
Abstract
People with amputations may find cycling advantageous for exercise, transportation and rehabilitation. The reciprocal nature of stationary cycling also makes it a viable model for research in motor control because the body is supported by the saddle allowing the researcher to focus on the cyclic movement of the legs without the confounding variable of balance. The purpose of this article is to provide an overview of the cycling task in intact cyclists and relate this information to understanding the challenges faced by cyclists with transtibial amputations (CTA). Ongoing research into the biomechanics of CTAs will be summarized to expose the differences between intact and CTA cycling mechanics, asymmetries between limbs of CTAs as well as neuromuscular adaptation following amputation. The article will include recommendations for prosthetic design and modification of the bicycle to improve cycling performance for CTA at all experience levels.
Keywords
Introduction
People with amputations may find cycling advantageous for exercise, transportation and rehabilitation. The cycling task provides an opportunity to maintain cardiovascular health and overall fitness [1] without exposing either limb to the large impact loads associated with walking or running. [2] The reciprocal nature of stationary cycling, for example, makes it a viable method for use in neuromuscular and orthopedic rehabilitation because the body is supported by the saddle allowing the researcher/clinician to focus on the cyclic movement of the legs without the confounding variable of balance. The ability to reduce and control important variables during the cycling task also allows the researcher/clinician to investigate several aspects of how the motion is controlled (motor control).
Control of the cycling task involves integration of both the neuromuscular and musculoskeletal systems. This includes the appropriate timing of muscle activation in order to manage loads imposed on each joint,
[3]
the transfer of energy between joints
[4]
and imparting energy to the cranks
[5]
for propulsion. The strategy utilized then, must take into account each muscle's functional role[6-8] in controlling this task. To better visualize the various stages of this task many investigators have broken up the pedal stroke into four quadrants (Figure 1). While each cycle is part of a continuum of demands, understanding the different control requirements during each quadrant and how those requirements are met by coordinated activation of key muscles (Table I) is crucial. However, before one can understand the challenges faced by a cyclist with a transtibial amputation (CTA), one must understand these aspects of an intact cyclist and how that cyclist meets those challenges.
Pedal stroke quadrants. Zero is defined as when the crank is vertical or at top dead center (TDC). The top of the stroke is from 315–45°. The power phase is from 45–135°. The bottom of the stroke is defined as 135–225°. The recovery phase is defined as 225–315°.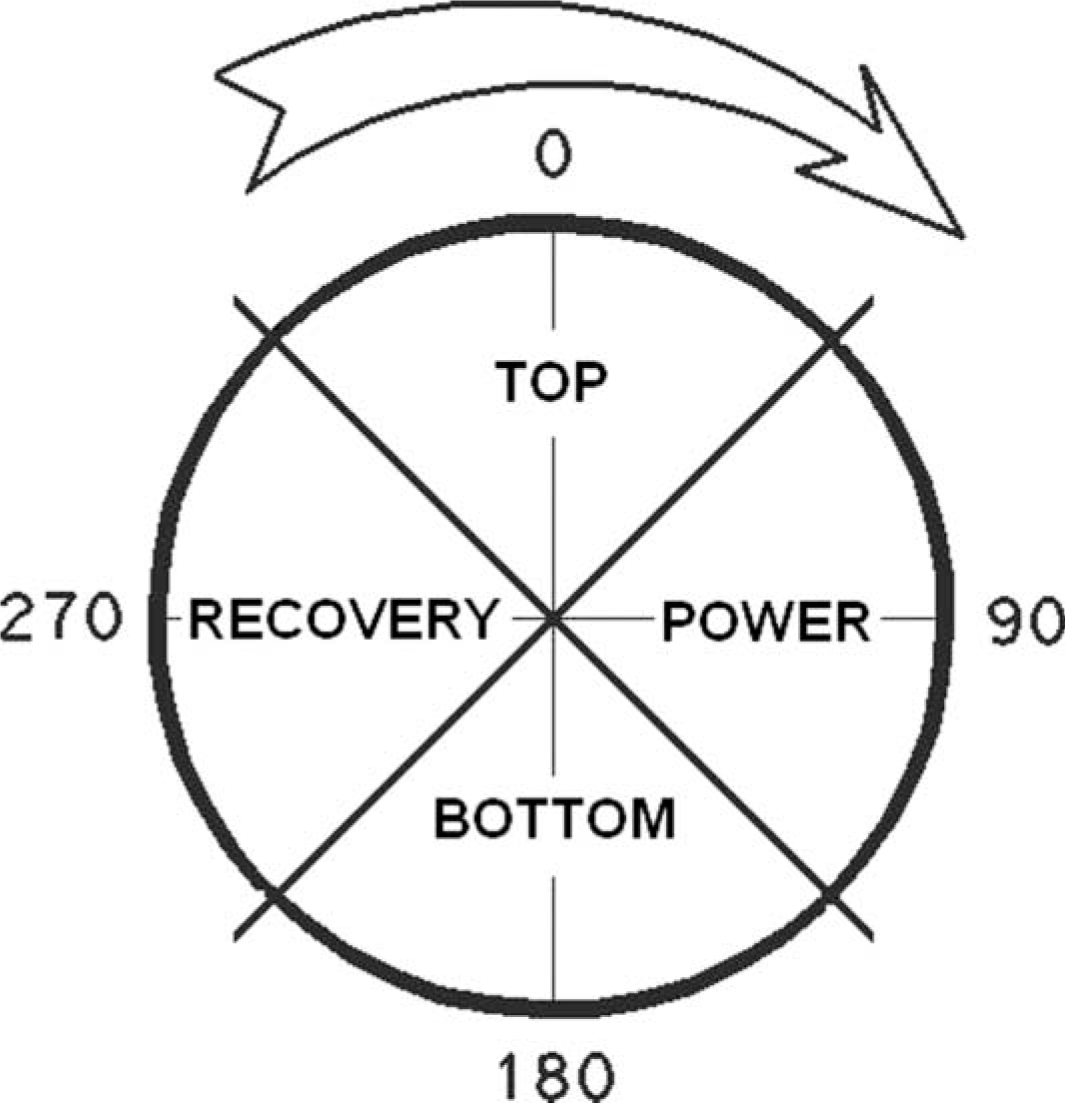
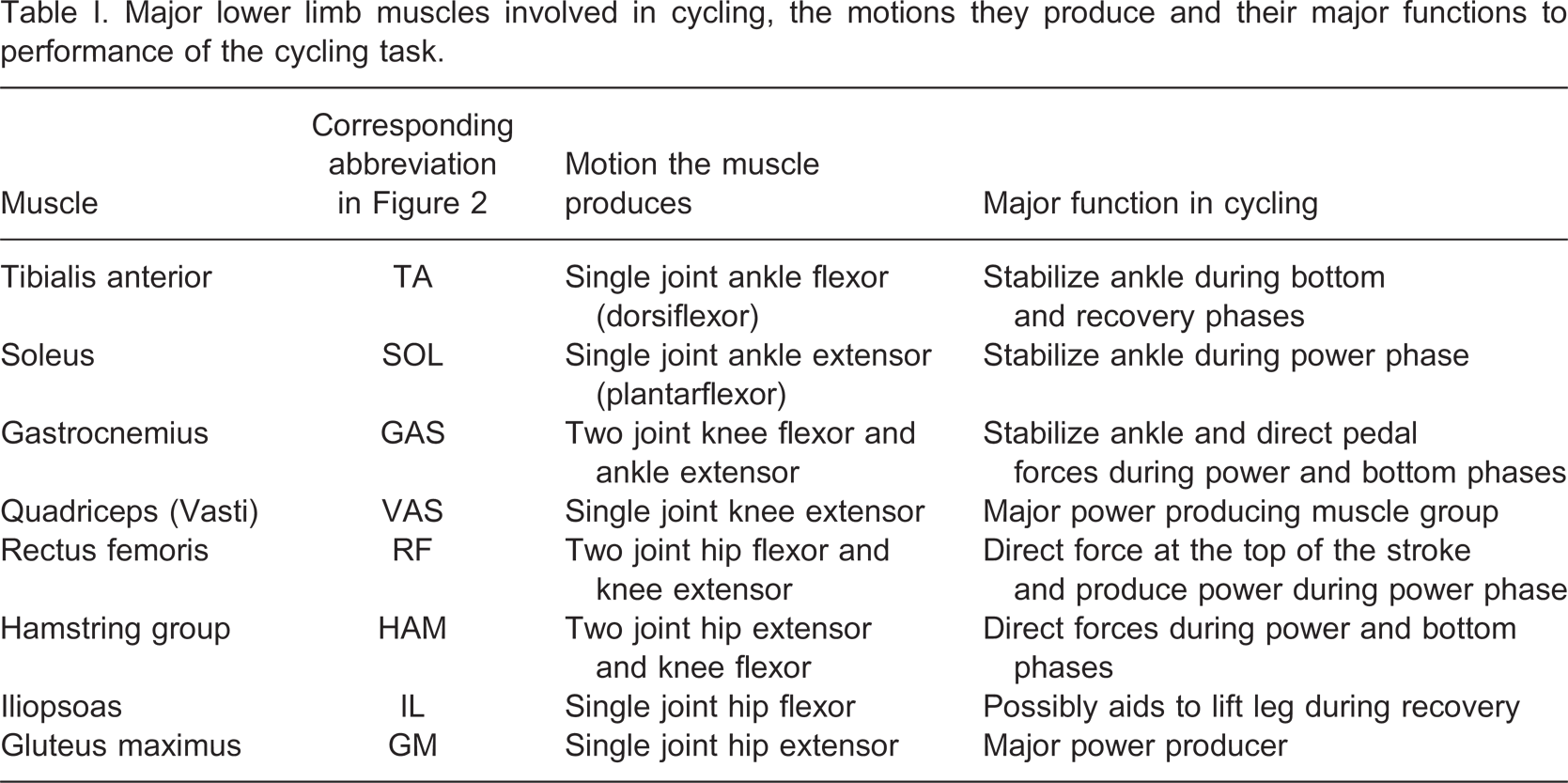
Major lower limb muscles involved in cycling, the motions they produce and their major functions to performance of the cycling task.
The purpose of this article is to provide a foundation of knowledge regarding the challenges faced within the pedal cycle, to have the reader better understand the task of cycling (Figure 2) and finally to better relate this information to understanding the challenges faced by a CTA. Recent ongoing research into the biomechanics of CTAs is summarized to expose the differences between intact and CTA cycling mechanics, asymmetries between limbs of unilateral CTAs as well as neuromuscular adaptation following amputation. The text includes recommendations for prosthetic design and modification of the bicycle to improve cycling performance for CTA at all experience levels. These recommendations are derived from experimental data from multiple studies, computer simulations, and personal experiences of the authors. The article concludes with possible directions for future research into the biomechanics of CTAs. All human subjects who participated in studies associated with this article provided a separate written informed consent and participated in protocols approved by the Institutional Review Board.
Schematic of the lower limb showing representative muscle activity of the lower limb, direction and magnitude of the force at the pedal, and limb positions in the four different quadrants of the pedal stroke. Muscle activity within each quadrant is indicated by the thickness and shade of the lines. Muscles may be very active (thick black), moderately active (thin black) or not active (thin grey). Numbers around the pedal arch denote the start and stop of the respective quadrant in crank degrees relative to TDC. Magnitude of the force vector corresponds to its length defined by the schematic key. Values for limb orientation, muscle activation and force production are derived from experimental data on an intact cyclist operating at 200 watts and 90 rpm. Refer to Table I for a summary of each major muscle group and their function during cycling.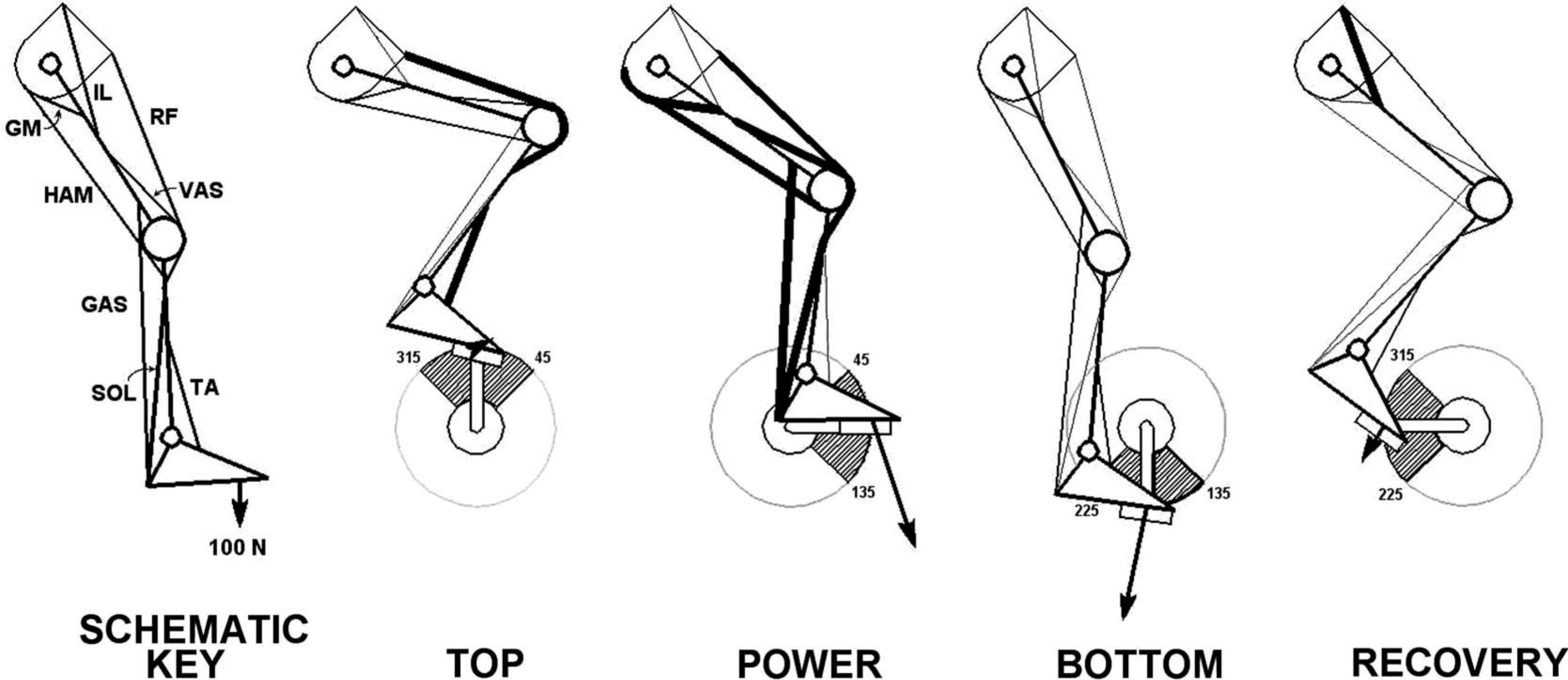
Review of the biomechanics of intact cycling
The top of the pedal stroke
The top of the pedal stroke is a transition area and occurs from approximately 315–45° relative to 0° or top dead center of the crank (TDC) (Figure 1). The pedal is traveling from posterior to anterior while transitioning from moving superiorly to inferiorly. To get through the top of the stroke the leg must direct force forward while preparing for the power phase (Figure 2). Effective application of force to the pedal during this phase is difficult but critical to the transition and development of an effective power phase. The Rectus Femoris (RF), for example, is active trying to flex the hip and extend the knee to direct forces anteriorly. To prepare for the power phase, the Gluteus maximus (GM) and Vasti (VAS) start to activate just before TDC while the hamstring group (HAM) begins activity to aid in hip extension.
The power phase
The power phase is where the body must produce enough force to overcome the resistance at the pedal as well as to help lift the opposite leg during its recovery phase. During this phase about 90% of the total power is imparted to the bicycle. The GM and VAS are generating most of the force seen at the pedal during this time. The ankle extensors (plantarflexors) activate to stabilize the ankle and allow the energy generated by the larger more proximal muscles to be transferred to the pedal and ultimately rotate the crank.
The bottom of the pedal stroke
The bottom of the pedal stroke is another transitional region of the pedal cycle. The HAM, Gastrocnemius (GAS) and Tibialis anterior (TA) are all active in this phase. The TA is active to stabilize the ankle so that tension developed in the GAS may be transferred to the knee joint to assist the HAM with knee flexion. [9] In CTA, the ankle is either absent or prosthetically simulated and thus cannot be stabilized by active muscular contraction. Furthermore, the GAS has been surgically changed to a single-joint knee flexor and can only act upon the knee joint concentrically (if at all) to aid in directing forces during this portion of the pedal cycle. Note: The large downward forces during this phase (Figure 2) are due to the inertia of the heavy limb being redirected from moving inferiorly to a superior direction and are not derived directly from muscular activation. Muscle activation during this phase is needed to direct as much of this force posteriorly. [7]
The recovery phase
This phase occurs when the pedal has cleared the bottom and is now ascending back toward TDC. As the name implies, this phase of the crank cycle is intended for recovery of several extensor muscle groups. During this phase, the Vastii show no appreciable activity. The TA and the Iliopsoas (IL) are most active 3, , [10] with the TA assuming two functions: (i) To stabilize the ankle for force transfer from hip flexor muscles, and (ii) to start dorsiflexing the ankle thereby allowing more clearance for the limb during the top of the stroke. This cannot be accomplished in CTA. Their prosthetic ankle cannot actively dorsiflex through TDC for limb clearance thus creating the need for accommodation through increased hip and knee flexion for these cyclists. The RF will begin activity during the end of this phase aiding in hip flexion, while preparing for the top of the pedal cycle.
The power during this phase is negative, i.e., power is being absorbed (Figure 3) because the forces during this phase are directed inferiorly (Figure 2). From the standpoint of mechanical effectiveness, this phase of power absorption may seem inefficient to the casual observer. However, there is a difference between mechanical effectiveness and metabolic efficiency. Mechanical effectiveness is the ratio between the total force seen at the pedal and the force directed to turn the cranks. In cycling, inertial and gravitational forces of a heavy (∼18 kg) spinning leg are large and generally directed inferiorly (impeding rotation) during the recovery phase.
[11]
The two limbs are coupled by the cranks so that while one limb is in recovery, the other is in its power output phase. In order to generate the same baseline power, the flexor groups of the ascending limb must increase muscular activity 1.1 to 3.4 beyond baseline performance and increase the whole body metabolic demand by 9%
[12]
to overcome these gravitational and inertial forces to pull the foot up faster than it is being ‘pushed’ up by the opposite limb. Attempting to ‘pull up’ and generate positive power during this phase will increase mechanical effectiveness but at a high metabolic cost
[13]
regardless of cycling experience and pedal type.
[12]
Korff et al. (2007) studied the energy requirements of different pedaling techniques and reported that the cyclist's ‘preferred technique’ was the one most metabolically efficient, and that consciously altering this technique, e.g., ‘pulling up’, resulted in a decrease in metabolic efficiency. This was the case even when the cyclists were ‘pulling up’ as they remained unable to generate positive power during this phase. Attempting to ‘pull up’ will certainly reduce the demand on the opposite limb but the costs appear to outweigh any possible benefits available at least to intact cyclists.
[12]
Exemplar Mean Power (dark line) of five continuous crank cycles ± 1 standard deviation (thin line) developed about the crank spindle during the pedal stroke. Data derived from one limb of an elite cyclist pedaling at 200 watts and 90 rpm. Note the large positive impulse during the power phase (45–135°) and the negative impulse during the recovery phase (226–315°).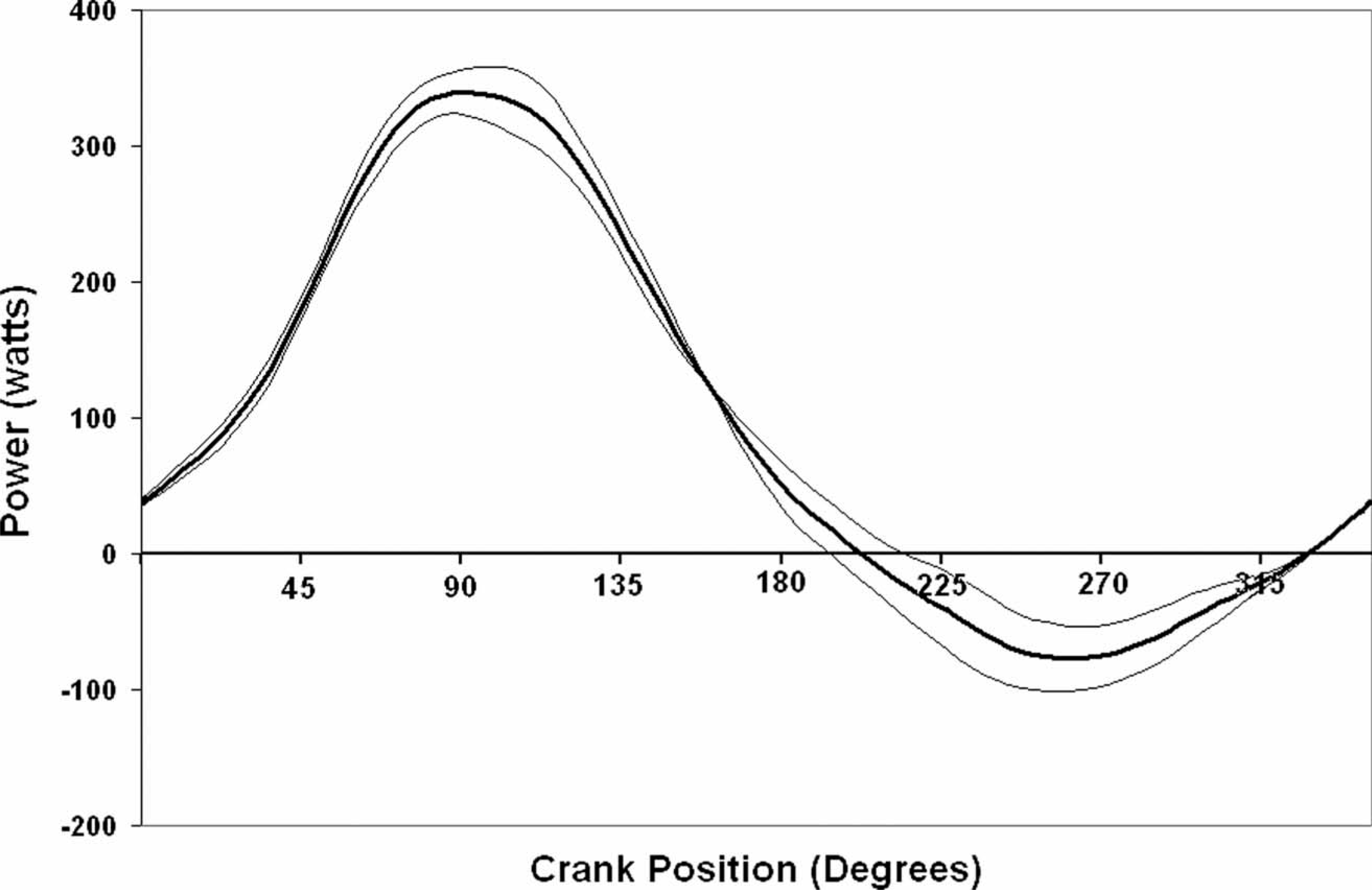
Biomechanics of cyclists with transtibial amputation
Cycling with transtibial amputation poses significant challenges resulting from the loss of the ankle joint structure, the muscles that control that joint, and the sensory input from the joint and surrounding musculature followed by alteration of muscle properties within the remaining, more proximal muscles. [14] These challenges are further compounded because CTAs must interact with their environment through a prosthetic limb on one side and an intact limb on the other. The geometric asymmetry between limbs contributes to asymmetric work (torque) production seen in cyclists with a uni-lateral CTA. 15, , [16] In one report, in eight CTAs work asymmetry was seven times greater than in a control group of nine intact cyclists. [15] Work asymmetry occurs when one limb has difficulty producing and/or directing forces appropriately. [17] This asymmetry could be related to multiple factors beyond a strength or mass difference between limbs [15] and may even represent a change in the motor control strategy used by the body to accomplish this task. Further research is needed to clarify what strategy CTAs utilize for propulsion, the underlying causes of this different strategy, and what affects that strategy. Increasing our understanding of how the body changes its strategy for locomotion following amputation is crucial for the design of improved rehabilitation programs.
EMG patterns in CTAs
Muscle activation patterns in one- and two- joint muscles generally reflect their biomechanical role in movement control.
[7]
Lower limb loss will affect the role played by individual muscles in limb control. The GAS muscle is altered following transtibial amputation, i.e., relegated to a one-joint knee flexor, while the more proximal, non-amputated, muscles retain their anatomical attachments. Analysis of muscle activation patterns collected using surface electromyography (sEMG) in six CTAs revealed that the neuromuscular system shifted activation in three amputated GAS muscles to later in the pedal cycle (Figure 4). This shift in timing appears to be more appropriate for the muscles' new role as a single joint knee flexor. The other three subjects showed almost no activation. Reasons for this lack of activation could be related to the surgical procedure, signal artifact of the electrode rubbing the socket, nerve damage and/or excessive scaring of the residual limb. When the remaining GAS was utilized by the CTA and those signals were collected, the neuromuscular system adapted to the change in muscle function to utilize the muscle in its new role as a single joint knee flexor.
[18]
Average sEMG of the Gastrocnemius (GAS) muscle from the sound (dashed) and amputated (solid) limbs showing a shift in activation to later in the crank cycle for the amputated GAS. sEMG signals were pre-amplified and bandpass filtered (3 db at 8 and 550 Hz), RMS was taken, averaged across 15 cycles and normalized to the maximum value. The sound limb data was derived from six CTA while the amputated limb data was derived from three CTAs.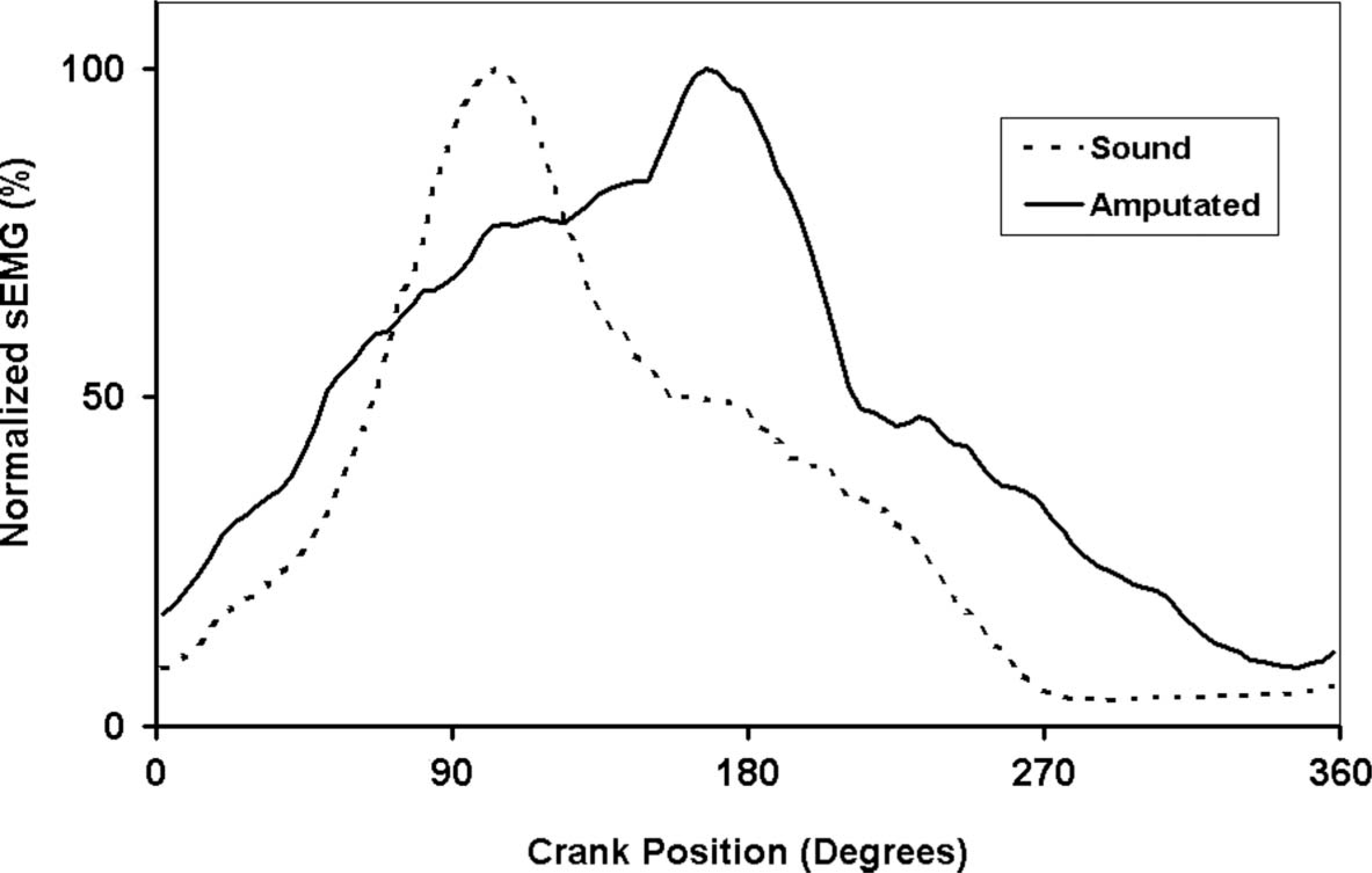
Other changes observed in CTA include: (i) Increased variability in the activity patterns of two-joint muscles in the sound and amputated limb compared to intact cyclists, and (ii) the GAS in the sound limb increased its duration of activity. [18] These results help explain the asymmetries observed between the two limbs as prolonged activation of the GAS will help apply more force effectively during the bottom of the pedal stroke, thereby helping the ineffective amputated side through the top of the pedal stroke. The increases in muscle activation variability observed in the two joint muscles in CTAs [18] may also reflect difficulty in energy management across multiple joints [4] and/or failure of the neuromuscular system to integrate sensorimotor information into the modified neural control system. 19, , [20] Additional research is necessary before these issues can be fully understood.
Recommendations for adaptation of the bicycle and cycling prosthesis design
Bicycle positioning
How the body interacts with the bicycle is affected by changes in body position.[21-23] The location of the saddle in relation to the crank spindle, the handlebar and the pedals defines the constraints imposed on the neuromuscular system to energize the bicycle. For example, alterations in saddle height will partially determine the functional joint range of motion (ROM), and thereby determine the range of muscle lengths and available contraction velocities. [24] Saddle height alterations also affect the location of the center of mass and thus the bicycle handling characteristics. [23] These interactions between multiple body segments and the bicycle however, are complex and beyond the scope of this article. The reader is encouraged investigate this topic further through textbooks [24] and lay publications 23, , [25] to better understand clinically acceptable practices for bicycle fitting.
Experience gained with CTA athletes suggests that following published guidelines for intact cyclists [25] is appropriate when no comorbitities exist. However, comorbitities and limitations in joint ROM are common following an amputation. [26] These will affect the position of the body thereby making the cycling task more complicated. It is recognized that the prosthetist's expertise lies with the alignment of the prosthesis for walking but the alignment of the prosthesis in conjunction with the alignment of the body on the bicycle incurs different and more complex challenges. When a person with a trans-tibial amputation desires to cycle, it is recommended that the clinician pair with someone trained and skilled in bicycle fitting 25, , [27] to produce the best clinical outcome. The interactions of the body and its position on the bicycle are very complex even in intact, non-symptomatic patients and overuse injuries have been associated with poor positioning. 24, , [25] These interactions are implicitly more complicated by the introduction of a prosthesis so the clinician should proceed with caution when fitting someone that wishes to cycle.
The effect of crank shortening
Shortening the crank on the amputated side will help reduce the geometric asymmetries between the two lower limbs of a CTA. The intact ankle in the sound limb actively plantarflexes at the bottom of the pedal stroke and dorsiflexes at the top.
[5]
Prosthetic ankles lack the ability to actively move and thus the amputated side can either compensate by increasing knee range of motion (ROM) and/or by greater movement at the hip joint. An increase in knee ROM would be accomplished by over extending at the bottom and being more flexed at the top of the cycle.
[28]
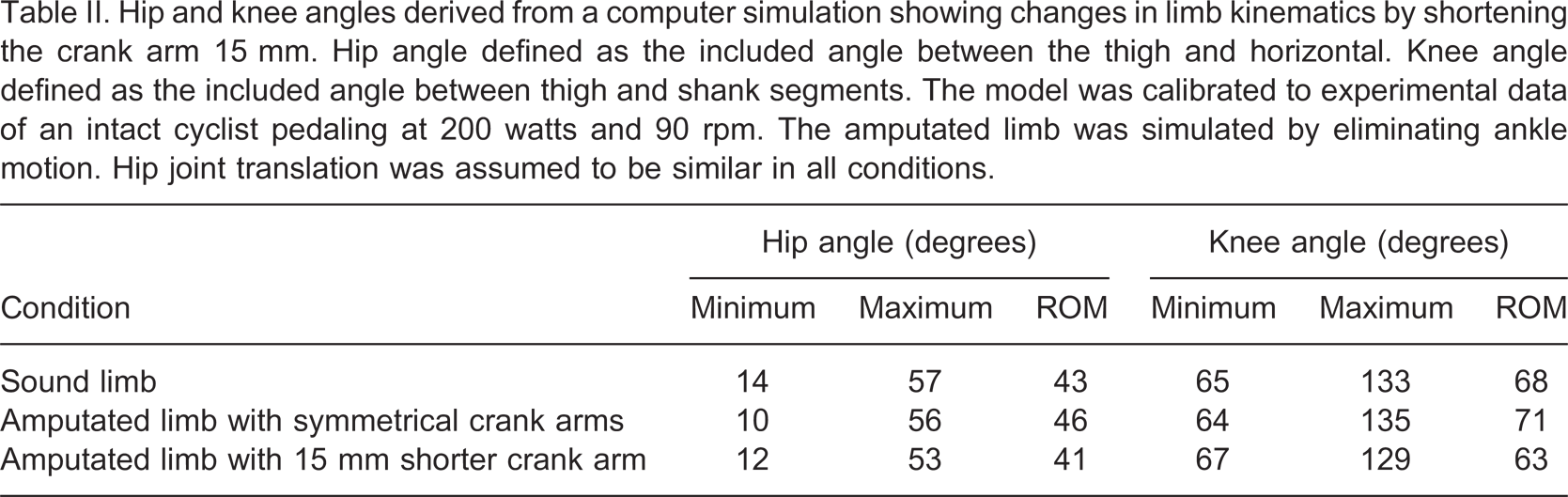
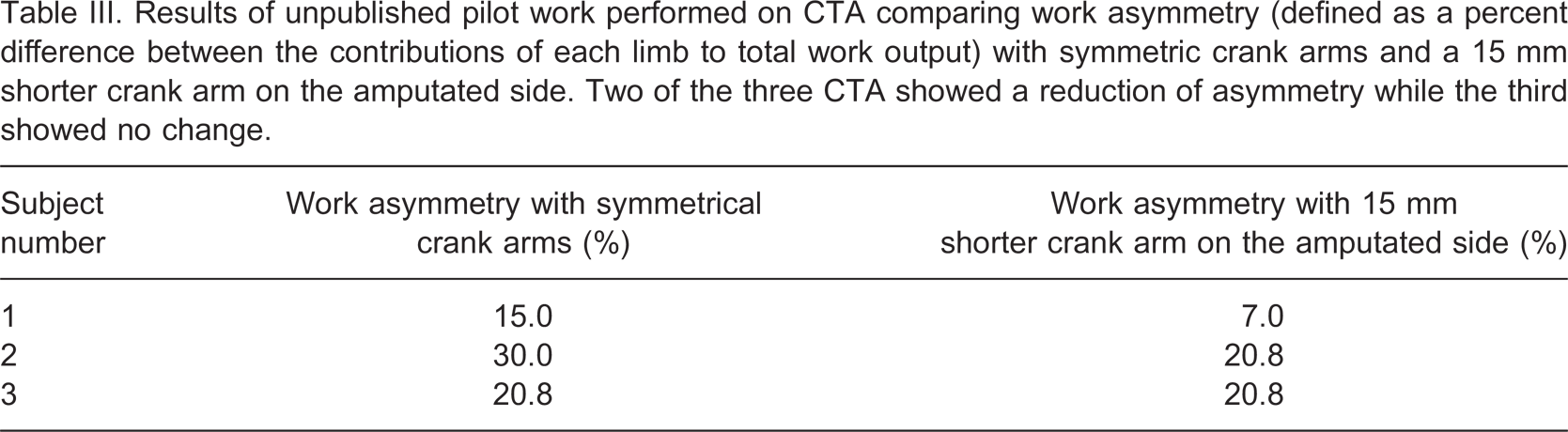
Inferior translation of the hip joint could prevent increased extension of the knee joint at the bottom of the crank cycle but may create irritation between the saddle and soft tissues of the cyclist. Shortening the crank on the amputated side brings the pedal closer at the bottom and further away at the top of the stroke making demands on the affected side knee ROM similar to the intact side while reducing the need for hip joint movement. A computer program has been calibrated with experimental data collected on an intact cyclist to simulate the kinematics of a CTA cycling with and without a shortened crank (Table II). Preliminary work completed in three CTAs to evaluate the effects of shortened cranks showed a reduction in work asymmetry in two CTAs while one CTA showed no change (Table III). Work asymmetry is the difference in work or torque production between the two limbs. Work asymmetry is calculated using instrumented pedals that measured the magnitude and direction of force produced at the foot/pedal interface of each limb.
[17]
A reduction in work asymmetry indicates the sound limb had to contribute less work to turn the pedals. Despite the reduction of work asymmetry with the shorter crank in two out of three subjects, no experimental data was taken on limb kinematics thus no conclusions can be drawn as to whether a reduction in knee ROM or hip joint translation occurred as predicted by the computer simulation. Furthermore, experience gained working with CTA cyclists showed that most inexperienced CTAs report an increase in comfort while more experienced CTAs (+10 years' experience) report initially use of a shortened crank arm but later converting back to symmetrical crank arms as they better adapt to cycling. Again, more research is necessary before a clear clinical recommendation can be made. Adaptation of the bicycle to a shorter crank can be achieved by obtaining a crank shortening adapter
[29]
available through local bike shops (Figure 5).
Example of a commercially available adapter to shorten the crank arm on the prosthetic side while moving pedal out laterally to increase clearance between the prosthetic heel and the crank. Photograph shows a frontal view of the installed bracket on a crank arm with a pedal (bottom left) as well as the bracket uninstalled (top right). This bracket allows for four different crank arm lengths and may be easily removed and installed on many different bicycles.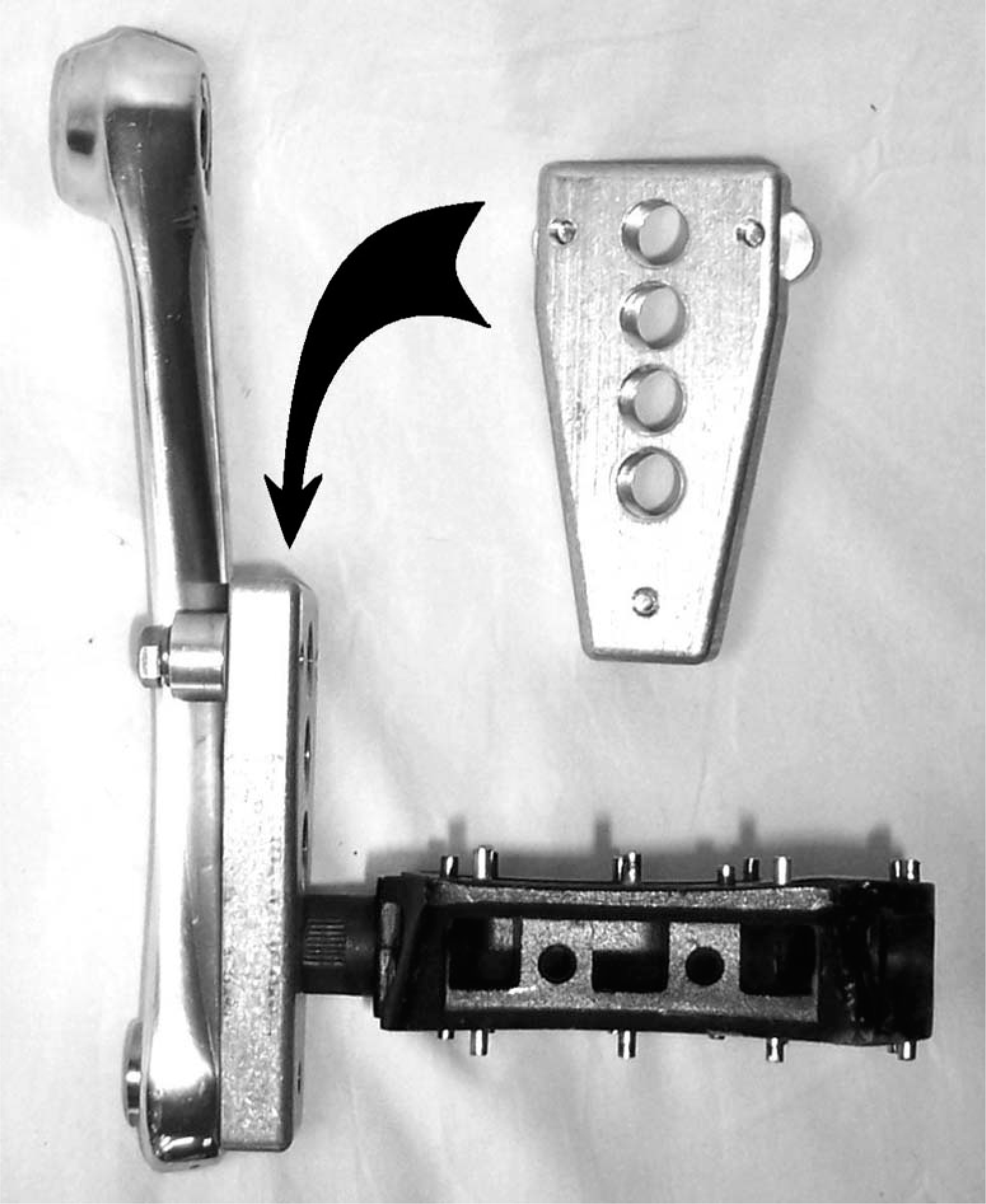
Hip and knee angles derived from a computer simulation showing changes in limb kinematics by shortening the crank arm 15 mm. Hip angle defined as the included angle between the thigh and horizontal. Knee angle defined as the included angle between thigh and shank segments. The model was calibrated to experimental data of an intact cyclist pedaling at 200 watts and 90 rpm. The amputated limb was simulated by eliminating ankle motion. Hip joint translation was assumed to be similar in all conditions.
Results of unpublished pilot work performed on CTA comparing work asymmetry (defined as a percent difference between the contributions of each limb to total work output) with symmetric crank arms and a 15 mm shorter crank arm on the amputated side. Two of the three CTA showed a reduction of asymmetry while the third showed no change.
The role of the prosthetic foot in cycling
The stiffness of the prosthetic foot influences cycling performance at high intensities (90% max heart rate) but not at low intensities, i.e., more recreational level intensities (70% max heart rate). [30] Cycling with an intact lower limb requires activation of the triceps surae and tibialis anterior muscles to stabilize the ankle so that energy generated by the knee and hip extensors may be transferred to the pedal. [3] While triceps surae and tibialis anterior muscle activation is necessary in walking, for example, for ankle stability, braking and propulsion, [31] these prosthetic feet are designed to mimic the ankle/foot complex during walking, i.e., allowing it to compress and store energy at initial contact then decompress and release that energy at toe-off. Forces and the timing of those forces are different between walking and cycling however, requiring a prosthetic foot be designed to meet the specific demands of cycling.
In cycling, the compressive forces used to store energy in a prosthetic foot are derived from muscular sources being used to turn the crank during the power phase. Then at the bottom of the stroke, these vertical forces are removed to allow the foot to decompress and release energy. The problem with a flexible prosthetic foot is that it requires muscular forces to compress it during the power phase thus removing energy that should be transferred to the cranks. The foot decompresses during the bottom of the pedal stroke. The forces during this phase are directed ineffectively to produce torque. Figure 2 shows limb orientation as well as the scaled magnitude and direction of typical forces at the foot/pedal interface during the power phase (when the foot is being compressed) and the bottom of the pedal stroke. The use of a flexible prosthetic foot results in energy removed from the crank cycle and not returned in an effective manner.
The energy removed from the crank by the flexible prosthetic foot requires compensation from the sound limb to increase its output in order to meet task demands. The result is an increase in pedaling asymmetry. [15] Furthermore, we have found that the increases in torque asymmetry are only apparent at higher cycling intensities. Cycling at lower intensity requires lower normal forces which in turn may not be sufficient to compress the prosthetic foot to create a noticeable asymmetry. Thus, for a cyclist in a rehabilitation setting or cycling for recreation, the stiffness of the prosthetic foot has little effect. It is not until the cyclist is operating at higher; more competitive intensities that an energy storage and return (or dynamic response) type prosthetic foot will begin to have a negative impact on their performance.
Combination of a shortened crank arm and a stiff prosthetic foot
Pilot work to optimize cycling performance in a Para Olympian cyclist was performed to minimize work asymmetry. The flexible prosthetic foot was removed and the cycling cleat was placed at the end of the pylon via a custom aluminum bracket. The anterior-posterior position of the cleat was maintained between both limbs at the 1st metatarsal head. The crank arm on the amputated side was shortened 15 mm. Work asymmetry was initially at a 30% difference between limbs meaning that the sound limb contributed 65% of the work while the amputated limb contributed 35% of the work. Work asymmetry was reduced with the stiff foot and the shorter crank to a 7% difference between limbs. There was also a corresponding reduction in HAM and GAS activity within the sound limb. The combination of a stiff foot interface along with a shorter crank arm reduced the work asymmetry to a level similar to intact cyclists 15, , 17, , [30] for this elite level athlete. It is not known however, if these results can be generalized to more recreational cyclists.
Foot/pedal interface for cyclists with amputations
Attaching the prosthetic foot to the pedal is necessary in order to keep the prosthetic foot in contact with the pedal throughout the pedal cycle. Several methods could be used to secure the foot to the pedal and pedal selection is a balance between the levels of security vs. the cyclist's ability to remove the foot in an emergency. The easiest, yet least secure, method is to use a studded BMX pedal with a soft soled shoe (Figure 6). Other methods include using Velcro® between the pedal and shoe, a neoprene strap or commercially available clipless pedal systems (Figure 6). Although all clipless pedal systems have been used successfully by CTAs, some are better than others. Using a double-sided mountain bike system allows the use of a cycling shoe with a recessed cleat that will ease walking off the bicycle. It also allows the cyclist to clip into either side of the pedal whereas most road pedal systems only allow access on one side. The pedal system should require 20° or less of axial rotation (known as float) to ease cleat disengagement.
Four examples of different bicycle pedals suitable for CTA. A studded BMX pedal (top left) provides the least foot/pedal security while being the easiest to dismount the bicycle. A LOOK brand road pedal (top right) provides a more secure method to attach the foot to the pedal but only allows entry on one side. The bottom two clipless pedal systems from Shimano (bottom left) and Crank Brothers (bottom right) are designed for mountain biking and allow entry on either side. A pedal designed for mountain biking also us a smaller cleat that may be recessed in the cycling shoe to ease walking off of the bicycle.
The cylindrical shape of the residual limb allows for poor rotational control and thus may limit the cyclist's ability to axially rotate the limb for disengagement of the pedal. When using a clipless pedal system, it is recommended that the cyclist clip in their amputated limb first, push off with that limb and then clip in the sound limb once they are moving. To unclip, it is recommended that the sound limb unclip first, the cyclist stops, moves their body toward the front of the bike, fully extending their still ‘clipped in’ amputated limb and use internal/external hip rotation to unclip (Figure 7). This technique has also been successful for people cycling with AFOs or limited ankle motion.
Diagram demonstrating a technique to disengage clipless pedals for cyclists with amputation. As the cyclist comes to a stop, they should disengage their sound limb and place on the ground for stability (left panel). The cyclist should then move their trunk toward the front of the bicycle while fully extending their amputated limb (right panel). Finally, to disengage, the cyclist may use internal or external rotation of their hip (arrows in left panel). There are other techniques to disengage clipless pedal systems the cyclist may adopt later but this is an example of a technique the cyclist may use initially. This technique works well for any cyclist with limited ankle mobility.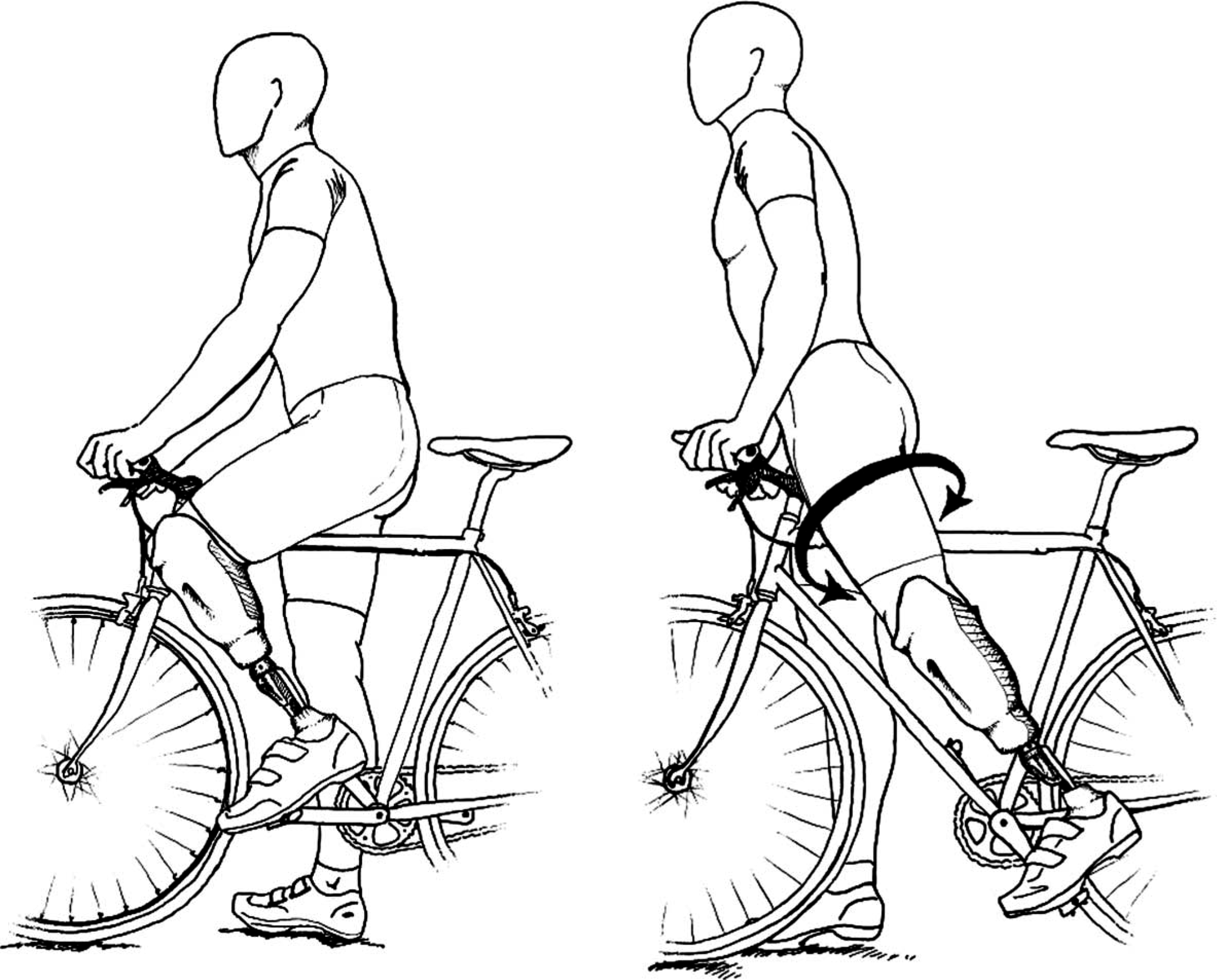
Prosthetic foot to crank clearance
The prosthetic foot should be aligned with no toe out as it creates a clearance problem between the prosthetic heel and the crank arm. If the individual utilizes their walking prosthesis for cycling that has been aligned with a toed out prosthetic foot, it is suggested they outset the pedal laterally using a pedal spacer
[32]
available at local bike shops (Figure 8). The use of these spacers may also be used to alter medial-lateral tracking of the knee in the frontal plane during cycling. Medial-Lateral alignment should consider individual comfort and allow the knee to track vertically over the pedal.
[25]
Medial-lateral deviation during the pedal stroke may increase varus/valgus knee moments
[24]
and predispose the cyclists to knee pain.
24,
,
[25]
Increasing varus/valgus knee moments may also result in irritation of the residual limb on the medial or lateral condyle of the knee and the distal tibia.
An example of a commercially available spacer to outset the pedal laterally and increase clearance between the prosthetic heel and the crank arm when a walking prosthesis is being used for cycling and heel/crank clearance is a problem. The crank arm shortening adapter (Figure 5) will also outset the pedal. Spacer pictured with a Shimano SPD mountain bike pedal (Figure 6).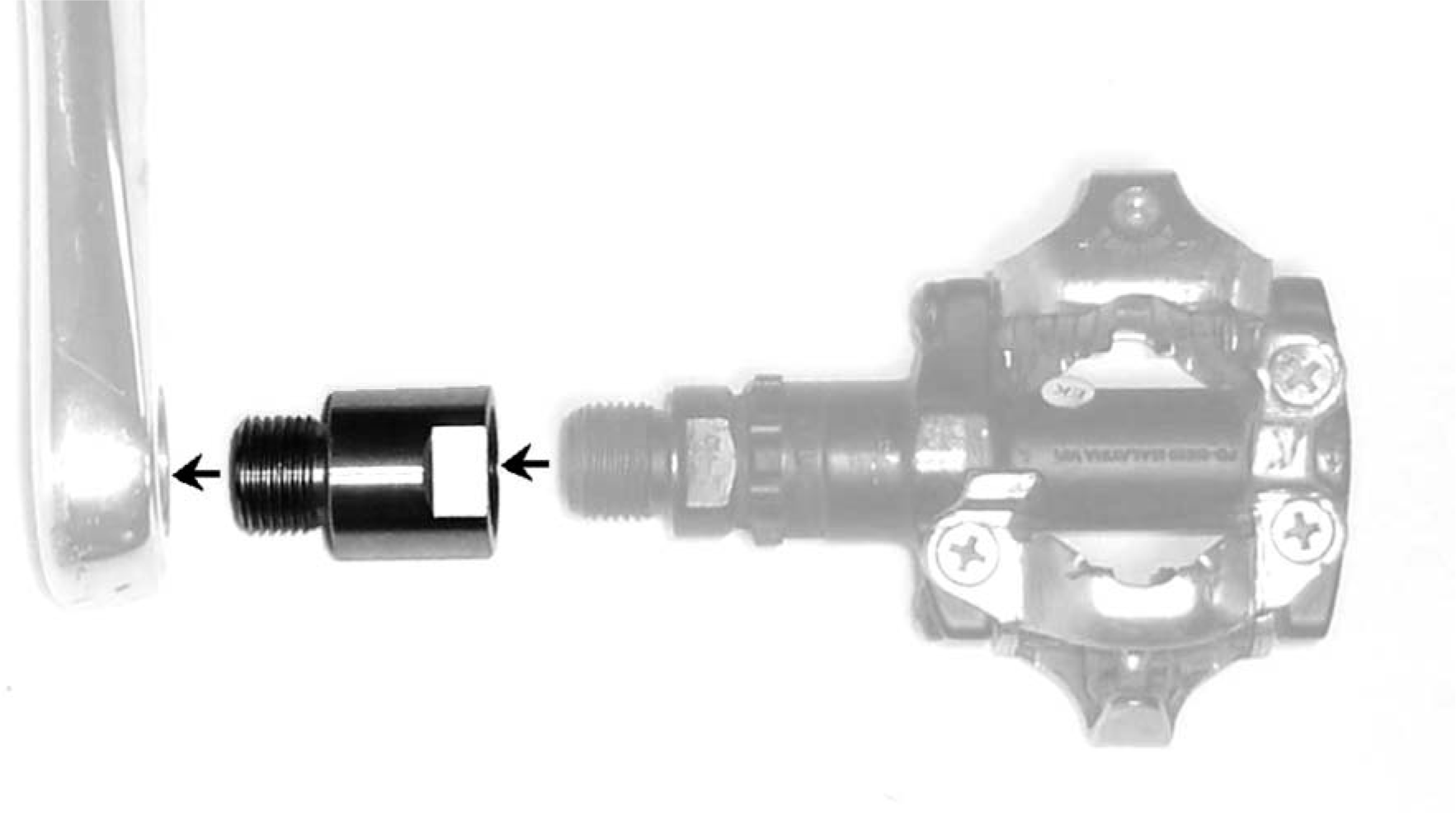
Anterior-posterior cleat placement and effective prosthetic length
Anterior-posterior (A-P) placement of the cleat does not affect metabolic efficiency in intact cyclists [33] or CTA [34] but will affect muscle activation of the GAS, SOL and TA in intact cyclists. [35] Minimization of muscle activation of these muscles occurred at or just posterior to the 1st metatarsal head and reflect established guidelines for intact cyclists. [25]
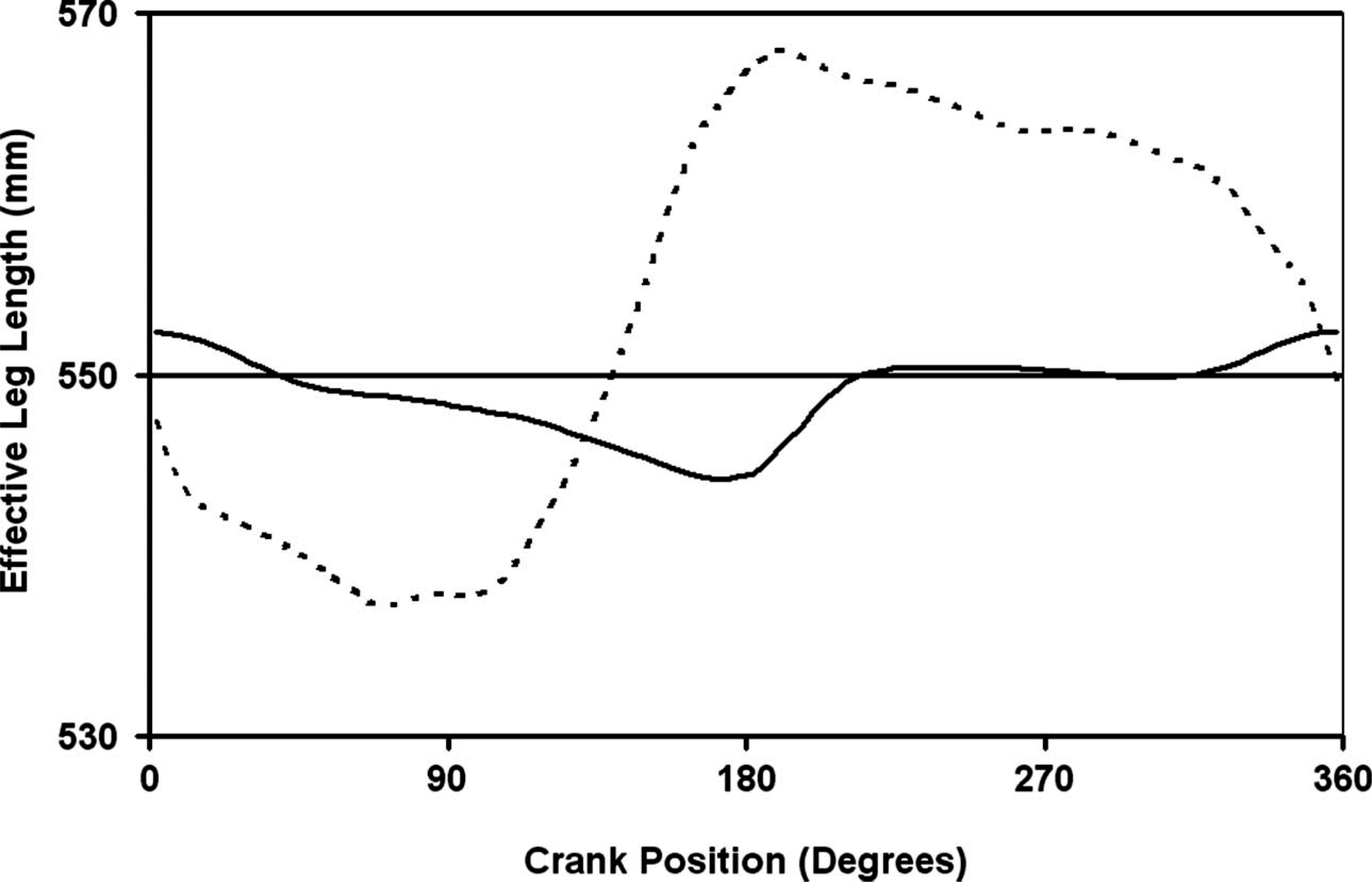
In CTA the A-P location of the cleat will determine the overall socket flexion/extension angle as well as determine the effective prosthetic length. The effective prosthetic length in cycling is different than walking. In walking, the effective length is the distance from the knee center to the bottom of the heel while in cycling, the end point is the pedal spindle and not the heel. Therefore, effective prosthetic length for cycling should be measured from the knee center to the centerline of the cycling cleat (Figure 9). Furthermore, the effective prosthetic length should be set similar to the sound limb to minimize geometric asymmetries. However, the sound limb ankle can actively move thus constantly changing this length throughout the pedal cycle (Figure 10). The same computer model used to analyze crank arm lengths
[28]
was used to analyze the kinematics of effective prosthetic length changes. A compromise was made so that if the effective prosthetic length was similar to the sound limb when the ankle was in the neutral position, kinematic asymmetries were minimized. These results however, should be used with caution as there is currently no experimental data to help determine optimal A-P placement of the cycling cleat or the complex interaction between A-P placement and effective prosthetic length. It is therefore left to the clinician and cyclist to make the best clinical judgment.
Diagram describing the difference in effective prosthetic length for cycling and walking. Effective prosthetic length in cycling is from the knee center to the cycling cleat. Effective prosthetic length should be matched to the sound limb. For example, if the cleat on the sound limb is positioned at the 1st metatarsal head yet the cleat on the prosthesis is positioned posteriorly then the prosthesis should be lengthened to minimize geometric asymmetries. Exemplar data for effective leg length during the crank cycle of the sound limb (dashed line) and a prosthesis (solid line) using a flexible dynamic response type prosthetic foot. The horizontal line at 550 mm represents the effective leg length of the sound limb when the ankle is in the neutral position for this particular CTA. Cleat location for both limbs is approximately the 1st metatarsal head. Effective leg length in cycling is measured from knee joint center to the center of the cycling cleat. Increases in effective leg length indicate the ankle is extending. Note: Although the prosthetic foot allows movement, is not similar to the sound limb in both amplitude and phase. Therefore allowing ankle motion in the prosthetic foot will not replicate the motion of the sound limb during cycling. Data derived from a CTA subject operating a 350 watts and 125 rpm during a simulated time trial.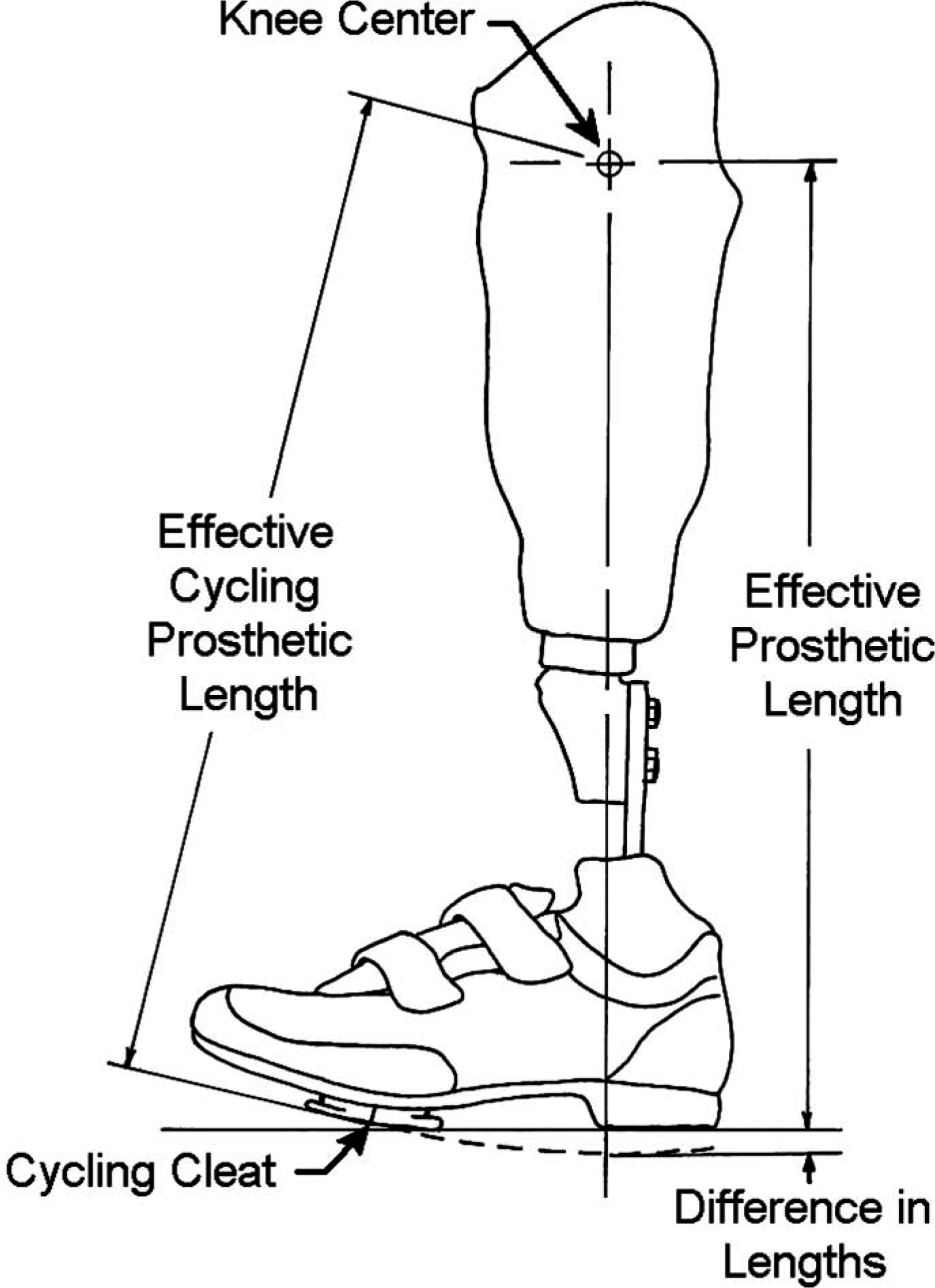
Suspension selection for cycling
Suspension selection for cycling varies according to cyclist preference and experience and generally reflects what is utilized for the walking prosthesis. Although suction suspensions have been used successfully, the increased bulk of the system needs to be considered. The prosthetic liner plus suspension sleeve will reduce knee ROM and create potential problems between the posterior aspect of the knee and the posterior trimline of the prosthesis. However, there has been no systematic evaluation of different suspensions and the problems (if any) associated with their use in cycling.
Cycling with bilateral transtibial amputations
A cyclist with bi-lateral transtibial amputations allows for alteration of the femur to shank ratio. Pilot work on a bi-lateral transtibial cyclist for triathlon competition was completed to optimize this relationship. Increasing the overall limb length requires raising the saddle thereby raising the center of gravity of the cyclist. This may create problems with bicycle fit and stability. Shortening the limb length increased stability but creates more knee flexion and ROM. An effective prosthetic length of 0.93 times the thigh length provided the best compromise between kinetic and kinematic variables. This ratio is similar to the average intact population. [36]
Conclusion
The cycling task provides a method for rehabilitation, exercise and investigations into motor control for people with amputation. This article provides a background in how intact persons cycle, the challenges faced by cyclists with amputation and how those challenges result in pedaling asymmetries. A change in motor control strategy is suggested as a cause of the asymmetries yet more research is warranted before a complete understanding of how this strategy differs from the sound limb or intact cyclists. This article provides recommendations on how the bicycle and the prosthesis may be adapted to improve cycling performance. These adaptations may be different for competitive and recreational cyclists. For competitive cyclists, a stiff prosthetic foot is recommended. Recreational cyclists may utilize their walking prosthesis if the pedal is moved laterally to allow clearance between the heel and the crank arm. Both groups may benefit from using a shorter crank arm on the amputated side as well as a commercially available clipless pedal system. It is recommended that the prosthetist team up with an experienced bicycle fitter to help with the complex problems of body positioning. Many questions still remain regarding the affect of different prosthetic alignment on cycling performance and will require additional research. Continuing efforts will help provide solutions to optimize prosthetic wearer outcomes for both recreation and rehabilitation.
Footnotes
Acknowledgements
The authors gratefully acknowledge Warren Mays, CPO, for his review of the manuscript, Peter Harsch, CP, and Bob Gailey, PhD PT, for their advice and support during the writing of this manuscript, Laura Clark Jones, Rob MacDonald, and Chris Hovorka for their help in data collection. The authors also acknowledge the incredible support from the students, faculty and staff of the School of Applied Physiology as well as the patience of all the subjects that participated in these research studies. We would also like to thank Ossur, Prosthetic Design Inc., Outback Bicycles and Serotta Bicycles for their donation of prosthetic components and bicycle equipment.