
Abstract
Background: Microprocessor controlled prosthetic knees (MPK) offer opportunities for improved walking stability and function, but some devices’ swing phase features may exceed needs of users with invariable cadence. One MPK offers computerized control of only stance (C-Leg Compact).
Objective: To assess Medicare Functional Classification Level K2 walkers’ ramp negotiation performance, function and balance while using a non-MPK (NMPK) compared to the C-Leg Compact.
Study Design: Crossover.
Methods: Gait while ascending and descending a ramp (stride characteristics, kinematics, electromyography) and function were assessed in participant’s existing NMPK and again in the C-Leg Compact following accommodation.
Results: Ramp ascent and descent were markedly faster in the C-Leg Compact compared to the NMPK (p ≤ 0.006), owing to increases in stride length (p ≤ 0.020) and cadence (p ≤ 0.020). Residual limb peak knee flexion and ankle dorsiflexion were significantly greater (12.9° and 4.9° more, respectively) during single limb support while using the C-Leg Compact to descend ramps. Electromyography (mean, peak) did not differ significantly between prosthesis. Function improved in the C-Leg Compact as evidenced by a significantly faster Timed Up and Go and higher functional questionnaire scores.
Conclusions: Transfemoral K2 walkers exhibited significantly improved function and balance while using the stance-phase only MPK compared to their traditional NMPK.
Instability, reduced function and falls are common in deconditioned transfemoral amputees. Selection and use of prosthetic componentry that promotes greater stability in more challenging environments is essential to improve the safety, function, quality of life and independence of individuals functioning at the K2 walking level.
Keywords
Background
Walking in the community presents numerous challenges for individuals with a transfemoral amputation, particularly when the environment includes ramps, curb cutouts and hills. Stance phase knee stability is most threatened when the surface slopes downward as the knee’s normal response is to flex as the limb is loaded.1,2 Lacking vastii to eccentrically control the knee and kinesthetic feedback for precise awareness of knee and ankle alignment, individuals must rely on transfemoral prosthetic design features, compensatory gait adjustments (e.g. reduced residual limb knee flexion during stance), 3 and the remaining hip musculature to ensure stability. However, the residual limb’s hip muscles are often compromised by the amputation. 4 Thus the intact limb’s muscles also must adjust to the needs of prosthetic gait. 5
While modern prosthetic designs that incorporate microprocessors have made major strides in replacing the deficits imposed by a transfemoral amputation, gait stability remains elusive to many users of traditional non-microprocessor controlled knee (NMPK) prostheses.6-11 Few older or deconditioned adults have sufficient strength, keenness of proprioception or the motor control acuity required to avoid falls when the NMPK prosthetic knee fails to reach the full extension required for stance stability. This capacity can be further compromised by the impact of diabetes mellitus (a frequent precursor to lower limb amputations) on the motor, sensory and visual systems.12,13
Microprocessor-controlled knee (MPK) prostheses can notably improve walking characteristics, stability and efficiency compared to NMPK prostheses6-11,14; however, some design features may exceed deconditioned users’ initial needs. For example, the C-Leg (Otto Bock HealthCare North American Headquarters, Minneapolis, MN) includes a sensor network that measures the ankle moment as well as the knee joint’s angle and angular velocity 50 times/second. The data are used to identify gait cycle phasing and adjust hydraulic cylinders to the user’s needs for stability and mobility, even when changing walking speeds. While the improved stance stability and efficiency would be particularly beneficial for adults with weakness and those at risk for injurious falls, some insurers have suggested that the system’s added swing phase capabilities may surpass the needs of those expected to maintain a relatively constant walking speed (e.g. Medicare Functional Classification Level (MFCL) K2 walkers). However, it is possible that some deconditioned transfemoral prosthesis users might benefit sufficiently from the added stance stability so that they are ultimately able to walk faster and at varying speeds.
The C-Leg Compact (Otto Bock HealthCare North American Headquarters, Minneapolis, MN) MPK prosthesis was introduced in 2002 to address the needs of deconditioned K2 level walkers. In contrast to controlling knee hydraulics mechatronically during both stance and swing, the C-Leg Compact’s sensor network modulates only stance mechanics. Swing is controlled hydraulically. This hybrid MPK prosthesis is designed for individuals expected to benefit from added stance phase knee stability, but whose invariable cadence limits need for sophisticated swing control.
To better understand the impact of the C-Leg Compact on function, this study compared K2 level ambulators’ gait mechanics and stability during ramp negotiation using a traditional NMPK prosthesis versus a C-Leg Compact prosthesis, and quantified differences in users’ locomotor function and perceptions of function/balance. We hypothesized that compared to the NMPK, usage of the C-Leg Compact during ramp negotiation would result in 1) improved stride characteristics (e.g. faster velocity, longer stride length); 2) greater knee flexion in weight acceptance and single limb support, and a more optimal trailing limb posture during the latter half of single limb support (i.e. greater extension of the thigh relative to vertical) to enable a longer step length; and 3) reduced muscle effort (electromyography (EMG)) in key lower limb stabilizers. We also hypothesized that general locomotor function and participant’s perceptions of confidence, balance and stability would be greater when using the C-Leg Compact compared to the NMPK. Empirical data from this research is expected to guide clinical decision making regarding prosthetic componentry selection to improve K2 level ambulators’ function, safety, independence, and quality of life.
Methods
Participants
Current users of articulating NMPK were recruited from prosthetic clinics and support groups in the local area. Only those classified as no greater than K2 level ambulators by a certified prosthetist were recruited. The MFCL K2 classification indicates that individuals have the ability to ambulate slowly with a prosthesis, but only limited capacity/potential to modify their walking speed or traverse low-level environmental barriers (e.g. curbs, stairs or uneven surfaces).
Five men and five women with unilateral transfemoral amputations comprised the study group (mean age 62 ± 11.3 years; mean height 1.701 ± 0.114 m; mean mass 68.7 ± 11.4 kg; mean time since amputation 9 years and range 2.5 to 21 years). All were over 21 years of age, free from skin ulceration and ambulated independently. Seven used upper extremity assistive devices (e.g. a cane or walker) while ambulating. The remaining three did not use an upper extremity assistive device. Six had experienced unilateral amputations of the left lower extremity and the remaining four had amputations of the right lower extremity. Additional criteria included sufficient vision to complete the walking tasks, and absence of secondary neurologic or orthopaedic conditions that would physically or cognitively limit participation. Each participant signed the HIPAA protection of health information form and an informed consent form approved by the Institutional Review Board at Rancho Los Amigos National Rehabilitation Center (RLANRC).
Procedures
All testing was conducted at RLANRC’s Pathokinesiology Laboratory (Downey, CA). Instrumented gait analysis and functional assessments were first conducted in the optimally aligned NMPK, and then again in the C-Leg Compact prosthesis after a training and accommodation period.
NMPK adjustment and training
Prior to quantified assessment of function in the NMPK, each participant met with a certified prosthetist to ensure proper fit and alignment of the device, including adjusting the socket as necessary to ensure optimal fit. Then each individual met with a physical therapist for a one-hour functional training ‘refresher session’ to review techniques on how to safely ascend and descend ramps and stairs.
Initial biomechanical assessment while using the NMPK
Quantified gait analysis was performed as each participant ascended and descended a 6.1 m ramp (12° slope, 1 m wide, 0.05 m curb on edges) at their self-selected speed using their NMPK and customary upper extremity assistive devices. Key prosthetic and assistive device features are provided in Table 1. Simultaneous recordings were made of foot-floor contact patterns, lower extremity kinematics, and EMG activity. A minimum of two ramp ascent and two ramp descent trials were recorded for subsequent analysis.
Select prosthetic componentry characteristics for the non-microprocessor controlled knee (NMPK) and the C-Leg Compact microprocessor controlled knee prosthesis.
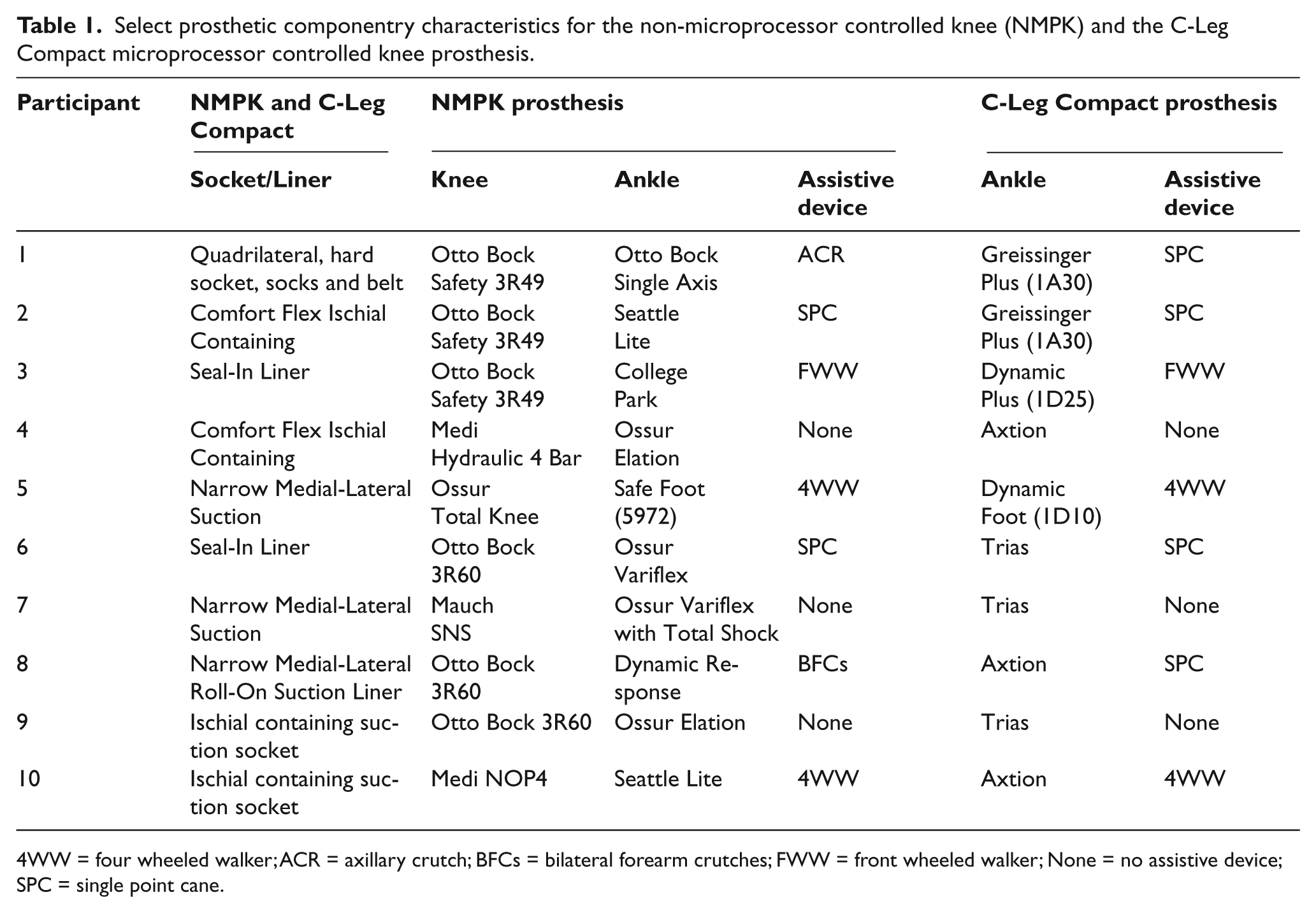
4WW = four wheeled walker; ACR = axillary crutch; BFCs = bilateral forearm crutches; FWW = front wheeled walker; None = no assistive device; SPC = single point cane.
A Stride Analyzer (B & L Engineering,Tustin, CA) measured foot-floor contact patterns to calculate stride characteristics and delineate EMG phasing. This system included a pair of insoles containing compression closing switches in the heel, first and fifth metatarsals, and great toe regions. Insoles were taped to the bottom of each shoe. FM-FM telemetry (Biosentry Telemetry Inc., St,Torrance, CA) transmitted signals from the Stride Analyzer package to a DEC 11/23 computer (Digital Equipment Corporation, Cambridge, MA).
A VICON motion analysis system (Vicon Motion Systems, Oxford, UK) defined three-dimensional motion of the lower limbs and pelvis. This system included six charge-coupled cameras with strobed infrared light-emitting diodes. 15 Fourteen retro-reflective markers (17 mm diameter) were taped onto skin overlying bony landmarks including the midline sacrum at the level of the posterior iliac spines, anterior superior iliac spine (bilaterally), greater trochanter, anterior thigh, medial and lateral femoral condyles, anterior tibia, medial and lateral malleoli, dorsum of the foot, first and fifth metatarsal heads and posterior heel of the intact limb or corresponding landmarks on the prosthesis. 16 Motion data were sampled separately for each lower limb at a rate of 50 Hz, filtered at 6 Hz (using a Butterworth digital filter), and recorded on a DEC PDP 11/23 computer (Digital Equipment Corporation, Cambridge, MA).
Intramuscular EMG was recorded using bipolar wire electrodes (50 µm Ni-Cr alloy wire in a 25-gauge needle) to quantify muscular activity. Fine-wire electrodes were inserted according to Basmajian’s technique 17 into the muscle bellies of the gluteus medius and lower fibers of gluteus maximus of both limbs, iliacus of the residual limb, and vastus intermedius, soleus and tibialis anterior of the intact limb. Electrode placement was confirmed by palpation of the tendon and muscle belly during mild electric stimulation through the inserted wires, and by recording the EMG signal during a five-second maximum voluntary isometric muscle contraction (MVC). EMG signals were transmitted by FM-FM telemetry (Model 2600) to a DEC 11/23 computer, band-pass filtered through an analog filter (150–1,000 Hz) and sampled and digitized at 2,500 Hz. The overall signal gain was 1,000. EMG recorded during a resting trial determined the baseline threshold for each muscle’s myoelectric activity.
Initial functional assessments while using the NMPK
Participants completed the Timed Up and Go Test (TUG) and three standardized questionnaires: the Prosthetic Evaluation Questionnaire (PEQ) mobility subscale, the Activities-Specific Balance Confidence Scale (ABC), and the Houghton Scale. In addition, participants’ anecdotal comments about device usage were noted. The TUG assesses the time taken to rise from a chair, walk 3 m, turn around, walk back to the chair and sit down. 18 The PEQ mobility subscale’s 13 items assess mobility and transfers. 19 A summary score was calculated by adding individual item scores together and then dividing by the number of questions answered. The ABC Scale asks participants to rate their level of confidence between 0 and 100% with performing each of 16 mobility items. 20 Responses were summed and then divided by 16 to provide an overall average balance confidence score. The Houghton Scale contains three questions rating the amount of prosthetic use and type of mobility aid used and three questions rating perceptions of stability while navigating different terrains. 21 A summative Houghton Scale score, ranging from 0 (poor performance) to 12 (maximum performance), was used.
C-Leg Compact fitting, adjustment, training and accommodation
Following a comprehensive biomechanical evaluation in the NMPK, each participant was re-fit by a certified prosthetist with a C-Leg Compact articulating MPK prosthesis. The NMPK’s existing socket and shoe wear were combined with the appropriate C-Leg Compact compatible knee, shank and foot components to reduce the potential confounding influence of socket design on walking ability (Table 1). The socket was re-assessed and modified as necessary to ensure optimal fit. Alignment was optimized by the prosthetist consistent with the manufacturer’s specifications and re-aligned as necessary during subsequent training and accommodation. Static alignment was confirmed using Otto Bock’s Laser Assisted Static Alignment Reference (L.A.S.A.R.TM) posture system (Otto Bock, Duderstadt, Germany). 22
Participants then received training in their C-Leg Compact and a three-month accommodation period prior to the second laboratory testing session. Training consisted of five to seven one-hour sessions with a physical therapist which included education to enhance each participant’s understanding of the capabilities of the prosthesis, and practice on stairs, ramps, curbs and uneven surfaces.
Final biomechanical and functional assessments in the C-Leg Compact
Following training and three months of accommodation, participants were reassessed using their C-Leg Compact. Biomechanical and functional assessment procedures were similar to those previously described except participants wore the C-Leg Compact. At the completion of C-Leg Compact testing, participants selected which prosthesis they preferred to keep.
Data Analysis
Footswitch data were processed using EMG-Stride Analyzer Software (B & L Engineering, CA). Spatio-temporal parameters (e.g. speed, cadence and stride length) were averaged across trials for each ramp condition. Kinematic data were processed with Adtech Motion Analysis Software (Adtech Inc., Honolulu, HI) to produce 3-D trajectories for each marker. The position and orientation of each lower extremity segment were obtained and sagittal plane joint angles for each percent of the gait cycle (% GC) were determined with computer algorithms using Euler embedded coordinates. An ensemble average of all strides (two to eight) for each prosthetic condition was calculated from each participant’s kinematic data. The number of available strides varied across participants and trials because assistive devices (e.g. walkers or canes) sometimes blocked the motion analysis cameras from viewing one or more reflective markers during a stride. Peak values were extracted from each participant’s ensemble averaged motion data for the hip (peak extension in single limb support), knee (peak flexion in weight acceptance and single limb support), and ankle (peak DF in single limb support).
EMG Analyzer Software (B & L Engineering,Tustin, CA)was used to calculate EMG intensity. The relative intensity of EMG (normalized by the MVC value) was calculated for each % GC where the intensity was ≥ 5% of the MVC value. Peak and mean EMG activity were quantified for each participant and condition.
Statistical Analysis
SigmaPlot 11.0 (2011 Systat Software Inc., Chicago, IL) software was used to perform paired t-tests to compare NMPK versus C-Leg Compact values for stride characteristics, peak lower extremity joint motion values, and EMG intensities during each ramp condition. Functional measures also were compared. Statistical significance was set at p = 0.05.
Results
Spatiotemporal characteristics
Ramp ascent was markedly faster (28%) in the C-Leg Compact compared to NMPK, owing to 14% increases in both stride length and cadence (Table 2). A modest but significant lengthening of the % GC spent in residual limb single limb support was documented during ramp ascent using the C-Leg Compact compared to NMPK (4% GC difference between prostheses), despite no significant differences in the residual limb’s stance duration (% GC) or timing of heel off (% GC). The intact limb’s stance duration was significantly briefer in the C-Leg Compact compared to the NMPK (4% GC difference).
Select stride characteristics (
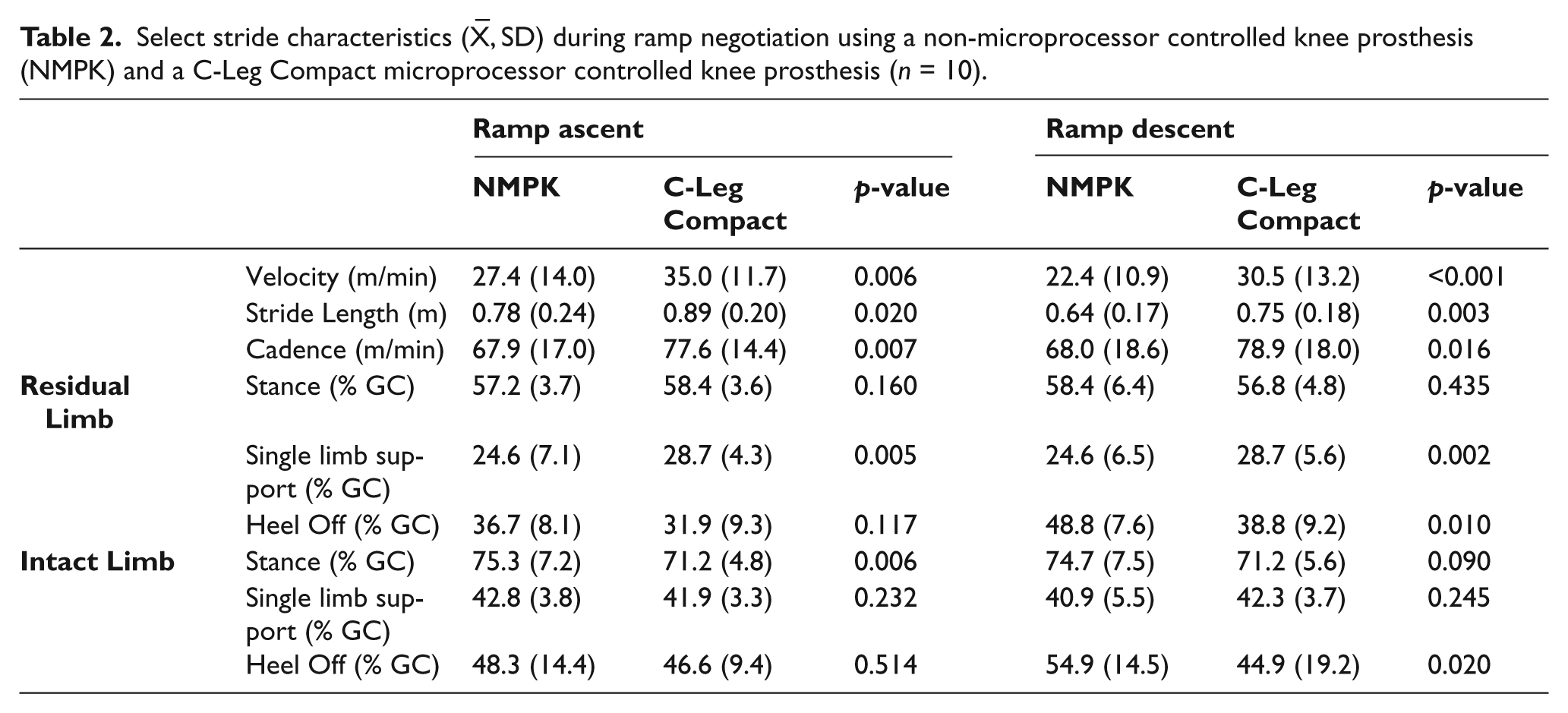
Differences between prosthetic conditions were even more pronounced during ramp descent, with velocity 36% more rapid when using the C-Leg Compact compared to NMPK (Table 2). The faster descent resulted from increases in both stride length (17%) and cadence (16%) while using the C-Leg Compact. The percentage of gait cycle spent in residual limb single limb support was significantly longer when descending in the C-Leg Compact compared to NMPK (4% GC difference), yet the residual limb’s heel off occurred markedly earlier in the gait cycle (10% GC difference). The intact limb’s heel off also occurred earlier in the gait cycle when using the C-Leg Compact (10% GC difference between prosthesis); however, the percentage of time spent in intact limb stance and single limb support did not vary significantly between prosthetic conditions.
Kinematics
The residual limb’s peak angles did not vary significantly between prostheses during ramp ascent despite a trend towards higher values in the C-Leg Compact for single limb support hip extension (5.6° more; p = 0.051), single limb support knee flexion (2.5° greater; p = 0.055), and single limb support ankle dorsiflexion (3.0° higher; p = 0.051) compared to the NMPK (Figure 1). During both prosthetic conditions, the residual limb lacked the characteristic weight acceptance knee flexion wave during ramp ascent. The intact limb displayed significantly greater single limb support peak hip extension (5.0° more) and thigh extension (2.1° more) during ramp ascent in the C-Leg Compact compared to the NMPK. During both prosthetic conditions the intact knee displayed a flexion wave during limb loading.
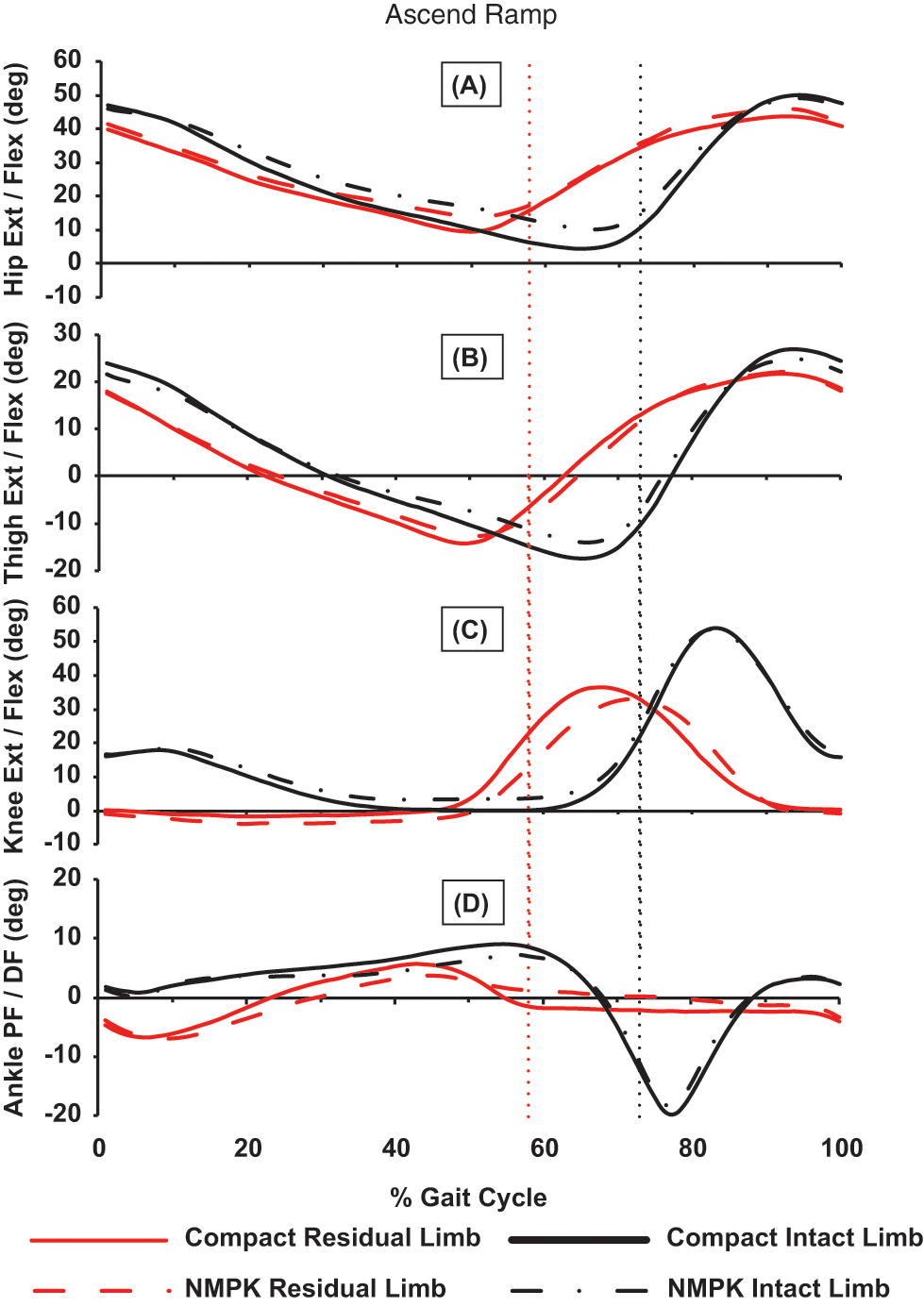
Sagittal-plane mean joint motion (degrees) of the residual and intact limbs’ hip (A), thigh (B), knee (C) and ankle (D) during ramp ascent wearing the non-microprocessor controlled knee (NMPK) and the C-Leg Compact microprocessor-controlled knee prosthesis. No significant between prosthesis differences were identified for the residual limb’s peak hip extension in single limb support, peak knee flexion in weight acceptance or single limb support, and peak ankle DF in single limb support. The intact limb displayed significantly greater single limb support peak hip and thigh extension compared to the NMPK. Although the residual limb lacked the normal knee flexion wave during limb loading for both prosthetic conditions, the intact knee displayed the flexion wave. Dotted vertical line delineates onset of swing for the residual limb (red) and the intact limb (black).
During the single limb support period of ramp descent, residual limb peak knee flexion was significantly greater (12.9° difference) as was ankle dorsiflexion (4.9° more) while using the C-Leg Compact compared to the NMPK (Table 3; Figure 2). The knee also displayed a modest trend towards increased flexion during weight acceptance while using the C-Leg Compact (2.6° difference; p = 0.063). The only significant differences recorded for the intact side were greater single limb support peak hip extension (6.4°) and thigh extension (3.1°) using the C-Leg Compact. The intact limb’s motion profiles otherwise were very similar during ramp descent.
Select lower extremity peak angles (
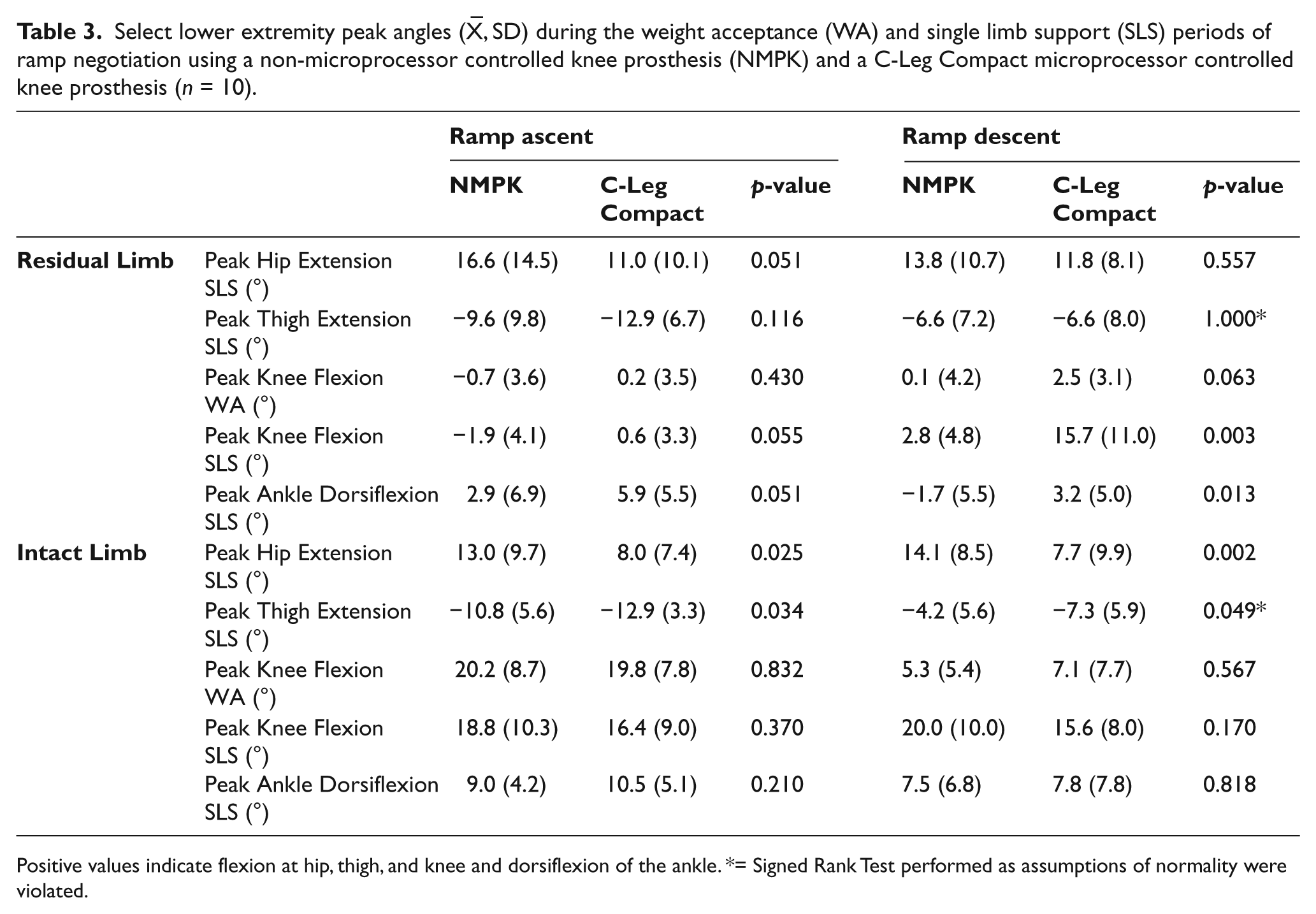
Positive values indicate flexion at hip, thigh, and knee and dorsiflexion of the ankle. *= Signed Rank Test performed as assumptions of normality were violated.
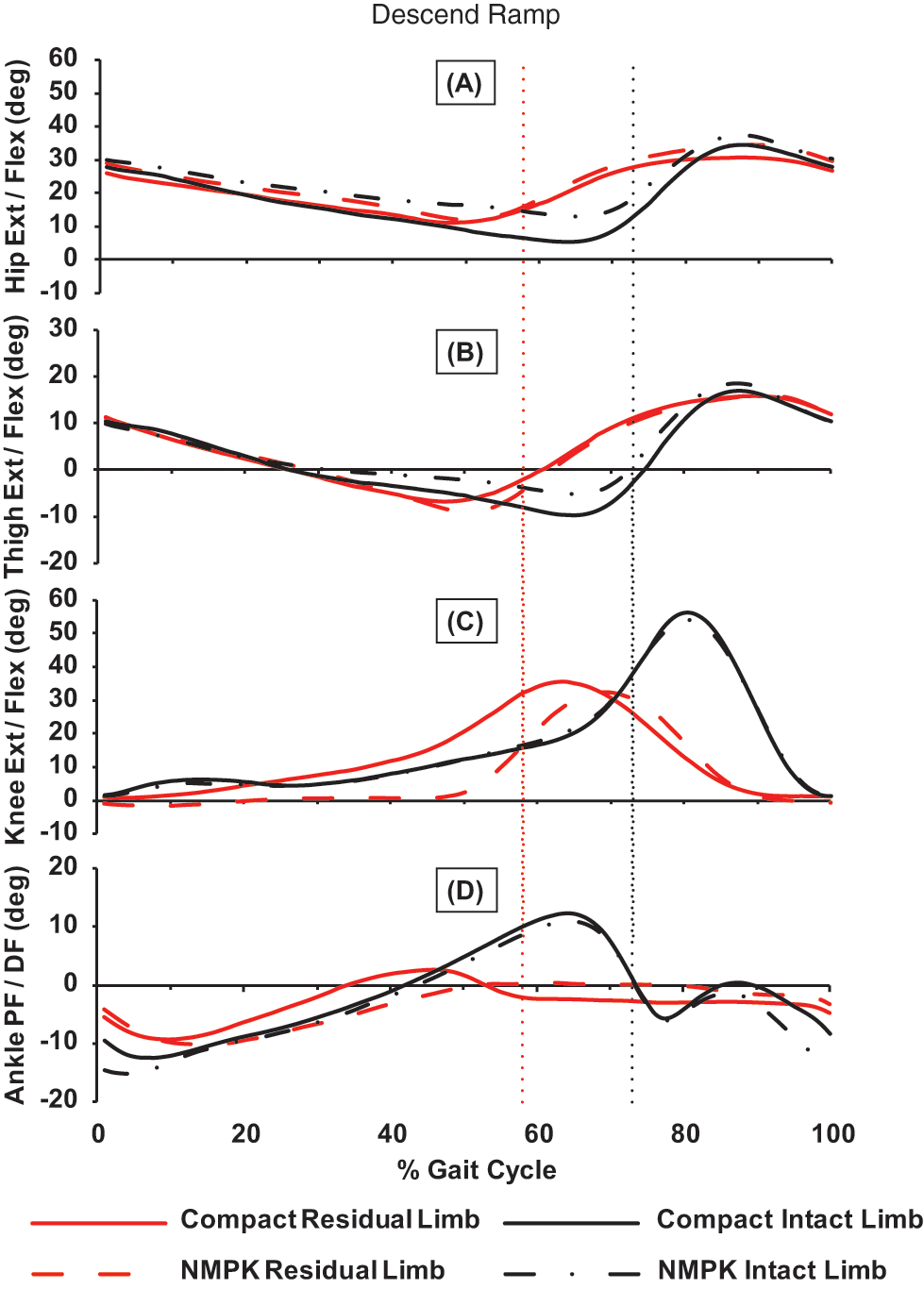
Sagittal-plane mean joint motion (degrees) of the residual and intact limbs’ hip (A), thigh (B), knee (C) and ankle (D) during ramp descent wearing the non-microprocessor controlled knee (NMPK) and the C-Leg Compact microprocessor controlled knee prosthesis. The residual limb’s peak knee flexion and ankle dorsiflexion were significantly greater during single limb support while using the C-Leg Compact compared to the NMPK. During single limb support, the intact limb achieved significantly greater peak hip and thigh extension using the C-Leg Compact compared to the NMPK. Dotted vertical line delineates onset of swing for the residual limb (red) and the intact limb (black).
EMG
Mean and peak EMG values did not differ significantly between the NMPK and C-Leg Compact conditions for the eight muscles studied. Proximity of the prosthetic socket’s brim to fine wire EMG insertion sites interfered with data acquisition for the residual limb’s iliacus and gluteus medius. EMG data for the residual limb’s iliacus were available for only four of the 10 participants during ramp ascent and three of the 10 participants during descent secondary to insertions pulling out prior/during the ramp trial. EMG data for the residual limb’s gluteus medius were available for only eight of the 10 participants during ramp ascent and descent.
TUG and functional questionnaires
The time required to complete the TUG was significantly shorter when wearing the C-Leg Compact compared to the NMPK (17.7 vs. 24.5 sec; p = 0.018). Functional questionnaire scores were higher after using the C-Leg Compact compared to those recorded while using the NMPK, including values on the PEQ’s mobility subscale (7.9 vs. 6.3; p = 0.039) and the ABC (75.7 vs. 60.1; p = 0.001). Houghton scores demonstrated a trend towards higher values following C-Leg Compact use compared to NMPK (8.5 vs. 7.3; p = 0.058).
Subjective comments regarding C-Leg Compact and NMPK prostheses
Positive attributes reported by participants while using the C-Leg Compact compared to the NMPK included moving from sit to stand more naturally, standing longer, taking longer steps, walking faster, fatiguing less, greater stability, greater confidence in new places, capacity to walk and think about other things or walk and talk on phone, and reduced fear and/or occurrence of falls. More specific comments included the ability to walk down a steep ramp to get into a boat, capacity to walk on uneven terrain (i.e. dirt with tree roots), and an absence of falls compared to falling two to three times a week in the NMPK prosthesis (a 65-year-old woman). One person reported a reduction in low back pain. Three negative attributes reported while using the C-Leg Compact were that the prosthesis was too heavy, had to be charged every night, and could not be used around a pool when playing with a dog. Of the nine participants offered the opportunity to choose which prosthesis to keep, all selected the C-Leg Compact.
Discussion
Despite the importance of maintaining a physically active lifestyle for health and wellness, many individuals with transfemoral amputations are limited in their functional capabilities and independence. Access to prosthetic componentry that enables safe and stable ambulation remains restricted. As evidence, approximately 2/3 of community dwelling individuals with a transfemoral amputation reported falling during a 12-month period. 23 Reports of injuries among 40% of those with lower extremity amputations who fell, and the need to seek medical attention by 19%, 23 highlight the personal and societal value of ensuring prosthetic componentry options that promote stability and safety for deconditioned individuals with transfemoral amputations.
The MFCL K2 individuals in the current study displayed significant improvements when negotiating challenging surfaces in the C-Leg Compact compared to their NMPK prosthesis. They ascended and descended ramps markedly faster and were more confident and stable when using the C-Leg Compact prosthesis. The faster ramp ascents and descents with the C-Leg Compact prosthesis were accomplished by not only increasing cadence but also by a longer stride length. This latter strategy reflected participants’ increased stability and was accompanied by a significant increase in the proportion of time spent in residual limb single limb support, another key indicator of stability. 24 The capacity to achieve a longer stride length in the C-Leg Compact prosthesis is consistent with findings of Hafner et al. 8 in their comparison of Level K2 and K3 prosthetic ambulators’ hill descent step length when using a C-Leg Compact versus an NMPK prosthesis.
While residual limb hip and thigh postures were similar between prosthetic conditions, the residual limb’s knee was more flexed throughout single limb support while descending ramps using the C-Leg Compact. This pattern is more characteristic of a normal ramp descent pattern, 1 and allowed for forward and downward progression of body weight in preparation for the next intact initial contact. It was accompanied by enhanced residual limb dorsiflexion, displaying a peak that more closely approximated the amplitude of dorsiflexion recorded for the intact limb but occurred earlier in the gait cycle. One consideration is that each participant’s prosthetic foot/ankle also was changed to address manufacturer guidelines for fitting with the C-Leg Compact. Thus it is possible that the altered biomechanical characteristics of the foot/ankle components contributed, in part, to kinematic changes documented in the residual limb between the NMPK and C-Leg Compact conditions.
While we had hypothesized that EMG amplitudes would be lower due to the increased stability provided by the C-Leg Compact, the results for the eight muscles studied did not support this conclusion. Instead, the greater stability in the C-Leg Compact enabled participants to negotiate ramps more rapidly and two had diminished assistive device needs (i.e. axillary crutch versus single point cane, and bilateral forearm crutches versus single point cane). These factors confounded interpretation of the EMG data. The lack of a significant increase in EMG activity in the eight muscles that are essential for residual and intact limb stability, progression and clearance could suggest that the limbs are not working harder with the improvements documented in the C-Leg Compact prosthesis. However, high inter-subject variability also made detecting significant differences difficult. Future studies that control for walking speed and use of assistive devices between prosthetic conditions (NMPK vs. C-Leg Compact) could help further elucidate the impact of prosthetic features on muscle demands.
Although the time required to complete the TUG was significantly shorter while using the C-Leg Compact (17.7 seconds) compared to the NMPK (24.5 seconds), both values were two to three times longer than the age referenced norm of 8.1 seconds for 60 to 69 year olds without disabilities. 25 These data reinforce the functional compromise of this study’s participants.
Balance is also a component of stability during walking and is critical to overall function for prosthetic users. While we did not have a direct measure of balance in this study, participants anecdotally reported that they had fewer stumbles and falls, were more active and were able to walk on more varied terrains. We identified that walking with the C-Leg Compact increased balance confidence scales 24 to 26% compared to walking in their NMPK prosthesis. While our participants’ mean score on the ABC Scale while using the NMPK prosthesis (60.1) closely mirrored the average value reported by Miller and colleagues for community dwelling adults with transfemoral amputations (60.9), the average score recorded while using the C-Leg Compact greatly exceeded that value (75.7). 26 These findings are particularly encouraging given the strong and positive relationship between balance confidence and mobility capability, mobility performance, and social activity previously documented in individuals with lower limb amputations. 27 Our results are consistent with findings of increased stability, balance and function for persons with a range of functional abilities (MFCL K2 to K4) when walking with the C-Leg.6,8-11,14,28
One limitation of the current study is that only relatively short-term outcomes when using the C-Leg Compact prosthesis were explored. It is possible that the improved walking function and balance documented after three months of using the C-Leg Compact provided a solid foundation for additional skill development. In addition, it is conceivable that individuals with transfemoral amputations might be able to participate in longer duration walking or weightbearing exercise interventions when using the C-Leg Compact given the changes in function and confidence documented in the current study. A longer follow-up period would be beneficial for understanding the impact of the prosthesis not only on changes in function, but also cardiovascular fitness and the development and management of secondary medical conditions often associated with inactivity.
In the current study, participants received a one-hour refresher course regarding how to safely negotiate ramps and stairs in their NMPK prosthesis as it was conceivable that some had not recently negotiated these environmental obstacles given their home/community environment. In addition, participants engaged in five to seven training sessions after receiving their C-Leg Compact in order to learn how to safely use the new features. This was followed by a three-month accommodation period, during which no additional training was provided. While the training sessions were purposefully kept short and an accommodation period was provided, it is possible that patient’s performance may have been impacted by the training.
In the current study, the finding that Level K2 prosthetic ambulators were able to increase their walking speed, particularly on challenging surfaces such as ramps, has important clinical implications. It indicates that prosthetic componentry can significantly impact function. As ramps and stairs are common features in most community environments (side walk access to every street crossing requires one to negotiate either a ramp or curb), the added capacity to negotiate these barriers is essential to enabling community access for deconditioned individuals with transfemoral amputations. The added skill and confidence associated with successfully negotiating community environments would be expected to promote greater community engagement.
Conclusion
Stability was greater ascending and descending ramps in the C-Leg Compact prosthesis compared to the NMPK as evidenced by the faster velocity, longer stride length, greater proportion of time spent in residual limb single limb support, reduced reliance on assistive devices, and the capacity to sustain residual limb knee flexion throughout single limb support. Patient preference to keep the C-Leg Compact versus the NMPK confirms empirical findings of improved performance in the C-Leg Compact. These results have important therapeutic implications when selecting prosthetic knee componentry for more physically disabled individuals who have experienced a transfemoral amputation. The C-Leg Compact may provide important benefits for function and stability for more deconditioned K2 level walkers and those at risk for injurious falls.
Footnotes
Acknowledgements
The authors would likely to greatly acknowledge Thad Buster, MS, Adam Taylor, BS and Yu Shu, PhD for their assistance with data processing.
Funding
This work was supported, in part, by a grant from Otto Bock Health Care LP grant title, Assessment of K-Level 2 Walkers.