
Abstract
Background: Objective design criteria for orthotic components is lacking. This paucity of data results in prescription guidelines based on assumptions or practitioners' past experience, and the potential for incorrectly designed components. The purpose of this study was to directly measure loads on the knee joint of a knee-ankle-foot orthosis.
Study design: Case series.
Case Description and Methods: Three subjects who had been prescribed a knee-ankle-foot orthosis for quadriceps weakness underwent gait analysis and orthotic upright load data collection. A load sensor to measure the three force and three moment components was used in place of the lateral knee joint while the subjects walked in three knee flexion positions.
Findings and Outcomes: Forces were highest in compression and moments were greatest in the sagittal plane. The kinetics did not increase solely with patient weight. There was substantial variability between subjects.
Conclusions: This data will help guide orthotic component design and prescription guidelines. Knowledge of loading conditions will lead to more optimal orthotic intervention for patients and increased patient satisfaction.
This study is one of the first to directly measure loads on the upright of a KAFO. These data provide objective targets for engineering design. The data from this small case series can also be used to establish guidelines for patient device selection.
Introduction
Nearly one million people in the United States use a knee-ankle-foot orthosis (KAFO). 18 Up to 80 percent of KAFO users abandon their brace and 40 percent state dissatisfaction with their orthotic device. 5,10,16 Recently, the introduction of stance control knee orthoses (SCOs) has brought the field of knee orthotics to the forefront. Because of the increased cost of a SCO compared to a conventional KAFO, it is important to investigate the use of properly sized orthotic components.
The main reasons cited for abandoning an orthotic are size, weight and bulkiness. 3 Because there is a lack of objective design standards for orthotics, it has been questioned whether braces are optimally designed for the loads a user will impart and how to obtain these target loads. 1,11,19 Over-designed components add unnecessary bulkiness to a KAFO. Manufacturers perform mechanical testing on components to ensure they meet design-load safety-testing specifications. Further, design loads are used to formulate component selection guidelines for practitioners. However, these target loads are often not available from objective tests on patients. Rather, practitioners’ experience, expertise from prosthetics, assumptions based on gait data or estimations are used to make orthosis prescription guidelines. Without objective evidence of the loads a device will experience, there is no way of knowing whether a patient is getting an optimally designed orthosis or whether a component is appropriate for the loads a particular patient will impart.
KAFO or SCO users generally have weakness that causes knee instability during stance. However, there is variability in clinical picture, demographics and physical ability. 4 Because of this variability, applying universal inclusion criteria to orthotic components may not be appropriate, especially when based on the assumptions described above. Choosing components based on practitioners’ experience or estimation may lead to a brace that is too stiff or too flexible. Using prosthetics industry standards is also unwise, as prostheses are meant to replace a missing limb and will bear complete body weight during ambulation, while an orthosis will bear only part of the load with the remainder taken up by the limb itself. Exact load sharing, however, is unknown. Intuitive assumptions are that it may vary with patient weight, height, strength and limb alignment. Basing recommendations on gait data needs similar cautions, as calculated joint loads represent the limb and orthosis as a unit. Also, gait data are typically reported as moments about the joint centre rather than the load at the orthosis. All of this could lead to over-designed components, designing to an absolute maximum load a device might see, and thus a device that may be too large for a patient’s needs. Both over- and under-designed components could have adverse effects. A brace that is too heavy or too stiff might decrease walking efficiency or increase compensatory motions, while the converse may not provide enough stability or not be durable in the long term.
Little has been done to measure loads on an orthosis used by a patient. One previous study reported on the pistoning forces in orthotic knee joints, 14 while another examined forces in a prophylactic knee brace as a measure of brace–knee motion mismatch. 17 Nearly three decades ago, Trappitt developed a transducer for measuring all components of orthotic loads 21 and referenced work as early as the 1960s, which attempted limited measurements. 13,15,20 Since then, many authors have discussed how this work is necessary and should be expanded, but few recommendations have resulted. 1,6,8 Recently, a study used a load sensor at the KAFO joint to directly measure the loads on the joint, and reiterated the importance of additional work to guide orthotic component design. 1
Until this lack of knowledge is addressed, orthotic design will continue to be based on conjecture rather than on sound engineering. As additional objective data are provided, manufacturers and practitioners can better serve patients with a device that will enhance function and lifestyle while minimizing device abandonment. The purpose of this study was to expand on previous work in directly measuring loads on a knee joint in a KAFO. By using objective measurements, we hope to provide additional guidelines for orthotic component design and device prescription criteria.
Case Description and Methods
Demographic information.

All subjects were provided with a custom thermoplastic KAFO. The lateral knee joint was replaced with a six-component load sensor (model MC2.5-6-1.2K-4670, Advanced Mechanical Technology, Inc., Watertown, MA). The sensor was oriented so that posterior, medial and compressive forces and external varus, extension and external rotation moments were positive. Adjustable mounts allowed the orthosis to be locked in varying degrees of flexion (Figure 1). The medial knee joint was a free-moving hinge. Ankle configuration was determined by the fitting orthotist to accommodate the subjects’ needs. The load sensor amplifier gains were set and output zeroed after installation in the KAFO and before donning.
Custom moulded (left) KAFO with load sensor installed in place of the lateral knee joint.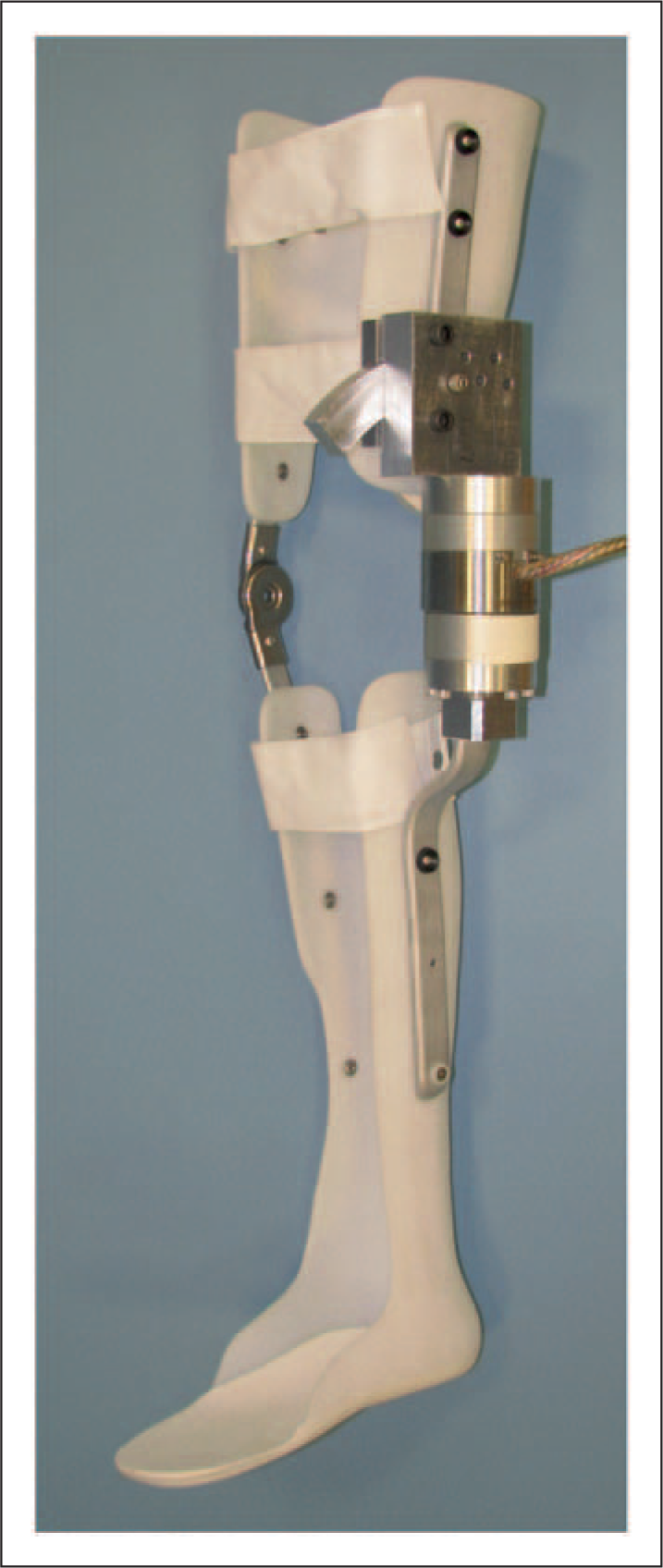
Gait and load sensor data were recorded simultaneously using commercial software (EvaRT 5.04, Motion Analysis Corporation, Santa Rosa, CA). Ground reaction forces were recorded using four force platforms (2 AMTI model BP400600, Advance Mechanical Technology, Inc., Watertown, MA and 2 Kistler model 9281B, Kistler Instrument Corp., Amherst, NY). A lower extremity marker set 9 was applied with markers on the braced limb placed directly on the KAFO. The medial and lateral knee markers defined the orthosis axis. Marker and force platform/load sensor data were collected at 60 and 600 Hz, respectively.
Data were collected with the KAFO fixed at 0, 10 and 20 degrees of flexion. Subjects performed multiple walking trials with the braced limb striking the force platforms. A minimum of three trials at each knee position were recorded. Test time per subject was approximately two hours.
Gait data knee moments were processed using commercial software (Visual 3D, C-Motion, Inc., Germantown, MD) and normalized to the gait cycle. Load sensor force and moment data were processed using custom MATLAB software (The MathWorks, Natick, MA) and normalized to the gait cycle. Forces and moments were examined in absolute values (N, Nm) as well as normalized to body mass (kg). Peak normalized forces and moments for each plane, subject and flexion condition were recorded. Averages for each parameter at each flexion position were calculated, and 95% prediction intervals were determined.
Findings and Outcomes
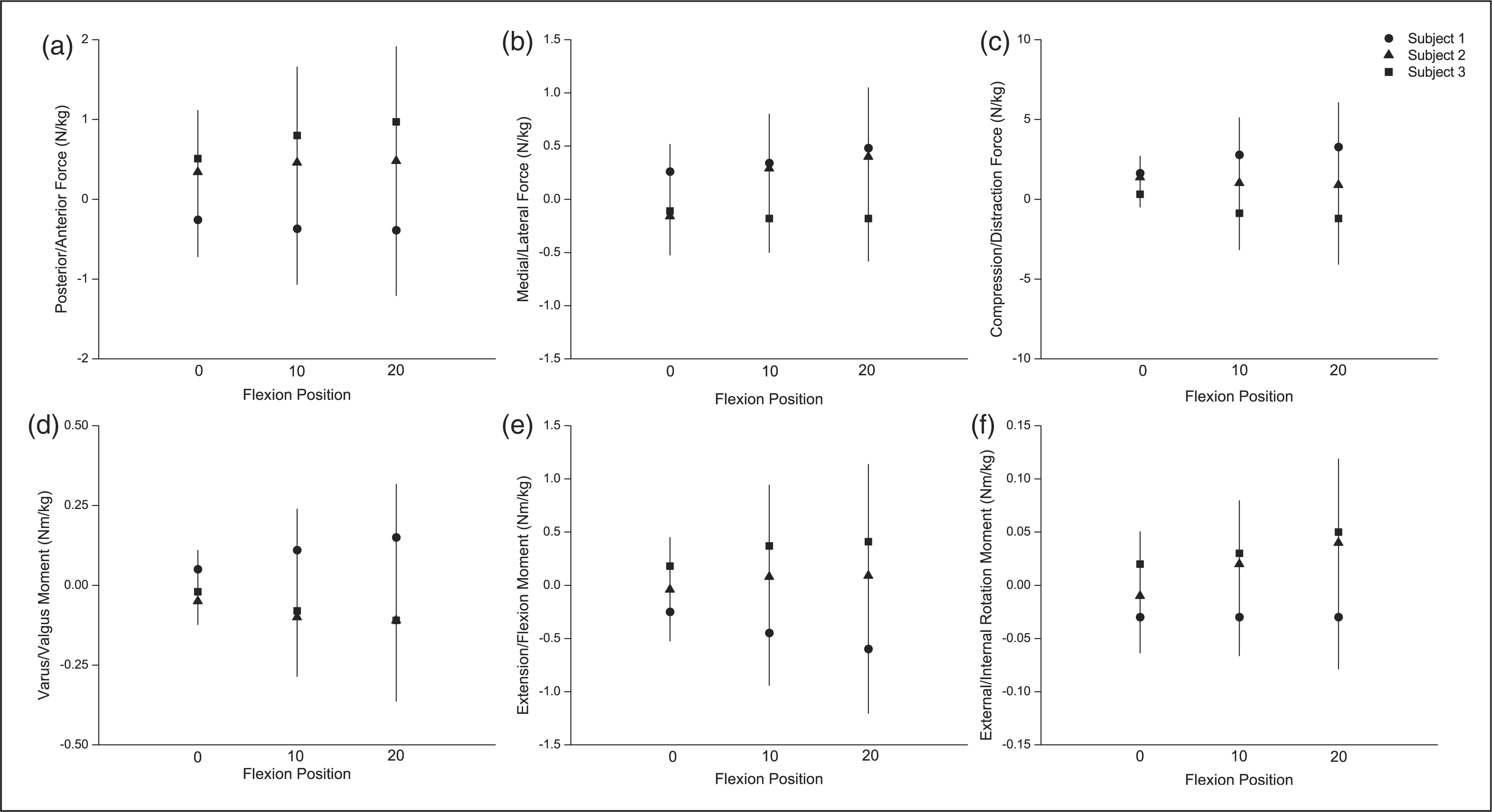
All subjects showed excellent trial-to-trial repeatability. Standard deviations over the gait cycle were less than 2 N/kg for posterior and medial forces, 6 N/kg for compression forces and 0.7 Nm/kg for all moments. However, there were differences in the patterns and magnitudes of loads between subjects (Figure 2). Examining the 95% prediction intervals (Figure 3), the variability among subjects for both forces and moments is evident. Forces were highest in compression and smallest in the medial/lateral direction. Moments were largest in the sagittal plane and smallest in the transverse plane. Magnitudes for all forces and moments increased with knee flexion.
Data for all three subjects with the brace in full extension. Individual lines are averages of a minimum of 3 trials per subject. Posterior (a), medial (b) and compressive (c) forces and external varus (d), extension (e) and external rotation (f) moment values are positive. 95% prediction intervals for posterior (a), medial (b) and compressive (c) forces and external varus (d), extension (e) and external rotation (f) moments measured on the load cell. Lines represent the prediction intervals; points represent individual subjects. Flexion position is denoted across the x-axis. For each variable, the first word in the y-axis descriptor denotes positive values.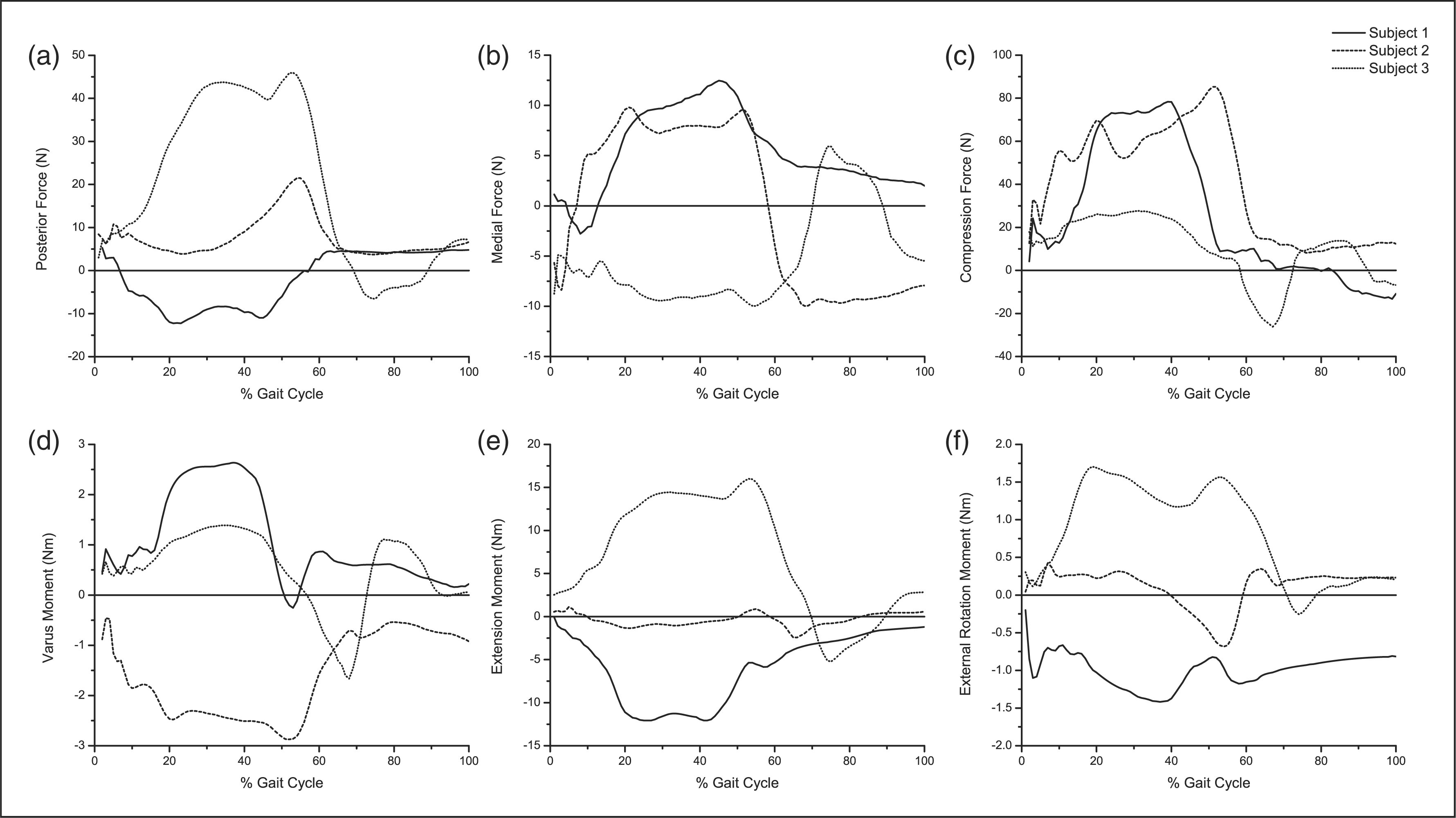
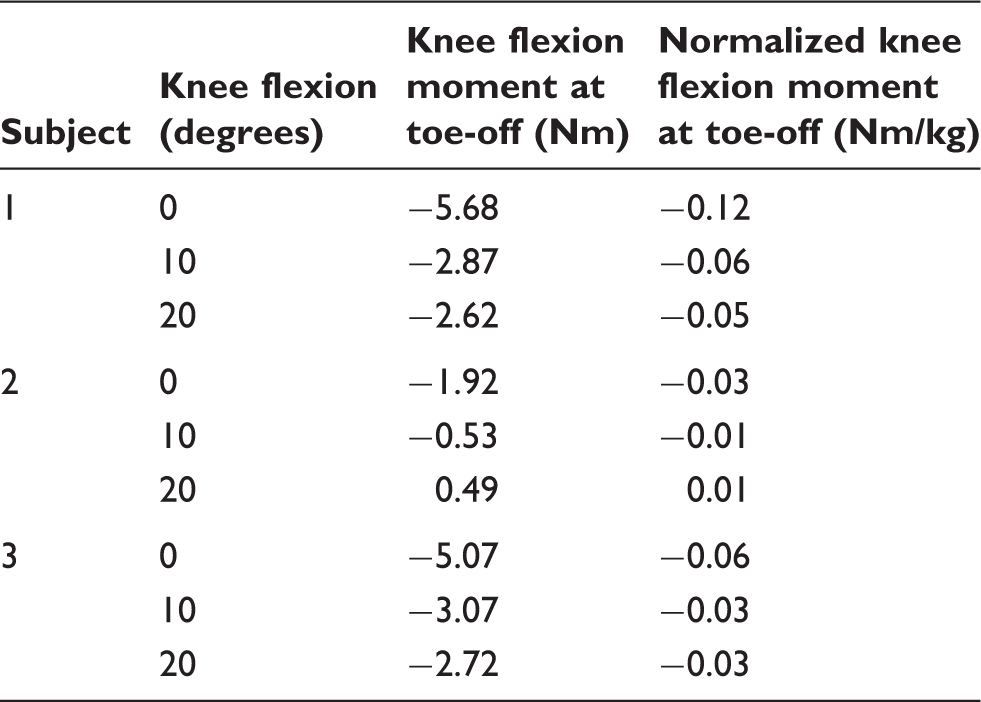
Loads on the upright did not simply increase with increasing body weight. The lightest subject had the highest compression forces, both in absolute terms and when normalized to body size. This subject also had higher sagittal and transverse moments than the middle-weight subject. Similarly, although the heaviest subject had the highest sagittal and transverse moments, he had the lowest frontal plane moments. Two of three subjects had the greatest moment in the sagittal plane, while one subject had higher moments in the frontal plane than in any other direction because of valgus instability. All subjects exhibited an external knee flexion moment at toe-off when in full extension (Table 2), ranging from 30 to 80 percent of their absolute peak sagittal moment. Sagittal moment at toe-off remained an external knee flexion moment for all but Subject 2 at 20 degrees of flexion. In all cases, sagittal peak moments measured by the load sensor were less than those calculated from the gait software (Figure 4). The most pronounced differences were in the frontal and transverse planes. Differences between the methods decreased as flexion increased.
95% prediction intervals for calculated gait software varus (a), extension (b) and external rotation (c) moments compared to measured load cell moments. Lines represent the prediction intervals; points represent individual subjects. In each pair of lines, the left line is the gait software moment and the right line is the load sensor moment. Flexion position is denoted across the x-axis. Positive values are external varus, extension and external rotation moments. Sagittal plane moments at toe-off. External extension moments are positive. All moments are external knee flexion moments, except for subject 2 at 20-degree knee flexion.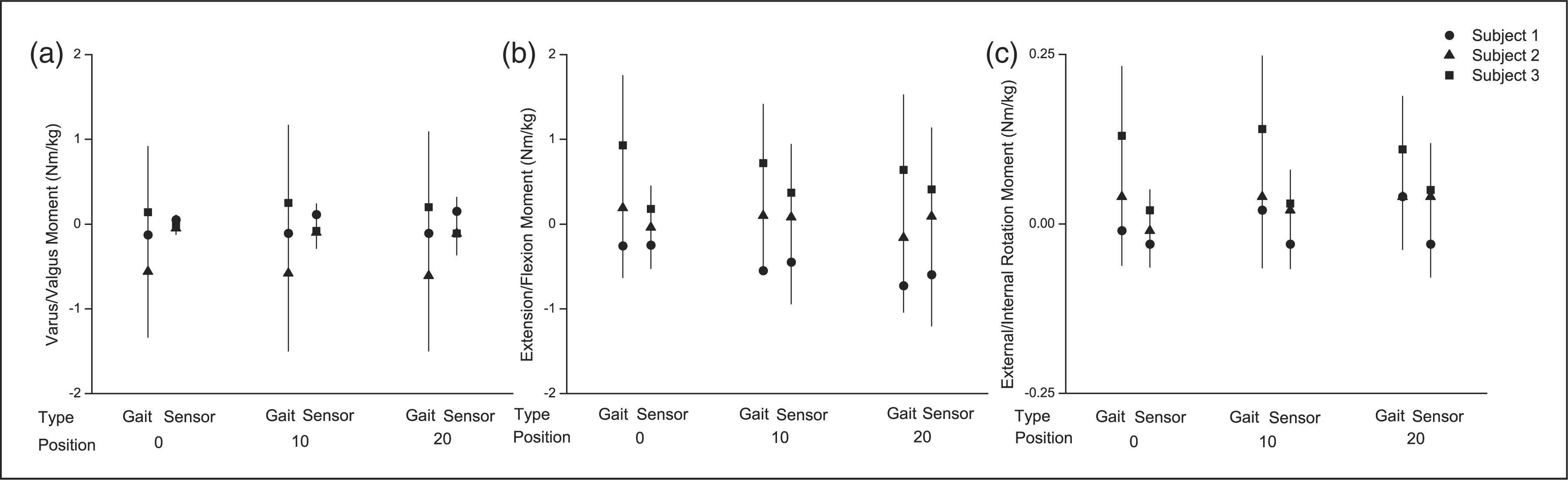
Discussion
This study is one of the first to directly measure loads on the upright of a KAFO. With the recent popularity of SCOs and re-emergence of interest in KAFOs, this study increases the objective joint load data published, which is of great importance. Directly measuring loads on KAFO uprights gives objective criteria that will aid engineering design. As devices become more complex and expensive, this study will help provide objective data for patient device selection.
Two of three subjects had conditions where the frontal and transverse load sensor moments were greater than those calculated by the knee joint centre of the biomechanical model used in the software. This is because the axis of the load sensor was not coincident with the gait software knee joint centre. No correction was applied to make the axes coincident because the goal was to compare the loads measured at the upright to those obtained with standard gait analysis methods and assumptions.
Absolute peak forces and moments varied among the subjects tested but were not related solely to body weight, as the lightest subject demonstrated some of the higher compression forces and sagittal moments. Similarly, the middle-weight subject exhibited higher absolute frontal moments because of frontal plane instability. These data provide evidence that orthotic prescriptions cannot be based on body weight alone. When walking in a semi-flexed position, greater absolute peak loads were seen. However, the increases were not necessarily linear with increasing flexion. These differences may be due to variations in strength across subjects. Regardless of strength, all subjects were prescribed a KAFO and represented the variability in patients that occurs. Some subjects exhibited sagittal moments that would tend to collapse the knee, while others showed moments that would extend the joint. This could be for a variety of reasons, such as their preferred flexion during walking or residual strength level. When normalized to body weight, peak forces and moments agree with previous work. 1,21 The absolute extrema of the 95% prediction intervals at full extension from this study match reasonably well with the values reported by Andrysek, the work most similar to the current study. 1
Few standards for design and testing of orthotic components exist. The Japanese Industrial Standard 2 proposes an endurance test for KAFO knee joints of a 10 Nm torsional moment and 50 Nm sagittal bending moment to simulate stance phase of gait. Comparisons of this study’s data to the loads recommended by the Standard are possible by taking the absolute maximum normalized moment from the 95% prediction intervals. Assuming a 100 kg patient, a number often cited as the weight limit for orthotic products, one can obtain example loads. While the values for this study are within the proposed endurance test loads for torsion, the Standard load is equalled at 0 degrees and surpassed at 10 and 20 degrees for sagittal moment. Heavier patients or higher demand walking conditions could impart even higher loads, so devices designed to this standard may fail. This shows the importance of basing design criteria on objective measurements.
Of particular note for SCO design are the loads at toe-off. All subjects exhibited an external knee flexion moment at toe-off when in full extension. Sagittal moments at toe-off in the flexed conditions were smaller, but in nearly all cases remained an external knee flexion moment. Previous work 7 showed similar joint loading at toe-off. For most currently available SCOs, this load at toe-off would bind the release mechanism. These data show the importance of considering a patient’s gait when choosing a device, especially a more expensive SCO. Some patients can learn to unload the joint for release, or the brace can be built with offsets at the knee to help achieve this unloading, but these solutions add effort and money to a fitting that is already more complex than a standard KAFO.
Measured moment peaks were less than those calculated from the gait software. This supports the idea that an orthosis component will only bear part of the total load, with the remainder being borne by the limb. The difference between the load sensor and gait moments varied from person to person. This may be due to residual strength and how much a subject relies on the brace, to placement of the knee axis of the orthosis, or to assumptions made about the placement of the knee axis in the gait software, which is known to affect moment calculations. The most pronounced differences between the calculated and measured moments were in the frontal and transverse planes, perhaps because the load sensor was offset laterally from the joint centre used for gait moment calculations. Orthosis sagittal plane moments were also overestimated by the gait software, especially in the flexed positions. These differences reinforce the importance of not basing orthotic device design simply on gait lab data. It is also important to note that the prediction interval bands for nearly all parameters cross zero, again indicating the variability among subjects, and that force direction may not always be in the expected direction.
This study has several limitations. Only three subjects were measured. Different subjects as well as variations in fit, material choice, ankle joint choice or other modifications to the KAFO could lead to different peak loads. However, the three subjects were diverse in their clinical presentation in terms of strength, alignment, diagnosis and current orthosis use. Therefore, these data are a good representation of patient variability and the range of possible loads that could be encountered. All loads were measured in a locked KAFO. Loads may be somewhat different in a free knee orthosis or SCO. Only the lateral joint of the KAFO was instrumented. The size of the load sensor used in this study precluded installation of a medial sensor. An instrumented medial upright would likely show similar results, as in previous work. 21 We unsuccessfully attempted to remove the medial upright in an effort to measure loads in a single upright design. The thermoplastic cuffs proved too flexible to provide a safe testing environment, and the data were deemed unreliable because of excess twisting of the orthosis relative to the leg. Future attempts at single upright data collections would be possible with stiffer constructs. This investigation only examined level walking, while orthotic components could endure higher forces from tripping and stumbling. However, such conditions would be unsafe without more safety precautions than were undertaken in this study. Finally, the load sensor and fixtures added 70% more weight to the base KAFO. Knee braces are already heavy, a known factor leading to abandonment, 3 and the added weight may have affected walking patterns. However, the additional weight is likely not greater than some of the current SCO designs, and therefore not unreasonable.
These data are significant for several reasons. They provide a substantial addition to the knowledge pertaining to knee orthosis loads during gait. Objective data such as these will provide an information base of loads that a device actually endures, leading to appropriate design standards for orthotics. Most current KAFO uprights are designed to support loads much greater than seen in this study, 12 and manufacturers frequently apply a factor of safety which adds more bulkiness and weight to the orthosis. Further, SCOs are gaining in popularity, but have an increased cost in time and money to both practitioner and patient. Most SCOs require an extension moment at toe-off to release, yet eight of nine conditions tested in this study showed a flexion moment. These objective data show that not all SCOs will work for all patients, and highlight the importance of understanding the fitting requirements of a particular design as well as the patient’s gait before choosing a device. Because of the many factors that could affect the loads on a device, these results should not be taken in isolation. Future work is warranted to further investigate loads imparted on a KAFO by different patient populations or brace configurations. Aside from providing the aforementioned objective design specifications, this could also allow clinicians to better match the patient profile to a matrix of available components.
Conclusion
This study shows the importance of considering a patient’s entire clinical picture when choosing a device. Loads did not necessarily increase with body weight. The presence of frontal plane malalignment or stance flexion adds to the total load on the joint. As greater knowledge is obtained, it will be possible to design an orthosis that is neither too flexible and liable to fail, nor too stiff and likely to be abandoned. By using objective evidence, the practitioner may be more effective in fitting and choosing devices for patients. Finally, manufacturers will be able to provide better guidelines for their products, and the patient will receive a brace better fitted to their functional needs.
Footnotes
Acknowledgments
Special thanks to Krista Coleman Wood, Diane Serfling, Meegan Van Straaten and Paul Kane.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
Kenton Kaufman has two patents on stance control orthoses that have been licensed to a commercial company. A product is on the market from which he receives royalties.