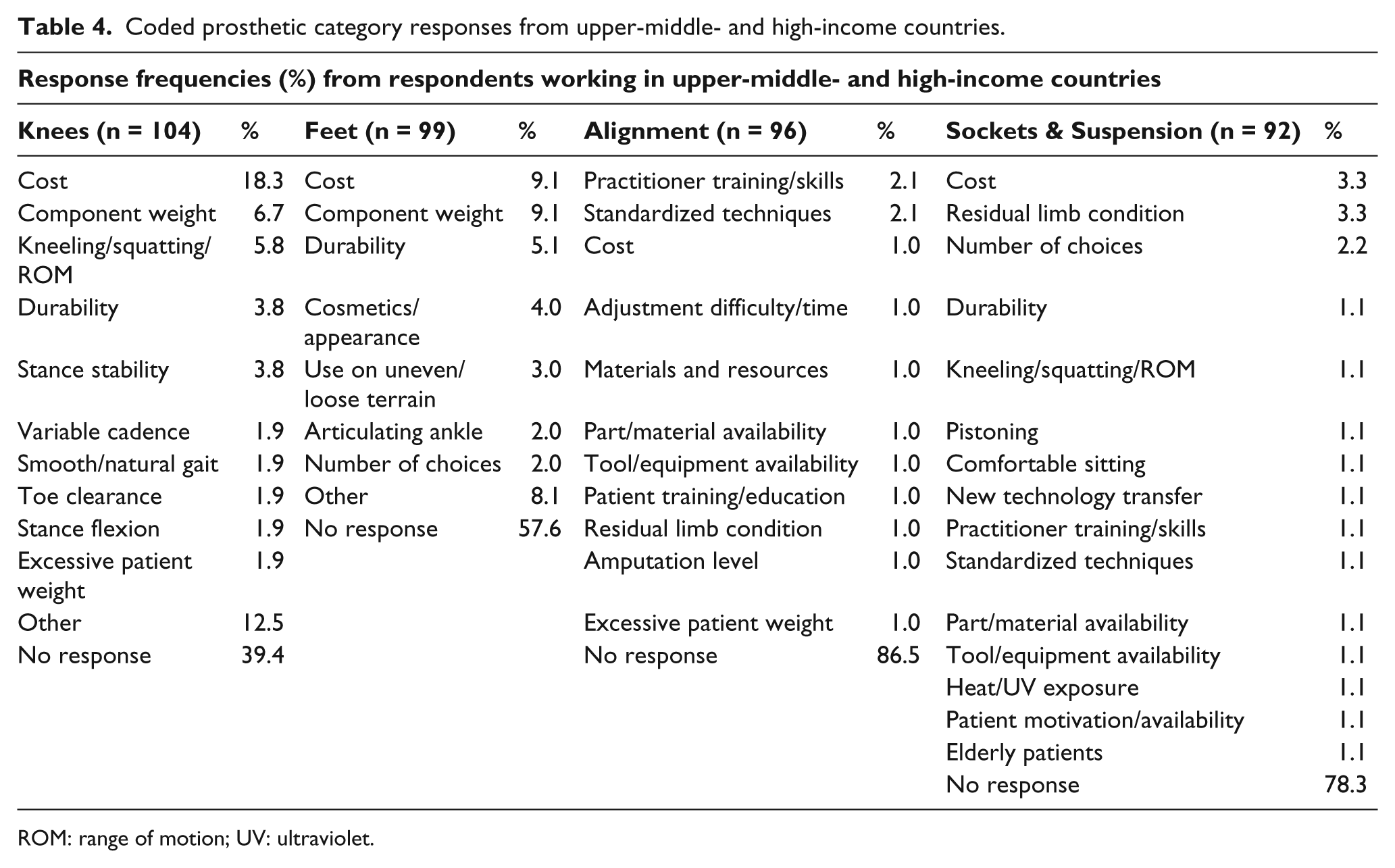
ROM: range of motion; UV: ultraviolet.
Coded responses by income level.
Representative responses from each prosthetic category.

Discussion
This study was designed to compare the top issues in different aspects of lower limb prosthesis delivery between services rendered in low- and high-income countries. Most research has primarily been focused on one end of the income spectrum, so this study has provided a unique set of comparative data with a global perspective. The first notable difference between the two income groups was that the lower income group had higher response rates, 66.8% compared to 40.5%. This may be suggestive of the respondents’ acknowledgement of more widespread or pressing issues in lower versus higher income countries. The response rates of each prosthetic category also revealed that for both the higher and lower income groups, the Knees and Feet categories showed the highest response rates, followed by Sockets & Suspension and finally, Alignment showed by far the lowest response rate. These are important new insights about potential prevalent issues in the delivery of prosthetic services, especially in LICs, relating strongly to the availability of appropriate components (i.e. Component Design). Additional insights are presented below individually for the predefined prosthetic categories (Knees, Feet, etc.), based on the three themes that emerged from the qualitative analysis: Component Design, Facility & Services and Patient Profile. These themes neatly encompass the different kinds of considerations to be made in the provision of prosthetic rehabilitation.
Knees
The knee is a very complex part of the prosthetic system, and its level of function has a significant influence on its overall success; this is reflected by the high number of codes from the Component Design theme. Cost was the top issue with knees in both the higher and lower income groups; however, for the higher income group, cost was much more highly ranked than any other issue. Among the LICs, a strong emphasis was also placed on Durability, Repairability and Stance Stability as summarized by one respondent’s comment: ‘The single axis CR prosthetics knees we have been using … don’t offer constant knee security at stance phase. Those knees are difficult to repair when exposed to any mechanical stress’ (Respondent 29) and as has been previously reported in terms of mechanical, structural and functional issues found in knee joints designed specifically for LICs.18,19 As a whole, these results highlight that technological advancements are needed to develop simple knee mechanisms that are functional, durable, easy to maintain and cost-effective and are supported by views of researchers and experts identifying the lack of an appropriate knee joint technology for developing countries.3,8 Such a technology does not yet exist, representing the first barrier in global health, as outlined by Howitt et al., 2 and has led to work on specific technologies by researchers aiming to address this need.20,21
Feet
The Component Design theme is also prominent within the Feet category; however, a number of Patient Profile codes are also present at the top of the list. Cost, Component Weight, Durability and Cosmetics/Appearance are the top four issues, with prosthetic feet among the higher income group; these are also the top issues with the lower income group; however, Durability stands out much higher than the rest and Cost is less important. In 2006 at a conference on prosthetic technologies for developing countries, experts agreed that the minimum acceptable amount of time a prosthetic foot should last in the developing world is 1 year, with 5 years being optimal. 8 However, due to the Patient Profile usage environment codes, heat/ultraviolet (UV) exposure and moisture resistance contributing negatively to the durability of prosthetic feet, multiple respondents are claiming shorter service lives: ‘In very hot place like Sudan this feet’s are easily breaks even in some cases less than 3 months’ (Respondent 110). These issues with durability, especially in hot and humid climates, have also been reported elsewhere.3,22 The inability to use the feet without shoes was also raised by some respondents in the lower income group as was cosmetic appearance. Respondents complaining about the cosmesis of prosthetic feet indicated that manufacturers should provide a wider range of colours and sizes and smaller, more feminine looking feet. Appearance can have a profound effect on patient satisfaction with a particular prosthesis and is considered a strong motivator for the continued use of the prosthesis.23,24 This is an example of the third barrier in global health where, in some cultures, the stigma associated with disability is a barrier in itself, and concealment of the disability is desired. However, this higher level barrier is only relevant in the case where the first and second barriers can be addressed first. 2
Alignment
This section had the fewest respondents, though Practitioner Training/Skills was the top item for both income groups. Poor prosthetic alignment has been widely reported in many LICs,4,8,18 which is largely attributed to deficiencies in the training of personnel. 1 Recommendations made by a panel of experts included defining what ‘acceptable alignment’ is and developing a tool to help novice prosthetists identify and correct misaligned prostheses. 8 These suggestions also relate to the Standardized Techniques, Technology Transfer and Tool/Equipment Availability codes, which were each rated higher by the lower income group and suggest that the problem of poor alignment in LICs is related to more than just poor training. Systems and tools to aid the alignment of prostheses must be economically and technologically appropriate for these regions, highlighting the necessity to overcome barriers 1 and 2 relating to global health.
Sockets & Suspension
Sockets & Suspension is an aspect of lower limb prosthetics that encompasses each of the three major themes, though, unsurprisingly, the Residual Limb Condition is the top issue in both income groups. The condition of the residual limb is influenced by a number of factors, including the cause of amputation, surgery outcomes and post surgery rehabilitation, 25 most of which are outside the control of clinicians. As with Alignment, availability of materials and components was a more significant issue in the lower income group. Diabetes comorbidity was raised as an issue with respect to Sockets & Suspension by the lower income group though not by the higher income group. This difference supports the reported growing trend of peripheral vascular diseases in developing countries leading to amputations26,27 and may also highlight a lack of effective medical treatments. Finally, based on the results here, practitioner training and skills are seen to play an important role in achieving good socket fit, a requirement that may be partially alleviated via simpler socket fabrication techniques, 25 such as the Center for International Rehabilitation (CIR) sand casting technique or the use of computer-aided design–computer-aided manufacturing (CAD-CAM). 3
General
In high-income countries, the availability of appropriate prosthetic technologies and trained personnel is lesser of a barrier than in LICs, but the high cost associated with prosthetic services and components was the top issue in all countries and economies. It has been shown to be a top priority by a number of studies focusing on developing countries.4,28 While very few studies focus on the cost of prostheses in the developed world because of the variability in governmental support, private insurance coverage and cost of available devices, from the qualitative responses of this and other studies, it is clearly still a significant issue for many patients. 29 Hence, relating to the second barrier in global health, greater access needs to be given to existing prosthetic services and technologies by significantly decreasing costs, especially in LICs. This may be accomplished by implementing innovative business and health-care delivery models, aiming to improve the efficiencies associated with manufacturing and distribution and consequently the provision of prosthetic care. For other examples of strategies that have been successfully utilized in other areas of health care, the reader is directed to Howitt et al. 2
Another interesting general trend emerged involving Part/Material Availability, which was shown to be a major issue for all but the highest income group. This could be a reflection of higher relative costs of materials and supplies or otherwise indicative of problems in distribution and a reliance on non-local materials. This is highlighted by a respondent’s complaint relating to the certifications some companies require for purchasing their products: ‘Large international companies are focusing on the development of “high tech” components and materials, while “blocking” the prosthetic developer by requiring expensive certifications to use their components …’ (Respondent 81). Another respondent mentions the difficulty in obtaining specific materials:
In some countries it is very difficult to obtain even the most basic materials and components for prostheses at a reasonable cost. For example, in Sierra Leone it was difficult to obtain plaster of Paris (bulk and bandages, liquid plastics, and durable components) (Respondent 193)
supporting the results from a similar study focusing only on practitioners within Sierra Leone. 12 However, this appears to be a more widespread problem, as Bigelow et al. 4 report on services in Haiti: ‘Unavailability of prosthetic treatment is partly due to the lack of trained professionals in the field of prostheses, partly due to a lack of supplies, and partly due to a lack of governmental support’. In these areas, where the correct part or material is unavailable, practitioners and patients must settle with what is available, as a respondent from Sudan states, ‘Where resources are limited many patients take what’s available even if it does not conform with activities, age and general health’ (Respondent 57).
The problem of practitioner training, which was raised by a higher percentage of respondents from LICs than those in the high-income group, also relates to the need for updating and retraining practitioners in LICs. This lack of familiarity with newer technologies and techniques has been documented in other studies.4,12 Issues with the transfer of new technologies to different regions can also be a reflection of the inappropriateness of the new product or component in the new regional context, such as prosthetic feet incapable of withstanding the heat and humidity of many warmer regions. Companies promoting their products and easier access by patients to product information have put pressure on some practitioners to serve the patients’ demands for more sophisticated products, which may in fact be inappropriate, as stated by one respondent:
Companies promoting components and systems that are not suitable to the country context, mainly due to expense – only aim is to get the material on the shelf making people and patients wanting a higher standard than is affordable and with only a small difference in positive impact when compared to a cheaper alternative. (Respondent 93)
A limitation of the qualitative data was that it lacked depth and was a secondary component of the survey. Nevertheless, analysing the open-ended qualitative questions on the survey allowed for an in-depth exploration of prosthetic services that are not captured in standardized outcome measures. A limitation of qualitative research in general is that inferences cannot be made outside the scope of the sample. However, the generalizability of our findings has in large part been improved due to the strength of the large sample size. Other limitations of this study include the possible sampling bias of relying solely on an electronic distribution method; however, as the invitations were sent to practitioners rather than patients, this limitation was mitigated by relying on workplace internet accessibility rather than on the individual respondents. Furthermore, the use of the World Bank’s income groupings based on country gross domestic products (GDPs) provides only a rough measure of the economic context of a particular facility, but the groupings have the benefit of being readily available and commonly used as a basis for the categorization of countries. Finally, the potential differences between practitioner and patient goals and values for prosthetic rehabilitation were not investigated in this study; however, a recent study found general agreement between patients and practitioners with only some differences in psychological outcomes apparent. 30
Conclusion
This study has highlighted numerous issues related to the provision of prosthetic rehabilitation within the global context. Findings suggest that there are both similarities and clear differences in the needs of patients and practitioners across countries with different income levels. These include differences in part/material availability, practitioner training generally and providing comfortable socket fit and prosthesis alignment specifically. The durability and repairability of prosthetic feet and knees are particularly important in LICs, while high costs were an issue raised by all practitioners. These results can be used to guide designs of more appropriate lower limb prosthetic technologies and development of services around the world.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.