
Abstract
Study Design:
Literature Review
Background:
We estimate that over 29 million people worldwide in resource-limited environments (RLEs) are in need of orthotic and prosthetic (O&P) devices and services.
Objectives:
Our goal was to ascertain the current state of O&P provision in RLEs and identify factors that may lead to more successful O&P provision.
Methods:
We conducted a comprehensive scoping literature review of all information related to O&P provision in RLEs published from 2000 to 2010. We targeted Vietnam, Cambodia, Tanzania, Malawi, Colombia, and the Navajo Nation, but also included information about developing countries in general. We searched academic databases and grey literature. We extracted information from each article in the areas of design, manufacturing, distribution, service provision, and technology transfer.
Results:
We identified commonly reported considerations and strategies for O&P provision from 431 articles. Analysis of expert consensus documents revealed recurring themes for improving O&P provision. We found that some suggestions from the consensus documents are being followed, but many are overlooked or have not yet been implemented.
Conclusions:
Areas for improvement include conducting field testing during the design process, providing services to rural environments, offering follow-up services, considering government collaboration, and encouraging an active role of the orthosis/prosthesis user. Outcomes and research studies will be further discussed in Part Two.
Introduction
In resource-limited environments (RLEs), there is a vast need for orthotic and prosthetic (O&P) devices and services. We consider an RLE to be an environment in which the material, human, and financial resources are inadequate to support some endeavor; in this case, that endeavor is provision of O&P devices and services. In general, low- and middle-income countries, or developing countries, are RLEs. It has been estimated that 0.5% of the population needs orthoses or prostheses and related rehabilitation services. 1 Based on the total population in 2011 for all low- and middle-income countries, of 5.8 billion people, 2 we can calculate that over 29 million people in RLEs are in need of O&P devices and services. Although many organizations are involved in O&P provision in RLEs worldwide, the need remains unmet.3,4 In an attempt to alleviate this immense need and remedy the resulting inequalities, the United Nations Convention on the Rights of Persons with Disabilities (CRPD) has mandated States Parties’ obligations to promote research and development for, promote availability of, facilitate access to, and encourage the production of mobility aids and assistive technologies. 5
Several recent publications have provided recommendations for O&P provision in RLEs based on consensus of experts in the field including project and program guides from Landmine Survivors Network6,7 (endorsed by the International Society for Prosthetics and Orthotics (ISPO)), and training guidelines from ISPO and the World Health Organization (WHO). 1 Suggestions have also been put forth through conclusions and recommendations from key conferences such as the 2000 ISPO Consensus Conference on Appropriate Orthopaedic Technology for Low-Income Countries,8,9 the 2002 ISPO Workshop on Prosthetics and Orthotics Training Institutes in Non-Industrialized Countries, 10 the 2006 State-of-the-Science on Appropriate Technology for Developing Countries,11,12 and the 2006 ISPO Consensus Conference on Appropriate Lower Limb Orthotics for Developing Countries. 13 These publications provided fundamental suggestions for successful O&P provision in RLEs.
Many organizations are involved in O&P provision in RLEs around the world working to meet the mandates of the CRPD. Different organizations use different strategies, and some are more successful than others in terms of the devices and/or services they provide. What lacks, however, is a comprehensive assessment of the current state of O&P provision in RLEs, including an assessment in relation to the recommendations from the above-mentioned consensus documents. To accomplish this, we undertook this scoping review.
We chose to target six countries/nations within three geographic regions: Vietnam and Cambodia in Southeast Asia, Tanzania and Malawi in Africa, and Colombia and the Navajo Nation (within the United States) in the Americas. These six RLEs and three regions were chosen to represent a diverse field in terms of economy, culture, geography, conflict status, relative presence of nongovernmental disability organizations, and United Nations Human Development Index. With this scoping review, we will lay the groundwork for future proposed research within these regions. Based on the estimate that 0.5% of the population needs O&P devices and services 1 and population statistics from 2011,2,14 we can calculate that there are a total of more than one million individuals in need of O&P devices and services in the six target RLEs. The World Bank categorizes the economies of Vietnam, Cambodia, Tanzania, and Malawi as low income, and Colombia’s economy as upper middle income. 2 Another indicator of the economic situation in these RLEs is the percentage of the population that lives on less than US$2 per day, which is 38% for Vietnam, 57% for Cambodia, 88% for Tanzania, 91% for Malawi, and 28% for Colombia. 15 The economic situation in the Navajo Nation is described by a 44% unemployment rate and 56% of Navajos living below the poverty line, the highest poverty rate in the United States. 16
Our aims were to determine the state of O&P provision in the six target RLEs and identify factors that may lead to successful O&P provision in RLEs. We addressed two broad research questions: (1) What is the status of O&P provision in RLEs? and (2) How can O&P provision in RLEs be improved or made more successful? We will answer these questions in a two-part series. In Part One, we will address our first research question by answering two specific sub-questions: (1a) What does the literature base look like? and (1b) What considerations and strategies are frequently reported for O&P provision? We will address our second research question by answering the sub-question: (2a) What do consensus documents suggest for improving O&P provision? In Part Two, we will examine reported outcomes from the full literature base and conclusions from relevant research studies, and analyze the evidence base. This scoping review will reveal the current state of O&P provision in RLEs and determine what can be done to make it more successful. The results will inform and guide all stakeholders in O&P provision including funding agencies, policy makers, governments, and researchers, as well as those directly involved in O&P provision, such as designers, manufacturers, and service providers.
Methods
We conducted a comprehensive scoping literature review of all information related to O&P provision in six target RLEs and developing countries in general, which was published over an 11-year period from 2000 to 2010. This scoping review differs from a systematic review in that our goal was not to answer one specific research question with strict inclusion criteria for the literature examined, but rather our goals were more broad—to determine the state of O&P provision in RLEs and identify factors that may lead to successful O&P provision, based on all types of literature. Still, we designed our protocol to be conducted in a very systematic, thorough, and transparent manner.
We defined O&P provision as inclusive of these aspects: design (including research and development) of the device, manufacturing, distribution, service provision (including delivery of the device to the end-user), and technology transfer (including knowledge translation). We focused our scoping review on six specific RLEs in three geographic regions as explained above. Because so much of the literature about O&P provision in RLEs is not related to any specific country, we widened our search to include developing countries in general as well. We recognize that work being carried out in RLEs is often not published in peer-reviewed journals or presented at academic conferences, and therefore, we sought out all types and sources of literature to get the most complete picture.
Protocol
A flowchart shows our protocol broken into two phases: search and review, and code and reconcile (Figure 1). We searched 12 databases and developed extensive lists of search terms for each of the following categories: device, organization, person, access, outcomes, and location (Table 1). All search terms within a category were connected with the Boolean operator “OR.” Search strings were made by linking together three categories with the Boolean operator “AND.” Searches were tailored for each database, and for smaller databases, the searching was much more restricted. We limited searches to publication dates of 1 January 2000–31 December 2010.
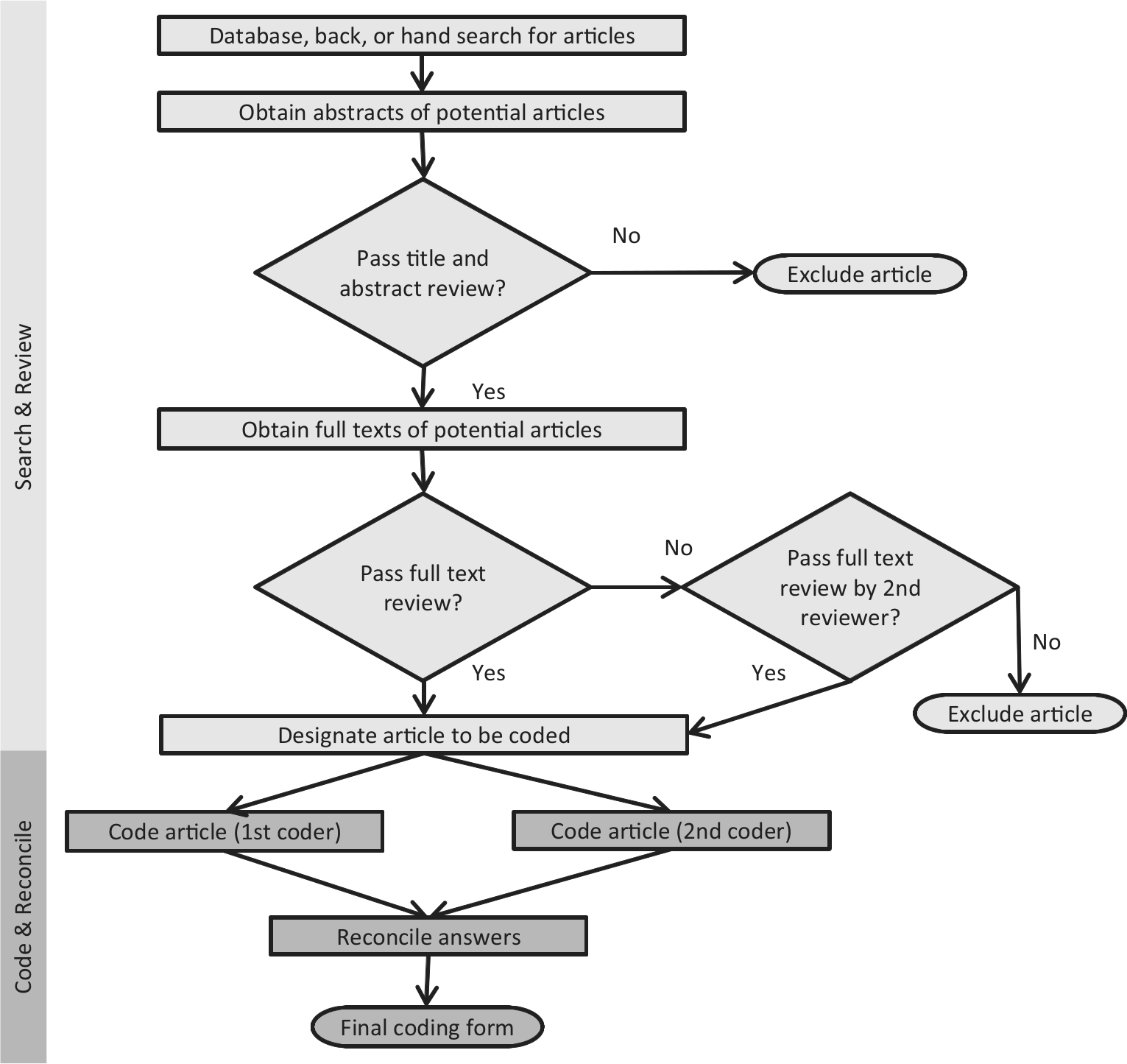
Phases of the protocol: search and review, and code and reconcile.
Databases searched, example search terms, and format of search strings used. Controlled vocabulary search terms were determined, as applicable, for individual databases. Search strings were made with all combinations of controlled vocabulary and natural language terms, as applicable by database.
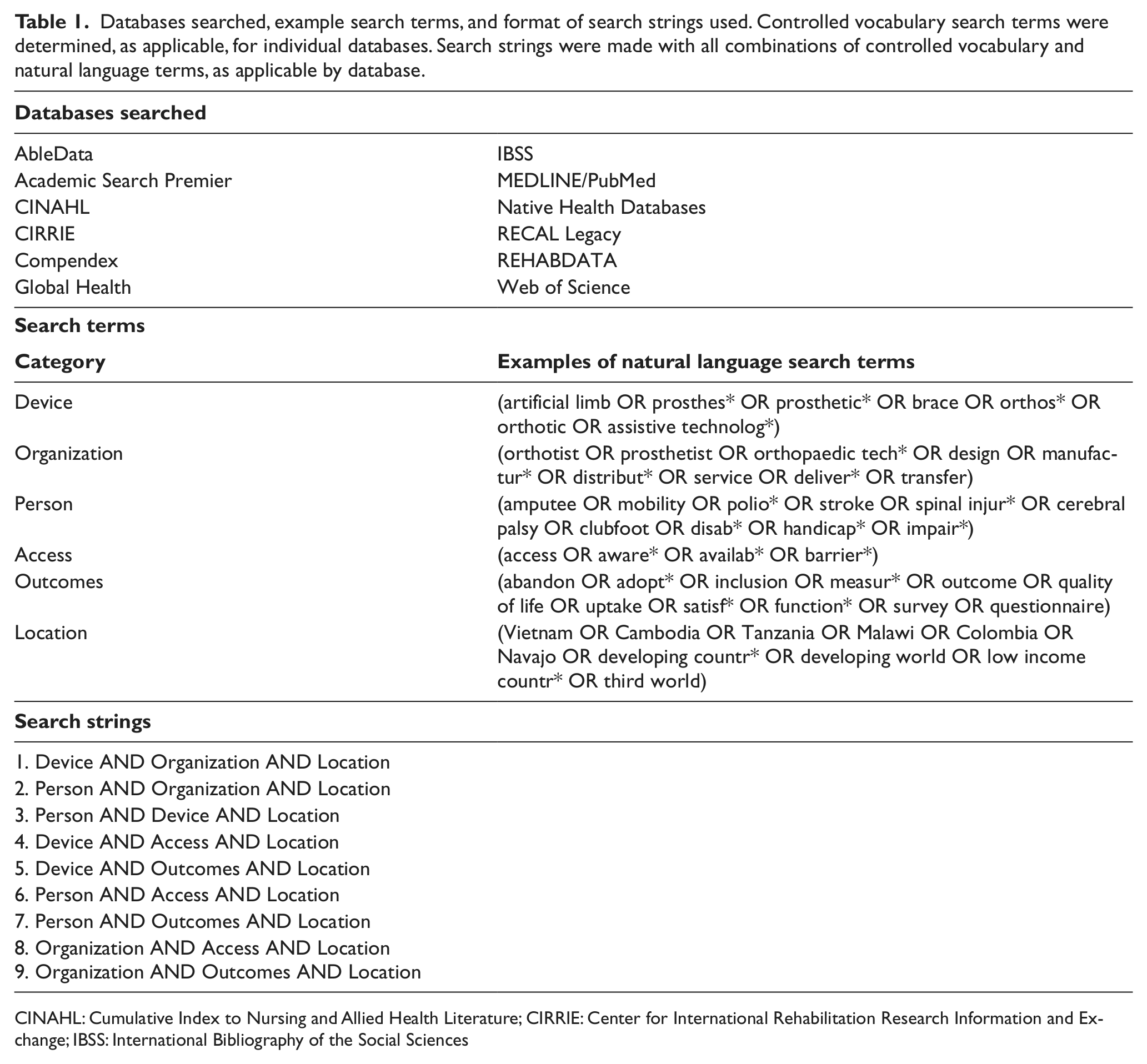
CINAHL: Cumulative Index to Nursing and Allied Health Literature; CIRRIE: Center for International Rehabilitation Research Information and Exchange; IBSS: International Bibliography of the Social Sciences
After database searching, we conducted hand, back, and grey literature searching. For hand searching, we searched the tables of contents from the most commonly found peer-reviewed journal (Prosthetics and Orthotics International) and the most commonly found magazine (OrthoLetter) for all issues published from 2000 to 2010. (Publication of OrthoLetter was discontinued after 2004.) For back searching, we searched the reference lists of all articles that passed full text review. We searched for grey literature primarily on websites of organizations that were identified from the literature, in conference proceedings of relevant conferences, and through general Internet searching with Google and Bing using simplified search strings. For websites with multiple pages, we combined several web pages from the same organization and downloadable information from those web pages to create a web “article.”
We reviewed all articles that were returned from searching for inclusion in our scoping review. Inclusion criteria were: (1) a significant portion of the article focused on O&P and (2) the setting was one of the six target RLEs or covered developing countries in general. If an article met both criteria based on its title and abstract (if there was an abstract), we retrieved the full text of the article and reviewed it for inclusion. If we thought it did not meet the inclusion criteria, we marked it for exclusion, but a second reviewer approved or disapproved exclusion of any article. We included no duplicates, but duplicates found through database searching were tracked in order to determine the overlap among databases. If the same exact content was published in more than one source, we designated it a “replica” article. We also checked for similar articles that covered primarily the same information, but may have had additional details; these we designated “derivative” articles of the main articles. Any articles that we came across serendipitously, which were not found by any of our search methods but which would pass our full text review, were included and designated as miscellaneous finds.
Subsequent to search and review, we conducted the code and reconcile phase of our protocol (Figure 1). For this phase, we developed an extensive coding form to extract all information related to O&P provision in RLEs from each article. Questions on the coding form covered areas related to general information, type of article, study design, measured outcomes, and each aspect of O&P provision (device design, manufacturing, distribution, delivery, service provision, and technology transfer). For each aspect of O&P provision, check box questions indicated whether or not specific considerations were mentioned in the article. The coding form also contained an open-ended question for each aspect of O&P provision, which was used to indicate how the authors described “successful” for that aspect of O&P provision. We coded articles by reading the full text and answering all questions on the coding form. We coded derivative articles together with their respective main articles, on the same coding form. Two individuals independently coded each article. After both individuals completed their coding forms, together they reconciled conflicting answers until they agreed upon a final version of the coding form that was used for data analysis.
Data analysis
We grouped together coding forms that described the same scenario, for example, the same organization distributing the same product, so as to compile all information about that scenario together. For check box questions, we tallied answers from all final coding forms. For open-ended text entries, we analyzed the text to identify recurring themes for each question. When appropriate, we grouped answers into subfields of orthotics, upper extremity (UE) prosthetics, transtibial prosthetics, transfemoral prosthetics, lower limb (LL) prosthetics for articles that did not specify transtibial or transfemoral, and O&P in general for articles that considered orthotics and prosthetics together as one field.
Results
The literature base
In total, we found 431 main articles, 71 derivatives, and 3 replicas that passed full text review and were included in our scoping review (Figure 2). The full list of all included articles can be found in the online supplemental material for this article. Grey literature searching produced the largest number of articles, with the majority from international conference proceedings, highlighting the importance of searching all sources of information. The articles we found from hand searching Prosthetics and Orthotics International appeared to be non-peer-reviewed articles, such as editorials, which were not consistently indexed in the databases we searched. Likewise, the articles we found from hand searching OrthoLetter were not consistently indexed in RECAL Legacy, the only database that indexed OrthoLetter. Taking into account the overlap among databases, 94% of the articles included from database searching were found in the top five databases: RECAL Legacy, MEDLINE/PubMed, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Academic Search Premier. These results emphasize the importance of each type of searching in order to find all information available.
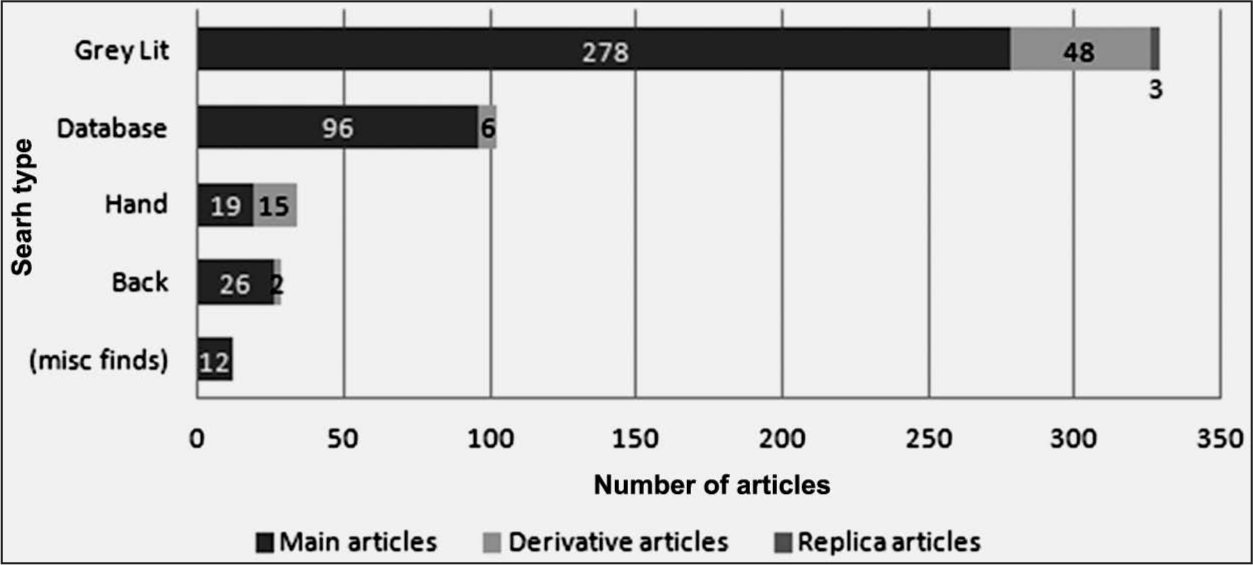
Number of main, derivative, and replica articles found from each type of search.
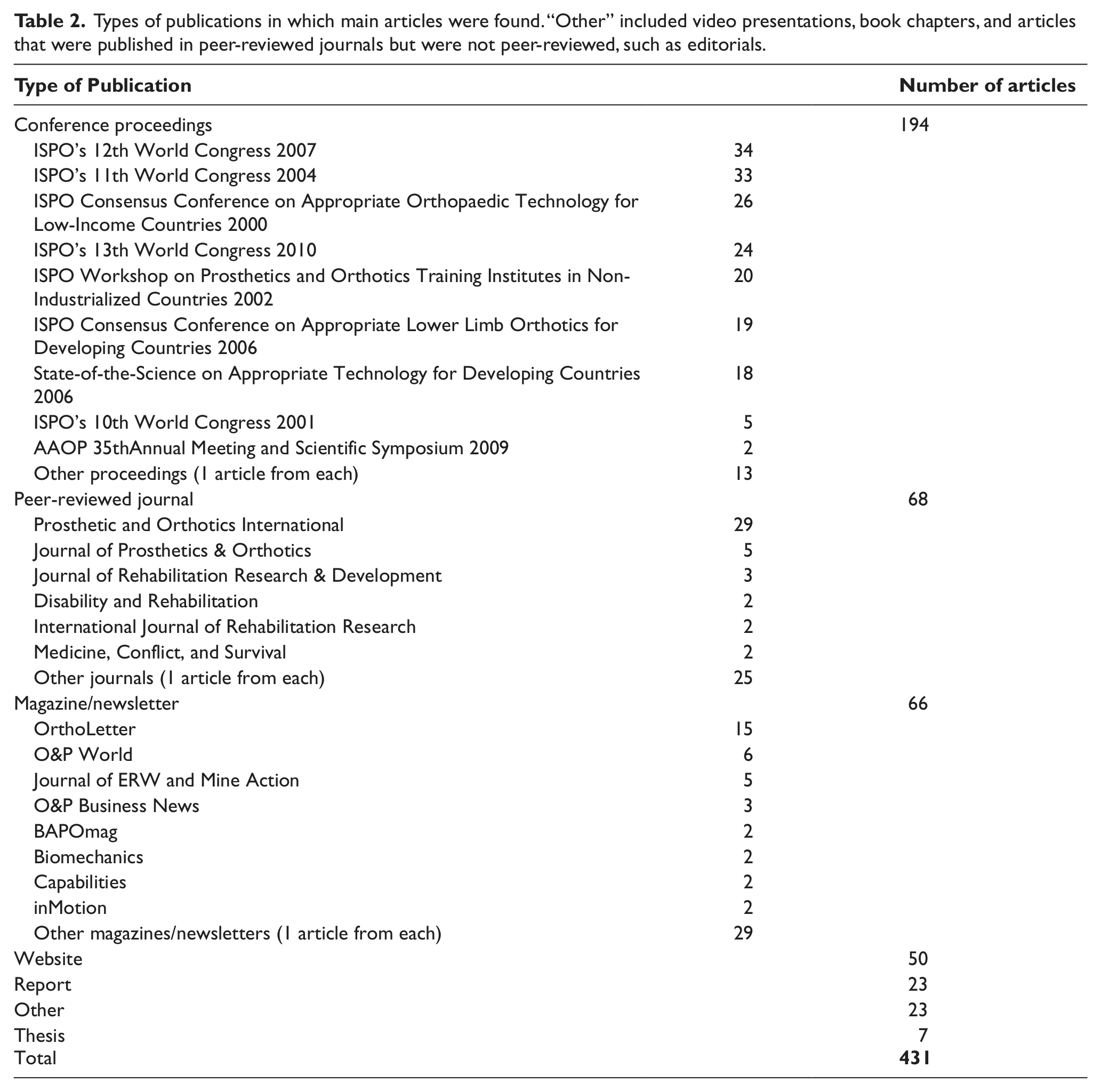
The types of publication sources in which we found the articles were quite diverse (Table 2). Most common were conference proceedings, which were mainly found through grey literature searching but were sometimes found through database searching. Back searching produced articles from sources such as magazines, independent reports, and more obscure journals. Some magazines and newsletters were indexed in databases; others were found through grey literature searching. The variety of types of publications provided a diverse field of literature.
Types of publications in which main articles were found. “Other” included video presentations, book chapters, and articles that were published in peer-reviewed journals but were not peer-reviewed, such as editorials.
Articles often contained information about multiple RLEs and had topics of more than one aspect of O&P provision (Figure 3). We identified 156 articles that corresponded to the six target RLEs; 320 articles mentioned developing countries in general. The large number articles for Vietnam, Cambodia, and Tanzania can be explained in part by the existence of formal training institutes in each of these RLEs. Minimal mention of the Navajo Nation may be a reflection of its relatively small population compared to the other five target RLEs.
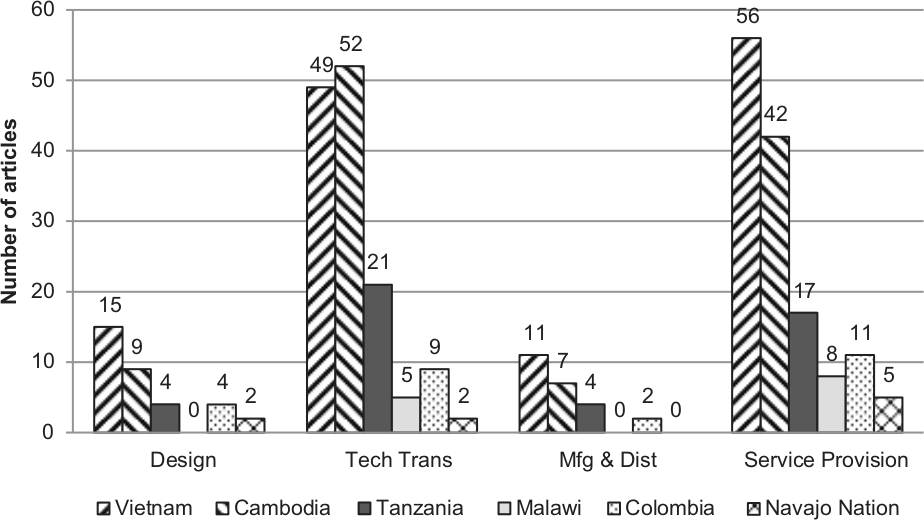
Number of main articles found by aspect of O&P provision and by RLE. Many articles contained information about more than one aspect of O&P provision and/or more than one RLE.
Design considerations
Information about the design of O&P devices or methods was presented in 137 articles, containing information about 101 distinct devices and methods (Table 3). We found 17 articles with information about the design of 17 distinct orthoses or orthotic components. The Steenbeek foot abduction brace (FAB) was mentioned in three articles,17–19 and three articles contained information about the prefabricated knee–ankle–foot orthosis (PFKAFO).20–22 The designs of 14 different UE prostheses or terminal devices were discussed in 15 articles. There were 89 articles containing information about the design of 59 different LL prostheses or prosthetic components, including feet. Commonly mentioned were a polycentric knee designed in collaboration between Stanford and Jaipur,23–25 polypropylene components from the International Committee of the Red Cross (ICRC),26–28 a prosthetic knee designed by LeTourneau Engineering Global Solutions (LEGS),29–34 the Shape&Roll foot,35–38 the monolimb,39–44 the Jaipur foot,45–53 and the Niagara Foot.54–62 There were 19 articles that included information about the design of 11 distinct methods related to prosthetics service provision such as the transtibial alignment system,39,40,63–66 sand casting,67–69 and CIR casting.70–72 Looking at all devices and methods together, the origin of the design was more than twice as often reported as international compared to local or regional within an RLE. Consideration of services or resources was by far the most commonly reported design consideration. Less than 8% of the articles describing device designs reported involvement of the end-user in the design process, either passively or actively.
Number of devices or methods for which common design considerations were reported.
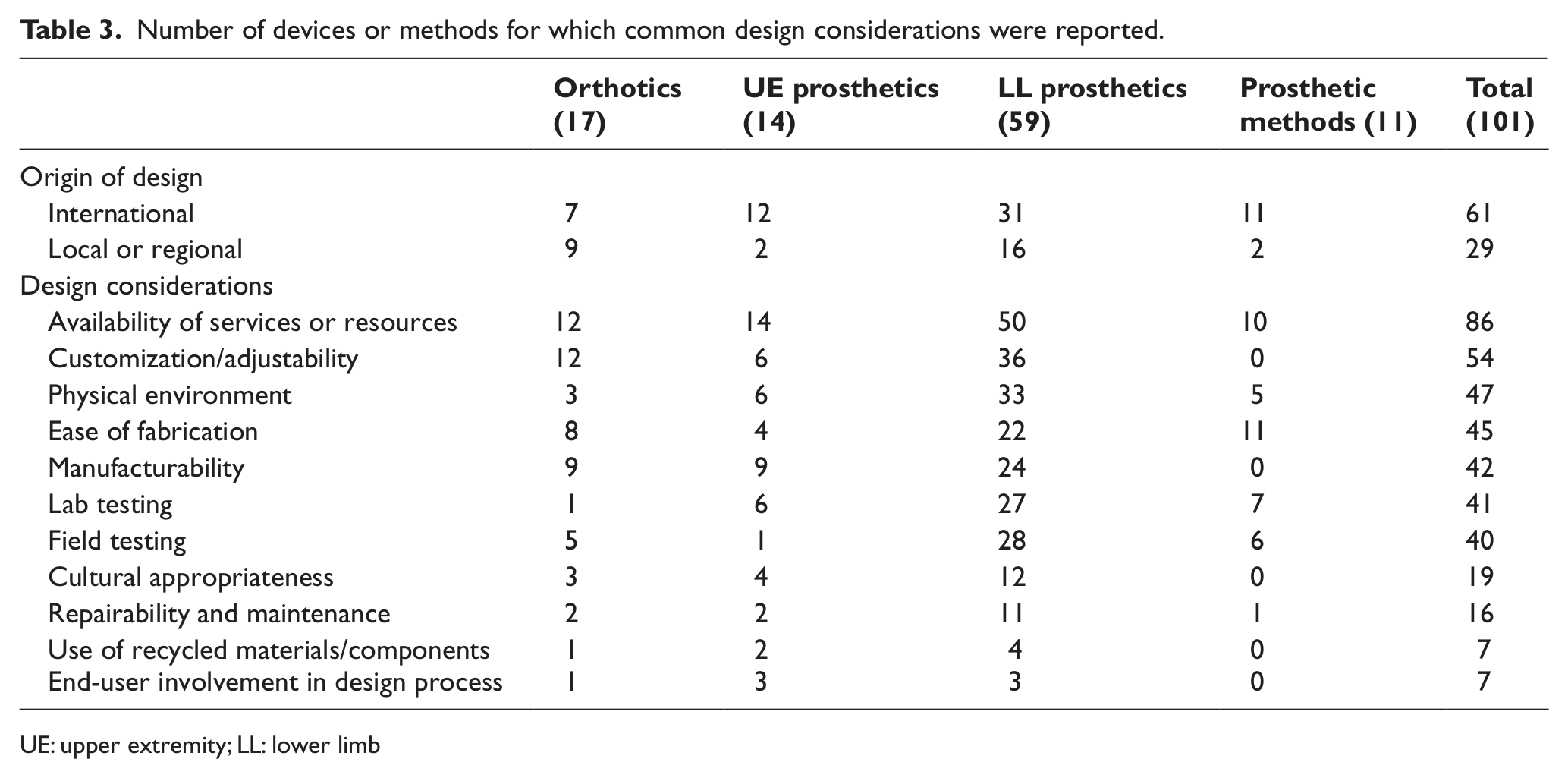
UE: upper extremity; LL: lower limb
Successful design themes and strategies
From the consensus documents, we identified several recurring themes that were suggested for successful design: the devices should be affordable,9,11,12 durable,9,11,12 and the design process should include field testing.8,12
We also identified common design strategies from the full body of literature. The design strategies for orthoses most frequently mentioned were that they should be affordable, lightweight, and use prefabricated devices. The use of prefabricated devices, such as Mobility India’s PFKAFO20,21,73 and the LETOR orthosis 74 were promoted by some articles. However, a contradictory view was also presented, that prefabricated devices were not adequate in terms of fit or function. 22
The most often mentioned strategies for UE prostheses were to be affordable, body-powered, durable, and comfortable. A literature review of UE prosthetics in the developing world noted that there were advantages of myoelectric prostheses, but that these devices were not generally appropriate for use in the developing world. 75 The comfort of the prosthesis was often mentioned in relation to the heat of the socket, suggesting socket designs should have ventilation or breathability.76–80
The most common strategies for design of LL prostheses or components were that they be affordable, durable, lightweight, cosmetically acceptable, and consider the physical environment/climate. The designers of the Niagara Foot suggested affordability would be dependent on the end-user’s annual income and that the cost of the prosthesis should be less than 3% of their annual income. 54 A recent literature review concluded that vulcanized rubber outperformed lighter weight foam, but the challenge remained to make feet more lightweight, 81 emphasizing the link between durability and device weight. Designing a prosthetic foot to be waterproof was mentioned in consideration of the environment for the Niagara Foot, 55 Jaipur foot,46,48,49,53 and other vulcanized rubber feet. 76 The types of cosmetic covers proposed ranged from high-definition silicone covers 82 to covers made of Bubble Wrap®. 83
When O&P devices were discussed together, the most common strategies for design were that the designs be affordable, use polypropylene, and consider the physical environment/climate. Regarding the use of polypropylene, its advantages included being multipurpose, recyclable, low cost, easy to store, long lasting, and environmentally friendly. 9
Manufacturing and distribution considerations
Several terms related to manufacturing and distribution were used in different ways by different authors. For consistency in our scoping review, we distinguished between manufacturing and fabricating. We defined manufacturing as making a non-custom device either in bulk or individually; it is done by a manufacturer, who could also be a service provider but often is not. We defined fabrication as individually making a custom device; it is done by a service provider. We also distinguished between the terms distribution and delivery. We defined distribution as the transfer of a product to a middleman, while we defined delivery as the transfer of a product to the end-user.
Details about manufacturing and distribution were reported in 59 articles, with information about 64 manufacturing and distribution scenarios. After we grouped together coding forms that described the same scenario, for example, the same organization manufacturing the same product, we determined that 53 of the scenarios were distinct (Table 4). Manufacturing related to orthoses (including therapeutic shoes and sandals) and orthotic components was discussed in seven articles. Authors of 33 articles discussed 31 distinct manufacturing scenarios for prosthetic components, including knees and feet. ICRC polypropylene prosthetic components26,27,84 and the ATLAS system85–87 were commonly mentioned. There were 10 articles that contained information about nine distinct manufacturing scenarios for O&P components together. Again, ICRC polypropylene components were commonly mentioned for this category of O&P together.88–90 Eight articles contained information about six distinct distribution scenarios. Overall, manufacturing usually produced a device in more than one size, used local materials, and did not often mention quality control.
Number of scenarios that described common manufacturing and distribution considerations. The distinction between high tech and low tech was not clear-cut; however, a device that was handmade indicated low tech, whereas automated processes were typically considered high tech.
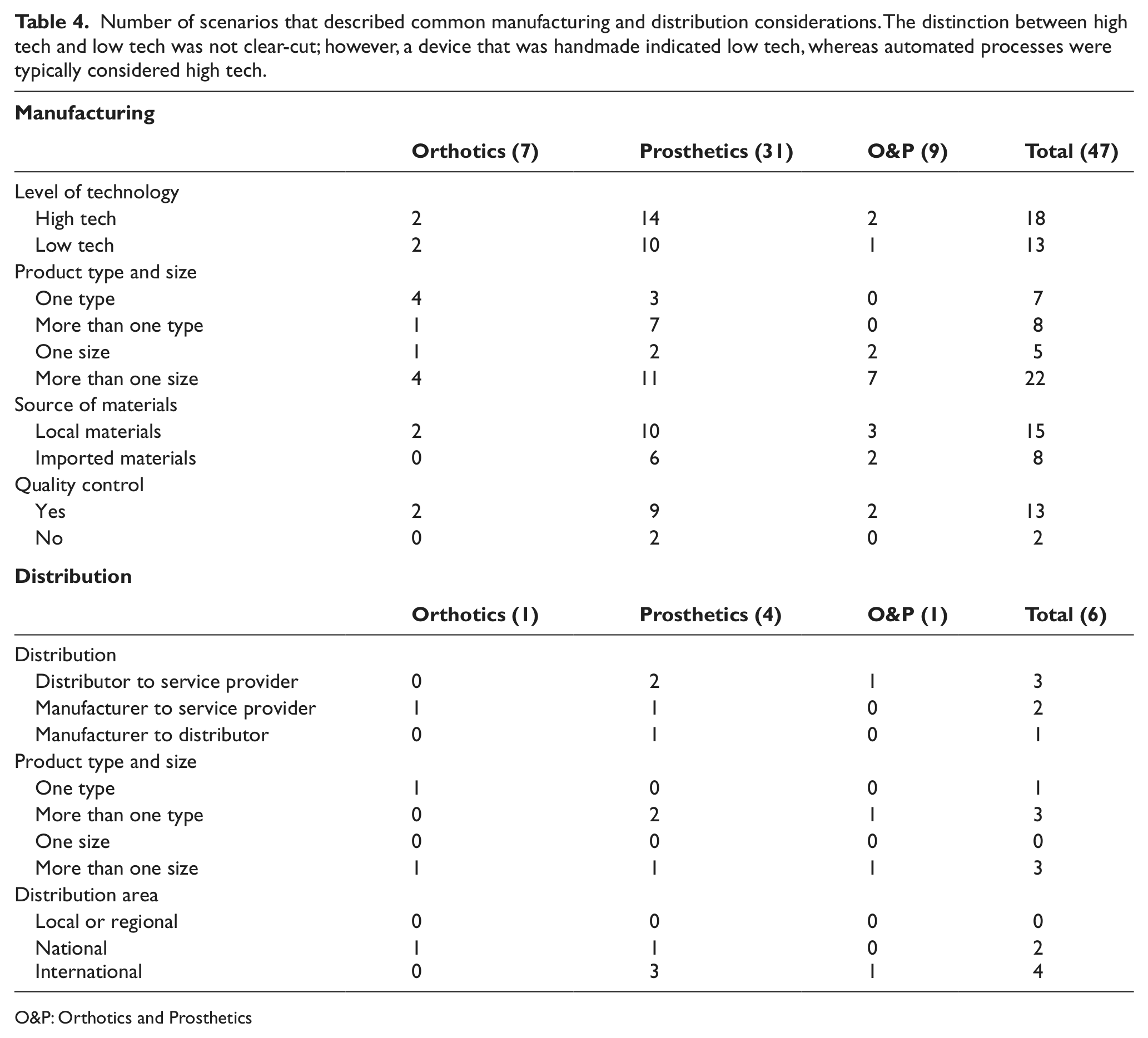
O&P: Orthotics and Prosthetics
Successful manufacturing and distribution themes and strategies
Manufacturing and distribution of O&P devices were sparingly mentioned in the consensus documents. Regarding successful manufacturing, the approach of establishing a regional manufacturer with standards for quality assurance was recommended. 11 However, it was also noted that local manufacturing was appropriate where demand was low. 12
Looking at the full body of literature, the most commonly discussed strategies for successful manufacturing were to be affordable, utilize simple techniques that require only basic/standard tools, and utilize either local manufacturing with local materials or centralized manufacturing. Ways to keep manufacturing affordable included mass production 91 and local manufacturing. 92 The LEGS knee,30,31,33,34,93 the Jaipur foot,48,49 the Shape&Roll foot, 38 and a prototype prosthetic knee 94 all used simple manufacturing techniques with basic/standard tools. Proponents of local manufacturing with local materials pointed out that it promotes a sense of pride and contributes to the sustainability of clinics, 30 and that locally manufactured components can reduce costs by more than 90% compared to imported components. 92 Another advantage of using local materials was that since local workers were familiar with the materials, they could be trained quickly. 46 However, proponents of centralized manufacturing suggested that locally made feet were not durable 58 and that centralizing manufacturing could result in lower prices and improved quality. 28 ICRC was a strong advocate for centralized manufacturing. ICRC started out using local manufacturing with local materials, but found that this model did not produce good quality products because the low demand could not justify the expensive equipment required. Also, for ICRC, regionalization was not a possibility because of the potential destabilization of candidate countries. 26 Centralized manufacturing produced positive results with the new components lasting longer. 26
Although very few articles contained ideas related to distribution, we identified strategies of working with local or regional partner organizations for distribution24,80 and using the Internet for inventory and managing distribution.95,96
Service provision considerations
Activities related to O&P service provision, including delivery of a device, were reported in 109 articles, with information about 135 scenarios. We grouped scenarios of the same service provider delivering the same device and found that we had 111 distinct scenarios (Table 5). In 19 articles, 18 different service provision scenarios for orthoses were described. There were 56 articles containing information about 54 distinct service provision scenarios for prostheses. Authors of 34 articles discussed 39 distinct service provision scenarios for O&P devices together. Service provision at, or in coordination with, training institutes in Vietnam, Cambodia, and Tanzania was commonly mentioned for both orthotics and prosthetics, especially when described as part of a research study. Some unique delivery scenarios were delivery of FABs for the treatment of clubfoot,18,97–100 and delivery of prostheses in camp49,53 or outreach settings. 101 Generally, service provision was center-based in an urban or semi-urban environment. The service providers were usually local or national, as opposed to foreign, and usually had an advanced level of education, if the level of education was reported. Low-tech fabrication methods were much more common than high-tech methods such as computer-aided design (CAD)/ computer-aided manufacturing (CAM).
Number of scenarios that described service provision characteristics and activities.
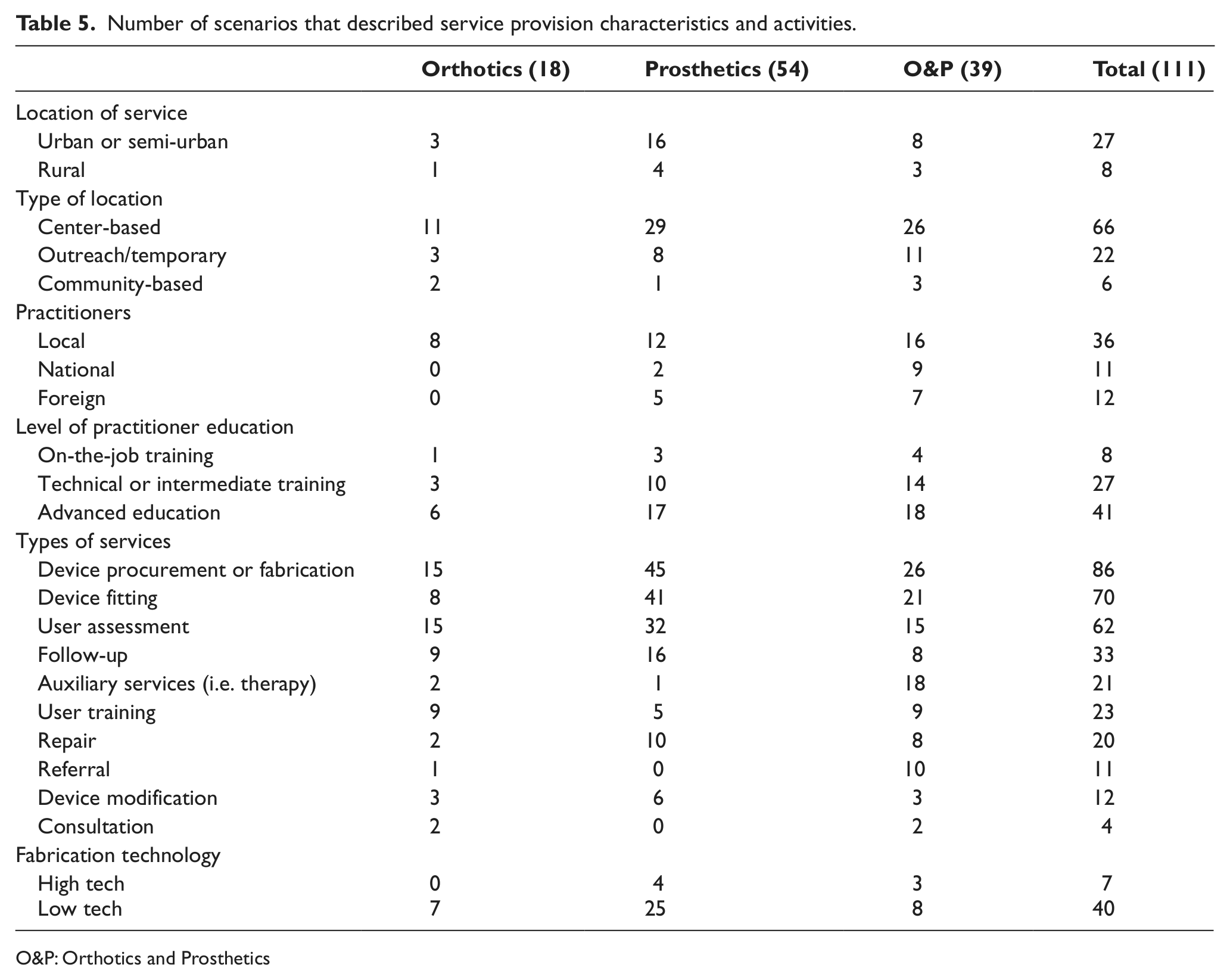
O&P: Orthotics and Prosthetics
Successful service provision themes and strategies
We identified many themes for successful O&P service provision suggested by the consensus documents: offer multi-disciplinary comprehensive services,1,7,9,13 work with community-based rehabilitation (CBR),1,8,9,12,13 be affordable,1,7–9 encourage an active role of the end-user,1,6,8,9,13 provide follow-up services,11,13 collaborate with the government,1,6–9 have well-trained service providers,1,7 and decentralize or reach rural areas.1,11
Among articles about orthotics service provision, the main strategies were to have early screening/referral/fitting services, reach rural areas, offer multi-disciplinary comprehensive services, and provide follow-up. Reaching rural areas was important, and distance from services was noted as a barrier to accessing them.18,102–105 Multi-disciplinary comprehensive services included physician services, physical therapy, social services, community outreach, vocational rehabilitation, and orthotics services.104,106,107 The need for early screening/referral/fitting services was often mentioned for conditions of clubfoot98,108,109 and scoliosis, 110 and it was recommended that CBR programs be used to facilitate this.13,103,105 Follow-up was noted as especially important for compliance with the Ponseti method for treatment of clubfoot.98,100,103
Few authors discussed service provision specific to UE prosthetics. When it was discussed, the most common strategy was to be affordable. Affordability and low cost were mentioned related to costs of material, fabrication, and setup and maintenance.111–113
The most common service provision strategies for LL prostheses were to be affordable, have quick services, have well-trained service providers, produce well-aligned devices, produce well-fitting devices, and use simple methods. Quick service was often mentioned when discussing methods for taking an impression,67,71,114 fabrication methods,115,116 or alignment methods.40,117 A goal of one day was proposed for delivery of a transtibial prosthesis, and two to three days for a transfemoral prosthesis. 11 Well-trained service providers were considered to be at least ISPO Category II level.1,118
The main strategies for service provision of O&P devices together were to offer multi-disciplinary comprehensive services, have well-trained service providers, be affordable, have sustainable/self-sufficient services, and work with CBR. Factors that contribute to project sustainability included confirming government support, identifying the role of national partners, employing skilled individuals, and planning for long-term financial sustainability.8,9 The roles of CBR related to O&P service provision included promoting inclusion, participation and integration,119–125 being a referral source,124–126 doing simple repairs,9,124 conducting home visits, 120 being an advocate to the community,121,124 reaching rural areas,127,128 and providing early detection of those who could benefit from an orthosis or prosthesis.37,124,129
Technology transfer characteristics
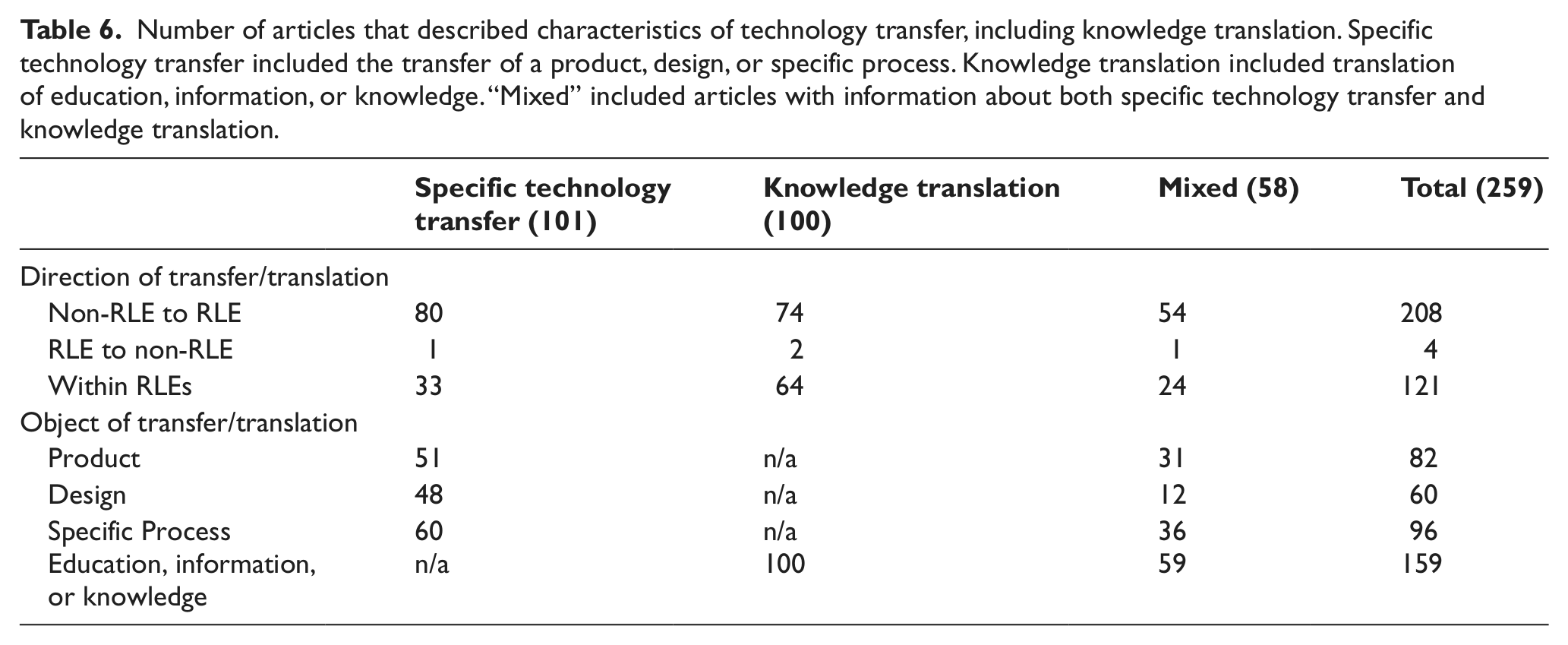
We defined technology transfer as providing a technology/process and associated knowledge to any stakeholder; this included knowledge translation. Technology transfer did not include the provision of a specific device to an end-user, as we considered this part of the service provision process. A large number of articles, 259, contained information related to technology transfer (Table 6). Technology transfer from a non-RLE to an RLE was almost twice as common as transfer within RLEs, and transfer from an RLE to a non-RLE was rare. Knowledge translation was discussed in 159 of the 259 articles (61%), including articles with information about both knowledge translation and specific technology transfer.
Number of articles that described characteristics of technology transfer, including knowledge translation. Specific technology transfer included the transfer of a product, design, or specific process. Knowledge translation included translation of education, information, or knowledge. “Mixed” included articles with information about both specific technology transfer and knowledge translation.
Successful technology transfer themes and strategies
Many ideas for successful technology transfer, especially knowledge translation, were proposed in the consensus documents. We identified the following themes for successful knowledge translation: provide continuing education,1,13 measure the outcomes of the training program or have quality management,1,8,13 and offer upgrade training 1 including strategies for upgrading from Category II to Category I. 10 Related to successful technology transfer of devices, recurring themes were not as evident, but suggestions included: collaborate with a local partner,6,9,12 conduct follow-up activities, 11 work with training institutes for technology dissemination, 12 and complete the device design cycle, including independent testing, before making the product available for transfer. 12
The most common strategies for knowledge translation were to measure the outcomes of training programs or have quality management, utilize distance learning, have a clinical placement as part of formal training, make schools sustainable, train to the ISPO Category II level, offer upgrade training, and providing continuing education opportunities to service providers. Distance learning was used for upgrade training,130–132 single discipline courses, 133 a train-the-trainer program, 134 and a program to upgrade from Category II to a bachelor’s degree program. 135
For technology transfer of specific devices/designs/processes, the most common strategies were to work with a local partner and include hands-on training. Working closely with strong local partner organizations was integral to the approach used by organizations such as LEGS 34 and Prosthetics Outreach Foundation. 92 Hands-on training scenarios were described for transfer of the PFKAFO technology, 21 transtibial alignment techniques,63,136 a sand casting and fabrication method, 69 and the OK Prosthetics method of socket fabrication. 115
Policy and structure
Consensus conferences have suggested that governments should be responsible for making national policy and ensuring that services are available, regulated, and funded. 9 Rehabilitation services are the responsibility of the Ministry of Labor, Invalids and Social Affairs in Vietnam, the Ministry of Social Affairs, Veterans and Youth Rehabilitation in Cambodia, and the Directorate of Social Welfare at the Ministry of Social Protection in Colombia. The Ministries of Health of Tanzania and Malawi are also concerned with rehabilitation. Malawi is the only one of our six target RLEs to have ratified the United Nations CRPD during the timeframe of this scoping review.
The role of the end-user
The consensus documents promoted an active role of the end-user, especially related to service provision. These documents suggested that end-users be active members of the rehabilitation team,8,9,13 participate in user groups for peer support,8,13and be involved in planning and execution of services6,13 and noted that end-users should be respected, listened to, and given the opportunity to choose their type of orthosis/prosthesis.1,6
However, we found that the involvement of the end-user was not a common consideration in any aspect of O&P provision, and only mentioned occasionally. The ways in which end-users were involved in device design included passive involvement for measurements for components or prefabricated devices,21,137 providing feedback through user trials and interviews,33,138,139 and the designer having an amputation himself. 140 Users were often subjects in research evaluating O&P devices, sometimes during the design phase but more often during independent field testing; we will discuss research studies in greater detail in Part Two. One article described a distribution program that was founded by a person who had an amputation. 96 The roles of the orthosis/prosthesis user related to service provision included being a peer counselor and motivator, 141 being trainees and hired to work in the fabrication (or manufacture) of O&P devices, 142 and being directly involved with carrying out O&P program activities and service provision.63,143,144 Related to knowledge translation, training programs for service providers often recruited individuals with disabilities. Therefore, orthosis/prosthesis users were the recipients of knowledge translation and also went on to become service providers.145,146 End-users were passively involved in knowledge translation when they served as subjects for final exams of service provider training programs. 147 Overall, user involvement in O&P provision was relatively infrequently reported, and often limited to passive involvement.
Discussion
The literature base
We compiled a very large literature base of 431 main articles and 71 derivative articles with supporting information. Articles from ISPO-sponsored conferences, ISPO’s journal (Prosthetics and Orthotics International), and a newsletter of ISPO (OrthoLetter), together accounted for 205 of the 431 main articles, indicating the substantial role ISPO plays in disseminating literature published about O&P provision in RLEs. The field of orthotics was underrepresented in the literature. For device design (Table 3), only 17% of the devices were orthoses; for manufacturing and distribution (Table 4), only 15% of the scenarios were in the field of orthotics while 66% were in the field of prosthetics (19% grouped O&P together); and for service provision (Table 5), only 16% of the scenarios were related to orthotics while 49% were related to prosthetics (35% grouped O&P together). This shortage of information in orthotics exists, despite the fact that there is a greater need for orthoses than prostheses.13,105,148 Stakeholders in O&P provision in RLEs should pay greater attention to the field of orthotics.
Many of the articles we included were written about developing countries in general; in fact, 170 articles did not cover any specific RLE, only developing countries in general. Therefore, we found it difficult to determine factors related to O&P provision that were most pertinent for specific countries or contexts or to explore regional differences and similarities, as we had hoped. Within the three target geographic regions, we found more than twice as many articles for the Southeast Asia region (135 articles) compared to the Africa and Americas regions combined (59 articles). Some reasons for the disparity in numbers of articles were as follows: both of the target countries in Southeast Asia have formal training institutes, many international organizations are active in Southeast Asia and published widely, and the total population for the two target countries in Southeast Asia is approximately equal to the total population of all four target countries in the Africa and Americas regions combined.
The state of O&P provision
The themes for successful design from the consensus documents have been followed to various degrees. One theme, to be affordable, was the most common design consideration reported. In 86% of the devices or methods described, availability of services or resources was considered, usually related to financial resources and affordability. This indicates that designers are largely following the recommendation to consider affordability. Another theme for successful design was to design for durability. Directly related to durability, consideration of the physical environment was mentioned for 47% of the devices or methods, indicating that this suggestion is not receiving as much consideration as affordability. Field testing as part of the design process was suggested by the consensus documents but only reported for 38% of the devices or methods. (When field testing was mentioned in the literature, it was usually not during the design phase.) More designers of O&P devices and methods need to incorporate field testing into their design process.
Relatively few articles contained specific information on manufacturing and distribution. The literature provided arguments for all types of manufacturing: local, regional, and centralized. The consensus documents did not delineate a preferred type of manufacturing practice. Among the manufacturers for which the source of materials was reported, 15 manufacturers (65%) used local sources and 8 manufacturers (35%) used imported materials. When information on distribution was reported, four of six articles reported international distribution, which would imply that centralized manufacturing was utilized. Due to a lack of information published related to manufacturing and distribution, and the differing opinions, we could not determine a preferred practice for O&P manufacturing and distribution in RLEs. We also recognize that the differing opinions in the literature may be a reflection of the different contexts of each scenario. Manufacturers should consider their own context to determine the best approach, taking into account factors such as demand, quality control, available materials, and possible import/export restrictions.
The data revealed that the state of service provision conformed to the suggestions from consensus documents to varying degrees. The consensus documents suggested having well-trained service providers, considered to be those trained to the ISPO Category II level or higher. 1 Out of 52 scenarios that described the service providers’ education level, 41 (79%) reported practitioners having an advanced, or ISPO Category II level; however, some of these scenarios also included other practitioners with lower levels of education. The consensus documents also suggested decentralizing service provision and reaching rural areas. However, we found that service provision facilities were usually center-based (70%) and in an urban or semi-urban environment (77%). In addition, Cavenett et al. 127 stated that the biggest challenge for O&P service provision was reaching rural and remote areas, and Eide and Øderud 3 found that individuals living in rural areas have less access to assistive technology, including O&P devices. Only 33 of 111 scenarios (30%) reported offering follow-up services, although this was suggested by the consensus documents for successful service provision. This number may be inflated because follow-up was reported for many research studies, but may not be a part of their usual service provision. 149 Other suggestions from the consensus documents included offering multi-disciplinary comprehensive services, working with CBR, and being affordable; these suggestions were commonly reported throughout the literature as strategies that were being employed. One suggestion from the consensus documents that was not often reported in the rest of the literature was to collaborate with the government. Service providers need to address the problem of reaching rural environments, adopt the practice of offering follow-up services, and consider collaboration with the government.
Themes from the consensus documents for successful technology transfer included providing continuing education, measuring the outcomes of the training program or having quality management, offering upgrade training, and collaborating with a local partner. All of these suggestions were also found in the full body of literature as common strategies that were being employed.
The role of the orthosis/prosthesis user was not commonly mentioned for any aspect of O&P provision, although an active role was recommended by the consensus documents. In addition to these documents, Lindstrom 150 described some advantages of employing individuals with disabilities such as being able to draw on personal experience and serving as a role model to other individuals with disabilities. When any involvement was mentioned, it was often related to service provision. There was, however, a conflicting opinion about employing end-users in service provision. After 20 years of giving individuals with disabilities job opportunities in manufacturing, ICRC came to a disappointing conclusion that in general their approach did not meet quality expectations, created extra expenses, and did not benefit a significant number of individuals with disabilities. 151 However, a later document published by ICRC stated that ICRC does strive to employ individuals with disabilities in their rehabilitation centers to facilitate their socioeconomic reintegration into society. 152 Overall, an active role of the end-user was promoted in the literature, although any role was rarely reported, indicating a need for greater efforts to include the end-user in all aspects of O&P provision.
Limitations
We were only able to search databases that were in English and include articles written in English. However, we were able to use Google Translate on some web pages to translate the information into English. Even with this language limitation, we were able to capture a vast amount of information.
We did not set any inclusion/exclusion criteria to control the quality of the articles included in this scoping review. Of the 431 main articles, only 16% (68 articles) were from peer-reviewed journals (not counting non-peer-reviewed articles such as editorials). However, we believe that if we had excluded some articles because they were non-peer-reviewed, possibly biased, or based on any other judgment of quality, we would have missed crucial information. Our goal was to capture as much information as possible, especially recognizing that much of what is published in or about RLEs may not always be published according to academic standards.
Our data analysis was limited to the information the articles provided. In many cases, articles did not include information on a given topic and an answer of “not reported” was entered on the coding form. An answer of “not reported” cannot be interpreted to mean that the specific item was not considered; it can only be interpreted to mean that it was not reported in the article.
Conclusion
In Part One, we analyzed what authors have written about the current state of O&P provision in RLEs. We found that there is significantly less information available about provision of orthoses compared to prostheses, yet the need for orthoses is greater. We compared common considerations and strategies for each aspect of O&P provision to recommendations put forth by consensus documents for making O&P provision successful. We found that some suggestions are being heeded, but many appear to be overlooked or have not yet been implemented. Specifically, areas for improvement include conducting field testing during the design process, providing services to rural environments, offering follow-up services, considering government collaboration, and encouraging an active role of the orthosis/prosthesis user. Because most of the literature was directed at developing countries in general, one must keep in mind that not all suggestions are applicable to all contexts. In Part Two, we will examine measured outcomes and conclusions from research studies.
Footnotes
Acknowledgements
The authors would like to thank Digital Active for developing the database used to store the data.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by the U.S. Department of Education, National Institute on Disability and Rehabilitation Research [grant number H133A090020].