
Abstract
Background:
Loss of the hand results in significant functional deficits and requires adaptation of movement patterns which may result in overuse injuries. An externally powered prosthesis may improve function of the affected limb and reduce the overreliance on the intact side; however, little research has been done in this area.
Objective:
Investigate changes in upper limb function and kinematics in individuals with partial-hand amputations performing a functional assessment by comparing results with and without a multi-articulating hand prosthesis.
Study design:
Cross-sectional.
Methods:
Three-dimensional kinematics of four- and five-digit limb loss participants were collected as they performed the Southampton Hand Assessment Procedure with and without a prothesis.
Results:
Ten males completed the protocol: five with four-digit loss (thumb intact) and five with five-digit loss. Significantly larger joint motions were seen without the prosthesis than with for all participants, which may be an indicator of higher risk for overuse injury. Significant improvement was seen in Southampton Hand Assessment Procedure scores in the five-digit limb loss participants using the prosthesis compared with not using the device (p < 0.05 for 6/7 Southampton Hand Assessment Procedure score categories).
Conclusion:
The prosthesis reduced functional deficits and decreased joint range of motion in individuals with partial hand loss. Results showed reduced compensatory motions throughout the upper limb and torso which may reduce the risk of overuse injury.
Clinical relevance
Results of this study indicate that externally powered partial hand prostheses can be effective in improving function and reducing compensation in individuals with partial hand loss.
Keywords
Background
There are an estimated 2 million people in the United States currently living with limb loss, with 35% involving upper limb loss. 1 Of those upper limb amputations, 90% occur at or distal to the wrist. 2 The American Medical Association guidelines estimate the loss of the hand results in 54% whole body impairment.3,4 In comparison, loss of the full leg at the hip disarticulation level results in 40% whole body impairment. Unilateral thumb loss at the metacarpophalangeal joint results in 22% whole body impairment, 3 a significant portion of full body function for a relatively small body part.
Absence of an upper limb requires the individual to learn new methods to complete activities of daily living (ADLs). For individuals with unilateral involvement, these adaptations may cause over reliance on the intact side, creating the potential for overuse injuries and musculoskeletal disorders (MSDs). While research into overuse injuries in individuals with upper limb amputations is limited, particularly in partial-hand amputations, it has been estimated that up to half of these individuals may experience overuse injuries.5,6 Increased use of the intact limb as well as compensatory motions of the affected extremity may lead to abnormal and awkward joint motions which can result in increased incidences of shoulder impingement, nerve entrapment, muscle and tendon strain, epicondylitis, and carpel tunnel syndrome.7–9
Use of an externally powered upper limb prosthesis may restore some level of function to the user and reduce the possibility of overuse and secondary injuries. Externally powered hand prostheses with individually articulating digits have transitioned from research to commercial availability over the past decade. Few research studies have been conducted to evaluate their functional capabilities with users. Due to the uniqueness and variability among partial-hand amputations, and the advanced technical aspects required, prosthetic technology has only recently begun to address the functional needs of persons with partial-hand amputation. 10 Externally powered hand prostheses are difficult to obtain due to cost, insurance company policies, and lack of peer-reviewed research on the function and capabilities of the devices.11–13 There is a need to evaluate these devices to provide an objective assessment of their ability to improve function of the user.
One tool to evaluate hand function is the Southampton Hand Assessment Procedure (SHAP), a standardized, objective assessment that has been used in studies of prosthesis performance. 14 The assessment includes a battery of 26 tasks broken into six grip subcategories: spherical, tripod, power, lateral, tip, and extension (Figure 1). The goal of the SHAP is to complete each task as fast and as accurately as possible. The times to complete tasks are combined to assess the six prehensile patterns, normalized to a score of 100, and an additional overall function score is determined. 14 Scores above 95 indicate normal function.14,15

The Southampton Hand Assessment Procedure.
The SHAP measures time and does not consider the compensatory motions needed to complete these tasks, though clinicians working with end-users of prostheses note a decrease in compensatory motions as a benefit of prosthesis use. 16 The main objective of this investigation was to compare the different compensatory motions at the wrist, elbow, shoulder, scapula, and trunk used by individuals with two types of partial hand loss as they completed the SHAP with and without a multi-articulating externally powered hand prosthesis. We hypothesized that the participants would have higher SHAP scores during the prosthesis condition than the non-prosthesis condition, indicating better function. We also hypothesized that the participants would demonstrate different kinematic outcomes, specifically trunk, scapula, shoulder, elbow, and wrist range of motion (ROM), between conditions, with the prosthesis condition resulting in reduced, joint ROMs.
Methods
Participants with partial hand loss were recruited from the Touch Bionics by Össur training facility in Ohio. Participants came from prosthetic facilities across the United States and were recruited with the permission of their treating prosthetist. Potential participants had to: have a unilateral partial-hand amputation (four-digit loss with intact thumb, or five-digit loss) due to trauma; be over 18 years old; have minimum of 10 h of occupational therapy focused on learning how to use their prosthesis; have good residual limb skin integrity; have good strength and ROM of the residual limb: minimum 40° wrist flexion/extension, 60° forearm supination/pronation, and lateral thumb pinch strength of 10 pounds, if applicable.
All participants had the i-digits prosthesis from Touch Bionics by Össur. The i-digits is an externally powered partial hand prosthesis with individual articulating digits. The system may include a manually rotatable thumb as necessary. The prosthesis has compliant grip, where each digit can conform to the shape of an object for stable grasp. For gripping delicate objects, proportional control is available and variable grip allows for an increase in grip force, both at the user’s discretion. Pre-programmed grips are available to the user based on their goals. A flexible wrist connection connects the battery pack to the prosthesis which helps maintain wrist ROM.
Two-handed participants were recruited to develop a set of outcomes for visual reference. These participants were recruited from the local community and met the following criteria: over 18 years old, and no previous upper limb surgery or severe injury such as a torn muscle, ligament or tendon, or a displaced fracture. This study was approved by The Ohio State University Institutional Review Board (IRB) and all participants provided informed consent prior to their participation.
Three-dimensional (3D) kinematics were estimated using passive marker data collected at 150 Hz using 10 Vicon MX-F40 cameras (Vicon Motion Systems, Oxford, UK) and filtered using a fourth-order Butterworth filter at 6 Hz. Custom BodyBuilder (Vicon Motion Systems), Visual 3D (C-Motion, Inc., Maryland, USA), and MATLAB (Mathworks, Inc., Natick, MA) scripts were used to calculate upper limb kinematics.
An upper limb marker set was utilized according to International Society of Biomechanics (ISB) recommendations 17 and included a scapula-specific marker set. 18 Markers were also placed on the metacarpophalangeal joint, proximal and distal interphalangeal joints, and the fingernail (Figure 2). Using the symmetrical center of rotation method, the functional shoulder joint center was determined using a star-arc pattern trial of the arm.18,19 The midpoint between the medial and lateral humeral epicondyle markers was used to estimate the elbow joint center. The midpoint between the ulnar and radial styloid process markers was used to estimate the wrist joint center. Joint and angle definitions followed ISB convention.
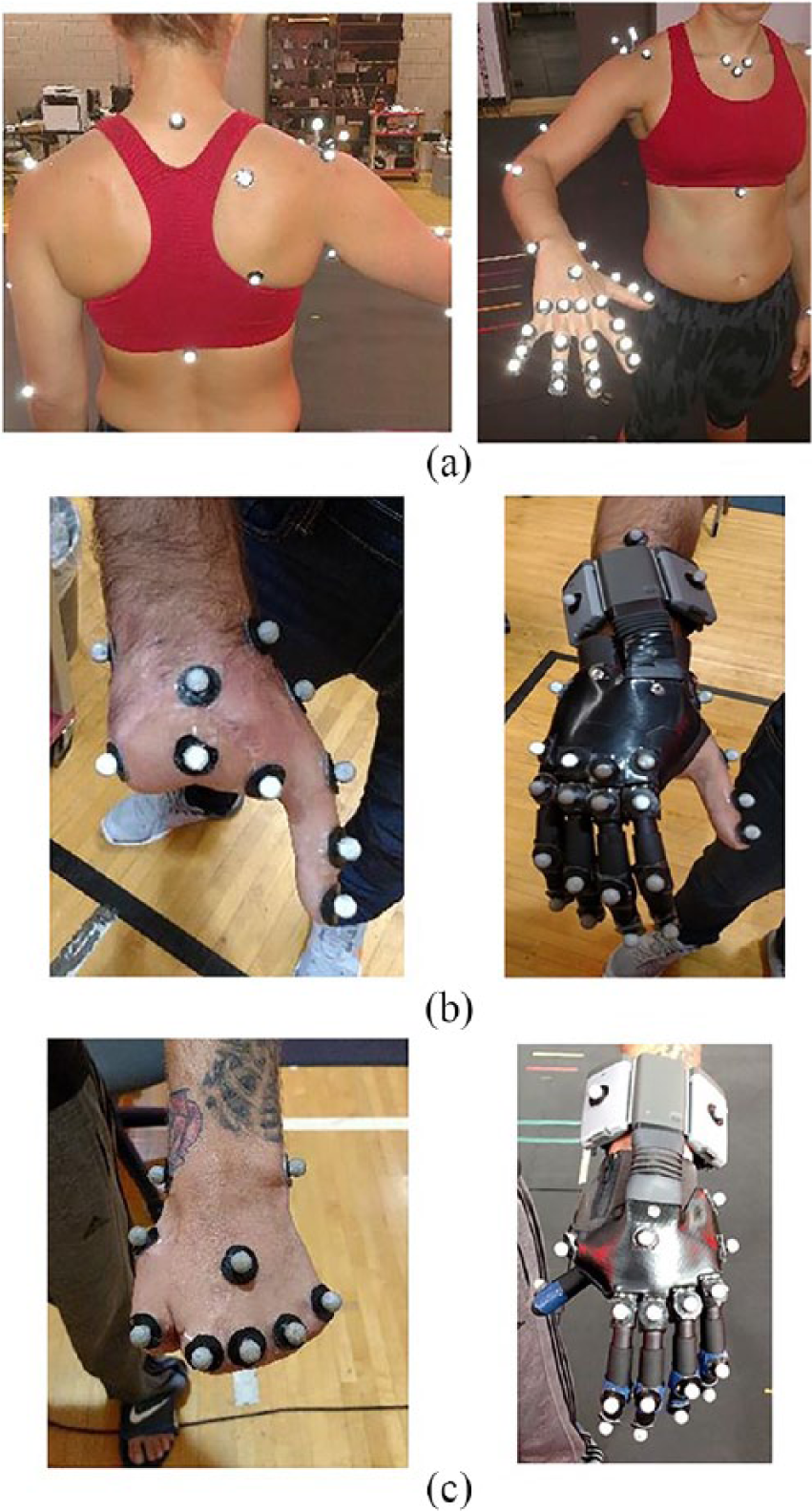
Example of the marker set used for 3D motion capture and kinematic calculations of upper limb movement. Only one side was assessed at a time during data collection while the contralateral side had a more basic marker set: (a) a healthy two-handed participant, (b) a four-digit limb loss, and (c) a five-digit limb loss participant.
The testing protocol involved participants performing the SHAP twice: once with their prosthesis and once without. Participants from the two-handed cohort also performed the testing protocol twice: once with their dominant hand as focus and once with their non-dominant hand. Because an amputation can affect either a dominant or non-dominant hand, we had the two-handed cohort perform the protocol using both sides for completeness.
The SHAP battery of tasks was administered according to protocol. 14 The participants were seated on a backless bench to avoid blocking markers from the motion capture cameras. When using the prosthesis, participants were allowed to select the grip they wanted to use prior to starting the task. Each task within the SHAP was performed twice within each hand condition. The best time of the two trials was used to calculate the SHAP score. For the kinematic analysis, both trials were used to create an average result. Kinematic analysis was limited to only when the participant was in contact with the object. The jar lid opening task was analyzed during the act of opening the jar, when the residual hand or prosthesis was in the act of twisting the lid off. Kinematic analysis was not completed on all 26 SHAP tasks due to insufficient marker data, as certain tasks resulted in the participant blocking the motion tracking markers from the camera. A total of 15 of the 26 SHAP tasks are presented here, including movement of various size, shape, and weight objects with the six grip patterns (sphere, tripod, power, lateral, tip, and extension heavy and light conditions each).
A composite score for joint ROM was calculated for each task using vector analysis. The square root of the sum of squares of each degree of freedom for each joint was found and the results were summed for all joints within each task. This primary analysis was done to determine the overall change in ROM between prosthesis and non-prosthesis tasks for the entire upper body. A secondary analysis within each task evaluated individual joint ROMs to pinpoint where the largest source of compensation occurred. Due to the importance of the thumb for movement,3,4 the four- and five-digit limb loss groups were analyzed separately.
Statistical comparison between conditions within each limb loss group was completed on the composite scores using two-tailed paired t-tests with a significance level of 0.05 (JMP Pro, Version 12.2.0, SAS Institute Inc., Cary, NC). Two-tailed paired t-tests also determined differences in individual joint ROM within each task, and Bonferroni correction was applied to reduce the risk of Type I error. Graphical analysis was used to compare limb loss results to two-handed results. No statistical analyses were done on the two-handed cohort, or between the two-handed and limb-loss cohorts. The two-handed data are presented alongside the limb loss data purely as a visual comparison to aid the reader in quantifying the joint ROMs seen in the limb-loss cohort.
Results
A total of 10 male partial hand limb loss participants and 24 two-handed controls (12 male) completed the testing protocol (Table 1).
Demographics of the limb loss and two-handed cohorts.
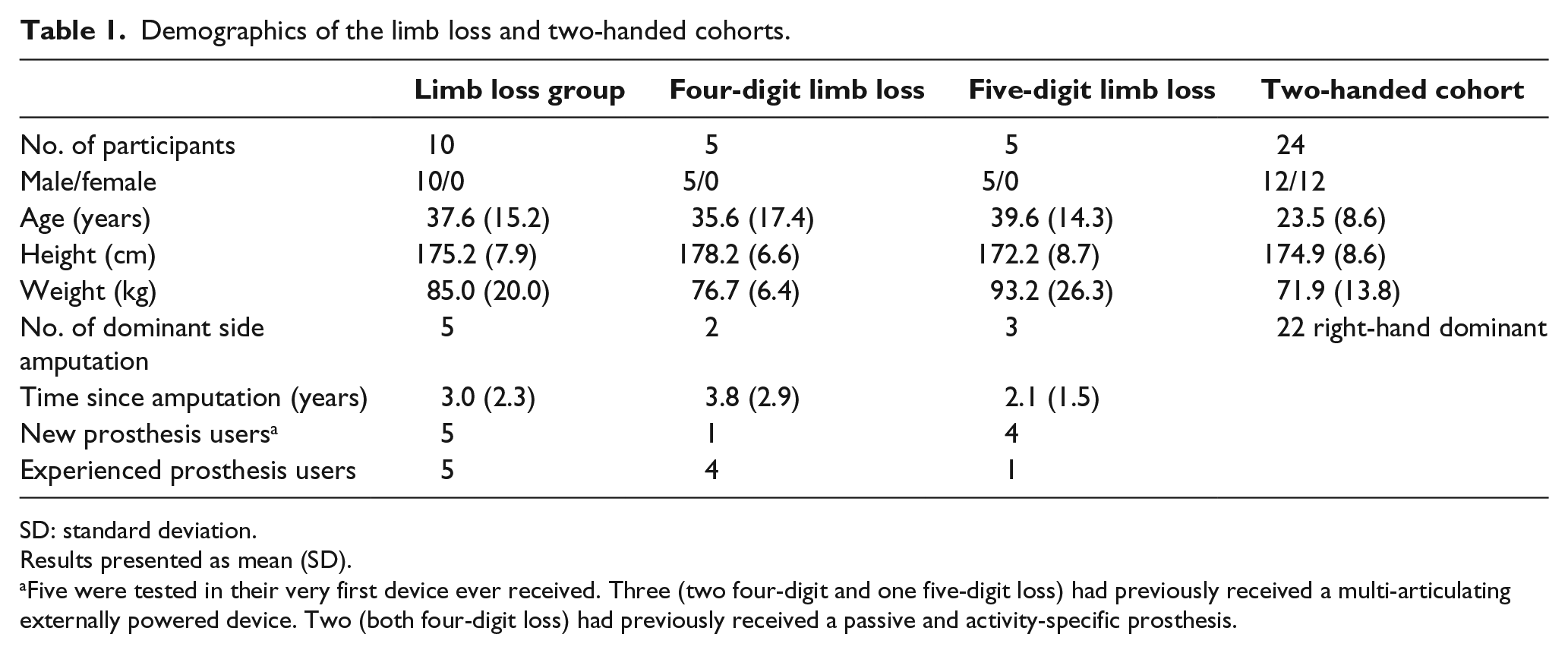
SD: standard deviation.
Results presented as mean (SD).
Five were tested in their very first device ever received. Three (two four-digit and one five-digit loss) had previously received a multi-articulating externally powered device. Two (both four-digit loss) had previously received a passive and activity-specific prosthesis.
The limb loss participants demonstrated several significant differences in SHAP scores, with the prosthesis scoring higher than the non-prosthesis condition (Table 2). As a subgroup, the five-digit group showed significant improvement in scores in almost every category, indicating improved function with the prosthesis.
SHAP scores for limb loss groups.
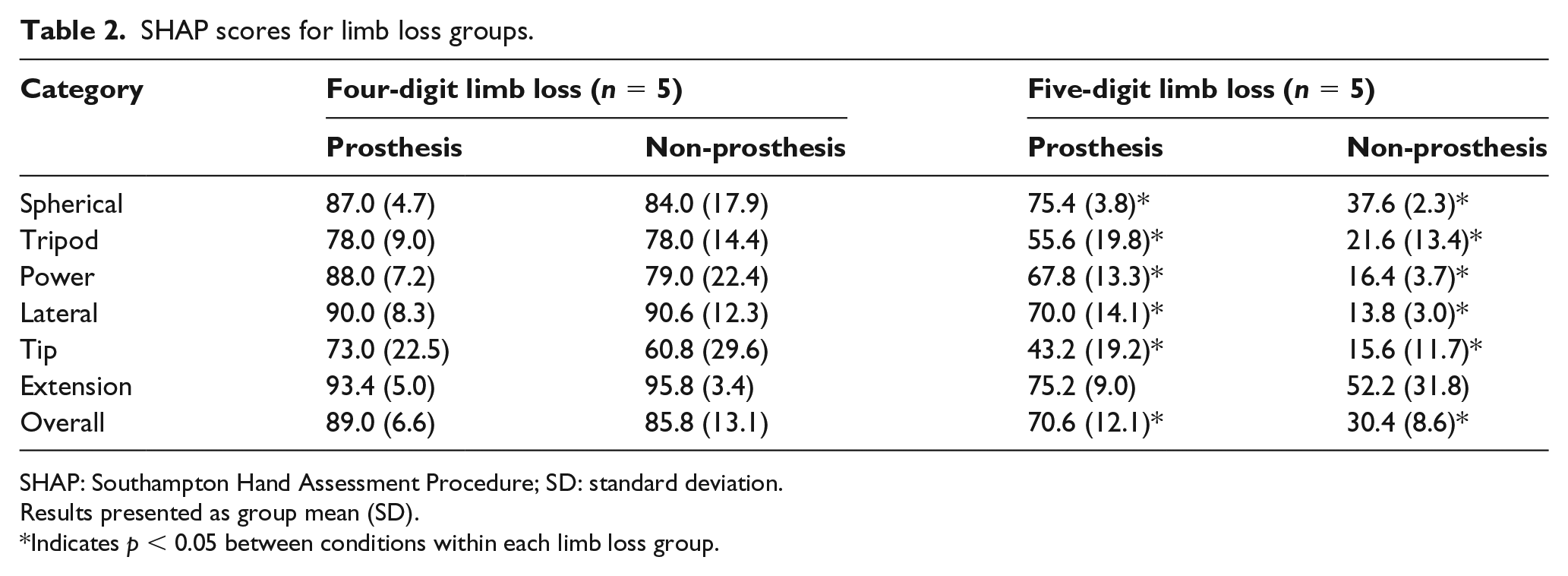
SHAP: Southampton Hand Assessment Procedure; SD: standard deviation.
Results presented as group mean (SD).
Indicates p < 0.05 between conditions within each limb loss group.
The four-digit limb loss participants were able to successfully complete all SHAP tasks, regardless of prosthesis condition. All five-digit limb loss participants were able to complete all tasks with the prosthesis, but one participant could not complete the picking up coins task within the maximum time allowed. All five-digit limb loss participants were unable to complete at least one of the following tasks without their prosthesis and received the maximum time: lateral light and heavy (n = 5), tip light (n = 2) and heavy (n = 3), extension light and heavy (n = 2), picking up coins (n = 5), button board (n = 4), simulated food cutting (n = 5), glass jug pouring (n = 5), carton pouring (n = 5), lifting heavy object (n = 5), lifting light object (n = 5), open/close zipper (n = 3), and rotate a screw (n = 5).
Several differences were seen in kinematics between prosthesis conditions during the SHAP, with almost every variable showing increased motion during the non-prosthesis condition (Supplemental Material). The tasks representing the largest changes between conditions included the power grip tasks (moving a weighted cylindrical object between specified locations) (Table 3) and jar lid opening (Table 4). Due to the complex nature of upper limb movement, and the frequent turning over of the palm during several tasks, the cameras sometimes lost sight of the wrist and elbow anatomical markers, leading to some temporal gaps in the data. Some variables could not be calculated due to missing or incomplete data. These missing variables are noted for each task. In addition, scapular movement was not captured for two participants (one four-digit and one five-digit limb loss) due to equipment malfunction.
Kinematic results for power tasks.
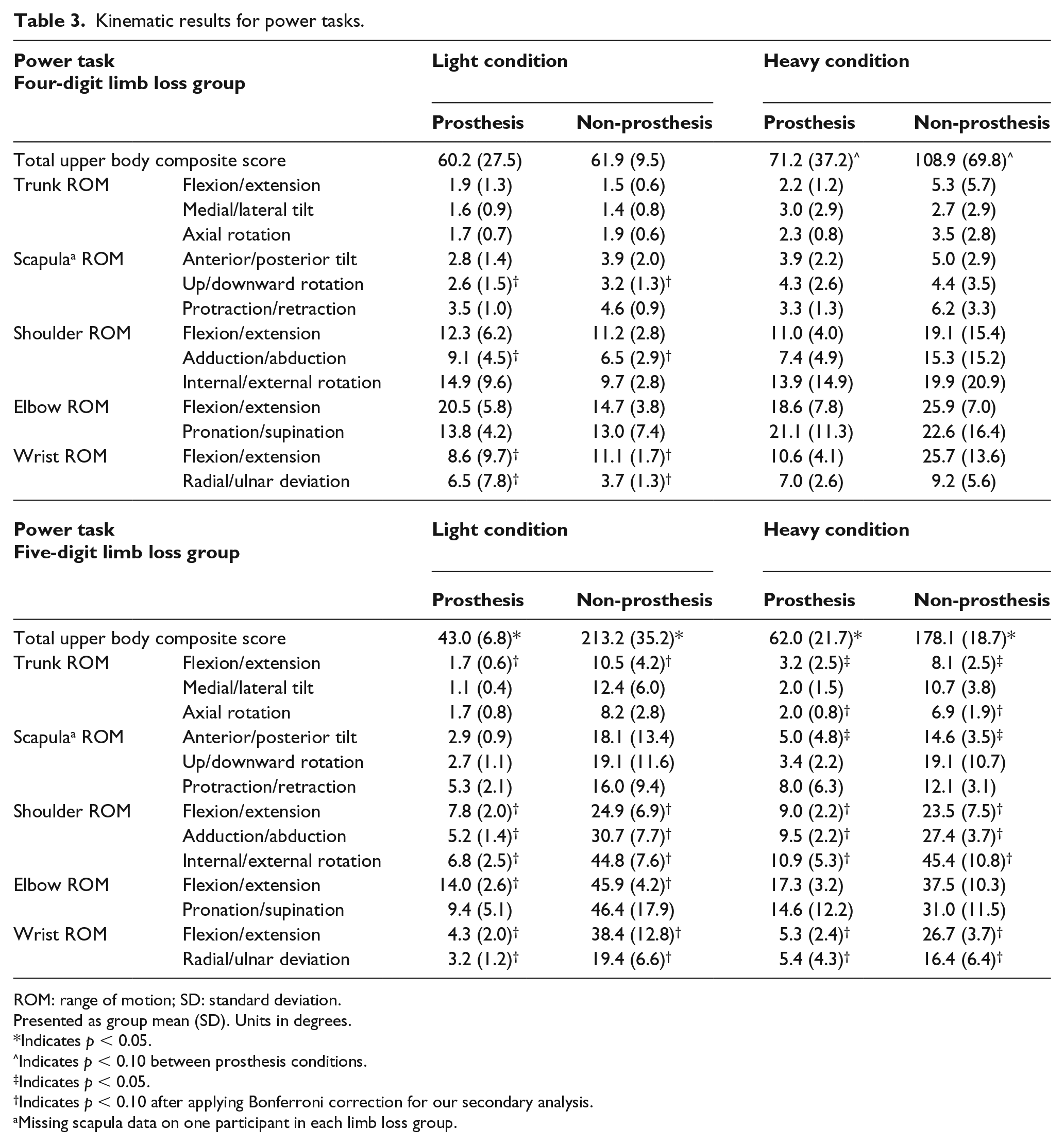
ROM: range of motion; SD: standard deviation.
Presented as group mean (SD). Units in degrees.
Indicates p < 0.05.
Indicates p < 0.10 between prosthesis conditions.
Indicates p < 0.05.
Indicates p < 0.10 after applying Bonferroni correction for our secondary analysis.
Missing scapula data on one participant in each limb loss group.
Kinematic results for jar lid opening.
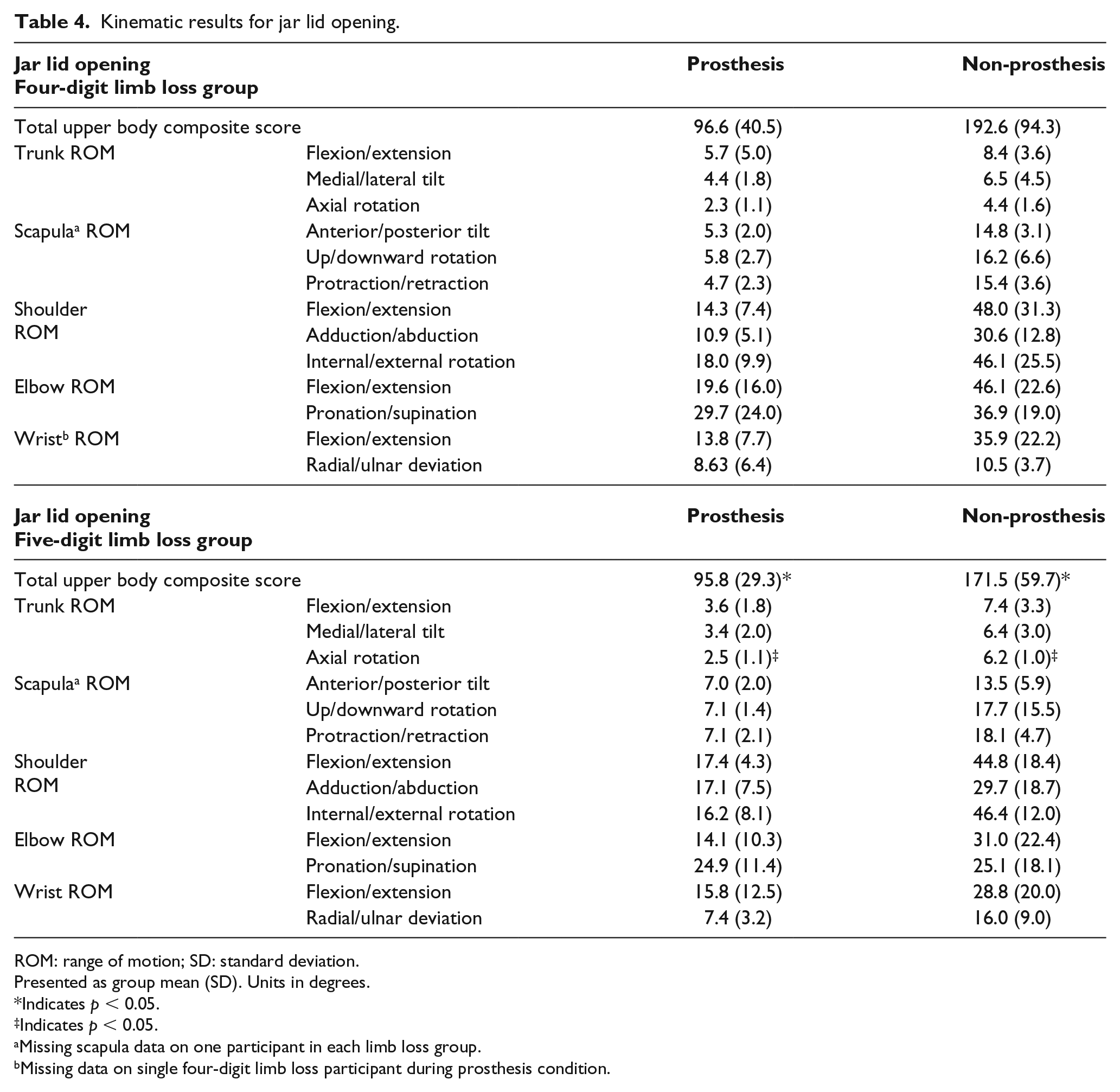
ROM: range of motion; SD: standard deviation.
Presented as group mean (SD). Units in degrees.
Indicates p < 0.05.
Indicates p < 0.05.
Missing scapula data on one participant in each limb loss group.
Missing data on single four-digit limb loss participant during prosthesis condition.
Visual comparison of kinematics to the ROM values for the two-handed group revealed that the prosthesis condition, regardless of amputation level, had joint ROMs similar to the normative sample whereas there were more apparent differences in the non-prosthesis results. A representative set of plots showing the differences between the limb loss and two-handed cohorts in kinematic outcomes for the jar lid opening task are shown in Figure 3.
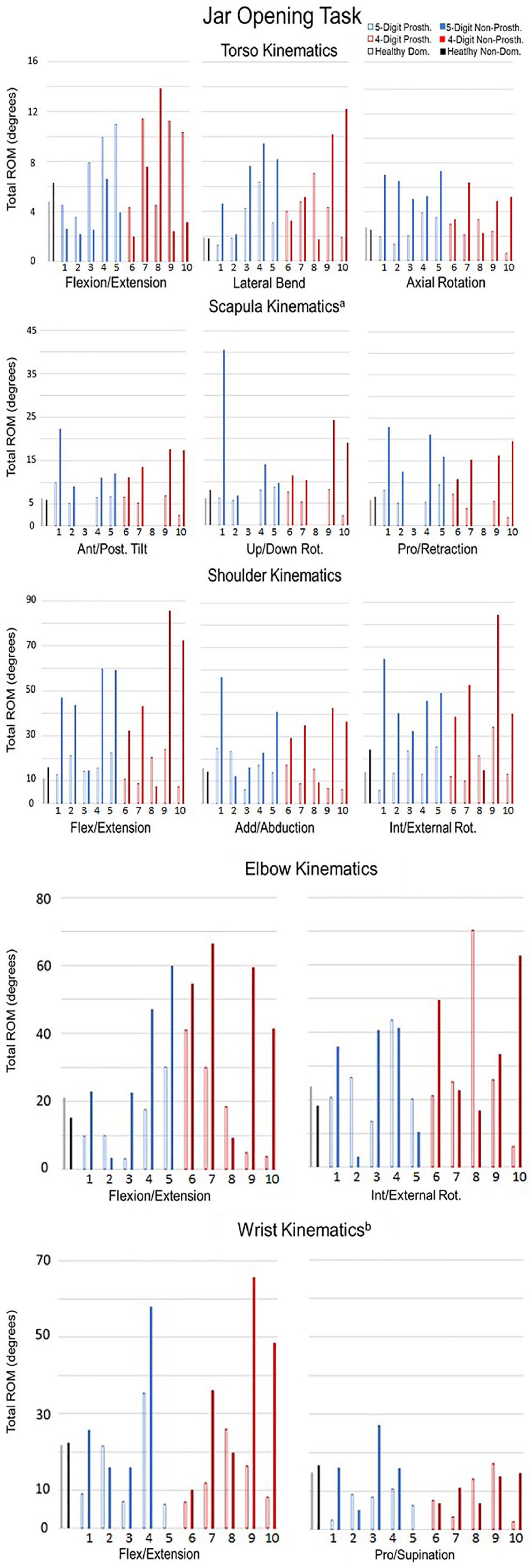
Total joint ROMs experienced during the jar lid opening task. Each limb loss participant is shown with their prosthesis (non solid bar) and without their prosthesis (solid bar) along the x-axis. Healthy dominant and non-dominant group mean shown as visual guide.
Discussion
The objective of this investigation was to examine how individuals with partial hand limb loss perform with and without a multi-articulating externally powered hand prosthesis while completing the SHAP, a standardized assessment of hand function. The results presented here indicated that the prosthesis was able to improve function for the five-digit limb loss group and reduce overall joint compensation for all limb loss participants compared with their non-prosthesis results.
The five-digit limb loss group had significantly higher SHAP scores with the prosthesis than without, in almost every category measured, indicating improved function. The four-digit limb loss group had no statistical differences between conditions in SHAP scores, but the kinematic results demonstrate decreased ROM with the prosthesis. In comparison to a previous study, Whelan and Farley, 16 individuals in this study demonstrated higher scores in the SHAP with and without the prosthesis in both four-digit and five-digit groups. Notably, in this study the four-digit group SHAP scores were considerably higher without a prosthesis. This may be attributed to the ROM and strength requirements for the remaining thumb, resulting in a sample that had a higher base level of function. Of the 10 limb loss participants, 8 had higher SHAP scores during the prosthesis condition than the non-prosthesis condition.
As the SHAP score estimated function solely based on speed, the kinematics of the movements were analyzed separately to determine differences in movement patterns between prosthesis conditions. Kinematic analysis showed the non-prosthesis condition resulted in significantly increased joint ROM across multiple variables. The heavy tasks resulted in more differences in outcomes than the light tasks, with the non-prosthesis condition resulting in increased joint motion. Kinematic analysis of SHAP ADLs (page turning, jar lid opening, simulated food cutting) resulted in similar larger joint ROMs for the non-prosthesis condition. While all participants were able to complete the page turning and jar lid opening, the five-digit limb loss group had a harder time for both. Page turning required different techniques between five-digit and four-digit participants. This resulted in more elbow supination/pronation for the five-digit group, but this was preferable to shoulder compensation.
Both limb loss groups struggled during the jar lid opening task without the prosthesis. To open the jar without the prothesis, participants were required to generate a strong friction force between the lid and their residual palm while stabilizing or applying a counter torque to the jar with their intact hand. This strategy contorted the body over the jar, as seen by increased composite score and trunk ROM.
It was clear that, for most joint motions, the prosthesis condition outcomes fell within or close to the bounds set by the two-handed data. The four-digit limb loss group did have fewer differences in joint ROMs between conditions and their non-prosthesis condition was more comparable to the two-handed results than the five-digit limb loss group’s non-prosthesis condition.
Due to a low number of kinematic analyses in the literature involving upper limb movement and people with limb-loss, it is difficult to compare this investigation to previous work. One investigation by Murgia et al. performed a kinematic analysis of two-handed participants performing the jar lid opening and carton pouring tasks within the SHAP. Their investigation noted the inherent difficulty in collecting useful kinematic data on upper limb movement due to the non-cyclical nature of the movement and inconsistency in data collection protocols. 20 As they collected data on two-handed participants, we are unable to compare the results to our population. It should be noted that their study indicated that there is inconsistency in the kinematics of upper limb movement, due to differing starting and stopping positions, which is why the presented study focused on the overall joint ROMs.
The field of ergonomics may be able to inform on the possible risks associated with the movements seen in our participants. The link between forceful exertions, repetitive movements, awkward posture, and the development of MSDs has been well studied and previous work has shown that these types of factors can increase the risk of developing a MSD.21–24 As demonstrated by the results presented in this investigation, the limb loss participants experienced more severe and awkward joint movements without their prosthesis. The use of the arms and wrists in an awkward or non-neutral posture has been reported by several investigations as a risk factor in the development of MSDs.25–27 In addition, tasks like the jar lid opening and simulated food cutting required the limb loss participants to leverage their residual limb to increase force to complete the tasks. The magnitude of hand force has been linked to the development of MSDs.24,26,28
Amputation of the upper limb can result in overuse injury developing on the intact side, as function is transferred away from the impaired hand. In these situations, the intact side would experience greater loads, would experience increased repetitions during certain tasks, and may experience muscle fatigue which can lead to further impairment and disability.24,29,30 The five-digit limb loss participants in the presented investigation were unable to complete at least half of the SHAP tasks without their device. With the prosthesis, the five-digit limb loss participants were able to complete all tasks. It may be that they cannot complete them as easily or quickly as their intact hand, but they can complete them, thereby reducing the increased burden on the intact side and possibly reducing the potential for the development of an MSD. In addition, the prosthesis can assist the intact limb in performing tasks to a greater extent than the residual limb, reducing the overall burden on the intact side.
Limitations
There are limitations to this investigation that should be considered when interpreting its results. Only 10 limb loss participants completed the protocol. Recruitment of limb-loss research participants can be challenging due to low population number, particularly for our target of people with partial hand loss with a specific prosthesis. This study was exploratory in nature and there is need for larger sample populations in future studies. Variability in methods to complete tasks increased variability in our results. The inclusion/exclusion criteria for the limb loss participants may have resulted in a cohort with good control and strength of the residual limb and may not be representative of the general population. Inclusion/exclusion criteria may have also resulted in the recruitment of highly functional four-digit limb loss participants, a possible factor for the lack of SHAP score differences between conditions. In addition, only one specific prosthesis was investigated, limiting the generalizability to other prostheses for individuals with partial hand loss. The limitations of skin-based passive marker motion systems should also be taken into consideration, though the within-subject research design should have minimized the effects of skin motion artifact associated with motion capture. The design of the SHAP made motion capture difficult, as several tasks resulted in either the SHAP box or participant’s body blocking cameras from view. We were unable to complete kinematic analyses on several tasks due to these limitations. The SHAP score is also limited to the speed at which the task is completed and does not take into account compensation or other factors important to return to function.
Conclusion
The use of an externally powered hand prosthesis with individually articulating digits resulted in improved SHAP scores and changes in upper limb kinematics. This may indicate that the prosthesis decreases overall upper body motion, improves function, and reduces the probability of overuse or other flow-through injuries by lessening the compensatory movements required. In addition, the use of the prosthesis allowed the five-digit limb loss participants to complete all tasks, something they could not do without the prosthesis.
Supplemental Material
PartialHand_SuppMat_Revision_edit – Supplemental material for Biomechanical analysis of users of multi-articulating externally powered prostheses with and without their device
Supplemental material, PartialHand_SuppMat_Revision_edit for Biomechanical analysis of users of multi-articulating externally powered prostheses with and without their device by Andrea B Wanamaker, Lynsay R Whelan, Jeremy Farley and Ajit MW Chaudhari in Prosthetics and Orthotics International
Footnotes
Author contributions
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All data collections, analyses, results, and conclusions were completed at the Ohio State University by the Ohio State University team (ABW and AMWC). The team from Touch Bionics (LW and JF) did not assist in these processes other than to recruit and transport participants to and from the research site for testing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was completed using funding and assistance from Touch Bionics by Össur.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.