
Abstract
Background:
The anatomical foot–ankle complex facilitates advancement of the stance limb through foot rockers and late-stance power generation during walking, but this mechanism is altered for persons with bilateral transtibial amputation when using passive prostheses.
Objectives:
To study the effects of bilateral foot and ankle immobilization on able-bodied gait to serve as a model for understanding gait of persons with bilateral transtibial amputation and associated compensatory mechanisms.
Study design:
Comparative analysis.
Methods:
Nine able-bodied persons walked at self-selected slow, normal, and fast speeds. They performed trials unaltered and when fitted with bilateral foot and ankle–immobilizing casts. Data from 10 individuals with bilateral transtibial amputation walking at self-selected fast speeds were used for qualitative comparison.
Results:
The average speeds for the able-bodied fast speed cast and normal speed no-cast trials were similar and were compared with bilateral transtibial amputation data. The able-bodied cast condition data more closely matched bilateral transtibial amputation data than the no-cast data. Ankle range-of-motion and power generation at pre-swing in the cast condition were markedly decreased, while trunk lateral flexion and transverse rotation range-of-motion and peak hip power generation increased.
Conclusion:
Results suggest that the absence of active ankle range-of-motion and power generation contributes to the development of characteristic compensatory gait mechanisms displayed by persons with bilateral transtibial amputation.
Clinical relevance
This study helps to improve understanding of compensatory mechanisms resulting from reduced foot and ankle joint motion to inform lower limb prosthesis design and function for improving gait quality of individuals with bilateral transtibial amputation.
Keywords
Background
Two critical functions of the foot–ankle complex during walking are to facilitate advancement of the stance limb through heel, ankle, and forefoot rockers 1 and generate power during pre-swing to facilitate forward propulsion of the body. 2 These functions are altered or diminished for persons with bilateral transtibial amputation (BTA) who walk with passive prosthetic foot–ankle mechanisms. 3 Individuals with BTA display notable differences in gait dynamics compared to able-bodied (AB) ambulation.3,4 For example, compared to AB ambulators, bilateral transtibial prosthesis users walk at slower self-selected speeds with relatively shorter step lengths and greater step widths. 3 Gait profiles of individuals with BTA exhibit altered kinematics of the hip, knee, and ankle joints when compared to AB gait. They have been observed to have reduced ankle dorsiflexion and knee flexion in stance phase and greater hip range-of-motion (ROM). 3 Possibly resulting from a lack of active ankle motion associated with passive prosthetic feet, persons with BTA employ compensatory mechanisms at the trunk (i.e. exaggerated lateral trunk flexion) to maintain forward ambulation despite these dynamics potentially reducing gait stability at faster walking speeds. 4
The causal factors of the compensatory gait dynamics utilized by persons with BTA are not fully understood. However, as compensatory dynamics are likely responsible for the reported increase in metabolic cost of gait and impaired dynamic balance compared to AB individuals,3,4,5,6,7 improved understanding could inform interventions for improved functional mobility of persons with BTA. One method for enhancing our understanding of pathological gait and overcoming the challenges of recruiting and testing patient groups is to observe the effects of systematically manipulating physiological gait mechanisms in AB persons. For example, Stefanyshyn et al. studied an AB subject walking with an ankle–foot orthosis with added prosthetic componentry to mimic unilateral transtibial amputee gait to better understand those factors that are responsible for gait compensations in this patient group. 8 Accordingly, given the function of passive prosthetic feet, limiting the active ankle contributions in AB ambulators seems to be a reasonable model to better understand gait of persons with BTA and associated compensatory mechanisms.
Studies have investigated the effects of ankle immobilization on AB gait, either full or partial (i.e. limiting joint ROM), and on the metabolic cost of walking, and they collectively report that immobilization generates an increase in energy expenditure.9,10 These studies suggest that active ankle motion aids in minimization of metabolic cost, which has implications for bilateral transtibial prosthesis users due to the passive nature of common prostheses. Persons with BTA walking with passive prosthetic foot–ankle components are not able to generate any active ankle motion, so ankle push-off power is absent. Some ankle push-off power may be observed in quantitative gait analyses performed on prosthesis users, but this represents the return of energy that has been stored in the elastic structures of the passive foot keel and ankle unit. There is some indication that metabolic cost when walking with ankle immobilization can be minimized through addition of a close-to-anatomical rollover shape,11,12 and such rollover shapes can be achieved with passive prosthetic feet. However, the gait of persons with BTA is primarily characterized by reduced ankle motion and increased metabolic cost. As the contribution of a lack of active ankle motion to a less efficient gait in persons with BTA is not well understood, these studies lend confidence that limiting active ankle motion may be a suitable model for studying the characteristic compensatory mechanisms displayed by this patient group.
Given the promising results of previous ankle immobilization studies and the need to address recruitment challenges for study designs that aid understanding of amputee gait, the purpose of this study was to determine the effects of bilateral foot and ankle immobilization on AB gait kinematics and kinetics. This study aimed to identify whether foot and ankle immobilization generates altered gait dynamics that approach those of persons with BTA and hence serve as a model for understanding associated compensatory mechanisms when ankle motion and power generation are greatly reduced. We hypothesized that bilateral foot and ankle immobilization of AB individuals would require compensatory mechanisms that resemble those observed in gait of persons with BTA, such as increased hip power, reduced late-stance ankle power, and exaggerated upper body dynamics. Understanding the resulting compensatory motions may help inform lower limb prosthesis designs for improving the gait quality of persons with BTA and identifying some of the current limitations of passive prosthetic technology.
Methods
Subjects
Healthy AB adults without any reported or detectable walking pathology and able to walk a 10-m distance without undue fatigue were recruited for this study. Ethical approval for this study was granted by the Northwestern University Institutional Review Board. Speed-matched kinematic and kinetic data from 10 participants with BTA (50 ± 18 years, 1.73 ± 0.08 m, 82 ± 16 kg) walking with rigid pylons and Seattle Lightfoot II prosthetic feet (Seattle Systems, Poulsbo, WA, USA) from a previous study3,4 were used to qualitatively compare against the cast and no-cast conditions.
Data collection and analysis
Participants visited the motion analysis laboratory for a single testing session. Prior to testing, participants provided informed consent, followed by measurement of height and body mass. The subjects’ legs were first cast from immediately distal to the knee joint to the toes with Delta-Lite Fiberglass Cast Tape (BSN Medical Ltd., Brierfield, England). The knee joints were able to rotate freely. As the subject was seated, the foot and shank were cast with the foot flat on the ground and the shank aligned vertically, with the goal of achieving neutral, constrained positions of the multiple joints in the foot and ankle. The mass of each cast was estimated to be approximately 400–750 g. Rubber tread and extra padding were glued to the plantar surface of the casts to prevent slipping while walking. A modified Helen Hayes marker set 4 was applied to the subjects and they were instructed to walk at three self-selected walking speeds (normal, slow, and fast in that sequence) along a 10-m walkway. Marker positions were measured with an eight-camera motion capture system (Motion Analysis Corporation (MAC), Santa Rosa, CA, USA), and ground reaction forces (GRFs) were measured with six force plates (Advanced Mechanical Technology, Inc., Watertown, MA, USA) embedded in the walkway. Motion and force data were collected at a sampling rate of 120 and 960 Hz, respectively, with motion data bi-directionally low-pass filtered using a Butterworth filter with 6 Hz cut-off frequency. Subjects walked back and forth along the walkway until five clean force plate strikes in which only one foot was within the border of a single force plate were recorded for both legs. The casts on both sides were then removed and the gait analysis procedure was repeated to collect control (no cast) data. For the no-cast walking condition, subjects wore lightweight gym shoes. OrthoTrac software (MAC) was used to estimate joint angles, moments, and power (via inverse dynamics), as well as gait temporal–spatial data.
Statistical analyses using SPSS (IBM, Armonk, NY, USA) compared quantitative gait data collected while subjects walked with and without ankle casts to identify main effect differences of cast condition. The statistical analyses utilized the Shapiro–Wilk test to confirm data normality and paired t-tests for comparison of conditions. The critical alpha was set at 0.05.
Results
Nine AB individuals participated in this study (27 ± 3 years, 1.75 ± 0.10 m, 76 ± 17 kg). The mean values for speed-matched data of temporal–spatial, kinematic, and kinetic parameters are displayed in Table 1, along with between-condition statistical results from t-tests. Participants displayed right–left symmetry for both conditions, so it was decided to use only right-side data for analysis. The normal self-selected walking speeds with and without ankle casts were 1.02 ± 0.18 m/s and 1.39 ± 0.12 m/s, respectively. However, the average walking speeds for the two conditions were comparable when the subjects walked at their fast speed with ankle casts (1.38 ± 0.25 m/s) and at their normal speed without casts (Table 1). Therefore, these two conditions were used for speed-matched comparisons of the gait data. This selection of data also facilitated qualitative comparison with the BTA data in which subjects walked at 1.3 ± 0.3 m/s.3,4
Speed-matched temporal–spatial, kinematic, and kinetic parameters for both cast conditions.
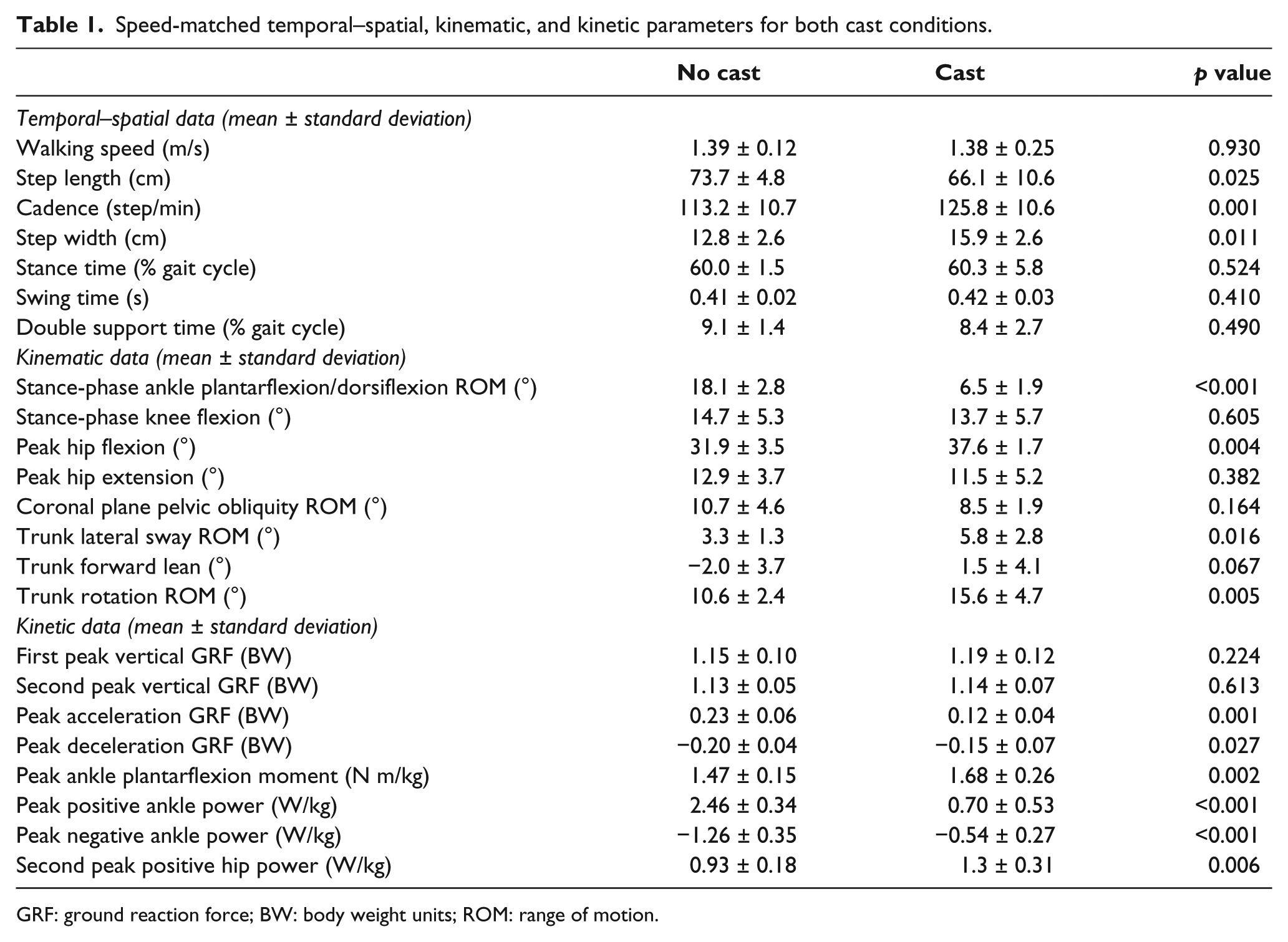
GRF: ground reaction force; BW: body weight units; ROM: range of motion.
Between cast conditions, subjects generally displayed significantly shorter step lengths, higher cadence, and wider step widths when walking with casts (Table 1). Ankle ROM during stance phase was greatly reduced in the cast condition, as expected (Table 1, Figure 1(a)). Peak knee flexion during stance was not significantly affected (Table 1, Figure 1(b)), but peak hip flexion increased marginally in the cast condition (Table 1, Figure 1(c)). Hip hiking—an increased elevation of the pelvis on the swing leg side—was also observed (Figure 2), but there was no significant difference in pelvic obliquity ROM (Table 1).
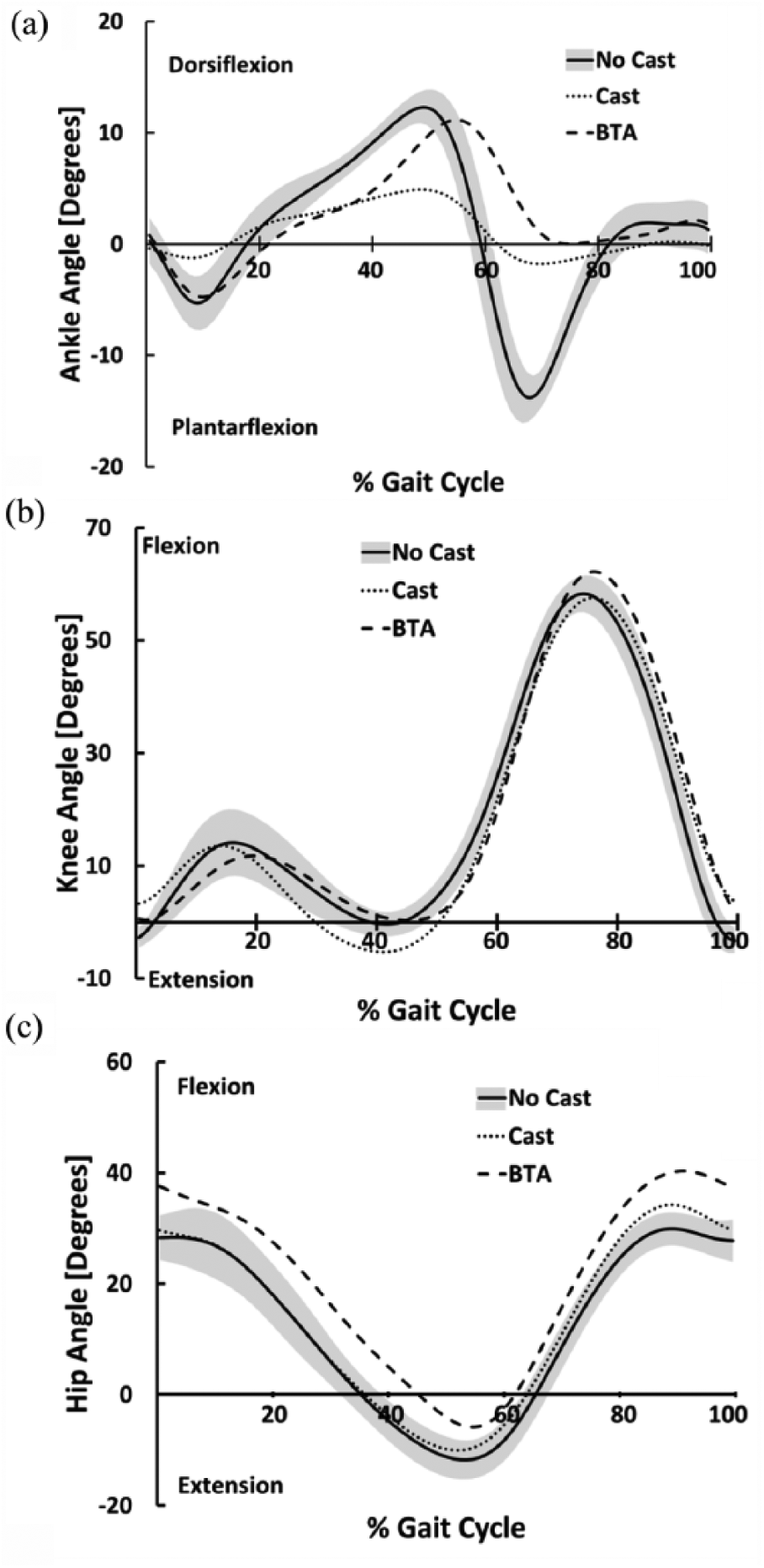
(a) Ankle, (b) knee, and (c) hip angle range-of-motion during the gait cycle for cast conditions and persons with bilateral transtibial amputation (BTA) walking at comparable speeds. The gray band indicates the standard deviation for the AB (no cast) condition.
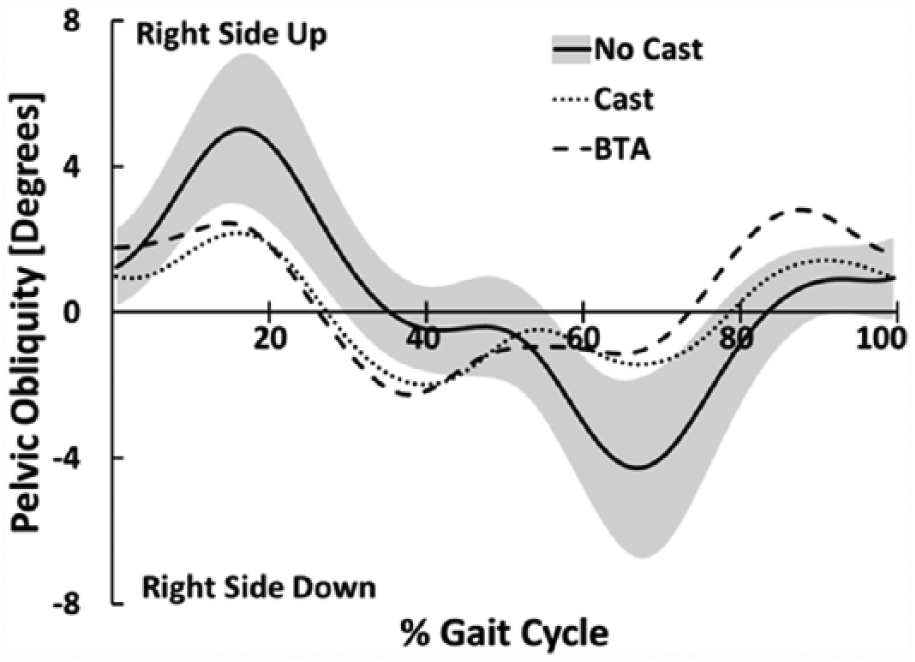
Pelvic obliquity during the gait cycle for cast conditions and persons with bilateral transtibial amputation (BTA) walking at comparable speeds. The gray band indicates the standard deviation for the AB (no cast) condition.
Regarding trunk dynamics, participants displayed an increase in average forward trunk lean and significant increases in trunk lateral sway ROM and trunk rotation ROM during the cast condition compared to the no-cast condition (Table 1, Figure 3).
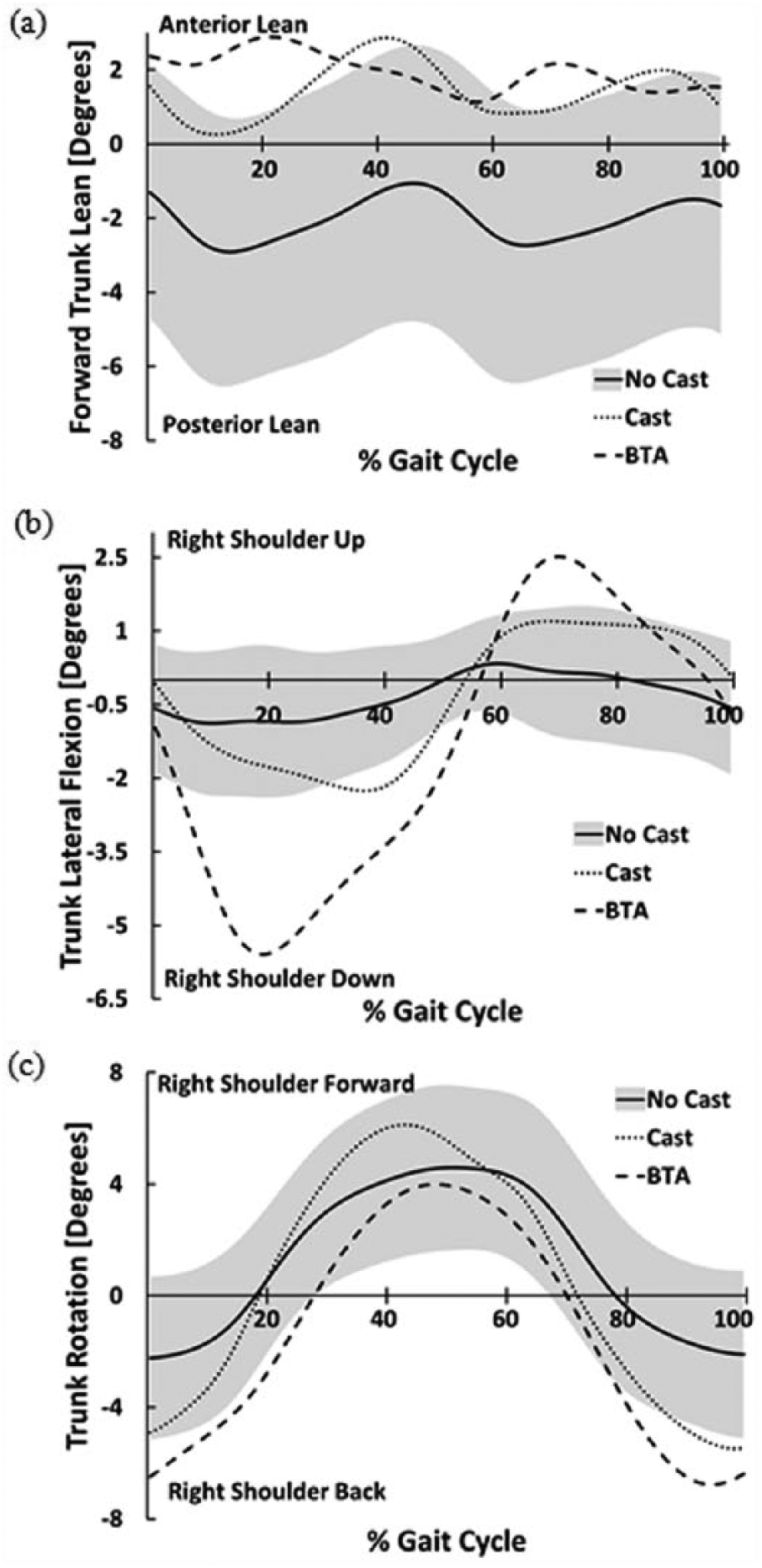
Trunk range-of-motion as (a) forward lean, (b) lateral flexion, and (c) transverse rotation during the gait cycle for cast conditions and persons with bilateral transtibial amputation (BTA) walking at comparable speeds. The gray band indicates the standard deviation for the AB (no cast) condition.
The vertical GRFs were comparable between the two conditions (Table 1, Figure 4), but the peak fore-aft (acceleration and deceleration) GRFs were significantly reduced for the cast condition. The peak ankle plantarflexion moment was significantly increased for the cast condition compared to the no-cast condition (Table 1). The peak ankle power generation and absorption during stance were greatly reduced in the cast condition (Table 1, Figure 5(a)). The second peak hip power generation during pre-swing increased in the cast condition (Table 1, Figure 5(b)).
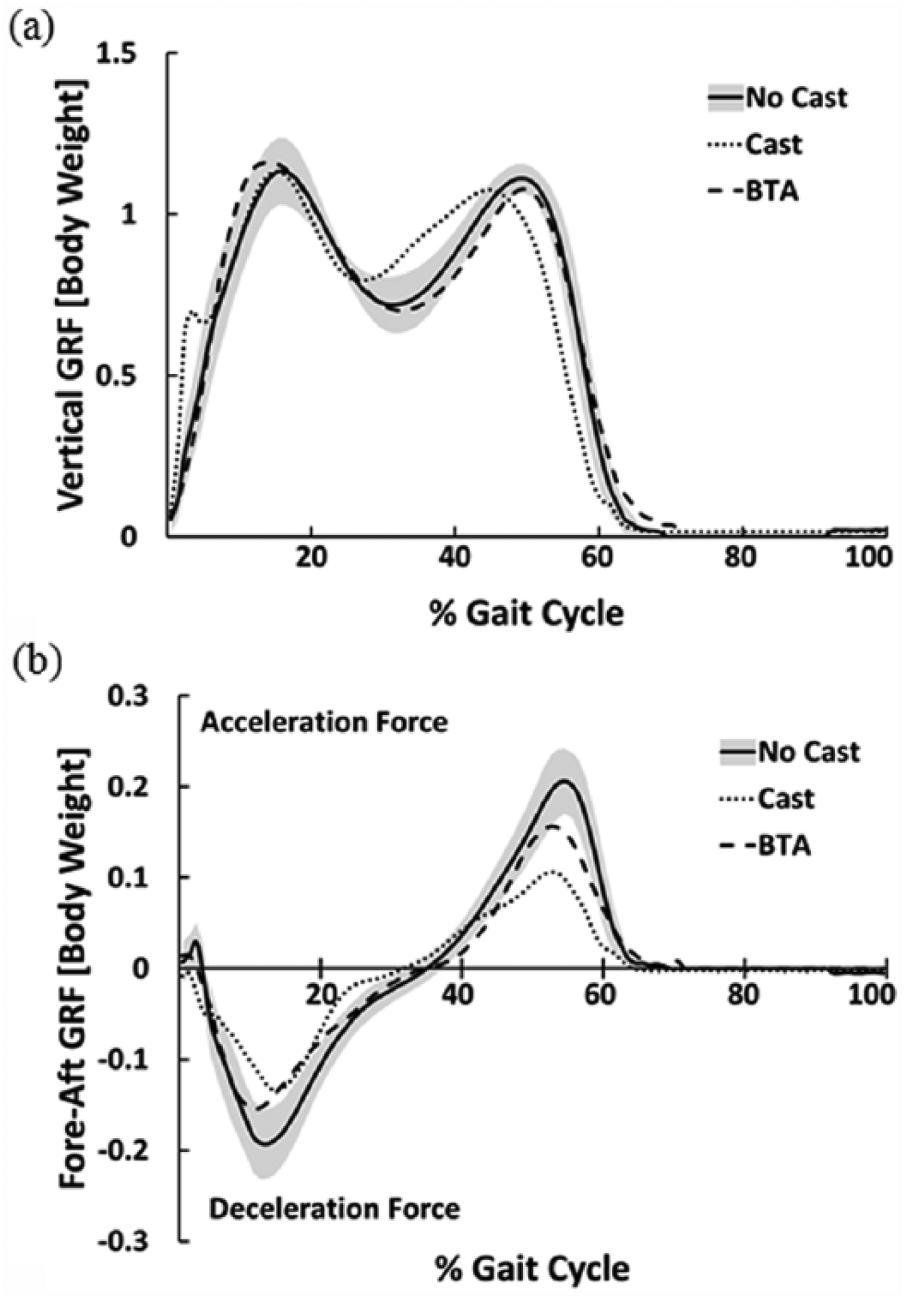
Ground reaction forces (GRFs) with respect to the body weight in the (a) vertical and (b) fore-aft directions during the gait cycle for cast conditions and persons with bilateral transtibial amputation (BTA) walking at comparable speeds. The gray band indicates the standard deviation for the AB (no cast) condition.
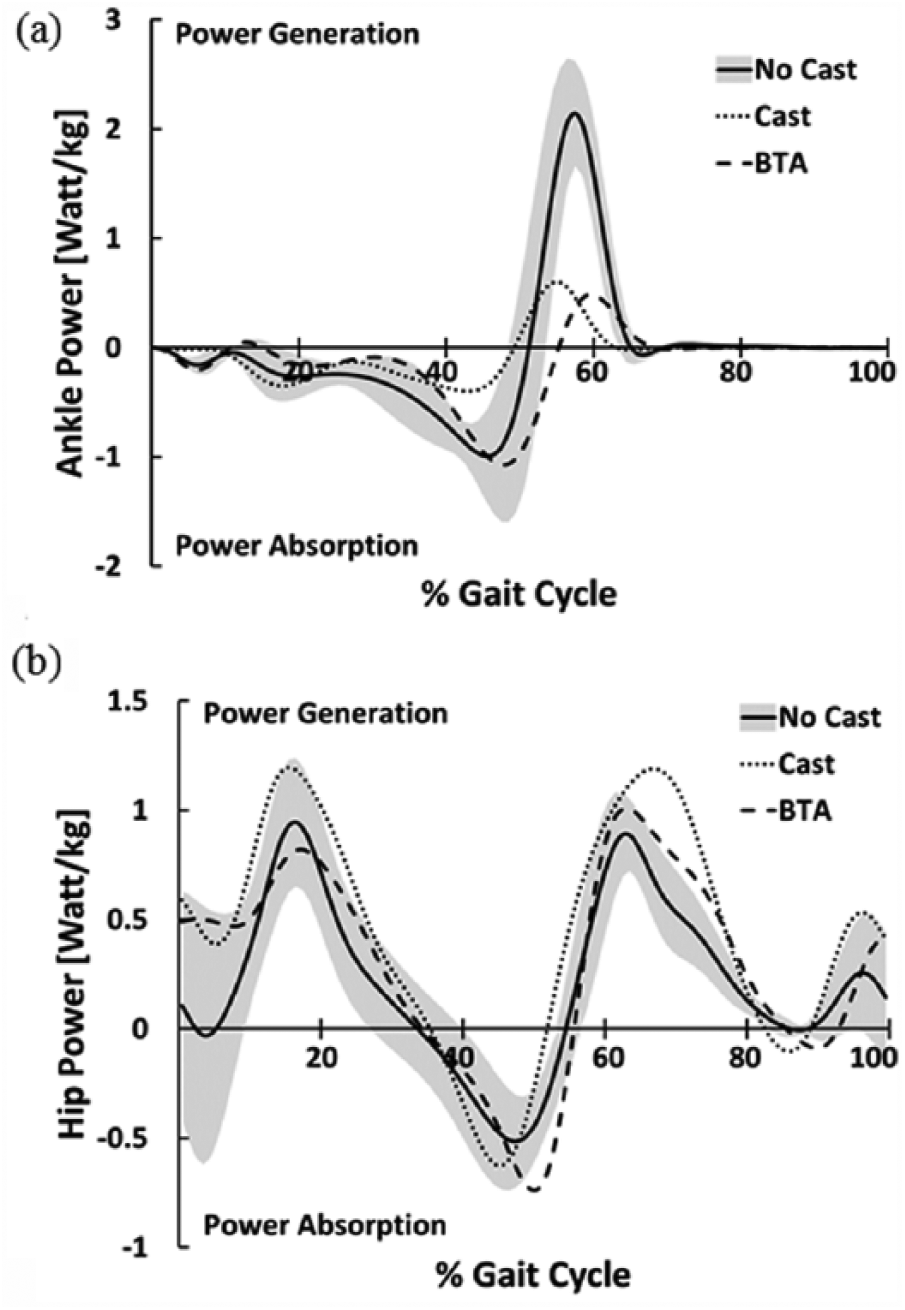
Power of the (a) ankle and (b) hip joint during the gait cycle for cast conditions and persons with bilateral transtibial amputation (BTA) walking at comparable speeds. The gray band indicates the standard deviation for the AB (no cast) condition.
Discussion
The purpose of this study was to determine the effects of immobilizing the foot and ankle joints in AB individuals to determine whether gait dynamics differed from normal walking and approached those of persons with BTA. It was anticipated that the cast condition would impose the same functional limitations as those faced by persons with BTA walking with passive prostheses and would yield similar gait dynamics as seen in previous studies 4 with gait differences observed between AB persons and those with BTA. 3 In most cases, the cast conditions appeared to follow these trends accordingly and generally support the hypothesis that foot and ankle immobilization in AB individuals may be a good model for gait of persons with BTA.
Ankle ROM for the cast condition was greatly reduced, but not completely eliminated, compared to the no-cast condition (Figure 1(a)). Specifically, the cast condition still permitted approximately 6.5 ± 1.9° ankle ROM (Table 1), primarily attributable to dorsiflexion during stance phase (approximately 5°). The prostheses of the BTA subjects in the previous study 3 allowed some bending of the keel in mid- to late stance and thus simulated ankle dorsiflexion near 10°. Consequently, the limitations for the cast condition may have caused even greater difficulty in walking compared to persons with BTA due to a more rigid ankle and foot complex, altering the rocker mechanisms of the foot and ankle which contribute to forward progression of the body center-of-mass. 1
Pelvic obliquity in normal gait assists in shock absorption as load is rapidly transferred from the trailing to the leading leg.1,13 For the cast condition, the pattern of pelvic obliquity was substantially altered and the ROM slightly reduced. Although not statistically significant in this study, a reduction in pelvic obliquity ROM has been previously observed in persons with BTA, 3 lending validity to our results. Hip hiking was exhibited during the swing phase for the cast condition (Figure 2(a)), which is consistent with the BTA data.3,4 Hip hiking is typically utilized in impaired gait to facilitate toe clearance during swing phase, which may be necessary due to the limitations to active dorsiflexion of the ankle. 13
Although not reaching significance, subjects exhibited anterior trunk lean during the cast condition, while posterior for the no-cast condition (Figure 3(a)), which appears to agree with BTA data. 4 The increased forward trunk lean for the cast condition may have been used to substitute for lack of tibial progression during stance, as may be the case when foot and ankle motions are reduced or absent. This enables the trunk to assist in forward progression and improve knee stability by shifting the trunk mass further forward. 1 However, this may produce greater metabolic cost by engaging the hip and trunk extensor muscles in order to maintain flexed trunk orientation.14,15 Similarly, the increase in lateral trunk sway ROM for the cast condition, which approached the ROM exhibited by persons with BTA 4 (Figure 3(b)), may assist in transferring trunk mass to the stance limb and facilitate foot clearance.1,3,4 Furthermore, the cast condition reflected the characteristic of gait for persons with BTA of increased transverse plane trunk ROM. 4 Since increased trunk rotation is used to assist progression of the limb, the similarities between the cast condition and BTA data confirm that the foot and ankle are active contributors to the forward progression of the limb. Overall, these results suggest that trunk dynamics may be used as a means to advance the body center-of-mass when active foot and ankle motion are limited.
The vertical GRFs for each condition were unchanged except for a small heel strike transient in the cast condition at initial contact (Figure 4(a)). This heel strike transient was likely caused by increased rigidity of the heel pad due to the cast materials, increasing the stiffness while reducing the ability to provide shock absorption. The peak fore-aft GRFs for the cast condition were significantly decreased compared to the no-cast condition (Table 1) and converged on the BTA data (Figure 4(b)). This result aligns with comparison of fore-aft GRF data from AB persons and bilateral transtibial prosthesis users of peripheral vascular disease and traumatic etiology 16 and may be directly attributable to the relatively shorter step lengths adopted by subjects walking with casts given the positive relationship between step length and peak fore-aft forces. 17 Finally, we observed a higher peak ankle plantarflexion moment for the cast condition compared to the no-cast condition (Table 1), which is probably due to a larger anterior progression of the center of pressure under the foot due to the stiffer foot and ankle condition imposed by the casts.
Ankle power generation was substantially reduced for the cast condition compared to the no-cast condition (Table 1), which agrees with previous work that reported significantly decreased ankle power generation in gait of persons with BTA compared to AB gait. 3 This result is likely due to the lack of active ankle plantarflexion that limits the ability to generate push-off during pre-swing (Figure 5(a)). Ankle power absorption was also greatly reduced for the cast condition (Table 1), while persons with BTA demonstrated absorption very similar to the no-cast condition which may have been due to the passive nature of the prosthetic foot. Additionally, the second peak hip power generation for the cast condition was significantly greater than the no-cast condition (Table 1), and this is likely a substitution for the lack of ankle power generation to provide pre-swing push-off. Similarly, persons with BTA also demonstrate significantly greater peak hip powers than AB subjects. 3
Given the results from this investigation, it appears that bilateral foot and ankle immobilization through fiberglass casting may be a suitable model for further investigating the gait of persons with BTA. By understanding the development of compensatory mechanisms resulting from reduced active ankle joint motion, we can better inform prosthetic and therapeutic interventions to improve gait quality of persons with BTA. For example, follow-up studies may involve systematic investigations on methods to modify movement patterns or provide supplemental push-off to aid in forward propulsion while minimizing metabolic cost and/or maximizing stability. Importantly, these results suggest that the gait patterns observed in the AB individuals walking with bilateral ankle casts may represent optimal gait for BTAs walking with passive prosthetic components. Therefore, it may not be reasonable to expect BTAs to walk with an AB-type gait pattern. However, with the development of prosthetic components that provide active ankle power generation, the gait characteristics of persons with BTAs may further approach AB patterns.
There are several limitations to this study. First of all, subjects had limited time to practice walking following foot and ankle casting. There was some concern that extended walking in the rigid, unpadded casts may have led to discomfort and produced further gait alterations. Thus, the subjects only practiced walking in the casts for a few minutes before the gait analyses were performed. Future studies should consider providing more but still reasonable accommodation time. Second, the foot and ankle joints were not rigidly constrained by the casts. Ankle motion was greatly reduced for the cast condition compared to unimpeded gait, but there was some motion in the order of about 7° on average. Similarly, there was some bending of the foot keel during stance phase. This small amount of foot and ankle motion was likely beneficial during walking, contributing to a smaller and more desirable rollover shape radius than could be achieved with a completely rigid foot and ankle without a rocker sole. 18 Nonetheless, the ankle ROM for the cast condition was substantially smaller than that observed in the subjects with BTA from the previous study. Third, it is not possible to identify direct causality, whereas although the immobilization of the joints of the foot and ankle produced a gait similar to that of persons with BTA, the factors which generated these dynamics are not confirmed. Finally, given the purpose of this study to identify whether AB dynamics that broadly characterize gait were distinct between foot–ankle casting and unimpeded walking, and hence could serve as a model for BTA gait, a critical alpha correction factor was not used to account for Type I error and this should be considered when interpreting results.
Conclusion
Reduced foot and ankle motion due to bilateral casting was found to greatly alter the gait characteristics of AB subjects such that they resembled those found in gait of persons with BTA due to limitations in the design of passive prosthetic foot–ankle components. Particularly, the loss of ankle power generation and the notable increase in hip power generation to compensate for this loss were relevant for both the cast condition and BTA gaits. Compensatory movements of the pelvis and trunk observed during the cast condition also closely matched those of persons with BTA and are probably utilized to facilitate forward progression. These results suggest that the absence of active ankle motion and power generation contribute to the development of compensatory mechanisms observed in characteristic gait patterns of persons with BTA with passive prosthetic feet. Further studies of AB subjects that systematically manipulate other degrees of freedom may better inform us of deficiencies in passive prosthetic components that require the necessity to adopt compensatory motions while walking.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.