
Abstract
Background:
To date no review has been published that analyzes the efficacy of assistive devices on the walking ability of ambulant children and adolescents with spina bifida and, differentiates between the effects of treatment on gait parameters, walking capacity, and walking performance.
Objectives:
To review the literature for evidence of the efficacy of orthotic management, footwear, and walking aids on gait and walking outcomes in ambulant children and adolescents with spina bifida.
Study design:
Systematic literature review.
Methods:
A systematic literature search was performed to identify studies that evaluated the effect of any type of lower limb orthoses, orthopedic footwear, or walking aids in ambulant children (≤18 years old) with spina bifida. Outcome measures and treatment results for gait parameters, walking capacity, and walking performance were identified using International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) as the reference framework.
Results:
Six case-crossover studies met the criteria and were included in this systematic review. Four studies provided indications of the efficacy of the ankle–foot orthosis in improving a number of kinematic and kinetic properties of gait, stride characteristics, and the oxygen cost of walking. Two studies indicated that walking with forearm crutches may have a favorable effect on gait. The evidence level of these studies was low, and none of the studies assessed the efficacy of the intervention on walking capacity and walking performance.
Conclusions:
Some data support the efficacy of using ankle–foot orthosis and crutches for gait and walking outcomes at the body functions and structures level of the ICF-CY. Potential benefits at the activities and participation level have not been investigated.
Clinical relevance
This is the first evidence-based systematic review of the efficacy of assistive devices for gait and walking outcomes for children with spina bifida. The ICF-CY is used as a reference framework to differentiate the effects of treatment on gait parameters, walking capacity, and walking performance.
Background
Children with spina bifida (SB) often present with impairments in the muscle and sensory functions of the lower limbs and with gait pattern deviations that are related to the level of spinal involvement. These impairments result in restrictions in activities of daily living, particularly walking. The ability to walk and the prognosis for independent ambulation depend mainly on the level of spinal involvement: the lower the level, the higher the expected maximal level of ambulation and the greater the chance to maintain this ambulation level during the adolescent years.1–4 Studies also suggest that other factors, such as bony deformities, muscle contractures, aerobic fitness, an active lifestyle and daily physical activity, can influence ambulatory status.4–9 The gait pattern deviations seen in children with SB result in a higher level of energy cost of walking that may lead to lower levels of daily physical activity and in early fatigue during daily physical activity.10–13
The use of lower limb orthoses, specialized footwear, and walking aids by children with SB aims to prevent foot deformity, protect the sensorily impaired feet, and distribute pressure and improve gait pattern and the energy cost of walking. The ultimate goal is to improve the ease of performing daily activities related to ambulation, both from the perspective of the child and the parent, such as standing, transfers, and walking. According to the framework of the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY), 14 outcome measures are classified at the level of either “body functions and structures” or “activities and participation.” From the patient’s perspective, improvement in walking capacity and in actual walking performance is the ultimate goal of treatment. Evidence of the efficacy of the assistive device at the level of “activities and participation” requires the use of outcome measures of walking capacity and performance 15 but evidence at the “body functions and structures” level must also be taken into account when assessing the biomechanical efficacy of the orthosis. 16 There are many types of assistive devices, including reciprocal gait orthoses, knee–ankle–foot orthoses, ankle–foot orthoses (AFOs), shoe adaptations, orthopedic footwear, and walking aids such as forearm crutches. The choice of assistive device is an important one that is made by the clinician. To evaluate the biomechanical efficacy of an orthosis and footwear, the type, the design, and biomechanical alignment of the device must be specified.
There is one previous literature review from 2004 that analyzed the efficacy of bracing the lower limbs in children with SB. 17 That review concluded that orthotic treatment is efficacious in children with low lumbar SB; however, the ICF-CY level was not specified, and no advice was given concerning orthoses and footwear prescriptions. Therefore, the purpose of this comprehensive study was to update the review of the literature using ICF-CY as a reference framework.
Our specific aims were as follows: (1) to systematically assess the evidence in the literature that supports the efficacy of lower limb orthoses, footwear, and walking aids on gait and walking outcomes for ambulant children and adolescents with SB; (2) to identify the treatment results at different ICF-CY levels; and (3) to discuss the implications for clinical practice.
Methods
The review was conducted as follows: (1) a systematic literature search was conducted using specific search terms; (2) articles were selected based on predetermined inclusion and exclusion criteria; (3) the reported outcome measures and treatment results were identified using ICF-CY as a reference framework; (4) the level of evidence was graded based on predefined quality criteria.
Two authors (BI and MS) independently assessed the abstracts identified in step 1 and selected relevant articles. An epidemiologist (NV) evaluated the selected articles and discussed the levels of their evidence with the other two authors to resolve any disagreements until consensus was reached.
Step 1: systematic literature search
The Cochrane Library (Wiley), Embase (Elsevier), and Medline (OVID) databases (1948–March 2013) were searched using the search terms “spina bifida,” “myelomeningocele,” “meningocele,” “lipomyelomeningocele,” “neural tube defects,” and “spinal dysraphism” in combination with terms that concern gait and walking ability such as “locomotor performance” “locomotion walking,” “gait,” “ambulation,” and “gait disorders” and limited with intervention-specific terms, such as “walking aid,” “ambulation training,” “gait training,” “orthosis,” “orthopedic footwear,” “brace,” and “orthotic device.”
Step 2: article selection
Abstracts and, when needed, full texts were searched for the following inclusion criteria: (1) the study population included children with SB up to 18 years of age; (2) the study evaluated the effects of any type of lower limb orthoses, orthopedic footwear, and/or walking aids; (3) outcome measures that included gait parameters and/or walking capacity and/or walking performance; (4) the study was published in English, Dutch, German, or French. Studies with a limited number of participants (N < 10) or those which included fully wheelchair-dependent children were excluded.
Step 3: identification of outcome measures and treatment results
Articles selected in step 2 were assessed for outcome measures for gait, walking capacity, and walking performance and were assigned to one of the ICF-CY levels based on the ICF-CY definitions. 14 Data related to the type and design of the orthosis, footwear, and walking aid, as well as treatment results, were extracted from each article.
Step 4: grading the level of evidence
The level of evidence of each study was determined using the criteria shown in Table 1. These criteria are based on the GRADE (Grading of Recommendations Assessment, Development and Evaluation) assessment of intervention studies published previously.18,19
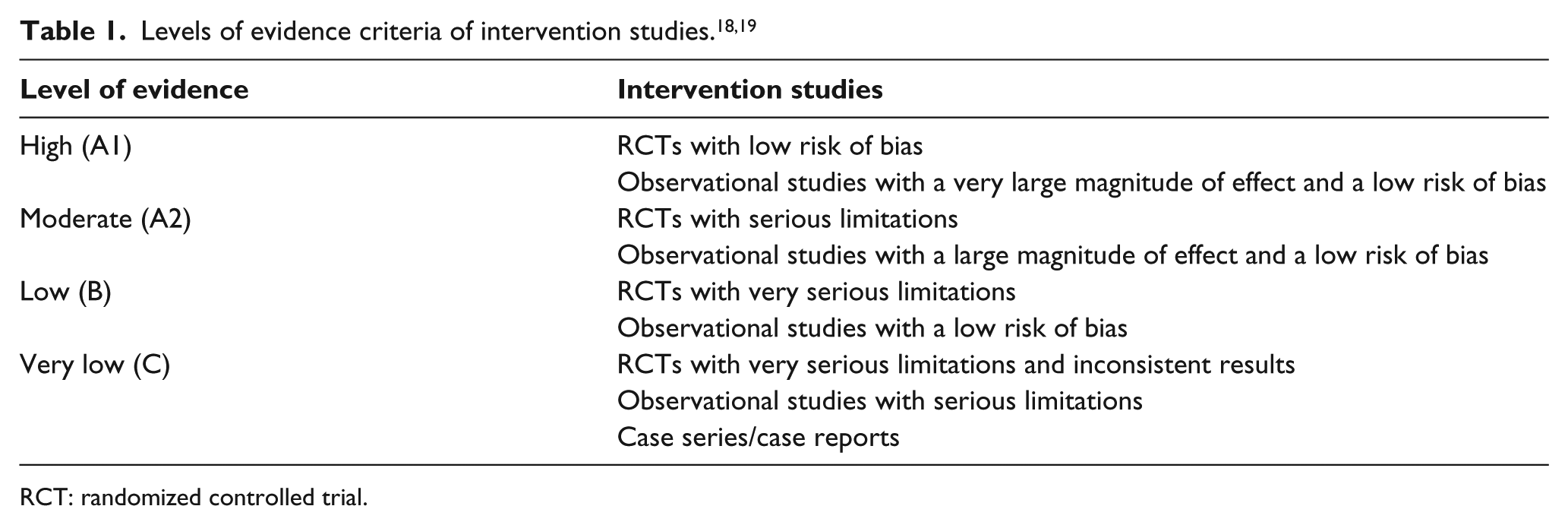
RCT: randomized controlled trial.
Results
Literature search and article selection
Of the 353 articles identified, six met our inclusion criteria. The included studies are summarized in Tables 2 and 3. Four articles reported data about the effects of AFOs, while two presented data about the effects of crutches.
Level of evidence and outcome measures of the studies included in this review.
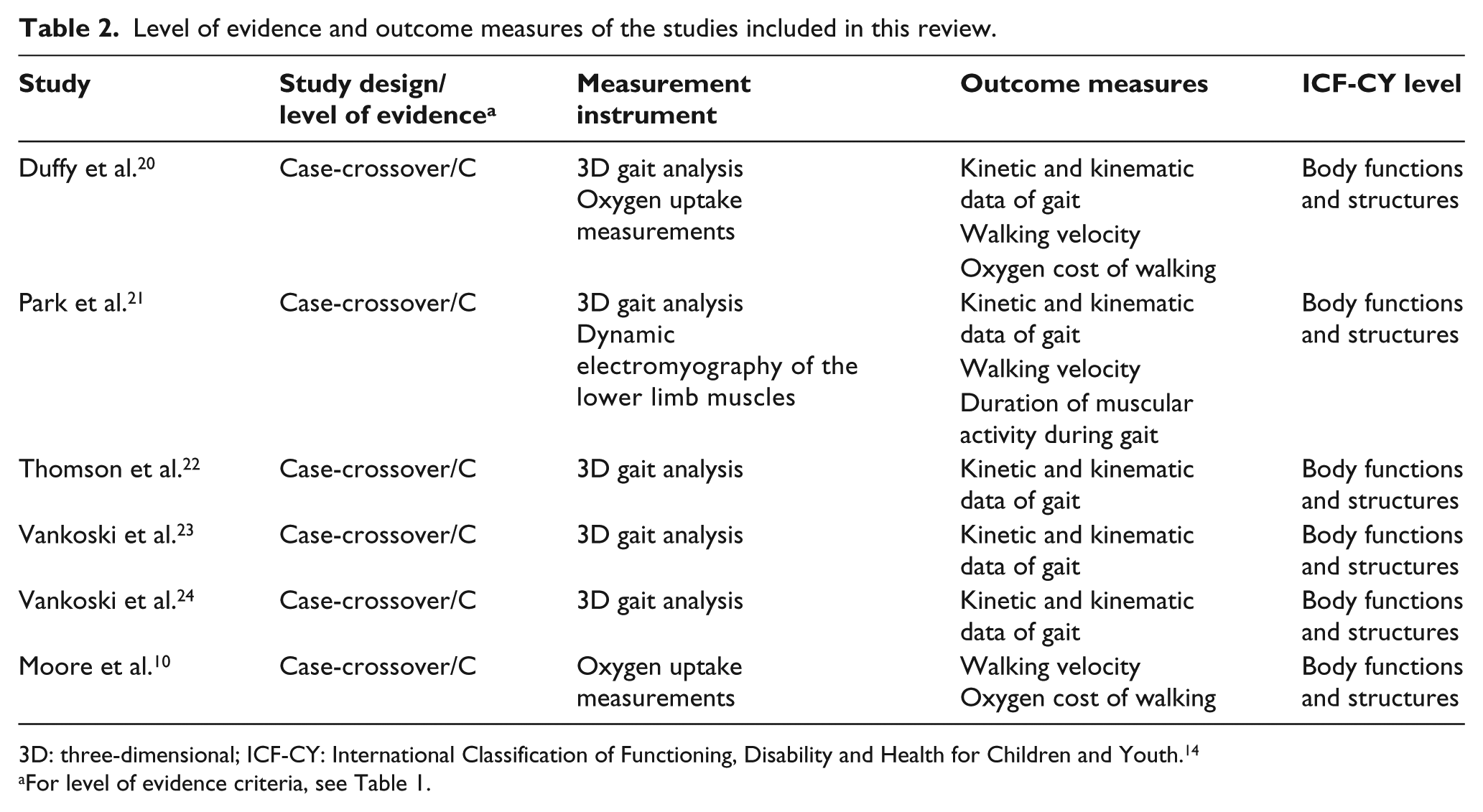
3D: three-dimensional; ICF-CY: International Classification of Functioning, Disability and Health for Children and Youth. 14
For level of evidence criteria, see Table 1.
Study population and treatment effects reported by the studies in this review.
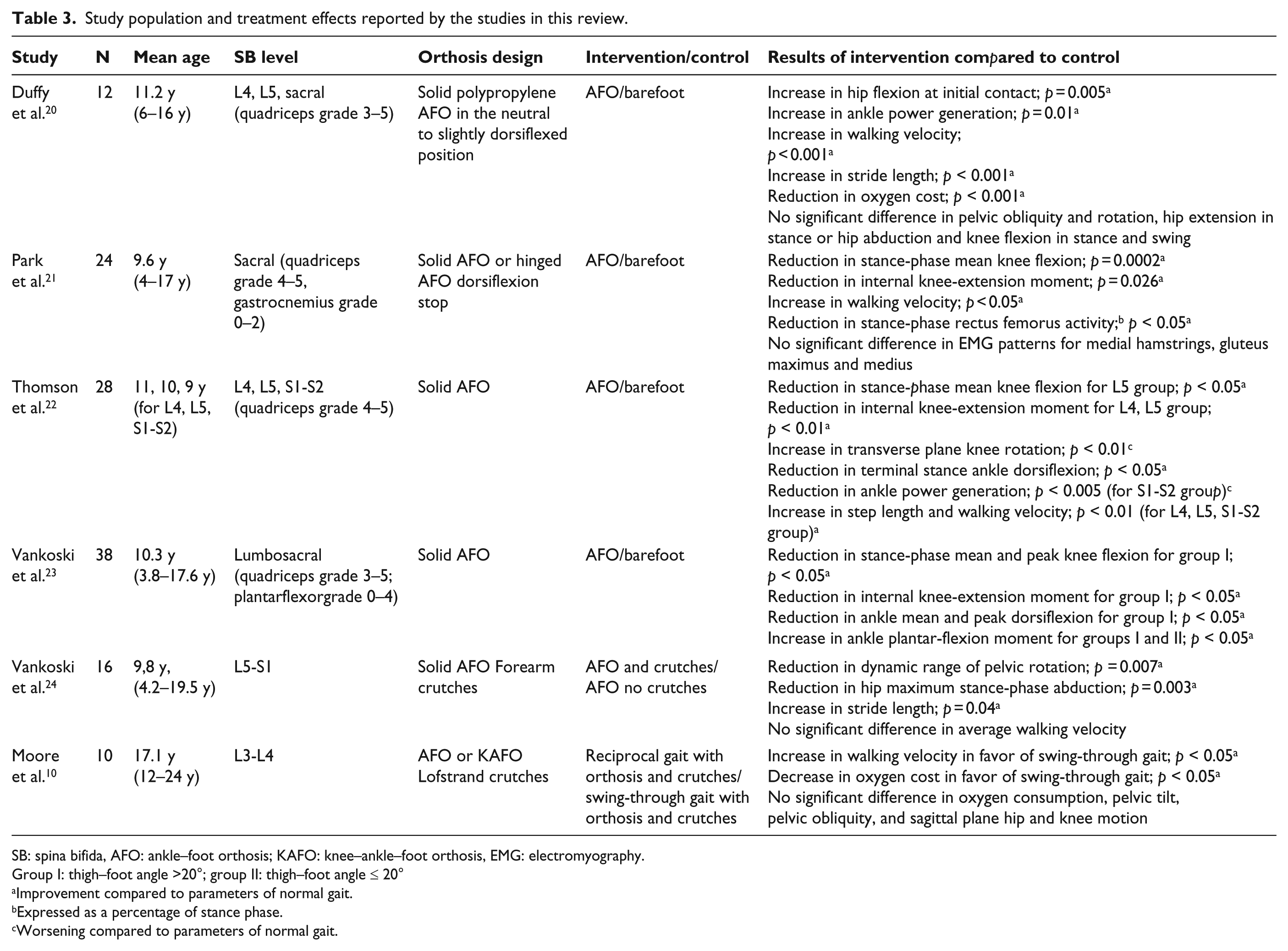
SB: spina bifida, AFO: ankle–foot orthosis; KAFO: knee–ankle–foot orthosis, EMG: electromyography.
Group I: thigh–foot angle >20°; group II: thigh–foot angle ≤ 20°
Improvement compared to parameters of normal gait.
Expressed as a percentage of stance phase.
Worsening compared to parameters of normal gait.
Outcome measures and ICF-CY classification
The outcome measures were mainly related to the ICF-CY level “body functions and structure” (Table 2). These measures consisted of gait pattern kinematic and kinetic data, stride characteristics, and oxygen cost of walking data that were assessed using three-dimensional (3D) gait analysis and breath-by-breath gas-analysis systems. Neither time-scored walking capacity tests nor other outcome measures of the “activity or participation” level of the ICF-CY were included in any of the studies.
Level of evidence
No systematic reviews or randomized clinical trials were identified. All of the included studies were studies with a case-crossover study design. The level of evidence of each of these studies was level C, that is, a very low level of evidence (see Table 2).
Effects of treatment
Ankle–foot orthosis
Four studies compared the effects of AFO to walking barefoot. All of the studies involved children with L4, L5, and/or sacral level SB. The studies gave limited information about the properties of the AFO. The type of orthosis was mostly described as being a solid AFO but no details about the design or alignment of the AFO/footwear combination were provided. Keeping in mind the low level of evidence, these four studies indicated that for children with lumbosacral level SB, walking with AFOs has a positive effect on a number of kinematic and kinetic properties of gait, stride length, walking velocity, and oxygen cost of walking.20–23 The most consistent finding concerning the kinematic and kinetic data was that walking with an AFO reduced stance-phase knee flexion and the internal knee-extension moment. One of the studies indicated that the improvement in the kinetic and kinematic data was less favorable in the presence of an external tibial torsion of more than 20°. 23 In terms of the stride characteristics and the oxygen cost of walking, the most consistent finding was an increase in walking velocity with the use of an AFO (Table 4).20–22
Effect of AFO use on walking velocity and on the oxygen cost of walking.
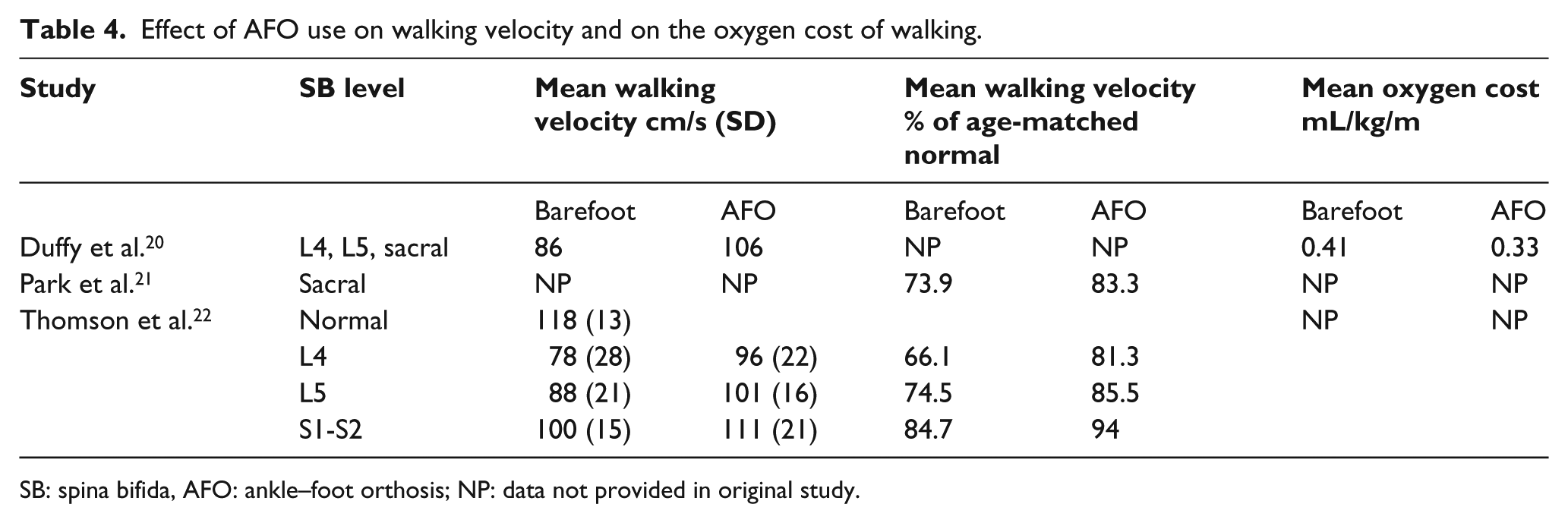
SB: spina bifida, AFO: ankle–foot orthosis; NP: data not provided in original study.
Forearm crutches
One study indicated that in children with L5-S1 level SB, walking with forearm crutches may have a favorable effect on pelvic and hip kinematics compared with walking without the crutches. 24 Another study indicated that in children with L3-L4 level SB, walking with crutches in a swing-through gait pattern may have a positive effect on walking velocity and on the oxygen cost of walking compared to walking in a reciprocal gait pattern. 10
Adverse effects
Although one of the studies showed a significant increase in transverse plane knee rotation while walking with an AFO, 22 possible adverse effects that could be related to the long-term use of orthoses or walking aids, such as knee or shoulder pain, were not studied systematically.
Discussion
Our review identified six studies of children and adolescents with SB. They reported that AFOs and crutches had positive effects on a number of kinematic and kinetic properties of gait, on stride characteristics, and on the oxygen cost of walking. These studies only included patients with lower neurological level SB. They had been performed before the development of validated time-scored walking capacity tests, such as the Six-Minute Walk Test, 25 and the outcome measures only covered the ICF-CY level “body functions and structure.” None of the studies included outcome measures at the “activities and participation” level; therefore, we cannot draw conclusions about the benefits of these assistive devices on walking capacity and performance. Although many children with SB wear orthopedic shoes, the effects of footwear were not addressed by any of these studies.
The reported shift of the kinematics and kinetics data toward normality is thought to indicate the biomechanical efficacy of the orthotic intervention, but this depends on the design of the orthosis. 16 The lack of information on the type, design, and biomechanical alignment of the AFO therefore makes it difficult to apply this information in clinical practice.
The studies in this review measured walking speed during the 3D gait analysis. From a clinical perspective, only increases in gait speed that result in improved walking performance are considered meaningful. 26 Therefore, the reported increase in walking speed when walking with an AFO needs to be confirmed in future studies that use validated time-scored walking capacity tests, such as the Six-Minute Walk Test.25,27
The oxygen cost of walking is widely used as a measure of gait efficiency. 28 The reported reduction of the oxygen cost of walking as the result of wearing an AFO or using crutches indicates a more efficient gait and could result in decreased fatigue and increased levels of daily physical activity. Future longitudinal studies that include outcome measures at the “activity and participation” level are needed to confirm this hypothesis.
The six studies that met our inclusion criteria only involved children with L4, L5, and/or sacral level SB. Studies in children with high-level SB that compared intensive walking programs at an early age, including the use of surgical procedures, orthoses, crutches, walkers, physical therapy, gait-training, and management directed at the early use of a wheelchair, were inconclusive regarding the impact on functional independence at a later age.29,30 Potential benefits of lower limb orthoses, footwear, and walking aids in terms of enhancing the walking ability of children with high-level SB require further research. These results are in accordance with the earlier review by Mazur. 17
Implications for clinical practice
Currently, indications of the biomechanical efficacy of the use of AFOs and forearm crutches by children with lumbosacral level SB are the only evidence that can help clinicians in daily clinical practice. For a given child, the mechanical efficacy of the AFO depends on the correct design of the orthosis. The orthosis should help correct the unfavorable alignment of the ground reaction force that results from impairments in muscle function. The footwear that is worn with the AFO will add to the overall biomechanical control. Fine-tuning of the footwear, along with the AFO, is another prerequisite of proper alignment of the ground reaction force and must be considered carefully. 31 Although the use of crutches by children with lumbar and high sacral level SB has been advocated, more research is needed to determine the indications and long-term gains and adverse effects of the use of crutches in this population. 24
Study limitations
This systematic review has a number of limitations. Few of the included studies described the AFO properties in sufficient detail to allow us to analyze the AFO properties across the studies. Therefore, it was not possible to conduct a statistical analysis of the outcome data. Publication bias was not assessed. The level of evidence of the available studies was low, so the results should be considered with caution. Additional research is needed to bolster our confidence in the estimate of treatment effects and is also likely to change the estimate.
Conclusion
There are some indications that the use of an AFO can improve the gait pattern, stride characteristics, and the oxygen cost of walking in children with lumbosacral level SB. Potential benefits on walking capacity and performance have not been investigated. Further research should include outcome measures of walking capacity and performance and a test-specific hypothesis regarding the design of the orthosis/footwear combination.
Footnotes
Author contribution
B Ivanyi drafted the article and contributed to the design of the study, to acquisition of data and to the analysis and interpretation of the results. MAGC Schoenmakers and NHJ van Veen critically revised the article and contributed to the design of the study, to acquisition of data, and to the analysis and interpretation of the results. CGB Maathuis, F Nollet, and M Nederhand critically revised the article and contributed to the analysis and interpretation of data.
Declaration of conflicting interests
None declared.
Funding
This project was supported by the “Stichting Kwaliteitsgelden Medisch Specialisten.”