
Abstract
Background:
Despite the activities of many orthotic and prosthetic provision organizations in resource-limited environments, there is still a great need and there are several areas for improvement, as identified in Part One of this series.
Objectives:
Our goal was to examine outcomes and conclusions of research studies to produce an evidence base for determining factors that may lead to successful provision of orthoses and prostheses in resource-limited environments.
Study design:
Literature review.
Methods:
We conducted a scoping literature review of all information related to orthotic and prosthetic provision in resource-limited environments published from 2000 to 2010. We extracted measured outcomes reported in all types of articles and analyzed conclusions from research studies.
Results:
Reported outcomes included durability, cost, satisfaction, use/nonuse of device, amount of utilization, walking speed, discomfort, pain, fit, misalignment, capacity for service provision, number of devices produced or delivered, and number of graduates from training programs.
Conclusions:
There are many gaps in the evidence base, notably in measuring inclusion, participation, and quality of life for orthosis and prosthesis users in resource-limited environments. There is a paucity of reported outcomes for orthotics. Valid, reliable, and standard methods of data collection and reporting are needed to advance the field and enhance the evidence base.
Keywords
Introduction
In resource-limited environments (RLEs), there is an immense need for the provision of orthotic and prosthetic (O&P) devices and services. Based on estimates that 0.5% of the population need O&P devices and services 1 and greater than 5.8 billion people live in low- and middle-income countries, 2 the number of people in need of O&P devices and services in RLEs exceeds 29 million. In Part One of this series, we reviewed the state of O&P provision in RLEs according to our expansive literature base, for each aspect of O&P provision: design, manufacturing, distribution, service provision, and technology transfer (including knowledge translation). We also discussed consensus documents’ suggestions for making O&P provision more successful. In Part Two, we will analyze measured outcomes and research studies related to O&P provision in RLEs. Part Two aims to provide the evidence to support recommendations for successful O&P provision.
We sought to determine the state of O&P provision in RLEs and identify factors that may make this more successful. We addressed two main research questions: (1) What is the status of O&P provision in RLEs? and (2) How can O&P provision in RLEs be improved or made more successful? In Part Two, we will address our first main research question by discussing the types of research articles we found and reporting the measured outcomes from our literature base. We will address our second main question by analyzing conclusions from research studies for each aspect of O&P provision. We will conclude by examining how current outcome measures and research efforts stand up to the consensus documents’ suggestions from Part One of this series and benchmark measures from Part Two.
Methods
We conducted a scoping literature review of all information related to O&P provision in RLEs published from 2000 to 2010. We focused our review on six target countries/nations within three geographic regions: Southeast Asia (Vietnam and Cambodia), Africa (Tanzania and Malawi), and The Americas (Colombia and the Navajo Nation). We also included articles that were applicable to developing countries in general. Our scoping review protocol included searching for articles in 12 databases, back searching reference lists, hand searching tables of contents from key publications, and extensive gray literature searching. We reviewed all articles for inclusion or exclusion. Two coders extracted information from each included article by completing a detailed coding form and reconciled their answers to produce the final data. The data we analyzed for Part Two included outcomes from all types of publications and conclusions from research studies. We designed our scoping review protocol to be systematic and transparent, and it is presented in detail in Part One of this two-part series.
Results
First, we provide a breakdown of research studies, followed by an overview of an assessment system and benchmarks that have been set for O&P provision in RLEs. Then, we give an account of commonly measured outcomes and research conclusions, by aspect of O&P provision. Outcomes may reflect on more than one aspect of O&P provision, but they are presented with the aspect to which they are most closely linked.
The evidence base
We included a total of 431 articles in our scoping review. The full list of all included articles can be found in the online supplemental material for Part One of this series. We categorized 75 articles as research studies (Figure 1(a)). Additional research results were presented in other types of articles such as program and device overviews. The most common research design was cross-sectional, followed by longitudinal. However, many of the articles that we categorized as longitudinal based on their reported methods did not report longitudinal results. To further distinguish research studies, we classified them as one of the following types: independent field testing, field testing, field testing not in an RLE, independent lab testing, lab testing, and survey (Figure 1(b)). To group similar articles, we also classified studies based on the type of device tested (Figure 1(c)). Transtibial prostheses were the most common type of device tested; for many of these studies, the main object of investigation was the prosthetic foot.
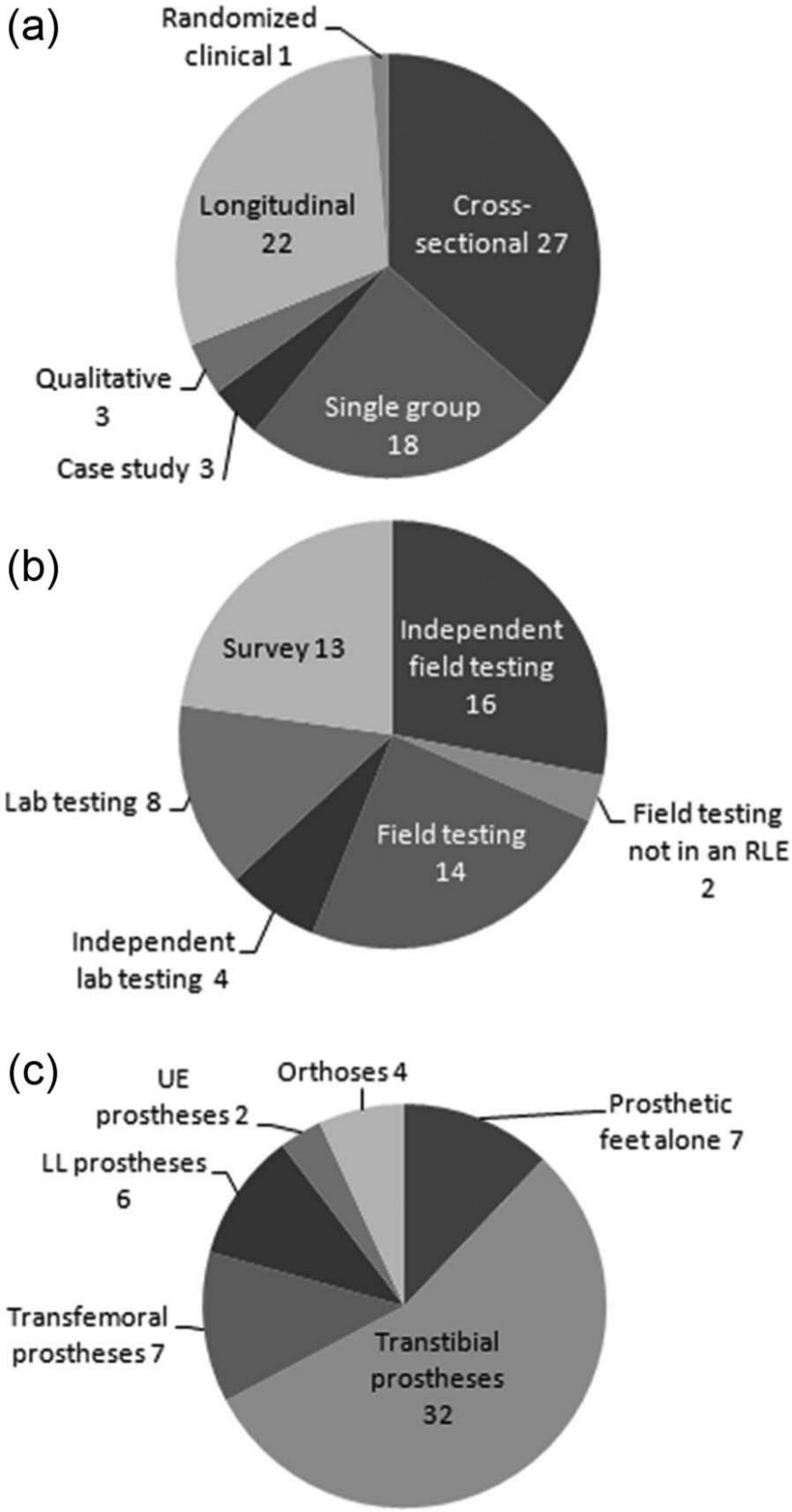
(a) Number of articles by research design, for all 75 articles classified as research (one study had ill-defined methods and is not shown). (b) Number of research studies by type, for all articles with measurable outcomes (not all research studies reported measurable outcomes). (c) Number of studies by types of device tested, for all articles with measurable outcomes that tested devices.
Measuring outcomes
We found that a protocol and assessment system developed by the International Society for Prosthetics and Orthotics (ISPO) was the most commonly used method for evaluating lower limb (LL) prostheses in RLEs. ISPO’s assessment system includes collection of patient background information, use of the Harold Wood/Stanmore amputee assessment system, in-person patient follow-up through an interview assisted by an interpreter, and an examination of the patient and the device.3,4 Subject selection criteria are aimed at obtaining a homogeneous group of active male subjects aged 20–60 years, with amputations as a result of trauma, and with no significant mobility limitations. 4
Jensen et al. 5 proposed a set of benchmarks for transtibial prostheses in RLEs for several of the outcomes measured by ISPO’s system and later revised the benchmarks to higher standards. 6 They proposed benchmark values that assessed the following: use/nonuse of the prosthesis, ability to walk > 1 km/day, discomfort, pain, satisfaction, good socket fit, misalignment, insufficient craftsmanship, and need for a socket change. Raab and Jensen 7 proposed benchmarks for transfemoral prostheses in RLEs in four areas: improper craftsmanship, need for a new socket/prosthesis, patient compliance, and ability to walk > 1 km/day. We found no benchmarks for upper extremity (UE) prostheses or for orthoses. The transtibial and transfemoral benchmark values can be viewed as quality standards that service providers in RLEs should strive to attain. We considered cases that met or exceeded the benchmark values to be successful.
Outcomes for design
Commonly used outcomes to assess the success of design included durability, cost, and preference. One persistent problem for O&P devices in RLEs has been durability. Measures of device durability were reported in 24 articles (Table 1). It is interesting to note that there were no reported durability outcomes for UE prostheses. Although there are no benchmark values for durability or failures, benchmarks that could be related to durability are that a socket change is needed for 10% ± 5% of subjects with transtibial prostheses 6 and a new socket/prosthesis is needed for <20% of subjects with transfemoral prostheses. 7 However, the benchmarks do not specify when this should be assessed. Durability of prosthetic feet is one of the top concerns in RLEs, and the data indicate that polyurethane feet have a greater percentage of failures in a shorter time period, when compared to vulcanized rubber feet. The durability of prosthetic feet ranged from 11% failures at 9 months for the CR-SACH foot 8 to 86% failures at 5 (1–9) months for the Shape&Roll foot (mainly the foot cover). 9
Examples of measured outcomes related to durability.
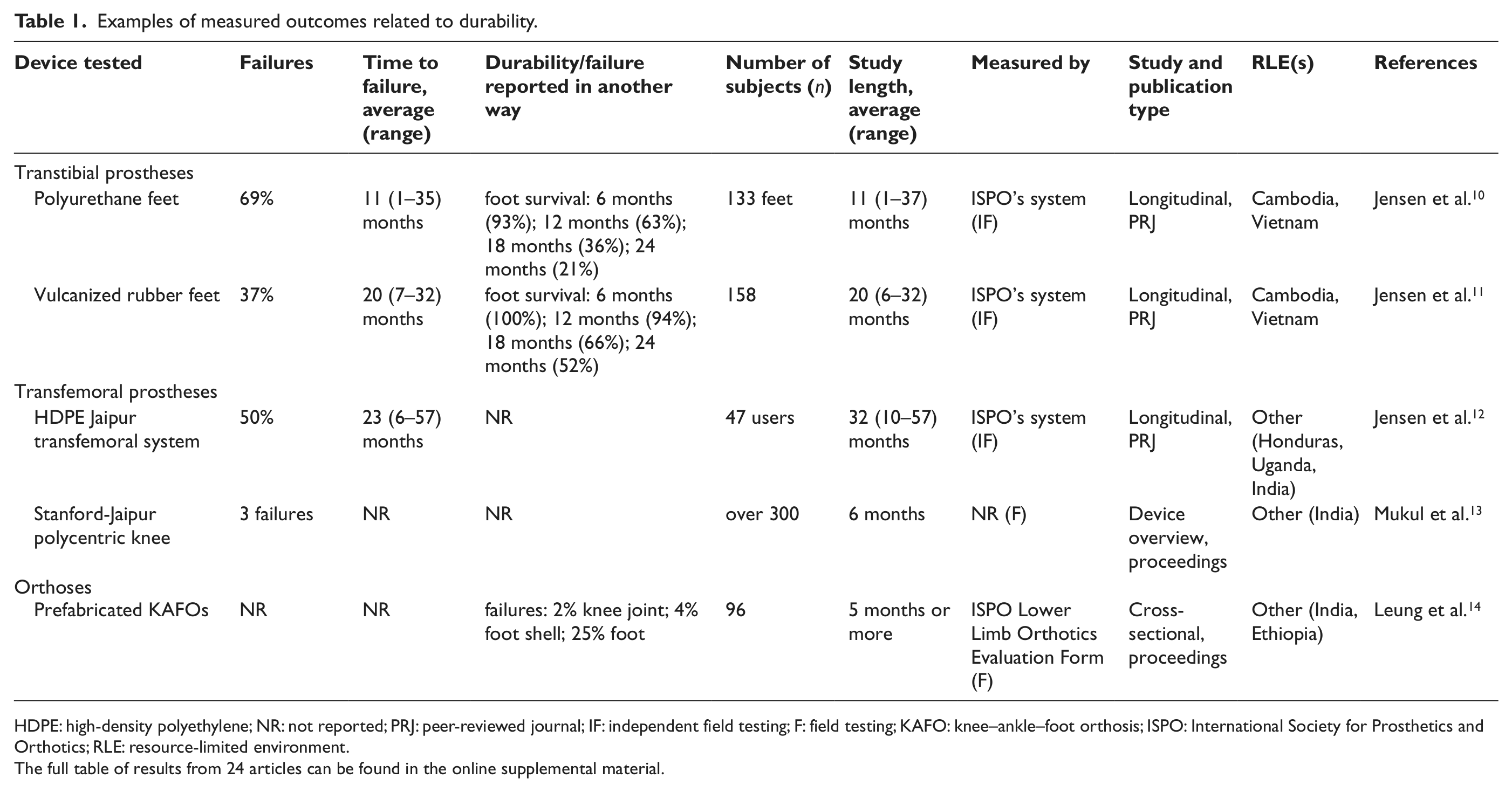
HDPE: high-density polyethylene; NR: not reported; PRJ: peer-reviewed journal; IF: independent field testing; F: field testing; KAFO: knee–ankle–foot orthosis; ISPO: International Society for Prosthetics and Orthotics; RLE: resource-limited environment.
The full table of results from 24 articles can be found in the online supplemental material.
An important consideration for successful design, manufacturing, distribution, and service provision was cost or affordability. The costs of 37 devices or components, and sometimes associated services, were reported (Table 2). Cost could be a reflection on many aspects of O&P provision, but is strongly linked to the design, including the selection of materials. There was a wide range of reported costs, with prosthetic feet ranging from US$5 to US$70 and prosthetic knees ranging from US$5 to US$300.
Examples of reported costs.
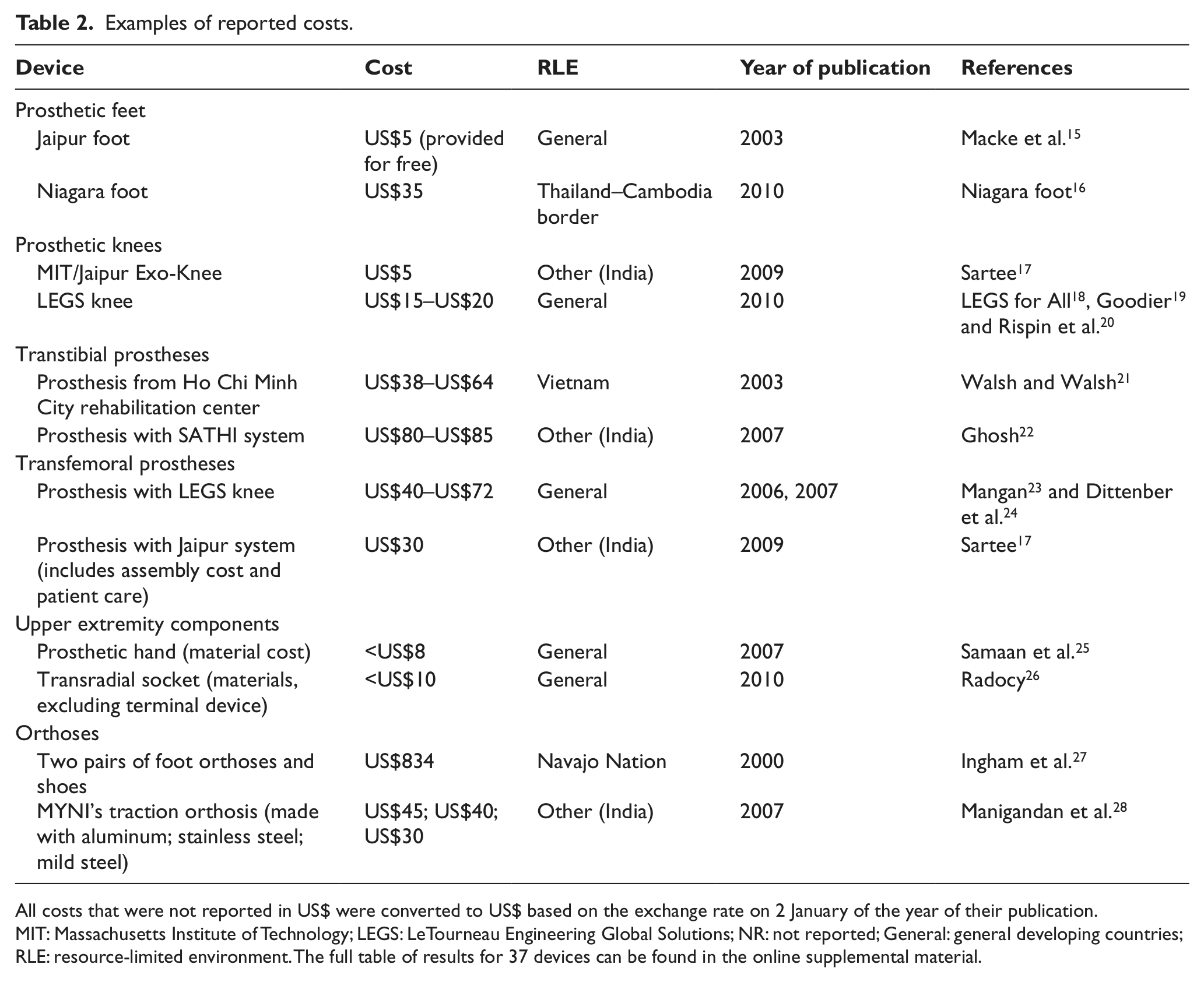
All costs that were not reported in US$ were converted to US$ based on the exchange rate on 2 January of the year of their publication.
MIT: Massachusetts Institute of Technology; LEGS: LeTourneau Engineering Global Solutions; NR: not reported; General: general developing countries; RLE: resource-limited environment.The full table of results for 37 devices can be found in the online supplemental material.
Preference of one device or method over another was reported in eight studies (Table 3). These studies measured subjects’ preference using surveys, either by interview or self-administered survey. Preference indicated the relative success of a device or method, but it is not easy to extrapolate the results to other devices or methods.
Preference.
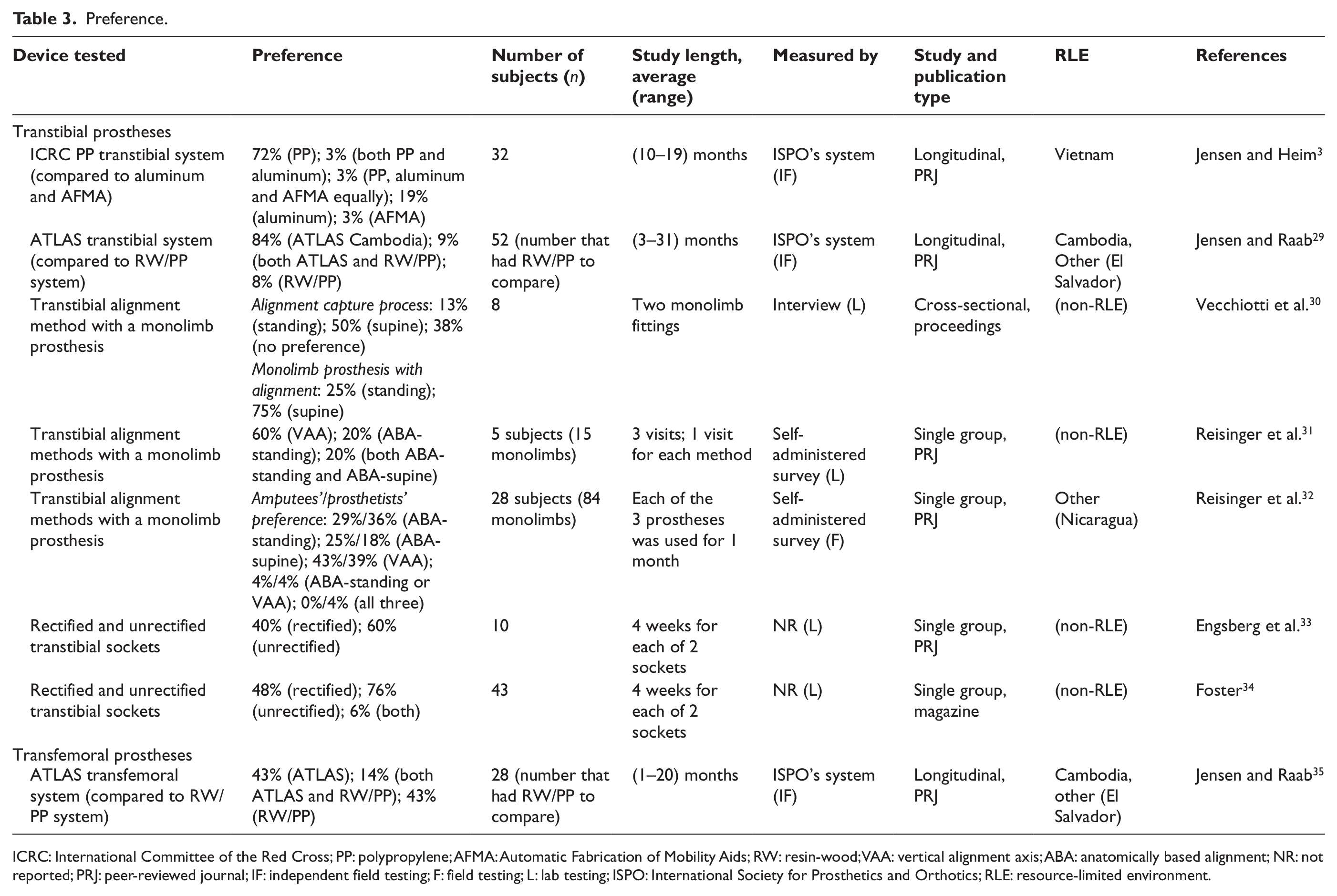
ICRC: International Committee of the Red Cross; PP: polypropylene; AFMA: Automatic Fabrication of Mobility Aids; RW: resin-wood; VAA: vertical alignment axis; ABA: anatomically based alignment; NR: not reported; PRJ: peer-reviewed journal; IF: independent field testing; F: field testing; L: lab testing; ISPO: International Society for Prosthetics and Orthotics; RLE: resource-limited environment.
Conclusions about design
Studies of prosthetic systems recommended the use of the International Committee of the Red Cross (ICRC) polypropylene system and the SATHI system, but did not recommend the ATLAS system. One study evaluated ICRC polypropylene prosthetic technology for transtibial prostheses and concluded that it was a durable system and was recommended. 3 A further study concluded that both resin-wood and ICRC polypropylene systems were acceptable designs for transfemoral prostheses. 36 A study of the SATHI system concluded that more work was needed to fix some technical problems, but the SATHI system could be recommended for developing countries. 22 Two studies that tested the ATLAS system for transtibial and transfemoral prostheses found the ATLAS system to be unacceptable due to high failure rates and safety concerns.29,35
Several authors investigated the design of monolimbs (transtibial prostheses with an integrated socket and pylon made from one sheet of thermoplastic material) in areas related to acceptance, dynamic properties, and fatigue failure. One study found that the new design of the monolimb was not always accepted by subjects in a study in rural China. 37 Lee et al. 38 concluded that a monolimb with an elliptical-shaped pylon may have some effects similar to a dynamic energy return prosthetic foot and found an elliptical shank monolimb to be more flexible than a circular shank monolimb. Chen et al. 39 calculated the fatigue failure probability and determined that after 200,000 steps, the patient should have the monolimb inspected and possibly replaced to prevent fatigue failure. Another study fatigue tested two elliptical shank monolimbs for up to 500,000 cycles and concluded that proper design of the foot bolt adapter was crucial. 40 Overall, the monolimb is recommended for its low cost and light weight, but the shape of the shank and design of the foot bolt adapter should be carefully considered when designing monolimbs.
Many researchers conducted field testing on different prosthetic feet commonly used in, or specifically designed for, RLEs. One independent field test investigated four different polyurethane feet and concluded that none could be recommended for tropical developing countries. 10 Another study compared five different vulcanized rubber feet and found the VI-Solid Foot and VI-Cavity Heel, both made by Vietnam Veterans of America Foundation in Cambodia, to be the best. 11 These low-cost feet were considered durable and were locally manufactured in Cambodia. An evaluation of two Jaipur vulcanized rubber feet concluded that they were not more durable than the other vulcanized rubber feet from Cambodia that were previously tested in the aforementioned study. 41 One study compared the Niagara foot to the stationary ankle flexible endoskeleton (SAFE) foot and concluded that the Niagara foot met the needs in RLEs in terms of cost, durability, and simplicity. 42 The Niagara foot was evaluated in the field and received positive feedback from users such as being lightweight, 43 comfortable, 44 and durable.44,45 However, field testing also lead to the recognition that the durability of the cover needed to be addressed,44,45 the heel flexibility was a concern for some subjects, 45 and the cosmesis and ability to fit into a shoe were also issues.43,44 The Shape&Roll foot was field tested and the investigators concluded that the Shape&Roll foot improved subjects’ walking performance.46,47 However, another field test of the Shape&Roll foot found that the polyurethane cosmetic cover, which was not sealed on the top or glued to the keel, was unsatisfactory and recommended that the Shape&Roll foot not be used. 9 Overall, vulcanized rubber feet are recommended over polyurethane feet for their durability. These studies highlight the importance of field testing in identifying factors important to the end users and also areas for improvement in the design.
In addition to field testing, mechanical and analytical testing were also utilized to evaluate prosthetic feet. Several authors performed ISO 10328 testing on prosthetic feet used in developing countries. Jensen and Treichl 48 tested 21 different feet and found that only 1 (HCMC foot) passed the static proof test, but of the 18 feet that underwent cyclic testing, all passed two million cycles. Goh et al. 49 tested 24 feet and did not report results of the static proof test but stated that the feet which did pass the static proof test underwent the static failure test and two of those feet did not pass the static failure test. All feet passed the cyclic test. In another study, five Shape&Roll prosthetic feet (one with a polyurethane cover) were tested to over 2 million cycles without failure. 50 The SACH foot manufactured at the Tanzania Training Centre for Orthopaedic Technologists (TATCOT) underwent cyclic testing, and the authors concluded that the feet would last 5 years for users walking 2 km/day. 51 Glynn et al. 52 used finite element analysis to determine locations of stress concentrations in prosthetic feet and found them to be anterior to the ankle and in the saddle region. An investigation that characterized prosthetic feet commonly used in developing countries concluded that the roll-over shape was a useful design tool for prosthetic feet with regard to walking function, but that walking function may not be the most important factor to the end user. 53 Mechanical and analytical testing indicate that the design of prosthetic feet still needs to be improved, and we recommend these types of testing during the design process.
Studies involving prosthetic knees were not common although research and development activities for a few new knees were reported. One study tested a prototype stance-control knee and found that it improved gait and had more reliable stance control compared to the subjects’ conventional knees. 54 Dittenber et al. 24 reported that ISO 10328 testing of the LeTourneau Engineering Global Solutions (LEGS) knee indicated that the knee should last for at least 2 years, but field test results were not yet conclusive. In addition, they considered the design goal of being low cost to have been met with the knee costing US$72. Rispin et al. 20 evaluated the LEGS M1 knee and concluded that it was an affordable and stable option for RLEs. Mukul et al. 13 developed and field tested the Stanford-Jaipur knee. They reported benefits of the polycentric design, and stated that the knee was extremely affordable, although the price was not given. The conclusions from these studies imply that these knees have great potential for use in RLEs. However, independent testing still needs to be conducted.
Research on UE prostheses was limited to evaluations of prototypes and one survey of compliance and acceptance. One case study evaluated a plastic soda bottle socket for a transradial prosthesis and concluded that it was an appropriate solution in contexts with limited financial and human resources. 26 Sitek et al. 55 tested prototype transradial and transhumeral prostheses on five subjects and identified areas for improvement including grip strength and comfort but concluded that the prostheses were adequate for light use. A survey of 71 patients with UE amputations found that the top two reasons for inadequate prosthesis usage were repeated mechanical failure and high costs associated with repair and replacement. 56 More research and development, which should include field testing, is needed to advance the field of UE prosthetics.
Research related to orthoses was not common, especially for evaluating design. Field testing of the prefabricated knee–ankle–foot orthosis (PFKAFO) revealed that most of the prefabricated shells fit appropriately but increasing the number of sizes of shells would be beneficial.14,57 Although several studies included the use of foot abduction braces (FABs), they did not evaluate the design of the FABs. Further research on the design of FABs and other orthoses used in RLEs is needed.
Outcomes for manufacturing and distribution
One outcome to assess the successfulness of manufacturing and distribution is the number of devices or components manufactured or distributed. However, this was rarely reported, and when it was reported, we were often unable to determine whether the authors were referring to manufacturing versus fabricating or distributing versus delivering. Therefore, all data related to the number of devices or components produced, distributed, or delivered were analyzed together and are discussed with other service provision outcomes.
Conclusions about manufacturing and distribution
Few research studies drew conclusions related to manufacturing and distribution, and none directly compared local versus centralized manufacturing, which was an unresolved issue discussed in Part One of this series. However, prosthetic feet that were produced from local manufacturing and centralized manufacturing were analyzed. Jensen et al. 10 tested four polyurethane feet and found that the CIREC foot, which was locally manufactured in Colombia, outperformed the CR-SACH foot, which was produced from centralized manufacturing. In another study, two locally manufactured vulcanized rubber feet were found to be sufficiently durable. 11 Specific manufacturing processes were rarely discussed, but two studies tested CR-SACH feet with a new manufacturing process and concluded that the new polymerization method was successful because it improved the life span of the foot.8,58 Very few studies have reported information about the benefits or drawbacks of local versus centralized manufacturing, thus more information is needed to identify best practices for specific contexts.
Outcomes for programs and service provision
The majority of reported outcomes were related to general O&P programs and service provision and included quality of life (QoL), satisfaction, use of device, degree of utilization, walking speed, quality of services, service time, number of devices produced or delivered, and number of service providers.
Of significance is that only six articles reported measures of QoL, inclusion, or participation. One study used the Pediatric Quality of Life Inventory (PedsQL™) to compare health-related QoL between children with unilateral LL amputations in Cambodia and Norway. 59 The PedsQL total scores were 80.6 for the Norwegian children and 57.4 for the Cambodian children. It was not clear whether the lower QoL for the Cambodian children was related to prosthetic services or other differences between the two countries. Powell et al. 60 measured QoL in Cambodia using the Comprehensive Quality of Life Scale—Adult—Fifth Edition (ComQOL-A5), which was adapted and translated for use with a Khmer-speaking population and administered via interview. They compared QoL among 164 subjects divided into groups based on the amount and type of rehabilitation services they received, and they concluded that rehabilitation services had a significant impact on improving the QoL of individuals who used O&P devices and other mobility aids. Engsberg et al. 33 used the Prosthesis Evaluation Questionnaire (PEQ) to compare QoL with a transtibial prosthesis with a rectified socket for 4 weeks versus an unrectified socket for 4 weeks and found no significant difference (PEQ score = 82% ± 12% for rectified sockets and 83% ± 12% for unrectified sockets). Another article described a similar but larger study by Engsberg which again used the PEQ to measure QoL and again found no difference between the group with the rectified sockets (PEQ score = 82% ± 11%) and unrectified sockets (PEQ score = 81% ± 13%). 34 A survey in Cambodia of individuals with mobility impairments, including those who used O&P devices, investigated challenges they faced. 61 Using a study-specific questionnaire, they found that exclusion and discrimination were evident in ways such as being called names, being made fun of for the way they walked, in school attendance, and in discrimination in entering marriage. One study reported a positive relationship between having an assistive device (including prostheses and mobility aids) and school attendance or employment, for four countries in southern Africa, including Malawi, but could not conclude that this was a causative relationship. 62 More studies to assess inclusion, participation, and QoL of orthosis/prosthesis users are needed to ensure that O&P devices and services are having a positive impact on the end user.
User satisfaction and/or the percentage of subjects who used their device were reported in 28 articles (Table 4). The benchmark for satisfaction for individuals with transtibial prostheses is 90% ± 5%; 6 there are no benchmarks for individuals with transfemoral prostheses. Of the 12 studies that measured satisfaction with transtibial prostheses, 9 met or exceeded the benchmark. The benchmark for use of a transtibial prosthesis is 95% ± 5%; 6 for transfemoral prostheses the benchmark is >80%. 7 Of the 15 studies that measured use with transtibial prostheses, 11 met or exceeded the benchmark; 2 of 3 studies for transfemoral prostheses exceeded the benchmark. On average, a greater percentage of subjects with transtibial prostheses were satisfied and used their prostheses, compared to subjects with transfemoral prostheses. This is not surprising and is also reflected in the fact that the benchmark for use of the prosthesis is greater for transtibial than transfemoral prostheses. However, this does indicate that more needs to be done to improve the provision of transfemoral prostheses.
Examples of satisfaction (percentage of subjects satisfied unless otherwise noted) and use of device (percentage of subjects who used their device).
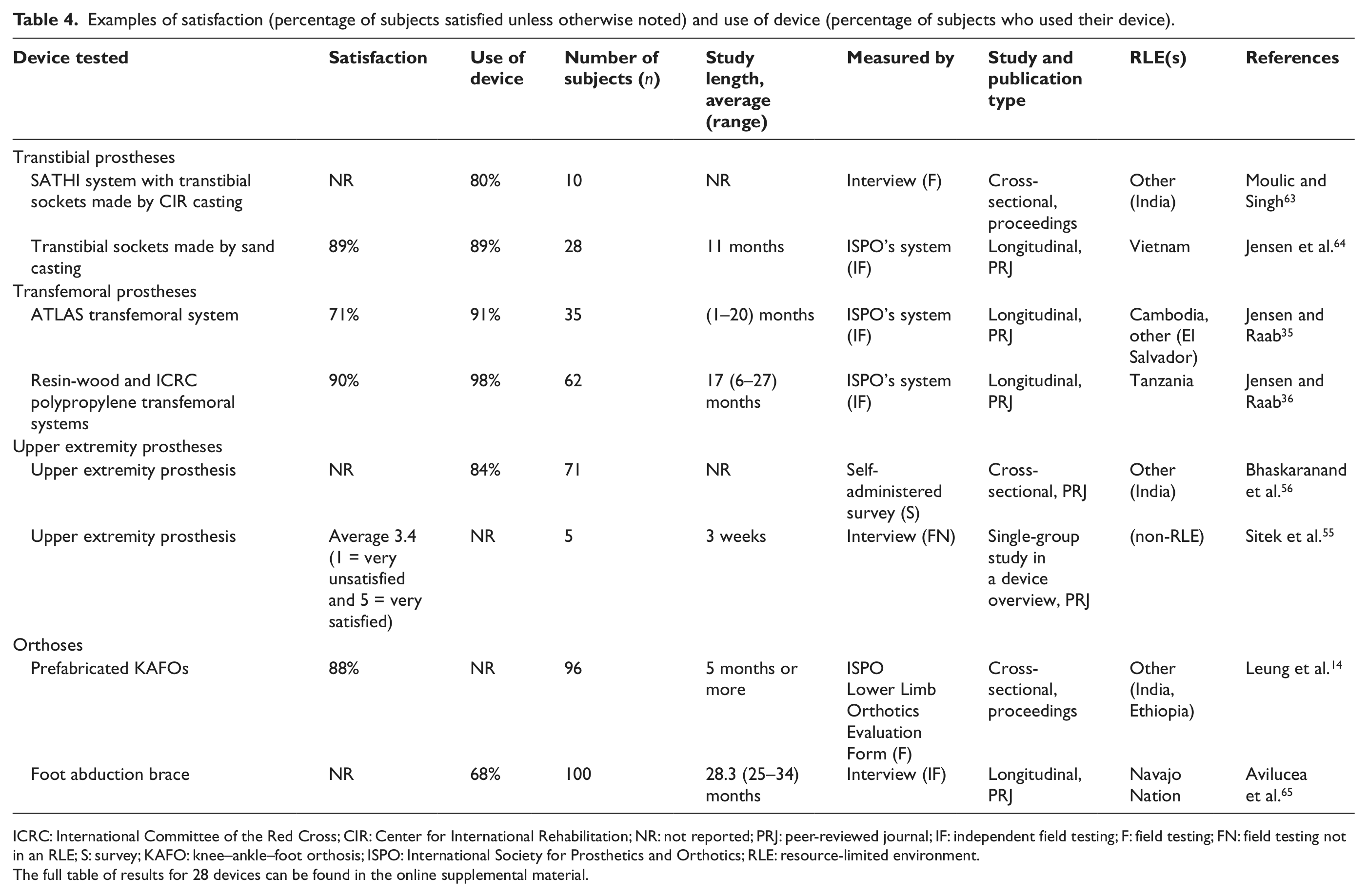
ICRC: International Committee of the Red Cross; CIR: Center for International Rehabilitation; NR: not reported; PRJ: peer-reviewed journal; IF: independent field testing; F: field testing; FN: field testing not in an RLE; S: survey; KAFO: knee–ankle–foot orthosis; ISPO: International Society for Prosthetics and Orthotics; RLE: resource-limited environment.
The full table of results for 28 devices can be found in the online supplemental material.
Mobility-related outcomes included the degree of utilization of a device, usually reported as the percentage of subjects who walked >1 km/day with their device, and walking speed (Table 5). The transtibial benchmark for individuals who walk >1 km/day is 90% ± 5%; 6 for transfemoral prostheses, the benchmark is >75%. 7 Only 5 of the 12 studies that recorded the percentage of subjects with transtibial prostheses who walked >1 km/day met or exceeded the benchmark; for transfemoral prostheses, only 1 of 3 studies met the benchmark. There are no benchmark values for any speed-related parameters. Other measured gait parameters included number of subjects exhibiting specific gait deviations, 3 rated improvement in walking performance over uneven ground, 47 number of subjects who walked with good stability, 14 improvement in physiological cost index, 66 and roll-over shapes with different prosthetic feet. 53 Standard metrics for analyzing gait are needed to enable comparisons among studies.
Examples of distance-related and speed-related walking parameters.
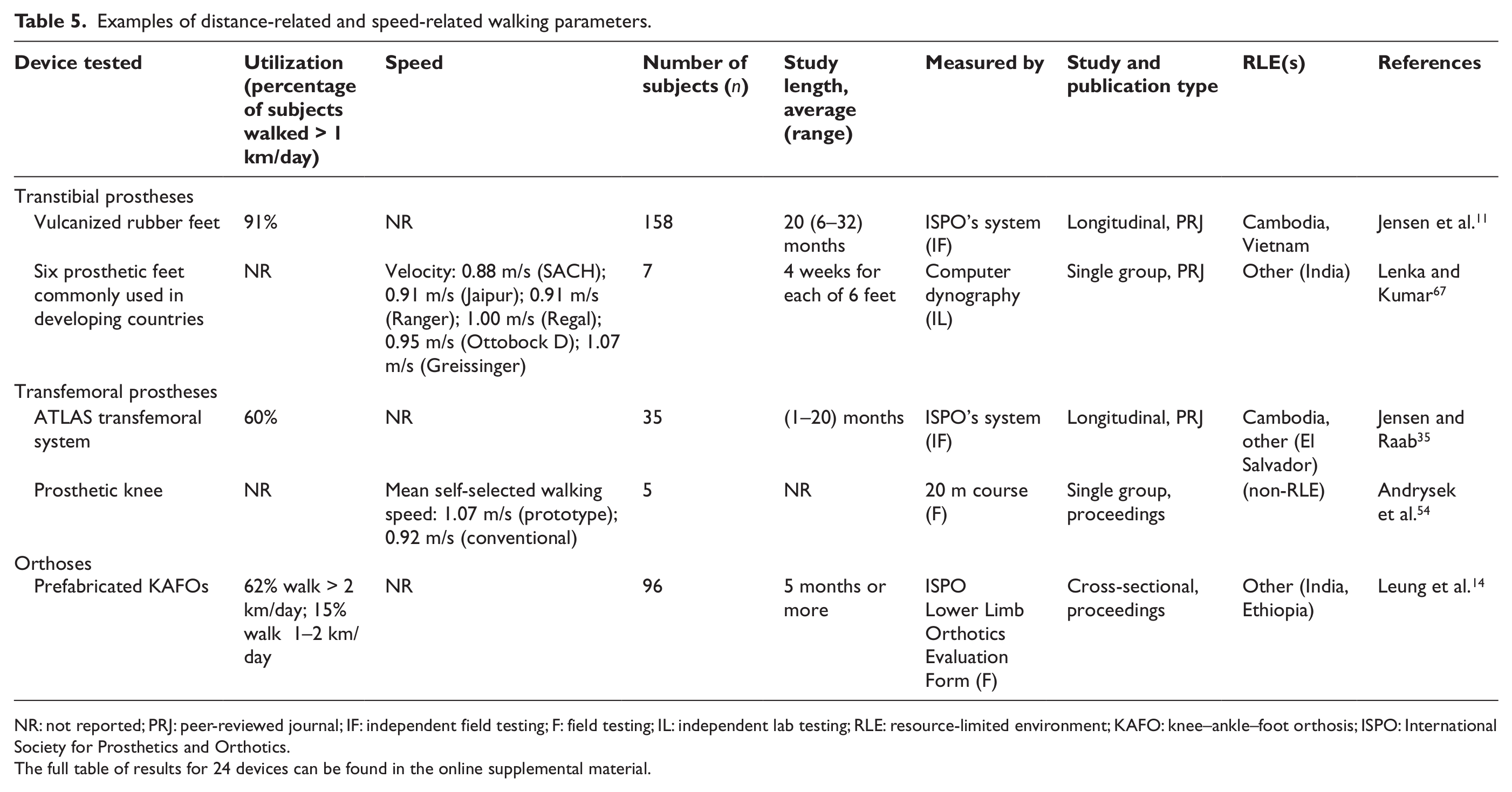
NR: not reported; PRJ: peer-reviewed journal; IF: independent field testing; F: field testing; IL: independent lab testing; RLE: resource-limited environment; KAFO: knee–ankle–foot orthosis; ISPO: International Society for Prosthetics and Orthotics.
The full table of results for 24 devices can be found in the online supplemental material.
Some indicators of the quality of services include discomfort, pain, good socket fit, and misalignment; they were reported in 21 studies (Table 6). There were no reported outcomes for these parameters for UE prostheses. Transtibial benchmarks for these outcomes are as follows: 5% ± 5% of individuals report discomfort, 5% ± 5% of individuals report pain, 60% ± 5% of sockets are assessed to have a good fit, and 10% ± 5% of prostheses are assessed to be misaligned; 6 there are no transfemoral benchmarks for these specific outcomes, although there is a benchmark for improper craftsmanship, which is <35%. 7 The number of studies that met or exceeded benchmark values were as follows: 3 of 9 studies that reported discomfort, 5 of 11 studies that reported pain, 9 of 16 studies that reported good socket fit, and 5 of 9 studies that reported misalignment. These results suggest that there is much room for improvement in the quality of services.
Examples of measures of quality of service: pain and discomfort, socket fit, and misalignment.
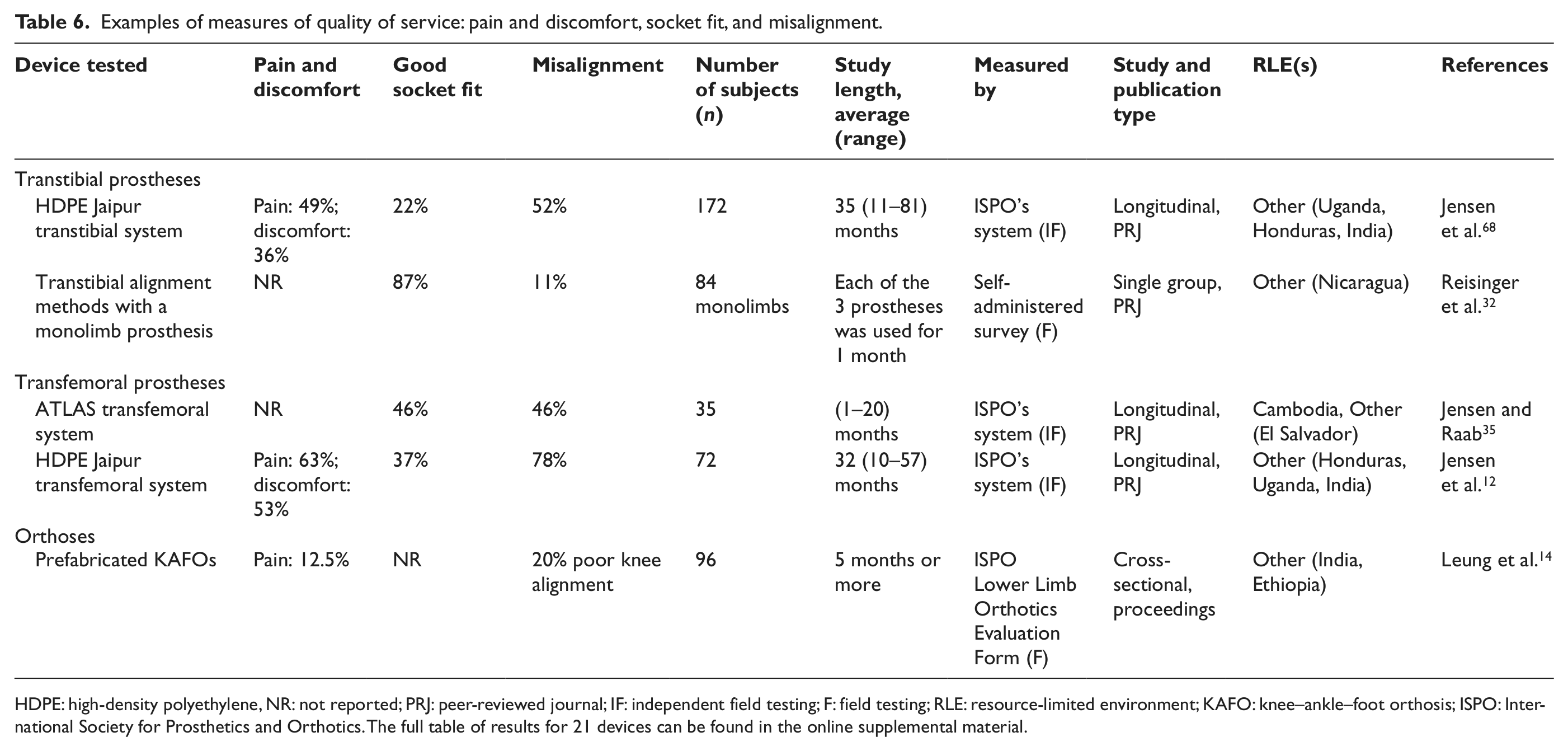
HDPE: high-density polyethylene, NR: not reported; PRJ: peer-reviewed journal; IF: independent field testing; F: field testing; RLE: resource-limited environment; KAFO: knee–ankle–foot orthosis; ISPO: International Society for Prosthetics and Orthotics. The full table of results for 21 devices can be found in the online supplemental material.
Many program and device overviews published in magazines, reports, conference proceedings, and on the Internet provided information about the number of devices produced, distributed, or delivered (Table 7). In general, a high number of devices may indicate successful service provision, manufacturing, or distribution and may also reflect on the sustainability and impact of a program.
Examples of number of devices delivered, distributed, or produced.
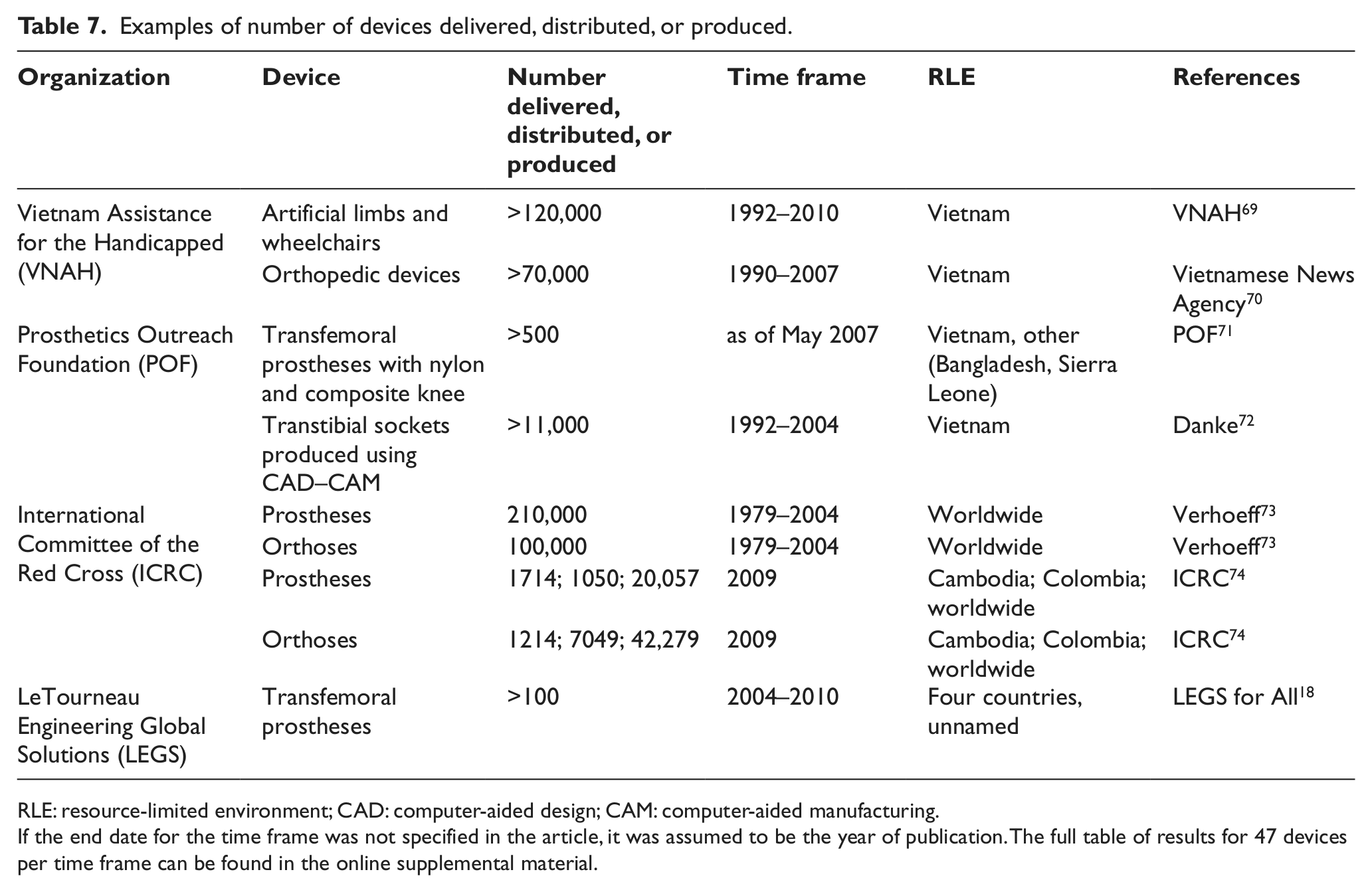
RLE: resource-limited environment; CAD: computer-aided design; CAM: computer-aided manufacturing.
If the end date for the time frame was not specified in the article, it was assumed to be the year of publication. The full table of results for 47 devices per time frame can be found in the online supplemental material.
The number of service providers in the target RLEs offered insight into the current state of service provision. According to Harte, 75 one service provider (trained to ISPO Category-I or Category-II level) is required for every 500 individuals in need of orthotic devices or services. Based on population estimates, we calculated the number of service providers needed for our six target RLEs, and we can clearly see that there is a substantial lack of service providers in the target RLEs (Table 8).
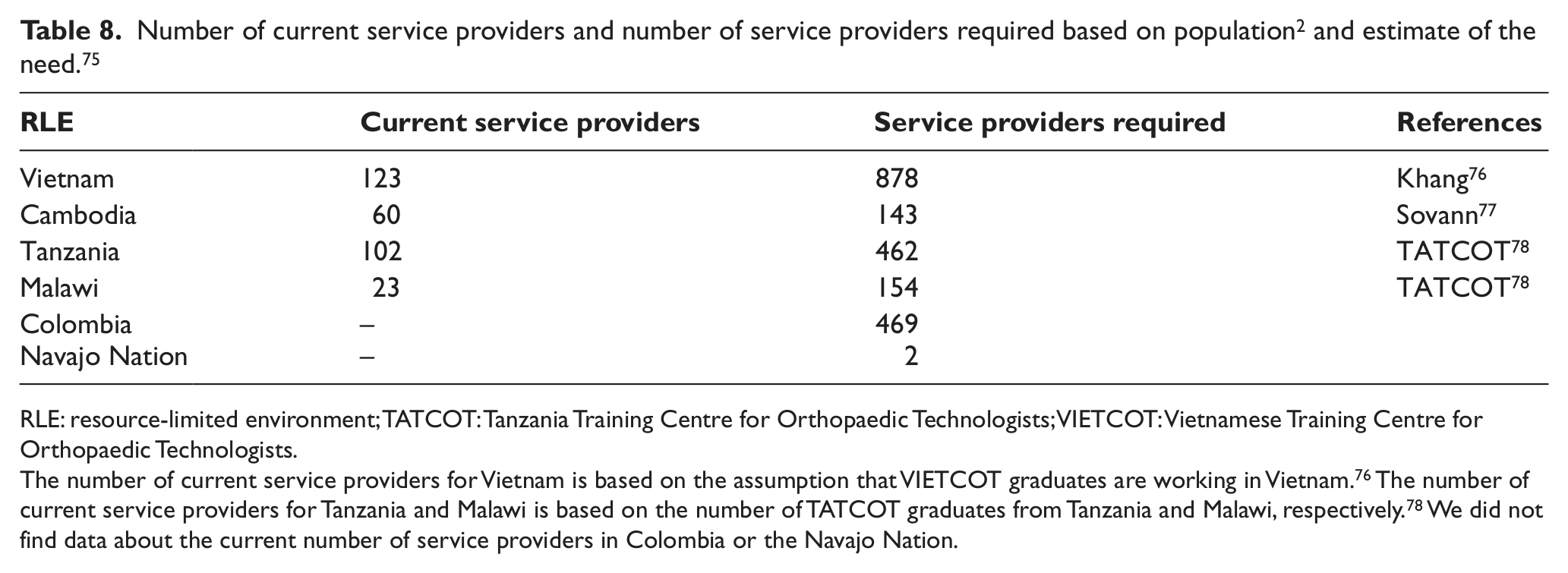
RLE: resource-limited environment; TATCOT: Tanzania Training Centre for Orthopaedic Technologists; VIETCOT: Vietnamese Training Centre for Orthopaedic Technologists.
The number of current service providers for Vietnam is based on the assumption that VIETCOT graduates are working in Vietnam. 76 The number of current service providers for Tanzania and Malawi is based on the number of TATCOT graduates from Tanzania and Malawi, respectively. 78 We did not find data about the current number of service providers in Colombia or the Navajo Nation.
Conclusions about programs and service provision
Several articles evaluated different methods of taking an impression and fabricating transtibial sockets. One goal of these methods was to make service provision faster and/or easier. Abu Osman et al. 79 compared a transtibial socket made from a hydrocast method to a standard patellar-tendon-bearing socket and found the hydrocast socket to be more comfortable. Two studies tested sand casting for transtibial sockets and concluded that it was more cost-effective than casting with plaster of Paris, 80 but did not eliminate the need for a professional prosthetist. 64 Two studies evaluated Center for International Rehabilitation (CIR) casting, the technique that evolved from sand casting, and concluded that it was simple, cost-effective, took less time, 63 and produced a good fit. 81 Two studies by Engsberg used alginate to take an impression of a transtibial residual limb, made rectified and unrectified positive plaster models, and then compared the rectified and unrectified sockets.33,34 They concluded that the sockets were similar and the unrectified socket was more often preferred. A good socket fit is extremely important for the user’s comfort, and an advanced level of training is usually required to take an impression and fabricate a well-fitting socket. These methods show potential to simplify the processes, and with further development, they could possibly be used by service providers with an intermediate level of training to produce well-fitting sockets.
Six articles evaluated alignment methods for transtibial prostheses. Hansen et al. 82 analyzed roll-over shape alignment and concluded that although it did explain alignment in the sagittal plane, it did not provide the complete answer for alignment. Two studies evaluated an alignment system specifically designed for monolimbs and found that a supine alignment capture method was preferred over a standing method, 30 and although alignment was generally very good, it was not as good as dynamic alignment by a skilled prosthetist. 37 The vertical alignment axis (VAA), anatomically based alignment—supine (ABA-supine), and anatomically based alignment—standing (ABA-standing) methods were compared in two studies, which concluded that all three methods could be used for outreach services 31 and that there is a wide range of alignments that are considered acceptable. 32 One study compared the VAA, ABA, and traditional bench alignment and did not find any differences. 83 Proper alignment is crucial for a well-functioning prosthesis. These studies showed that there may be more than one way to produce an acceptable alignment, but more research is needed.
The Ponseti method for clubfoot treatment, including the use of FABs, was investigated by several studies, although the main focus was not the FABs. The availability of FABs,84,85 patient compliance with follow-up, 86 and compliance with the FAB protocol65,87 were important in determining the outcome of the treatment. One study concluded that orthopedic clinical officers could effectively use the Ponseti method to treat clubfoot in Malawi 88 . The Ponseti method seems to be well suited for RLEs, and more research specific to the FABs should be conducted.
Outcomes for technology transfer
One measure of the successfulness of knowledge translation through a formal training program is the number of graduates the program produces. There are three Category-II training institutes in the target RLEs, the Cambodian School of Prosthetics and Orthotics (CSPO), Vietnamese Training Centre for Orthopaedic Technologists (VIETCOT), and TATCOT, which together have produced 737 graduates (Table 9). In addition, the longevity of these schools indicates their sustainability.
Total number of graduates from formal training institutes from the date the institute was founded until the most recent data available.
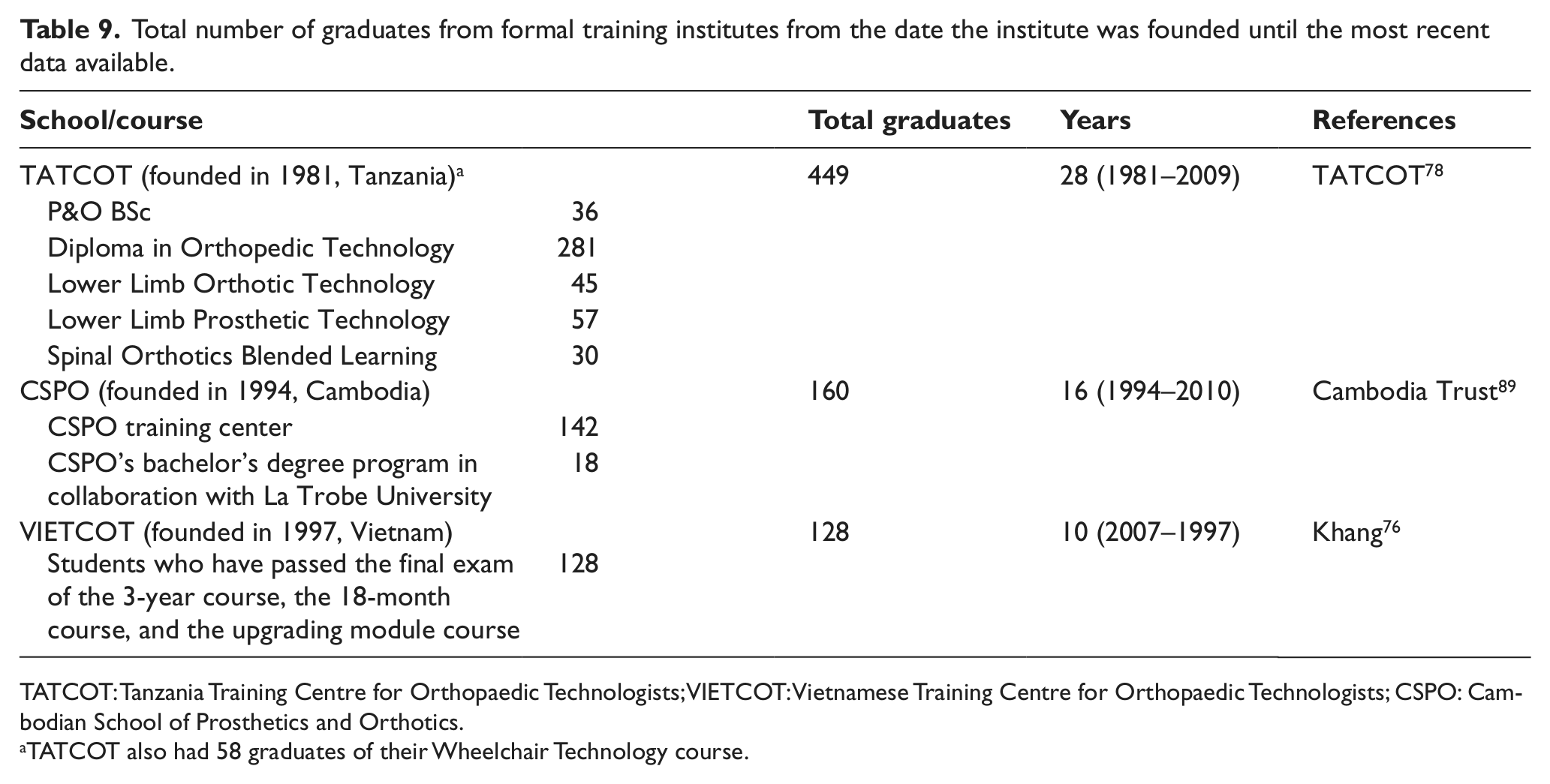
TATCOT: Tanzania Training Centre for Orthopaedic Technologists; VIETCOT: Vietnamese Training Centre for Orthopaedic Technologists; CSPO: Cambodian School of Prosthetics and Orthotics.
TATCOT also had 58 graduates of their Wheelchair Technology course.
Conclusions about technology transfer
Four research articles drew conclusions related to knowledge translation, and two research articles presented results directly related to technology transfer of techniques related to O&P service provision. One study assessed the impact of O&P guidelines that were provided to centers in Vietnam and concluded that the guidelines were well known and used. 90 Kheng 91 conducted a survey of CSPO graduates and found that continuing professional development was crucial for providing the most up-to-date services to the end users. Another survey of students at CSPO found areas where they could improve their training program, concluding that regular evaluation of the program was necessary. 92 In Tanzania, a survey with an aim to improve training concluded that using modern information and communication technology with problem-based learning could be effective and affordable. 93 Reisinger et al. 32 transferred transtibial alignment techniques to prosthetists in Nicaragua and found a 23% improvement in quiz scores following hands-on training. The Ponseti method, including the use of FABs, was taught in a 3-day course in Vietnam, and a survey showed that 27 of 36 respondents were using the method after at least 12 months; 8 of the 9 respondents who were not using the method reported that they had not seen any clubfoot cases. 86 Measuring the results or effectiveness of technology transfer was not common, but is necessary, as was pointed out by the consensus documents discussed in Part One.
Discussion
Gaps in measured outcomes
According to many experts in the field and many of the consensus documents, inclusion, participation, and QoL of the end user are some of the most important outcomes of O&P provision.94–100 However, we found that measurements of inclusion, participation, or QoL were rare among all the articles in this scoping review; they were discussed in only six articles. Some studies that used ISPO’s system for data collection reported the subjects’ socioeconomic background by categorizing the subjects as child, student, skilled work, unskilled work, soldier/police, unemployed, or pension/retired. These categorizations may give some insight into the subjects’ inclusion or participation related to school attendance or employment, but they show a limited picture. Authors have concluded that more studies are needed to assess the impact of O&P provision on the end user’s social participation 98 and QoL,98,99 and the results of this scoping review highlight the desperate need for more of these types of studies.
The breakdown of studies according to type of device highlighted the gross lack of outcomes in the field of orthotics; only 4 of 58 articles dealt with orthotics. There were some studies related to the use of FABs for treatment of clubfoot, but they did not have any measurable outcomes that were related to the FABs. We note that there is a huge deficiency for orthotics, even though there is a greater need for orthotic services than prosthetic services.96,99,101
Areas for improvement
Researchers conducting studies involving human subjects should consider including more female subjects and obtaining and reporting on ethical approval. Most of the research involving human subjects was heavily biased toward male subjects. Subjects’ gender was often not reported, but when it was, males were much more common. In addition, ISPO’s system aims to select male subjects. 4 Prospective studies should aim to include more female subjects. We do acknowledge that the bias for male subjects in research studies could be a reflection of a general bias for men to more likely receive O&P devices and services. The World Health Organization (WHO) has recognized this issue and stated that there should be extra emphasis on services for women and girls. 1 Also related to human subjects’ testing, authors conducting studies in RLEs rarely reported whether or not they sought and obtained approval from an ethics committee or institutional review board for conducting their study. This should be reported for all studies involving human subjects.
Survey instruments that have been tested for reliability and validity in RLEs are greatly needed. The PEQ is a standard survey instrument for measuring QoL in individuals with LL amputations, and PEQ results were reported for two studies;33,34 a third study included PEQ in its methods but did not report results. 67 The PEQ has been shown to be reliable and valid, 102 although we found no information about these properties in RLEs. One study used the PedsQL 59 but did not report on its psychometric properties. Powell et al. 60 reported using the ComQOL-A5 complemented by additional independent population variables. The authors reported that their instrument underwent cross-cultural translation and adaptation from English to Khmer and was validated; however, the study lacked statistical power to fully test its reliability and validity. Jensen 103 investigated the use of the WHO Quality of Life–BREF (WHOQOL-BREF) as a tool for community rehabilitation workers to use to identify individuals who needed assistance, repair, or replacement of their orthosis or prosthesis. He concluded that the WHOQOL-BREF must be used in conjunction with a physical examination to determine those in need, but did not comment on its usefulness in measuring QoL. The use of the PEQ, PedsQL, ComQOL-A5, and WHOQOL-BREF has been quite limited with populations of orthosis/prosthesis users in RLEs, and more work is needed to test the reliability and validity of these surveys with these populations and in these settings.
Validated tools for measuring other outcomes such as durability, fit, and alignment are also needed. Durability was reported in several different ways; when a failure was reported, it was usually not specified whether it referred to the entire device or just one component. Good fit and misalignment are subjective parameters, and authors often did not state who made these determinations. Some authors who used ISPO’s system stated that the assessments were done by an orthopedic surgeon and an ISPO Category-I prosthetist/orthotist. The most commonly used protocol for field studies was ISPO’s system, but we found no information regarding the reliability, validity, or cross-cultural adaptation of the face-to-face interview of ISPO’s system. Jensen 4 stated that revisions had been made to ISPO’s system since they began field testing, with the goal of keeping the format simple, versatile, and not requiring cumbersome instructions. Rispin et al. 104 developed the preliminary LEGS Functional Parameters Questionnaire, which measured items such as daily time spent by walking, satisfaction with walking, standing comfort, walking balance, and agility. They conducted preliminary validation of the questionnaire on 19 subjects with transfemoral prostheses in Kenya and Bangladesh. Part of the Orthotics and Prosthetics Users’ Survey was included as a measure of satisfaction in one study, but the study’s methods were unclear. 59 Conclusions from the ISPO Consensus Conference on Appropriate Lower Limb Orthotics for Developing Countries recommended the development and use of standard tools and methods, 99 and it is clear from the data presented here that this would be very helpful to the research field. Moreover, for subjective assessments, authors should state how the assessments were made.
Outcomes related to recommendations and benchmarks for successful O&P provision
In Part One, we identified themes for successful O&P provision in RLEs based on recommendations from consensus documents. We also identified common O&P provision strategies from the full body of literature. Many of these themes and strategies do not readily lend themselves to being measured, but some do and are discussed below.
Designing for durability and considering the physical environment/climate were recommended for successful design in Part One. Durability was frequently measured, and although consideration of the physical environment/climate was not directly measured, its impact was discussed relative to the durability of many prosthetic feet. Durability was discussed at the State-of-the-Science on Appropriate Technology for Developing Countries Conference, and participants suggested that there should be a warranty for prosthetic feet for a minimum of 1 year, but ideally 5 years, 105 and that prosthetic knees should last 3 years without servicing and 5 years with servicing. 106
Designing devices for affordability and making service provision affordable were very frequently mentioned by the consensus documents. Standard practices and terminology for reporting costs are needed, as authors often did not state what devices and services were included in a cost or whether a given cost was the cost to the patient, service provider, or distributor. Guidelines for cost would need to take into account the economic setting to determine what would be considered affordable. At the State-of-the-Science on Appropriate Technology for Developing Countries Conference, participants suggested that the price of a prosthetic foot should be a percentage of the user’s average wage 105 and the economy of the region or nation. 106
One commonly reported design strategy for orthoses and LL prostheses was to be lightweight. There are no benchmarks or guidelines for weights of O&P devices, and few articles reported device weight. Guidelines for weights of components or devices would need to account for numerous variables related to the end user and type of device. Also, the weight of a device or a component may be inversely related to its durability; thus, the trade-off between weight and durability would need to be considered.
The consensus documents recommended having well-trained service providers and sustainable training programs. Three formal training institutes in the target RLEs have been operating for at least 15 years; their longevity can be considered evidence of their sustainability. The total number of graduates is an indication of the number of service providers receiving training through ISPO-recognized Category-II schools. Category II is considered an acceptable level for practitioners in developing countries, as an interim solution, with the goal being to move toward Category-I practitioners.1,107,108 Despite the productivity of these schools, there is a tremendous deficiency in the number of well-trained service providers in Vietnam, Cambodia, Tanzania, and Malawi.
One of the most common strategies for service provision of LL prostheses was to have quick services. Authors reported outcomes related to service time for casting and fabrication with the ATLAS transfemoral system, 35 fabrication of a Syme’s/Boyd prosthesis, 109 casting and fabrication methods for transtibial prostheses,63,80 assembly time for the PFKAFO, 110 and alignment capture and transfer time for different alignment methods. 32 Service time is another example of an outcome for which standard reporting terminology would be useful.
ISPO’s benchmarks are considered quality standards that those involved with provision of prostheses could strive to achieve. We compared study averages to the benchmarks and found that the benchmarks were frequently not being met. In addition, we compiled data from studies that measured satisfaction and found some conflicting results. Of 12 studies that measured satisfaction involving transtibial prostheses, 9 met the benchmark, and in fact, the average percentage of subjects satisfied for all 12 studies was 88%. However, for these same 12 studies, the average percentage of subjects with a good socket fit was only 52% (would not meet the benchmark) and only 80% of the prostheses were correctly aligned (would not meet the benchmark). This demonstrates a discrepancy between a high rate of satisfaction (88%) and lower rates of well-fitting sockets (52%) and correctly aligned prostheses (80%). There may be many explanations for the differences, but this again points to the need for standardized measurement instruments that are valid and reliable for measuring outcomes in RLEs.
Limitations
The tables presented in this article and in the online supplemental materials attempt to summarize large amounts of data from many different sources reported in many different ways. A line-by-line comparison of the data would need to take into account the numerous differences in the studies or reports that cannot be fully explained by the tables. In addition, when the number of subjects is reported in the tables, the number is the total for the study. However, the percentages reported for some parameters may not always be the percentage of the total number; sometimes they are a percentage of a subset, such as users, or it was not clearly stated. Some articles had conflicting data within the article itself.
Conclusion
O&P provision in RLEs would benefit from more high-quality research studies, although we realize that the logistics of conducting research in developing countries often present many significant obstacles. There are considerable gaps in the evidence base for reported outcomes of inclusion, participation, and QoL of O&P users in RLEs, and for all outcomes in orthotics. There is a noteworthy lack of representation of women as subjects in research studies, which may also reflect on a lack of services for women. The compilation of data from research studies highlights the need for standard, valid, and reliable methods of data collection and reporting.
An evidence base of available literature and reported outcomes has been presented to better inform and guide stakeholders in O&P provision in the six target RLEs and developing countries in general. We hope that the results presented here will help guide decision making and planning so that O&P provision can be more fruitful and successful.
Footnotes
Acknowledgements
The authors would like to thank Digital Active for developing the database used to store the data.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the US Department of Education, National Institute on Disability and Rehabilitation Research (grant number H133A090020).