
Abstract
Background:
When walking in footwear with a positive “heel sole differential”, the sagittal kinematics of the base of the footwear appear to mimic normal barefoot foot kinematics, creating an “effective foot,” yet sagittal shank, thigh, and trunk kinematics appear to remain unchanged. These observations have not been quantified.
Objectives:
To quantify these observations by assessing the effect of different heel sole differentials on sagittal shank and foot segment kinematics of able-bodied walking.
Study design:
Cross-sectional study.
Methods:
Gait data from 10 nondisabled females were collected while they walked with no-heel (mean heel sole differential = 0 (standard deviation = 0) mm), mid-heel (mean heel sole differential = 37 (standard deviation = 10) mm), and high-heel shoes (mean heel sole differential = 71 (standard deviation = 17) mm) to calculate the shank-to-vertical angle and foot-to-horizontal angle.
Results:
There were no significant differences between shoe conditions in stride lengths (p = 0.056) or shank kinematics between 0% and 50% gait cycle (p = 0.079). There were significant differences in foot kinematics (p = 0.000), with foot segment angle increasing with increasing heel sole differential.
Conclusion:
The ankle joint and actual foot segment adapt their kinematics to maintain consistent shank kinematics. The finding that heel sole differential and foot segment angle can be varied without influencing shank segment kinematics has implications for orthotic and prosthetic practice.
Clinical relevance
Heel sole differentials of footwear can be varied without implications for shank kinematics, which is relevant for both orthotics and prosthetics. Assessments and interventions with varying heel sole differential footwear may be helpful in patients with short calf muscle or restricted ankle motion who may walk more normally if an appropriate heel sole differential were provided.
Background
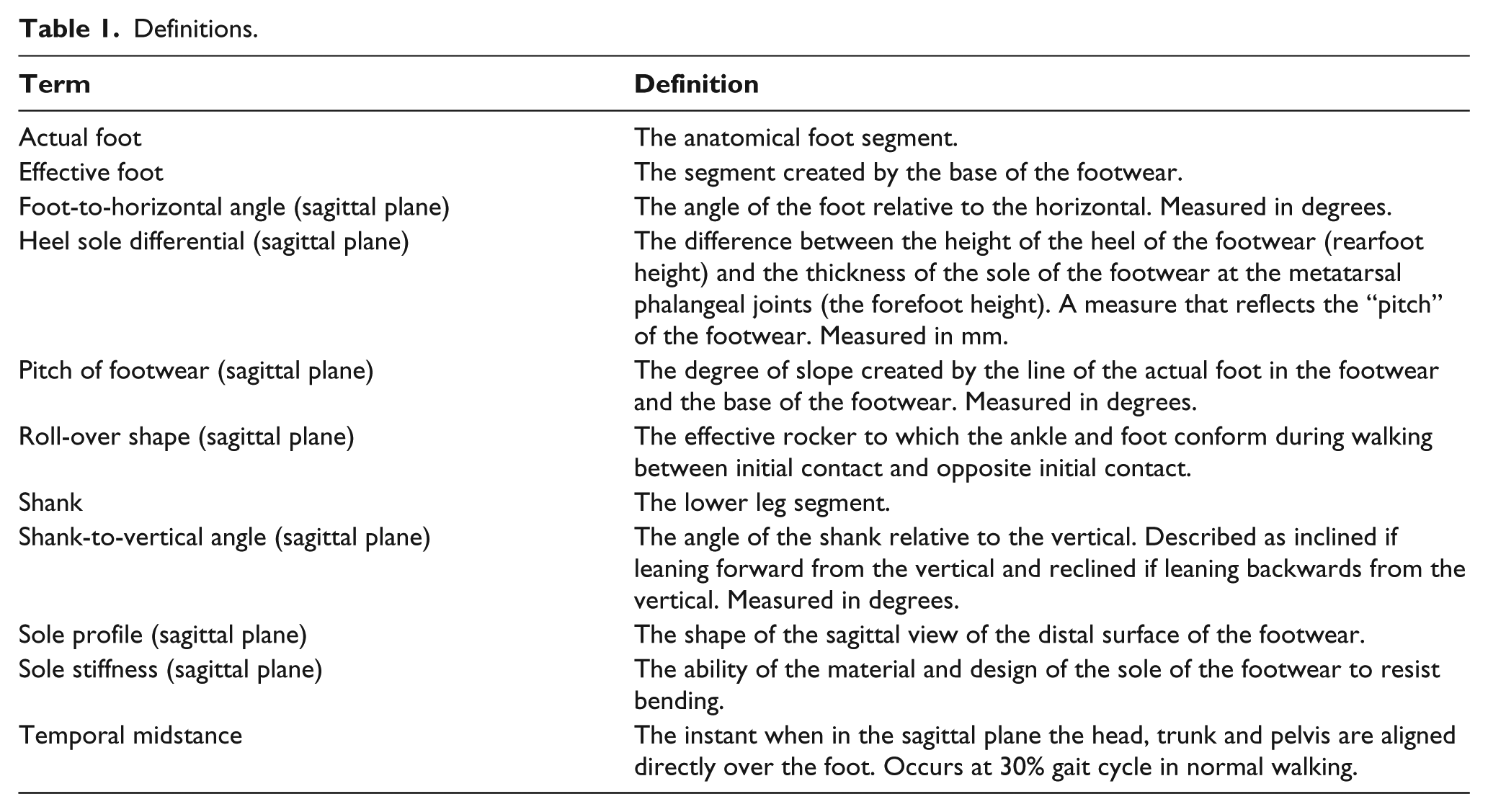
Adults and children walk in footwear that is described as being either “flat” or having a “heel.” Footwear with a heel has a positive pitch or “heel sole differential” (HSD); the difference between the height of the heel and the thickness of the sole of the footwear at the metatarsal phalangeal joints (MTPJs). When walking in footwear with a positive HSD, the sagittal kinematics of the base of the footwear appear to mimic the kinematics of the foot in normal barefoot walking creating an “effective foot” that is separate from the “actual foot.” Furthermore, sagittal lower leg (or shank), thigh, and trunk kinematics appear to remain unchanged. In fact, when observed by eye, walking in footwear with a positive HSD is virtually identical to walking barefoot except when very high-heel shoes are worn. These observations require description and quantification as they have not been previously reported and are an important phenomenon for orthotic and prosthetic practice. Table 1 provides definitions for terms used in this article.
Definitions.
When analyzing walking, it is usual to identify the orientation of the segments of the lower limbs and then calculate segment kinematics, joint kinematics, and joint kinetics. 1 Most gait laboratories report kinematics for all the major lower limb joints (hip, knee, and ankle) and provide segment kinematics only for the pelvis. There are rare exceptions where full sagittal segment data, for pelvis, thigh, shank, and foot, have been published for barefoot walking in children and adults.2–7 Shank kinematics for children were reported by Pratt et al. 8 and thigh kinematics for children by Sutherland and Olshen. 9 Reporting of segment kinematics was popular when gait analysis was first developed,2,4,10 but waned until a group of researchers became interested in the significance of segment kinematics to human walking and the development of intersegmental coordination in children.11,12 Other researchers used segment kinematics and center-of-pressure data to develop the “roll-over shape,” which is the effective rocker to which the ankle and foot conform between initial contact and opposite initial contact,13–17 and segment kinematics have become important for “tuning” orthoses.8,18–22
Despite a resurgent interest in segment kinematics, there remains a paucity of segment kinematic data for walking shod. Inman et al. 2 presented sagittal thigh, shank, and foot segment data for one footwear condition. Observational segment kinematics have been reported for barefoot compared to high heels.18,20 There are some reports comparing walking barefoot and shod where the pelvis segment and lower extremity joint kinematics data were provided.23,24 One report compared barefoot and shod gait in children, reporting sagittal pelvis segment data. 25 Roll-over shapes have been reported for walking in footwear with a variety of HSDs, 26 a variety of sole profiles, 27 and ankle-foot orthoses. 28 Recently, shank segment kinematics have been reported for adults walking in ankle-foot orthoses. 29 However, there are no reports of shank and foot segment kinematics when walking in footwear of varying HSDs.
Analysis of segment data in footwear with varying HSD is clinically relevant as clinicians observe both segments and joints, and it may be possible to determine whether joint kinematics adapt to maintain constant segment kinematics or vice versa; if one changes to maintain the other, this has implications for rehabilitation practice. If ankle joint kinematics adjust to maintain normal segment kinematics, then it should be possible to find a pitch of footwear that will allow patients with short calf muscle or restricted ankle motion to walk with normal or improved effective foot and shank segment kinematics. For patients who use orthoses and prostheses, adjusting joint and segment alignments may help achieve normal effective foot and shank kinematics, and more proximal segment and joint kinematics.
Evaluation of walking in footwear with varying HSDs in adults, children, and patients is required but has not been reported. Hence, the purpose of this study was to assess the effect of footwear with different HSDs (no-heel, mid-heel, and high-heel) on the sagittal shank and foot segment kinematics of walking in able-bodied adult persons. We hypothesized that (1) stance-phase shank kinematics would not change with changes in HSD of footwear and (2) stance-phase actual foot kinematics would change with changes in HSD of footwear, with actual foot angle increasing with increasing HSD of footwear. These hypotheses are consistent with previous reports that the pattern of ankle motion is very similar for shoes with different HSDs, but shifted toward plantar flexion as the HSD increases, 30 and that roll-over shapes remain consistent for a variety of HSDs. 26
Method
This study was a retrospective analysis of cross-sectional data previously reported by Hansen and Childress. 26 The study was originally approved by the University’s Institutional Review Board. All subjects provided written informed consent prior to participating.
The methods were described in detail by Hansen and Childress 26 and recapped here. Walking data were recorded from a convenience sample of nondisabled adult female volunteers experienced in walking with shoes with different HSDs. No familiarization time with the different footwear conditions was provided given that subjects brought their own mid-heel and high-heel shoes for the study. Subjects were provided with a third pair of no-heel shoes that had a zero HSD and flexible soles for traction. High-heel shoes were required to have a sturdy, stable heel, not a stiletto heel. While not directly assessed, the mid- and high-heel shoes had soles that were flexible at the MTPJs, but nearly all the high-heel shoes were fairly stiff behind the MTPJs. The HSD of all the shoes were measured.
Gait data were recorded using an eight-camera motion analysis system (Motion Analysis Corporation, MAC, Santa Rosa, CA, USA). Motion data were sampled at 120 Hz. A Helen Hayes marker set 31 was used to collect multiple trials of walking data at self-selected normal speed for each condition, first wearing the no-heel shoes, then the mid-heel shoes, and finally the high-heel shoes. Of particular relevance, the heel marker was placed at the same distance above the shoe insole to reflect a consistent anatomical placement. The forefoot marker was placed on the dorsum of the foot just proximal to the MTPJs. One gait cycle from each trial, with a mean of 6 ± 2 trials per condition, was used in the analysis.
These data were used to calculate the shank segment angle with respect to the vertical of the laboratory frame as a function of the gait cycle (the shank-to-vertical angle) and the actual foot segment angle with respect to the horizontal of the laboratory frame as a function of the gait cycle (the foot-to-horizontal angle) (Table 1 and Figure 1). Since the subjects had normal gait, to determine the gait cycle, we assumed that the minimum of the shank angle occurred at heel strike. We also assumed that gait was symmetric and used only data from the right leg in our analysis. The shank and foot segment angles were plotted for each subject for each footwear condition at initial contact (0% gait cycle), temporal midstance (30% gait cycle), and the end of terminal stance (50% gait cycle). To simplify the analysis, we selected these normalized event times for all subjects given that they only vary slightly across able-bodied subjects. Stride lengths were measured as the distance between the heel marker positions at subsequent heel strikes, and walking speed was estimated as the stride length distance divided by the stride time.
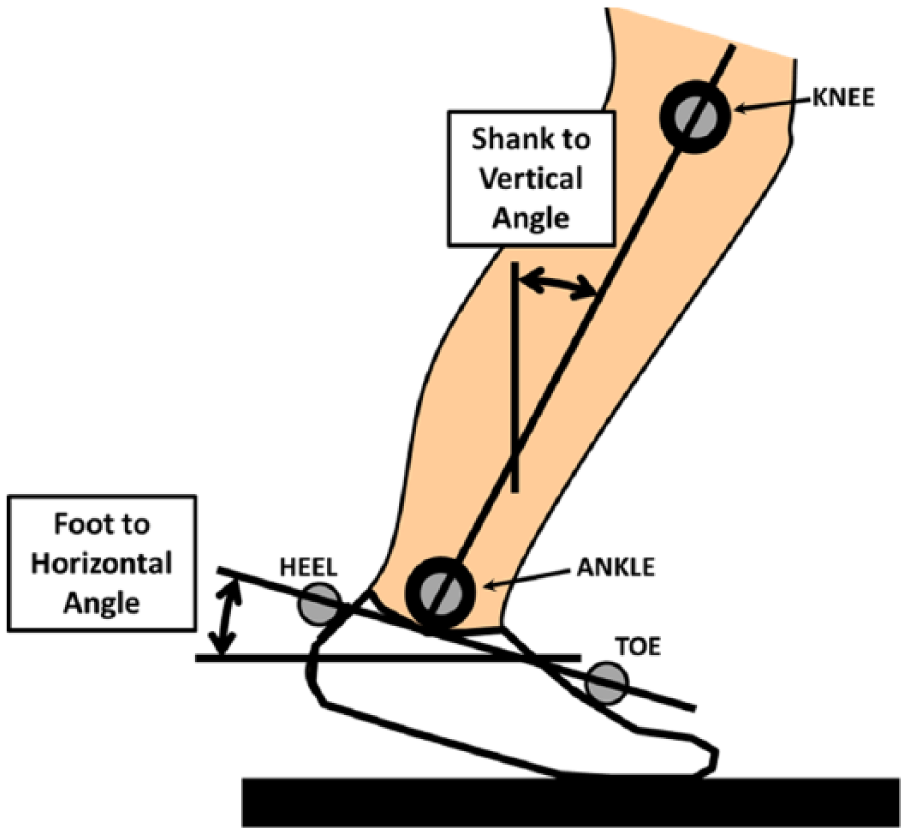
Definition of segment angles. Shank segment angle was calculated with respect to the vertical of the laboratory frame as a function of the gait cycle (the shank-to-vertical angle) and the foot segment angle was calculated with respect to the horizontal of the laboratory frame as a function of the gait cycle (the foot-to-horizontal angle).
An analysis of variance (ANOVA) with critical alpha set at 0.05 was conducted to ensure that stride lengths and walking speeds did not differ between footwear conditions. A one-way multivariate analysis of variance (MANOVA) was conducted to test each of our hypotheses. For each test, three dependent variables were used (shank angle at 0%, 30%, and 50% gait cycle and foot angle at 0%, 30%, and 50% gait cycle). The independent variable was HSD. Preliminary assumption testing was conducted to check for normality, linearity, univariate and multivariate outliers, and homogeneity of variance–covariance and multicollinearity with no serious violations noted except that shank angles were moderately correlated with each other and foot angles were highly correlated with each other. Since both correlated dependent variables and multiple comparisons inflate the possibility of type 1 error, critical alpha was set at 0.025 using a Bonferroni correction.
Results
Data from 10 nondisabled female subjects wearing three different HSD footwear were analyzed for this study (Table 2). The mean HSD of the no-heel shoes was 0 (standard deviation (SD) = 0) mm, mid-heel shoes was 37 (SD = 10) mm, and high-heel shoes was 71 (SD = 17) mm. These measurements show that the HSDs were different across footwear conditions and that variability in the HSD for mid- and high-heel shoes was small despite subjects bringing their own shoes.
Subject and footwear characteristics.
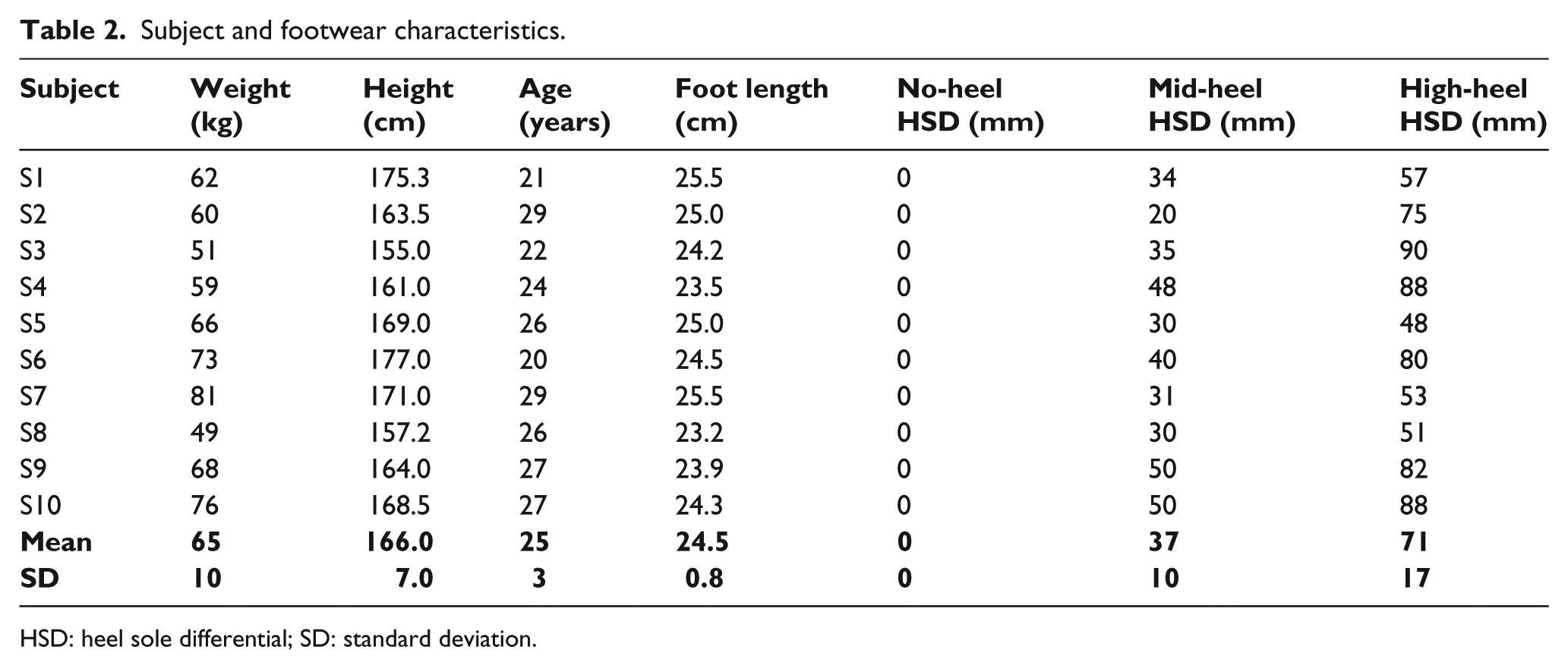
HSD: heel sole differential; SD: standard deviation.
There was no significant difference in stride lengths across the three conditions (no-heel = 1.44 (SD = 0.16) m; mid-heel = 1.47 (SD = 0.13) m; high-heel = 1.40 (SD = 0.13) m; p = 0.056). There was also no significant difference in self-selected speeds across the three conditions (no-heel = 1.40 (SD = 0.22) m/s; mid-heel = 1.41 (SD = 0.15) m/s; high-heel = 1.37 (SD = 0.18) m/s; p = 0.67).
There was no significant difference in shank kinematics with changes in HSD, F(6, 52) = 2.025, p = 0.079; Pillai’s Trace = 0.993; partial eta squared = 0.189. The mean shank kinematics graph (Figure 2(a)) shows that for all conditions, the shank segment angles were nearly identical during stance, except for 50% gait cycle, when shank inclination was slightly less for the high-heel shoe condition. Table 3 and Figure 2(c) provide the mean and 95% confidence interval (CI) for shank-to-vertical angles for the three HSDs at 0%, 30%, and 50% gait cycle.
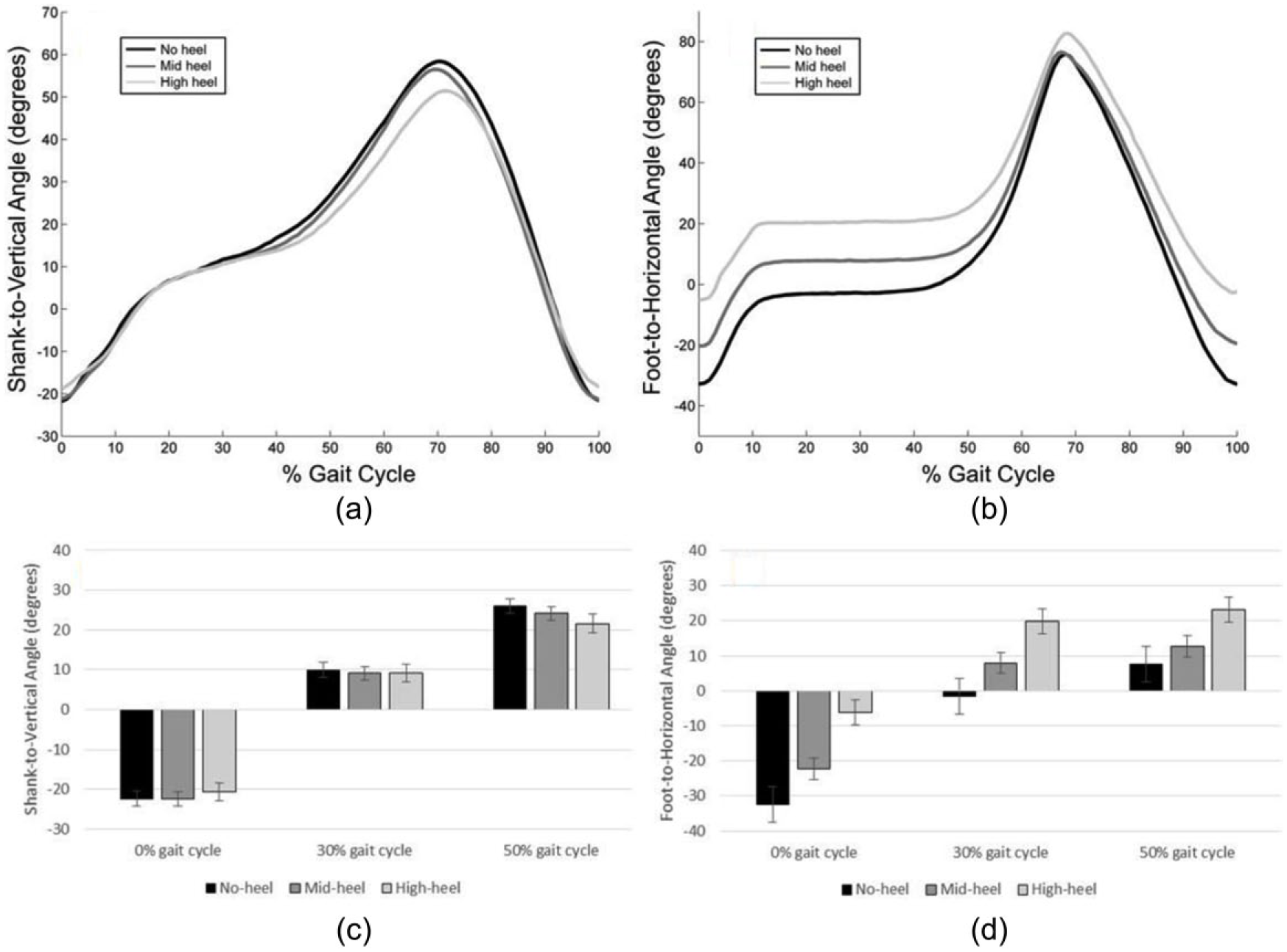
Mean (a) shank and (b) foot kinematics for three footwear conditions. Mean and 95% confidence interval for (c) shank-to-vertical angles and (d) actual foot-to-horizontal angles for three HSDs at 0%, 30%, and 50% gait cycle.
Mean and 95% confidence interval (CI) for shank-to-vertical and foot-to-horizontal angles for the three HSDs at 0%, 30%, and 50% gait cycle. Values for data shown in Figures 2(c) and (d).
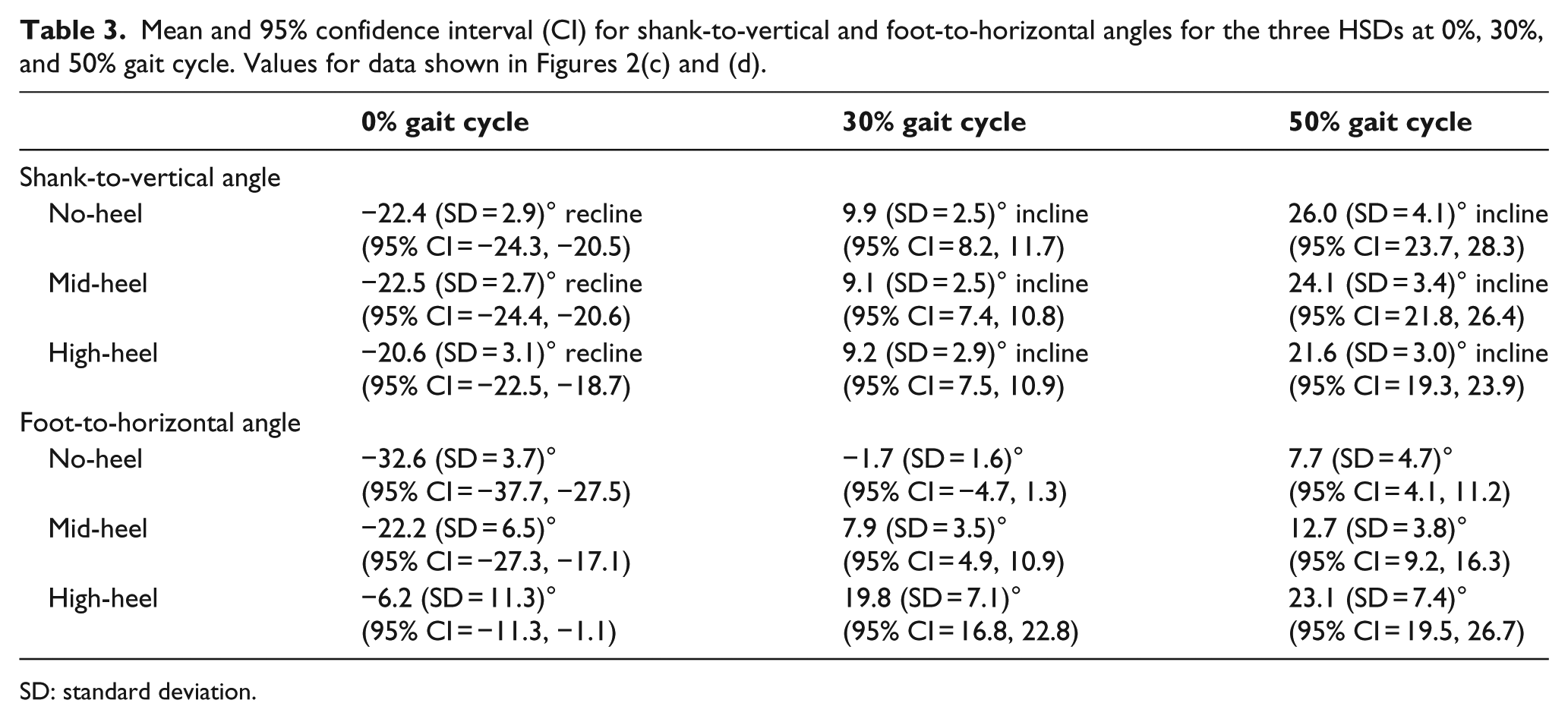
SD: standard deviation.
There was a significant difference in actual foot kinematics with changes in HSD, F(6, 52) = 8.182, p = 0.000; Pillai’s Trace = 0.971; partial eta squared = 0.486. Post hoc pair-wise comparisons (Table 4) show that there were significant differences between all HSDs at each time point, except for between no-heel and mid-heel at 50% gait cycle. Additionally, the mean foot segment kinematics graph (Figure 2(b)) shows that actual foot segment angle during stance phase increases with increasing HSD. Table 3 and Figure 2(d) provide the mean and 95% CI for actual foot-to-horizontal angles for the three HSDs at 0%, 30%, and 50% gait cycle.
Pair-wise comparisons for actual foot-to-horizontal angle.
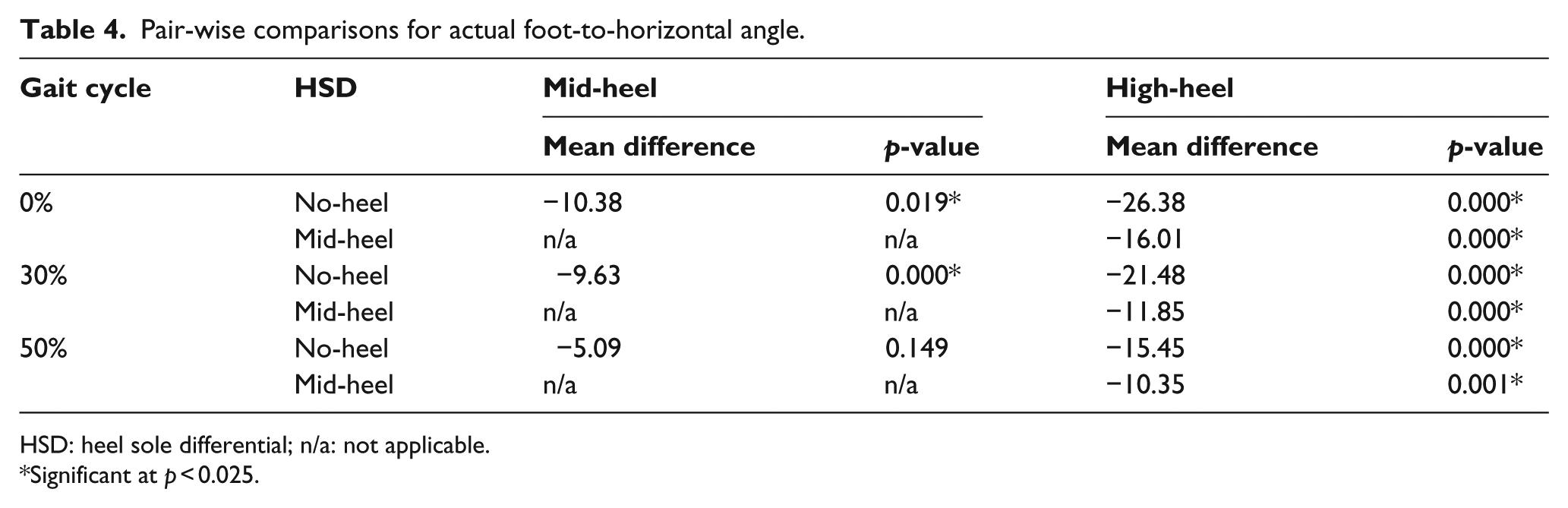
HSD: heel sole differential; n/a: not applicable.
Significant at p < 0.025.
Discussion
The purpose of this study was to assess the effect of footwear with different HSDs on the sagittal shank and foot segment kinematics of walking in able-bodied persons. Our results support the hypotheses that stance-phase shank kinematics do not change with changes in HSD of footwear, while stance-phase actual foot angle increases with increasing HSD of footwear.
Hansen and Childress 26 reported that nondisabled adult females adapt at the ankle when wearing footwear with HSDs of up to 50–60 mm to maintain similar roll-over shapes. They found that the ankle adopts more plantar flexion when wearing shoes with greater HSDs. This is illustrated in Figure 3. A similar observation was made by Murray 30 (Figure 4).
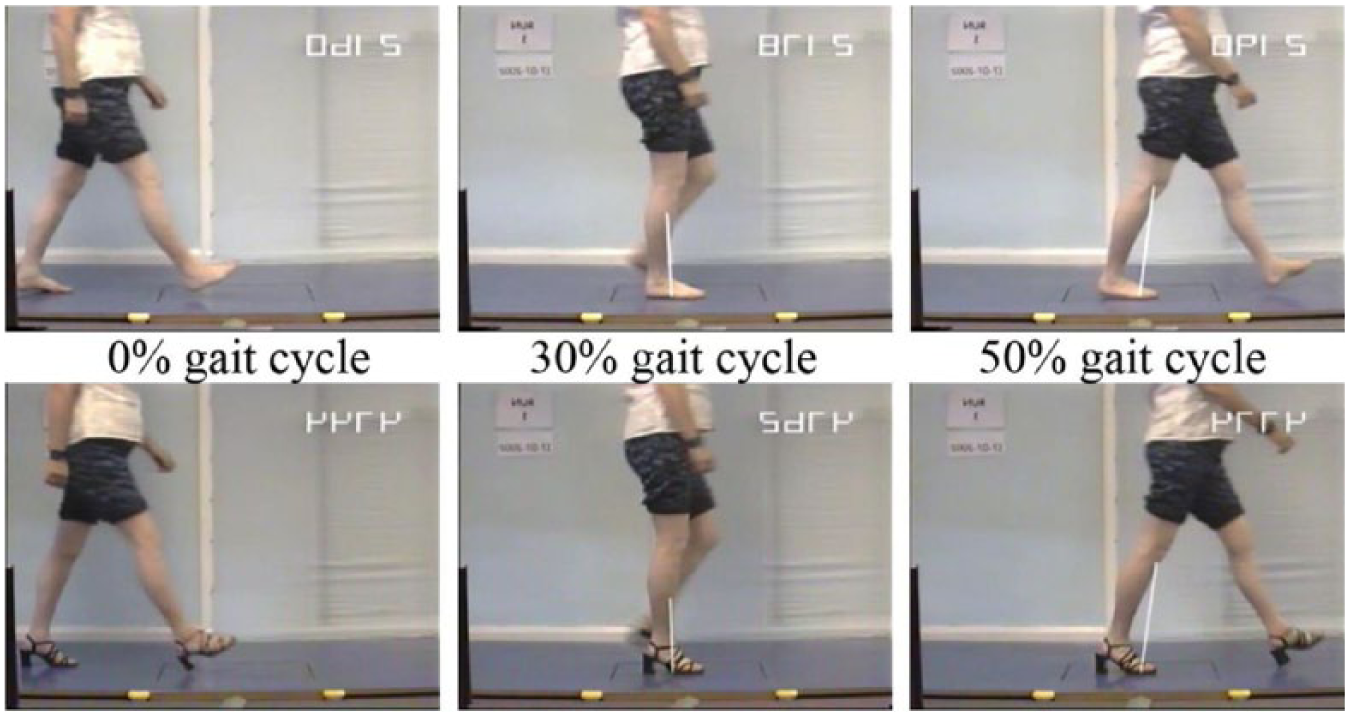
Video-vector screen images illustrating 0%, 30%, and 50% gait cycle when walking barefoot and in high-heel shoes. In the high-heel shoe condition, the shank-to-vertical angle remains the same as when barefoot but the ankle joint angle and the foot-to-horizontal angle change their alignment such that the “effective” foot created by the base of the footwear simulates normal barefoot foot kinematics. Images have been reversed across a vertical axis for clarity.
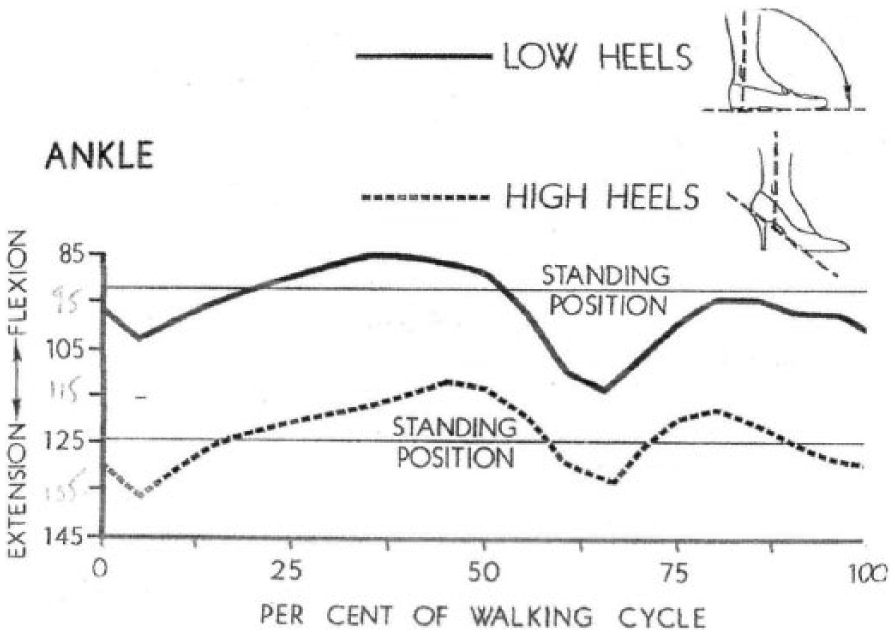
Previously published ankle kinematics for walking in low- and high-heel shoes. Ankle kinematics adjust to a more plantar flexed position.
The consistency of previously reported roll-over shapes for varying HSDs 26 suggests the need to maintain the segment kinematics of normal barefoot stance phase. Whatever the HSD of the footwear, shank kinematics will be similar to that of normal barefoot stance phase and the normal barefoot foot kinematics will be produced by an “effective” foot on the bottom of the shoe, with the actual foot shifting its kinematics by the degree of pitch of the footwear. The ankle adapts so that segment kinematics can remain consistent. One main purpose of walking is forward translation of a vertical trunk, and this is only possible if the segment kinematics of the thigh, shank, and foot behave as they do in normal barefoot gait.18–22 In particular, the specific alignments of the shank through stance phase are responsible for the ability of the thigh to move from a reclined to inclined alignment, which in turn allows for the forward translation of the vertical trunk.18–22 This is likely to be one reason for prioritizing the maintenance of segment kinematics.
Shank kinematics were consistent for all three footwear conditions for initial contact (0% gait cycle) and temporal midstance (30% gait cycle) and only slightly variable at the end of terminal stance (50% gait cycle). The consistency of shank inclination at temporal midstance (30% gait cycle) for all three conditions is notable. The importance of this degree of inclination coupled with the slowing of the angular velocity of the shank at temporal midstance has been described.18–22 The reason for the slight variability at the end of terminal stance (50% gait cycle) was not due to differences in stride length, but may have been due to differences in stiffness of the soles of the footwear at the MTPJs or perhaps the shorter foot length.
Foot kinematics varied with increases in HSD at initial contact (0% gait cycle), midstance (30% gait cycle), and the end of terminal stance (50% gait cycle). In barefoot gait, the foot makes initial contact with the heel in order to initiate a heel rocker.32,33 When wearing footwear with an HSD, the effective foot will act as “the foot” and the heel of the footwear will become “the heel” that makes initial contact. The effective foot alignment will be comparable to that of the foot when barefoot or in a no-heel shoe. The actual foot will adjust its alignment according to the pitch. At temporal midstance (30% gait cycle), in barefoot and no-heel shoes, the foot is horizontal to the floor and ankle rocker has occurred. 32 When walking in footwear with some pitch, the effective foot becomes “the foot” and remains horizontal, while the actual foot alignment is shifted to an angle equivalent to the pitch of the shoe. In this way, a horizontal and stable base of support is provided by the footwear, which is equivalent to that of the actual foot in barefoot gait. The importance of horizontal foot alignment in midstance has been described.18–22
The clinical relevance of these findings is that some patients will be able to walk with normal effective foot and shank kinematics when a short calf muscle or restricted ankle motion are present if footwear with an appropriate HSD is provided. The pitch can negate the need for the ankle joint to reach the amount of dorsiflexion required for normal barefoot gait, and if the HSD is great enough, can negate the need to even achieve plantigrade. Clinical groups that may benefit from this type of intervention include orthopedic conditions, stroke, cerebral palsy, toe walking, autism, and other disabling conditions of childhood and adulthood. Assessments with high HSD footwear are essential for patients with short calf muscle or restricted ankle motion. By trialing different HSD footwear, it is possible to determine if foot and shank kinematics can be corrected, and if any proximal kinematic and kinetic abnormalities are also corrected, indicating that the proximal abnormalities may be a secondary consequence of distal abnormalities.
The research relevance of these findings is that it is important to consider the effect of footwear on gait. For example, to compare “ankle-foot orthosis footwear combination” conditions to both “footwear” and barefoot conditions,34,35 to trial varying HSDs for the “footwear” condition, and to vary ankle angle alignments for the “ankle-foot orthosis footwear combination” condition where there is short calf muscle.18–20,22 Similar considerations apply to prosthetic research where footwear heel height can alter alignment and therefore mechanical function of the prosthetic components. 36
There are limitations to this study. Only young adult female subjects were tested and the cohort was small in size. The effective foot-to-horizontal angle was surmised from other data and not directly measured at the time of data collection. There was no accurate measure of the stiffness of the shoes at the MTPJs or the sole profile, both of which can affect foot and shank kinematics, especially in terminal stance.19,22 Thigh and trunk kinematic data were not collected.
Future studies are needed to ascertain full body segment and joint kinematics in all age groups for typically developing children, male and female adults, and the effect of varying HSDs and ankle angle alignments in orthoses on a wide range of patient populations. It would be clinically relevant to know at what age children obtain normal shank and foot kinematics when wearing various HSDs and whether this ability is retained in older adults.
Conclusion
Stance-phase shank kinematics of able-bodied females did not change with changes in HSD of footwear. However, stance-phase actual foot kinematics changed systematically with changes in HSD, with actual foot angle increasing with the increase in HSD.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Disability and Rehabilitation Research (grant/award number: H133E980023).