
Abstract
Background:
Prosthetic feet are prescribed based on their mechanical function and user functional level. Subtle changes to the stiffness and hysteresis of heel, midfoot, and forefoot regions can influence the dynamics and economy of gait in prosthesis users. However, the user’s choice of shoes may alter the prosthetic foot-shoe system mechanical characteristics, compromising carefully prescribed and rigorously engineered performance of feet.
Objectives:
Observe the effects of footwear on the mechanical properties of the prosthetic foot-shoe system including commonly prescribed prosthetic feet.
Study design:
Repeated-measures, Mechanical characterization.
Methods:
The stiffness and energy return was measured using a hydraulic-driven materials test machine across combinations of five prosthetic feet and four common shoes as well as a barefoot condition.
Results:
Heel energy return decreased by an average 4%–9% across feet in all shoes compared to barefoot, with a cushioned trainer displaying the greatest effect. Foot designs that may improve perceived stability by providing low heel stiffness and rapid foot-flat were compromised by the addition of shoes.
Conclusion:
Shoes altered prosthesis mechanical characteristics in the sagittal and frontal planes, suggesting that shoe type should be controlled or reported in research comparing prostheses. Understanding of how different shoes could alter certain gait-related characteristics of prostheses may aid decisions on footwear made by clinicians and prosthesis users.
Clinical relevance
Shoes can alter function of the prosthetic foot-shoe system in unexpected and sometimes undesirable ways, often causing similar behavior across setups despite differences in foot design, and prescribing clinicians should carefully consider these effects on prosthesis performance.
Keywords
Background
Recent systematic investigations have generated strong evidence that the stance-phase mechanical properties of passive prosthetic feet can have considerable effects on rehabilitation outcomes (e.g. walking dynamics and metabolic economy) of persons with lower-limb amputation.1–9 The mechanical properties of a prosthetic device quantified independent of the user10–12 are important for understanding end-user biomechanical performance. However, a prosthetic foot is almost always used with a shoe, and the effect of different shoes on the performance of prosthetic feet is poorly understood. A clinician may choose an appropriate prosthetic foot by matching rigorously engineered prosthetic foot characteristics with the patient’s functional level only to have the prosthetic foot-shoe system characteristics substantially altered by the patient’s choice of shoes. The effects of footwear on the mechanical function of prosthetic feet have received little attention in the literature, resulting in a lack of understanding of how shoe choices influence the end-user device which has been clinically optimized based on a patient’s mobility level and health status.13–17 Consequently, clinicians are unaware if their patients are deriving the full benefit of prosthetic components so they may achieve their full rehabilitation potential. Efforts have been made recently to establish standard guidelines for classifying prosthetic feet based on their functional characteristics, 18 and these standards have been used to aid in interpretation of results of biomechanical comparative studies. 19 The proposed classification scheme uses pass-fail thresholds of mechanical measurements, such as displacement and energy return under specified load magnitudes and direction, to categorize prosthetic feet by their mechanical function (e.g. dynamic and multiaxial). 18 Consequently, the addition of certain shoes may modify mechanical function of the prosthetic foot so dramatically that they produce a mismatch between outcome behavior and original classification assignments meant to facilitate clinical component recommendations.
The most comprehensive investigation on the effect of footwear on the mechanical properties of prosthetic feet is 25 years old, 20 but demonstrated the importance of using bench-top methods to quantify mechanical properties of prosthetic feet and shoes to improve understanding of their combined effects on walking performance. However, the van Jaarsveld study along with others has been concerned only with sagittal-plane effects such as roll-over shape 21 and heel viscoelastic properties. 22 A single type of prosthetic foot may be used for a wide variety of different activities and within a wide variety of different shoes, and understanding how the prosthetic foot functions within different footwear is an important part of the prescription process. Although an issue for clinical outcomes, the poorly defined relationships between footwear and prosthetic foot mechanical properties are also highly relevant for biomechanical studies of prosthesis comparative effectiveness that do not control for or accurately report subject footwear. Previous investigations have suggested that the addition of footwear tends to compromise the individual and intended design characteristics of prosthetic feet,20–22 which would indicate that this uncontrolled variable would potentially result in inconclusive findings of comparative studies. The purpose of this study was to evaluate the effects of footwear on the sagittal- and frontal-plane stance-phase mechanical properties of the prosthesis-shoe system including commonly prescribed prosthetic feet representing a range of mobility levels. Results from this study will facilitate a more complete and updated understanding of how current prosthetic designs are influenced by shoes and what implications this may have on clinical recommendations and biomechanical studies of prosthesis comparative effectiveness.
Methods
To assess the mechanical effects of shoes on prosthetic feet, linear stiffness and energy return were estimated for five prosthesis designs:
Cadence (Trulife, Dublin, Ireland);
Seattle Lightfoot 2 (Trulife, Dublin, Ireland);
Multiflex foot/ankle (Endolite, Miamisburg, OH, USA);
SACH (Ohio Willow Wood, Mt Sterling, OH, USA);
Single-axis 1H38 (Otto Bock, Duderstadt, Germany).
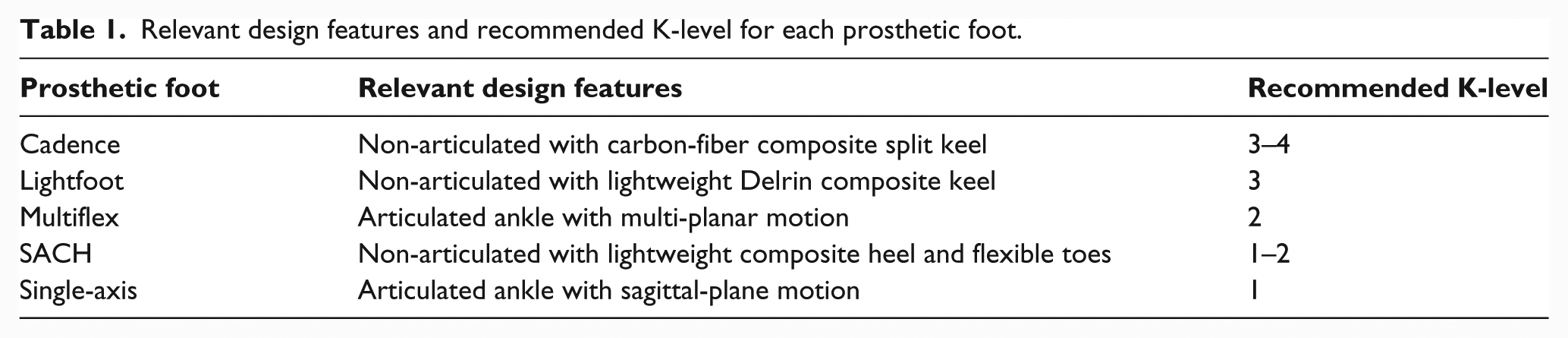
These prosthetic feet were selected based on anecdotal evidence from prosthetists as commercial devices available at the time of testing that cover a range of commonly prescribed functional designs and patient mobility as defined by the Medicare Function Classification Level system 23 per manufacturer recommendations (Table 1). For consistency, all feet were appropriate for an 80-kg patient with 27-cm foot length for the left side.
Relevant design features and recommended K-level for each prosthetic foot.
Each prosthetic foot was tested under five “footwear” conditions (Figure 1):
Barefoot;
Trainer (GT-2120, Asics, Kobe, Japan; heel of sole thickness 34 mm, durometer Shore 70 A, and curved with apex at 72% of shoe length from toe end; forefoot of sole thickness 19 mm, durometer Shore 70 A, and curved with apex at 76% of shoe length from heel end);
Hiking boot (Earthkeepers Rugged, Timberland, Greensboro, NC, USA; heel sole of thickness 34 mm, durometer Shore 55 A, and curved with apex at 75% of shoe length from toe end; forefoot sole of thickness 18 mm, durometer Shore 55 A, and curved with apex at 61% of shoe length from heel end);
Leather dress (Oxford, Stafford, Dallas, TX, USA; heel sole of thickness 29 mm, durometer Shore 110 A, and flat shape; forefoot sole of thickness 10 mm, durometer Shore 120 A, and curved with apex at 61% of shoe length from heel end);
Flat (Mossi Damien, Mossimo Supply Co., New York, NY, USA; heel sole of thickness 14 mm, durometer Shore 65 A, and flat shape; forefoot sole of thickness 7 mm, durometer Shore 65 A, and curved with apex at 76% of shoe length from heel end).

Images of the footwear used for each experimental condition (left to right: hiking boot, trainer, leather dress, and flat shoe) with the Ohio Willow Wood SACH foot included for scale.
Shoes were selected to represent a range of footwear commonly used during daily living and include types appropriate for laboratory-based gait analyses. For each footwear condition, the prosthetic feet were tested using a hydraulic-driven material test machine (Instron, Model 8800, Norwood, MA, USA; Figure 2) to measure instantaneous longitudinal force and displacement under four operational loading conditions:
Initial contact: 15° sagittal inclined loading surface (heel test);
Midstance: level loading surface (midstance test);
Terminal stance: 20° declined loading surface (keel test);
Inversion: 15° coronal inclined loading surface (inversion test).
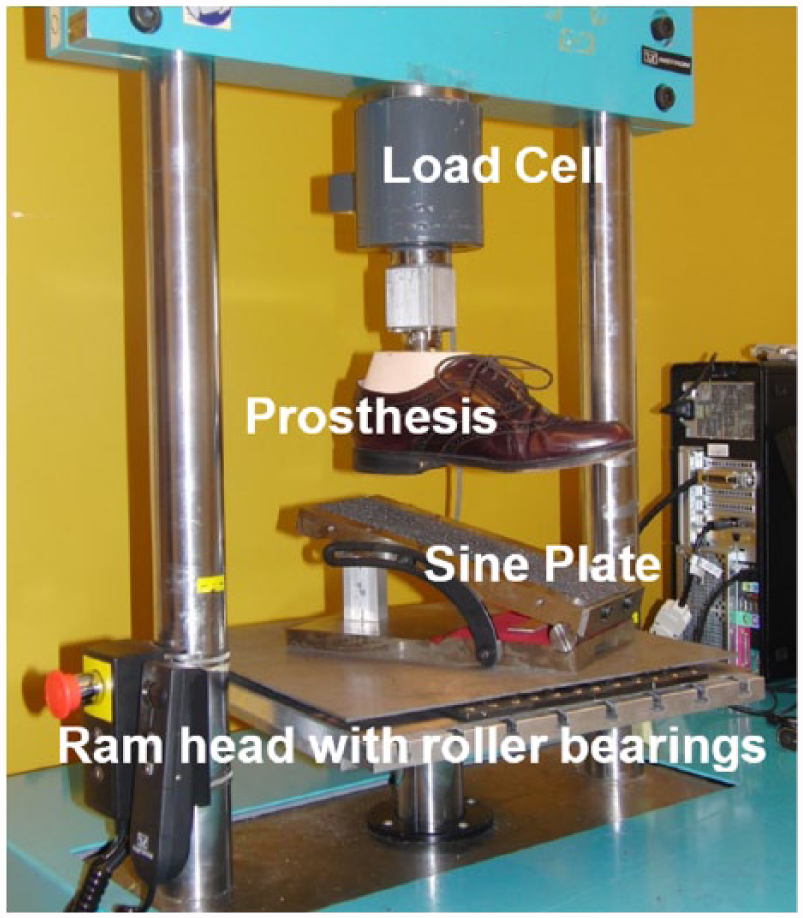
Materials testing machine used for mechanical tests and example setup for the heel test.
The setup and mechanical tests used in this study were adapted from those described in the American Orthotic & Prosthetic Association (AOPA) Foot Project Report 18 to characterize prosthesis mechanical behavior, which have been demonstrated to have excellent repeatability, 24 and are modeled after standardized methods for characterizing prosthesis mechanical properties independent of the user.11,12
For all loading conditions, the prosthetic foot was aligned on a level loading surface and a sine-plate was used to adjust the loading surface angle. The alignment process involved loosely attaching the foot male pyramid adapter to the load-cell fixture female pyramid adapter, slowly loading to 50 N, and then tightening the set screws to 12 N m using a torque wrench. Prosthetic feet were realigned and the proportional–integral–derivative control parameters of the materials test machine were optimized for each prosthesis-footwear condition. For all tests, the sine-plate rested on roller bearings to minimize shear forces and slipping of the foot. When testing the barefoot prostheses under the midstance and inversion conditions, a heel block was fixed to the sine-plate during alignment and testing to accommodate for foot heel height. For each footwear and loading condition, the prosthetic foot was pre-loaded to 50 N and then underwent two cycles of loading to 1230 N and unloading to 50 N at a loading rate of 200 N/s. Data from only the second load cycle were used for processing and this testing cycle was repeated four times.
Using custom software in MATLAB (MathWorks, Natick, MA, USA), the percentage of energy return (% Joules) was estimated by dividing the area under the unloading force–displacement curve by the area under the loading curve. Area was calculated using the trapezoidal numerical integration method. Stiffness (N/mm) was estimated as the average slope of a best-fit linear approximation of the loading and unloading curves using the least-squares regression method. Estimations of energy return and stiffness were averaged over the four loading–unloading cycles.
Results
A representative set of loading-unloading curves for the barefoot and hiking boot conditions (selected as an illustrative example of footwear effects) under the heel test are presented in Figure 3. This pattern generally reflects the behavior for all loading conditions, apart for the heel test in which the articulated devices (Multiflex and Single-axis) demonstrated distinct loading profiles for the barefoot condition as the feet rapidly transitioned to foot-flat. The estimated stiffness and energy return for each footwear and loading condition are displayed in Figures 4 and 5, respectively. The standard deviation of all measured outcomes was between 0.1% and 4.7% of the mean, demonstrating the high repeatability of these tests. Data for the average changes in energy return, stiffness, and displacement relative to the barefoot condition for feet (across footwear) and footwear (across feet) conditions are presented in Tables 2 and 3, respectively. Table 4 displays keel and heel classifications based on the AOPA guidelines for each combination of prosthetic foot and footwear conditions.
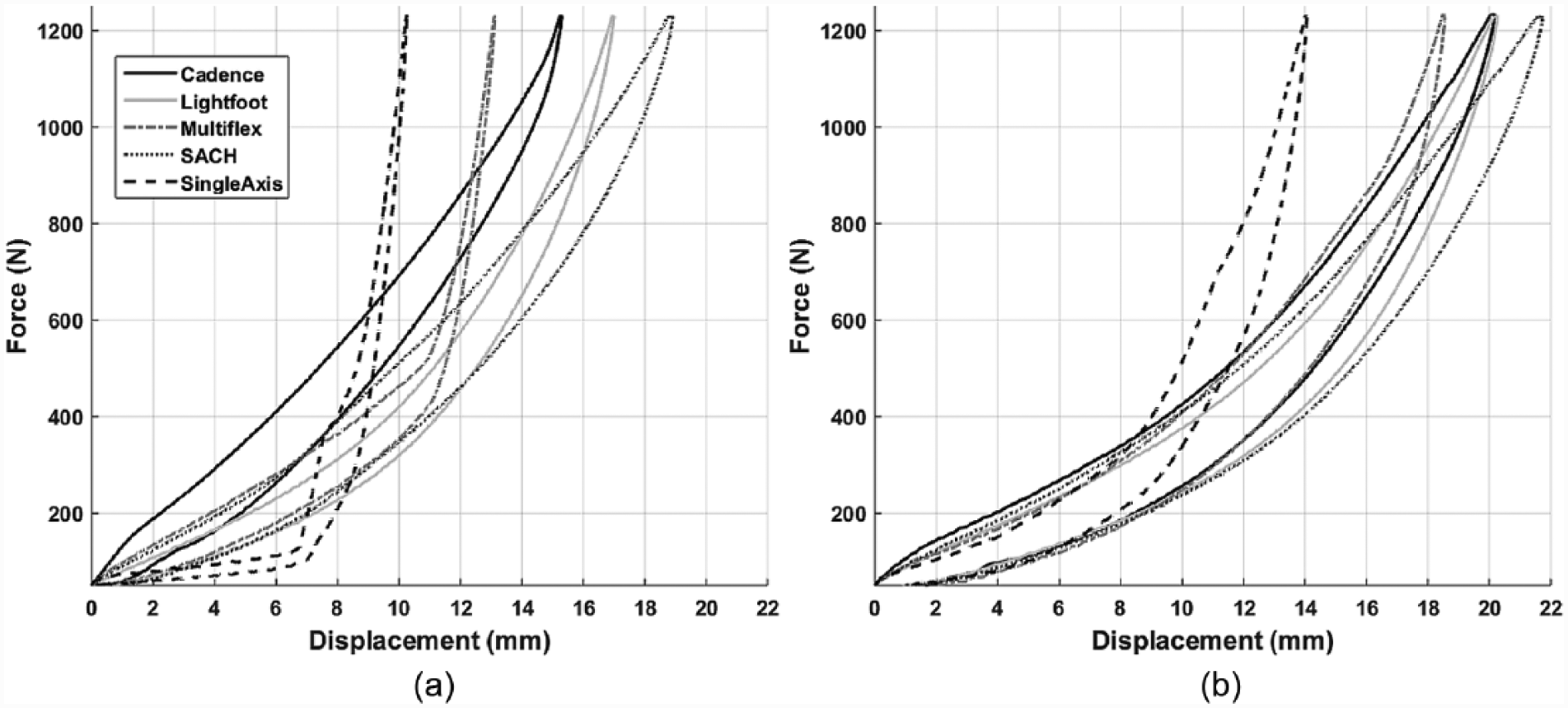
Representative loading-unloading curves for the heel test under the (a) barefoot and (b) hiking boot conditions.
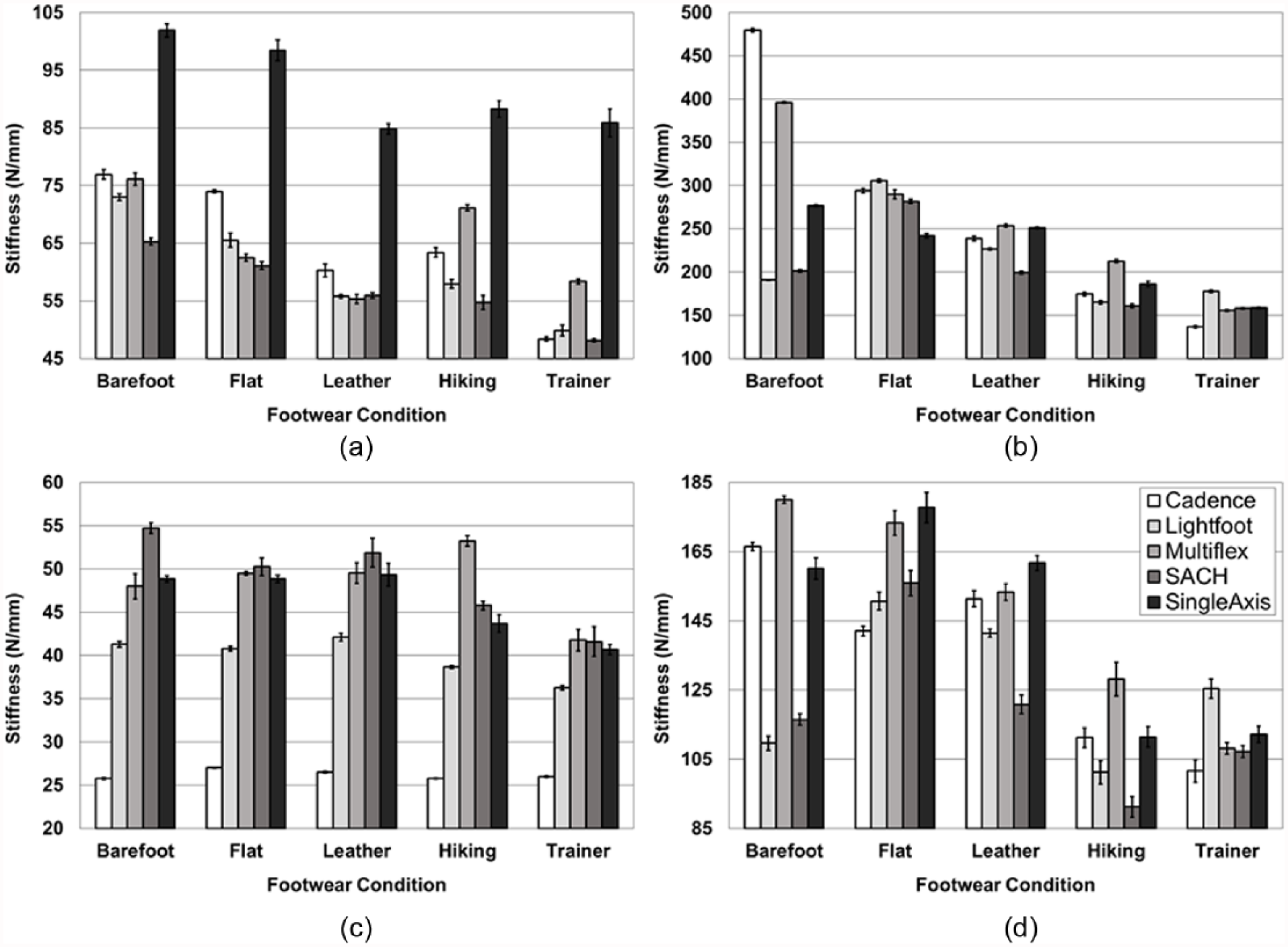
Estimated stiffness for all prosthetic feet and footwear conditions during (a) initial contact, (b) midstance, (c) terminal stance, and (d) inversion testing.
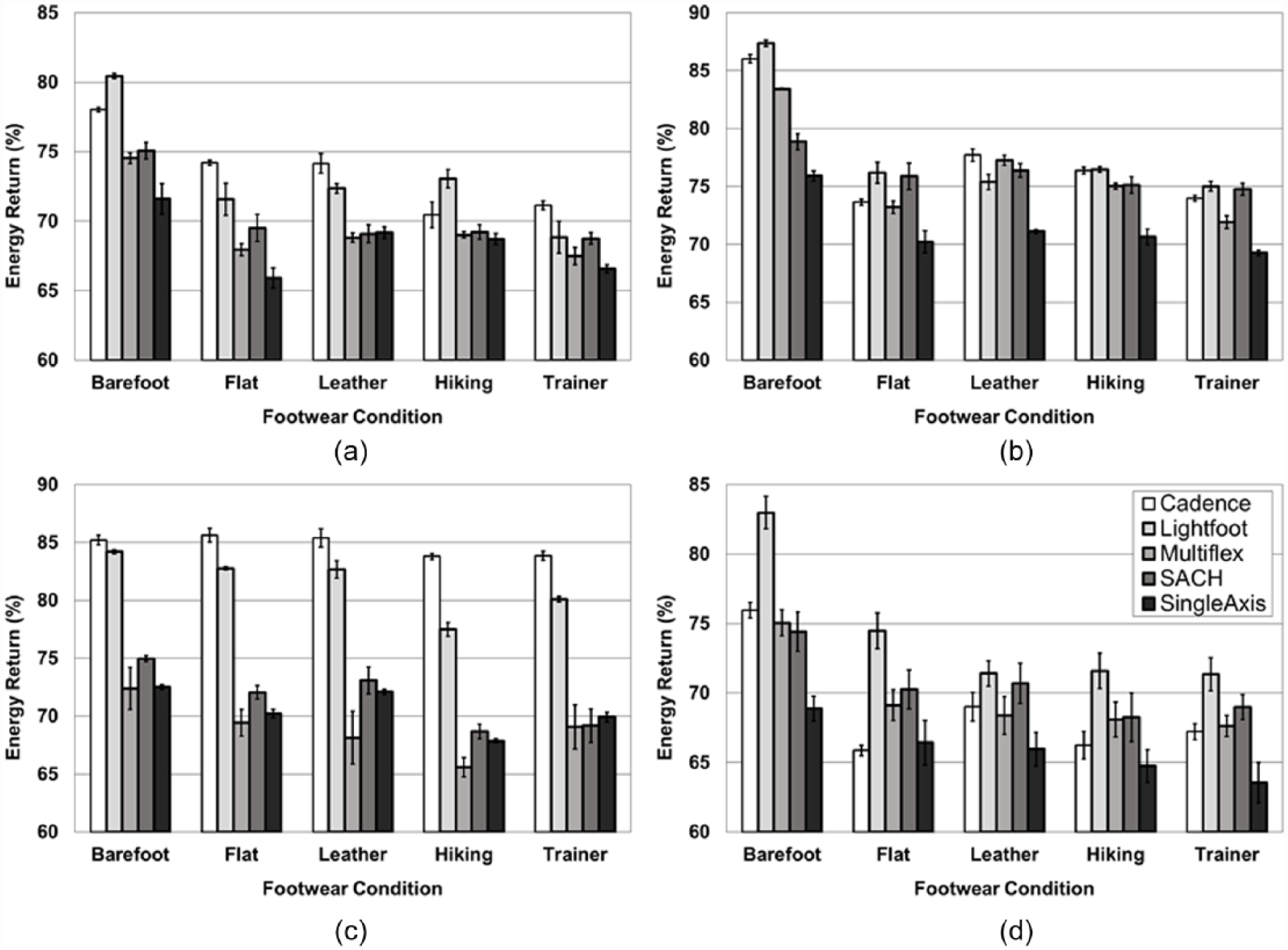
Estimated energy return for all prosthetic feet and footwear conditions during (a) initial contact, (b) midstance, (c) terminal stance, and (d) inversion testing.
Average (±1 SD) change in energy return, stiffness, and displacement relative to the barefoot condition (shoe value − barefoot value) across all footwear conditions.

Average (±1 SD) change in energy return, stiffness, and displacement relative to the barefoot condition (shoe value − barefoot value) across all feet.

Keel and heel classifications for each prosthetic foot and footwear condition as assigned based on AOPA guidelines (Keel: Rigid ≤ 25 mm displacement, Flexible = ≥25 mm displacement and <75% energy return, Dynamic = ≥25 mm displacement and ≥75% energy return; Heel: Dynamic = ≥13 mm displacement or ≥82% energy return, Cushioned ≤ 13 mm displacement or <82% energy return). 18
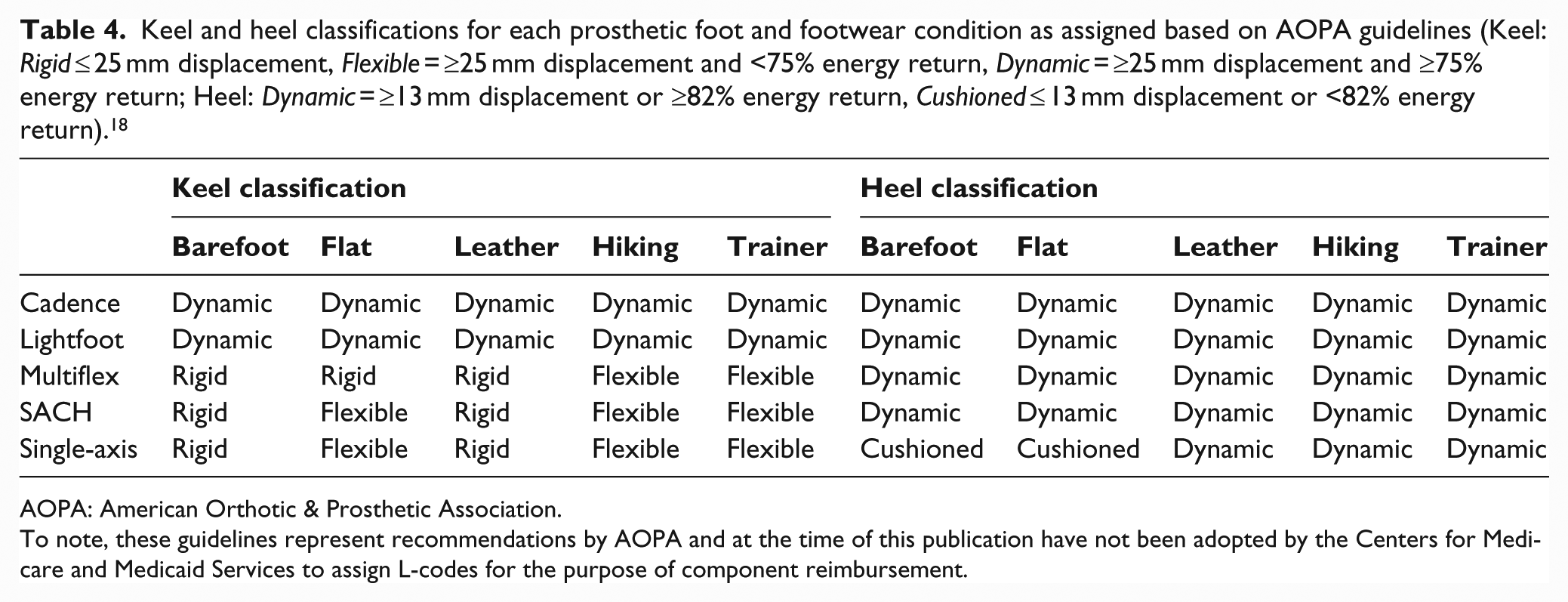
AOPA: American Orthotic & Prosthetic Association.
To note, these guidelines represent recommendations by AOPA and at the time of this publication have not been adopted by the Centers for Medicare and Medicaid Services to assign L-codes for the purpose of component reimbursement.
Discussion
Effects of shoes on prosthetic foot-shoe system loading behavior and stiffness
For the majority of loading conditions, the feet displayed a characteristic hysteresis curve for loading and unloading (Figure 3). However, the heel test was selected for presentation as the Single-axis and Multiflex feet demonstrated unique behavior for this testing scenario between the barefoot and shoe conditions. When barefoot, these feet exhibited lower stiffness as the foot rotated around the articulated joint and then transitioned to higher stiffness once the foot achieved full plantar contact with the loading surface (Figure 3(a)), and this behavior became less pronounced for all footwear conditions (Figure 3(b)). The barefoot behavior is a desired function of articulated devices as they are clinically recommended for patients of low mobility such that early foot-flat is achieved following initial contact to provide a stable base-of-support during weight transfer.25,26 A recent investigation suggested that prosthetic foot time to foot-flat may be inversely related to perceived gait stability of persons with unilateral below-knee amputation. 27 Importantly, the addition of shoes appears to alter the loading profile of articulated devices under low force levels such that foot-flat is not as readily achieved. Consequently, clinicians should be aware that shoes may cause an undesirable change in mechanical function of those systems using prosthetic feet meant to aid perceived gait stability. Given the increased fall risk, impaired functional balance, and low balance confidence of lower-limb prosthesis users28–30 and its relationship to patient quality of life,31,32 this issue warrants further attention.
In alignment with previous research,20,22 the addition of shoes generally tends to increase the compliance of prosthetic foot-shoe systems across loading conditions. In terms of walking dynamics, a decrease in stiffness would generate greater simulated ankle range-of-motion,1,2,7 but systematic investigations suggest that improved walking mechanics and metabolic economy are primarily encouraged through increased forefoot compliance which was not noticeably altered with shoes in this study. An increase in forefoot compliance would theoretically facilitate greater energy storage to aid in push-off during terminal stance for forward ambulation.33–35 Consequently, it seems unlikely that any mechanical or metabolic benefit would be provided from footwear, but this may be considered a positive result as the desired mechanical function of the keel is retained. However, to place this study’s results into context, a previous investigation suggested that changes in midstance, heel, and keel linear stiffness by as little as 56, 23, and 12 N/mm, respectively, can have noticeable effects on prosthetic ankle range-of-motion and bilateral ground reaction force peaks, knee moment peaks, and muscle activity. 7 The changes to midstance and heel stiffness with addition of footwear observed in this study (Figure 4, Tables 2 and 3) often exceeded these potentially clinically meaningful differences.
Patients anecdotally report an undesirable feeling of “sinking” into their step when heel and midfoot compliance is too low, and some of the greatest reduction in stiffness compared to the barefoot condition was observed for the heel and midstance test. Consequently, the use of certain shoes, such as the trainer, may in fact exacerbate this perception and this should also be considered when recommending devices and/or associated device settings/categories in conjunction with patient preferences on footwear. Similar interpretations can be made with the reductions observed in stiffness for the inversion test, in which additional compliance may in fact compromise a feeling of stability as the patient pivots and/or transfers weight over the device during stance. Furthermore, some shoes (i.e. trainer, leather, and flat) were successful in essentially reducing keel, inversion, and/or midstance stiffness such that most prosthetic foot-shoe systems converged on a similar level of compliance, thereby compromising the individual characteristics of each prosthetic foot design. These results are also supported by previous research that suggested that the addition of footwear to different prosthetic foot designs also tends to force the overall system roll-over shape, which can be influenced by prosthesis stiffness, to converge on a similar profile. 21 A global reduction in stiffness would generate a smaller roll-over shape radius. 12 While the trainer seemed to have the greatest effect, the flat shoe altered compliance the least across all conditions and this seems reasonable given its low profile and minimal material.
Effects of shoes on prosthetic foot-shoe system energy return
Similar to the effects on stiffness and aligned with previous research,20,22 the addition of footwear tends to diminish energy return for all loading conditions but less so for the keel test, with the trainer having the greatest influence. A decrease in energy return as generated with the addition of shoes may be an advantageous result for initial contact, as loads are absorbed and dissipated to help protect the residual limb from harmful forces. 1 However, for those loading scenarios such as midstance and inversion when the user is pivoting and/or transferring body weight across the prosthesis, an increase in energy dissipation may in turn increase difficulty in recovering energy to push-off on the prosthetic limb. This concept of energy recovery may be particularly important for terminal stance when the prosthetic foot should ideally demonstrate minimal energy dissipation to aid advancement of the prosthetic limb into swing without increased dependence on compensatory gait mechanisms for generating additional positive mechanical work.6,7,33–35 Fortunately, as with changes in stiffness, energy return for the keel test did not appear to be altered by the addition of footwear to the same degree as other foot regions, and so feet designed to assist terminal stance push-off through materials capable of high levels of energy return (e.g. carbon fiber) may still retain this function.
Implications for biomechanical studies, clinical recommendations, and prosthetic foot functional classification
Overall, the addition of shoes seems to modify the individual design characteristics of some prosthetic foot-shoe systems, often forcing a convergence of mechanical behavior. This result may partially explain the inconclusive findings of previous comparative effectiveness studies of different commercial prosthesis designs, 36 which rarely report subject footwear and consequently weakens their validity. Researchers should consider standardizing footwear to ensure that outcome differences are primarily due to modifications in prosthesis-specific mechanical function and not influenced by the uncontrollable effects of shoes, and/or including mechanical characterization data of the full prosthesis setup distal to the socket (foot, pylon, and shoes) alongside biomechanical outcomes to aid in interpretation of results. 11 Similar to prosthesis function, research participants would require acclimation to controlled footwear that could be addressed through targeted training and/or free accommodation with standardized shoes. Ideally, systematic investigations on effects of prosthesis properties would use experimental devices that do not require footwear and thus afford complete control over prosthesis mechanical function. 1
In terms of clinical recommendations, as clinicians do not commonly have control over a patient’s footwear selection, they may not be aware of the unpredictable effects of shoes on prosthesis mechanical function, consequently compromising their recommendations and resulting in suboptimal rehabilitation outcomes. Generally, it appears that the trainer and hiking boot had the greatest effect on heel and midstance properties across the tested iterations (Table 3), and this is likely due to the large heel height and relatively low durometer. These results suggest for clinicians that this combination of properties may create the greatest divergence from the intended function of the definitive prosthetic setup. The differences in heel-to-toe height differentials between shoes (ranging from 7 to 19 for the footwear in this study) would also compromise the original clinical alignment and modify the loaded roll-over shape of the prosthetic foot.12,21 Additionally, prosthetic users may change their shoes to meet the day’s anticipated challenges and substantial uncertainty remains as to the user-specific acclimation period needed when a user changes shoes and alters the mechanical properties of their prosthetic system. However, a clinical concept of equal importance is that both clinicians and users have the advantage of producing controlled adjustments in the prosthetic foot-shoe system mechanical function through the careful selection of footwear. Assuming that the user’s safety can be guaranteed, the same prosthetic foot could theoretically be used to generate different functional outcomes by changing the integrated shoe.
Furthermore, to optimize the clinical matching process of prostheses and patients for maximizing rehabilitation outcomes, steps have been taken to develop standardized methods to accurately and reliably classify prosthetic feet based on mechanical function (e.g. dynamic keel, cushioned heel).18,24 However, these classifications are based on displacement and energy return that may be problematic if footwear is not considered. For example, all three low mobility prostheses designs (Multiaxial, Single-axis, and SACH) displayed stiffness that allowed for keel displacement at 1230 N to qualify them as rigid per suggestions of the AOPA classification guidelines (<25 mm), but exceeded this threshold when combined with the trainer and hiking boot to be considered flexible (Table 4). Similarly, the Single-axis foot qualified as a cushioned heel for the barefoot and flat conditions, but qualified as dynamic when combined with the hiking boot, leather dress shoe, and trainer (Table 4). Furthermore, energy return of the Lightfoot heel (81%) was near the threshold to classify as dynamic (82%), but dropped well below this threshold with the addition of shoes (<72%) to in some cases match that of the cushioned SACH foot heel. To note, the Lightfoot heel classification did not change as it consistently passed the 13 mm displacement threshold. Critically, the addition of certain shoes may modify prosthetic foot-shoe system mechanical properties such that they no longer reflect the original prosthetic foot functional classifications that are used not only for clinical recommendations but also for healthcare reimbursement policy in some countries.
Limitations
A limitation of this study is that the implemented loading rates are below those that prosthesis users may experience during gait and this may partially explain why absolute values differ from another study which employed more realistic rates. 22 However, the purpose of this study was to demonstrate the trending effects of footwear on prosthetic foot-shoe system mechanical function and so this quasi-static application is an appropriate model for this purpose and has been employed in various prior investigations. 11 The absolute value results from this study closely match those observed in the similar investigation of 25 years prior which implemented a quasi-static assessment. 20 However, that study loaded prosthetic devices either to a maximum load or displacement, whichever came first, and this study may be considered an improvement on that assessment as all components were loaded to the same maximum force under a strict loading rate. Furthermore, although the force–displacement curves for all tested conditions demonstrated some level of non-linearity and this is commonly reported for testing composite structures such as prosthetic feet, 11 this study employed a consistent methodology of linear stiffness estimations that has been used in a similar clinically focused study. 37 Additionally, individual viscoelastic models of each shoe were not estimated and so it is not possible to evaluate the contribution of rotational and linear stiffness of the shoes to changes in mechanical properties. These methodological decisions allowed us to simplify interpretation of the results to better communicate the clinical relevance of our findings.
Finally, although a selection of common prosthesis designs and footwear were tested to cover a representative range of clinically relevant prosthetic foot-shoe combinations, these only encompass a small sample of available prosthetic feet and possible footwear choices. Further research should involve a greater range of shoe and prosthesis properties, possibly through experimental devices that allow for systematic modulations, to validate numerical modeling and aid interpretation of human subject experimentation results.
Conclusion
Results from this study emphasize that changes in compliance and energy return of a prosthesis setup are a function of the prosthetic foot and footwear, and both should be considered during the clinical process of recommending prostheses based on patient mobility levels and health status. Although some footwear could be used to enhance function of the prostheses by increasing compliance, minimal and/or rigid shoes should be considered if clinicians desire to retain the intended function of the device. However, future systematic and clinical studies are needed to identify the optimal mechanical characteristics of passive devices that maximize rehabilitation outcomes including factors of ambulation safety, metabolic economy, and comfort. Importantly, given the unpredictable but potentially clinically meaningful changes to prosthetic foot-shoe system function from use of shoes, researchers and clinicians should be mindful that this variable could potentially mask biomechanical outcome differences between different foot designs.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported, in part, by a Career Development Award (Award #1IK2RX001322-01A1) from the US Department of Veterans Affairs Rehabilitation Research and Development Service. The contents do not represent the views of the US Department of Veterans Affairs or the US Government.