
Abstract
Background:
Spina bifida is an uncommon cause for lower limb amputation. The causes and level of amputation and mobility outcome for these patients have not been reported previously.
Case description:
To identify the causes and level of amputation and the mobility outcome for amputee patients with spina bifida.
Study design:
Retrospective case series.
Methods:
Chart review of patients identified by computer as having an amputation secondary to neurological or congenital cause. Additional patients identified from the Regional Spina Bifida Medical Clinic. Demographics, cause and level of mobility pre- and post-amputation recorded from the prosthetic notes.
Findings:
In total, 16 patients were identified who had a diagnosis of spina bifida and a lower limb amputation. Mean age at the time of amputation was 28.5 years. In total, 15 patients had a transtibial amputation. In total, 14 patients post-amputation were able to maintain their mobility, wheelchair or walking, without any change in type of aid needed.
Conclusion:
Patients with spina bifida appear to require lower limb amputation at a younger age than patients with peripheral vascular disease. Almost all patients had prior chronic skin infection/osteomyelitis as precursors for amputation. The most common level for amputation was transtibial. Mobility was maintained for all patients, albeit for two in a more supported way.
Clinical relevance
Spina bifida is an uncommon reason for amputation. Patients, are often younger and medically complicated. Chronic skin ulceration, was the most common indication for amputation. Wheelchair or walking ambulance was maintained at the same level for most patients.
Background
Spina bifida is an uncommon cause for lower limb amputation.
It is a congenital malformation of the neural tube in which there is failure of fusing of the neural folds and vertebral arch by the 28th day of conception. It can result in varying degrees of lower limb and upper limb weakness and loss of sensation, including bowel and bladder dysfunction. Genetic predisposition with environmental precipitants accounts for most of the risk of neural tube defects, and primary prevention with folic acid fortification of food has been introduced in some countries as mandatory, although not in the United Kingdom yet. 1 Spina bifida can be a devastating condition with wide-reaching consequences for mobility, general health and lower and upper limb strength. 2
According to the Statistical Monitoring Report of the European Surveillance of Congenital Anomalies (EUROCAT), 3 the incidence of spina bifida has reduced by 10% over the last 10 years. The survival rate of patients with spina bifida has on the other hand been increasing due to the technological and therapeutic advances of modern paediatric care. 4
In the United Kingdom, there are on average 10 referrals each year to rehabilitation centres for patients with spina bifida, who have required a lower limb amputation and are considered possibly able to benefit from a lower limb prosthesis. 5
To our knowledge, this is the first study of patients with spina bifida who have required lower limb amputation in the United Kingdom.
The aim of this study is to define the causes and most common level of amputation and the mobility outcome for amputee patients with spina bifida.
Methods
The Amputee Rehabilitation Centre in Belfast is the only prosthetic centre in Northern Ireland. Patient referrals are coded on computer according to diagnosis, and basic demographics are also recorded. A computerized system has been in use since 1995.
Using Clinical Information Management System (CIMS) to generate patient names, all patient names in December 2014 which were coded ‘neurological’ or ‘congenital’ as a cause for lower limb amputation were collated. The corresponding prosthetic charts were then reviewed to confirm if the patient did have a diagnosis of spina bifida. In total, 13 patients were identified. In addition, prosthetists and physiotherapists at the centre were asked whether they were aware of any additional patients who had not been recorded on the initial computer-generated list, prior to 1995. One further patient was identified. Cross checking for additional names was undertaken through the Regional Spina Bifida Medical Clinic notes. This clinic is a review clinic for all patients who have spina bifida in Northern Ireland with or without coexistent limb amputation. Two further patients were identified. In total, 16 patients were identified. Due to the negligible risk to patients, ethical approval was not sought.
From the medical/prosthetic notes demographics, the documented level of spina bifida lesion, cause of amputation, mobility level pre-amputation and 1-year post-amputation were recorded.
Findings
In total, 16 patients were identified, who had both a diagnosis of spina bifida and a lower limb amputation, 6 were female and 10 were male. In total, 12 had a unilateral transtibial amputation. Three patients had bilateral transtibial amputation, two female and one male – one had both amputations performed on the same day, one had the second transtibial amputation performed 4 months later and one had a second transtibial amputation performed 6 months later. One patient had a through-knee amputation.
The mean age at time of amputation was 28.5 years, the age range was 6–58 years and the standard deviation was 11.68.
The clinical indication for amputation for eight patients was ongoing skin ulceration of the foot. Seven patients had osteomyelitis along with skin ulceration of the foot and one had calcaneal and tibial deformity at birth and required through-knee amputation to allow mobilization with a prosthesis.
Mobility pre- and post-lower limb amputation correlated against the level of meningomyelocele is shown in Figure 1.
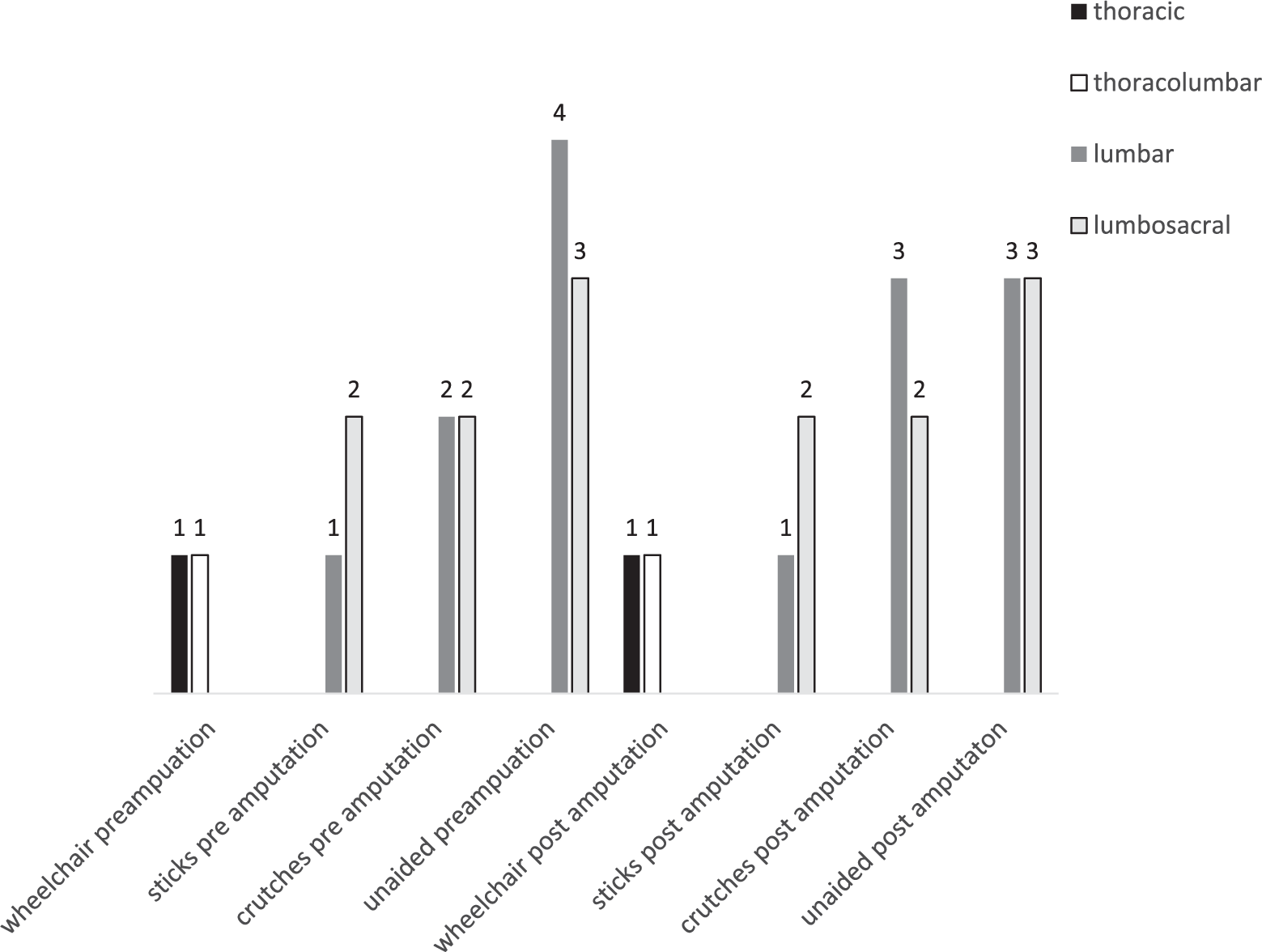
Level of spina bifida compared against mobility 1 year prior to amputation and mobility >1 year post-lower limb amputation.
In total, 12 patients post-amputation were able to maintain their mobility without any change in type of aid needed: 6 patients continued to be able to walk independent of walking aids, 2 of whom had bilateral transtibial amputations.
Two patients, who had prior to amputation needed two sticks as aids for walking, continued to need sticks post-amputation. Four patients, who prior to amputation had required crutches to mobilize, continued to need crutches post-amputation.
Both patients who were wheelchair ambulant for mobility prior to amputation and patients who subsequently needed a unilateral transtibial amputation and bilateral transtibial amputations, at 1 year post-amputation continued to be able to transfer independently. Both relied on the prosthesis to prop and provide leverage for transfers.
One patient who prior to amputation had walked unaided, required two sticks to mobilize post-amputation. One who had prior to amputation used two sticks, needed crutches post-amputation.
Discussion
Patients with spina bifida who ultimately require a lower limb amputation are uncommon. They do however represent a cohort of patients who are most likely complex both in neurological deficits and in medical issues, necessitating a multifaceted approach by the multidisciplinary team to ensure the best outcome for the patient. 6
Patients with spina bifida, according to the level of the myelomeningocele, can be prone to skin damage due to a combination of neurological anaesthesia and also lymphedema. Lymphedema is chronic swelling of the soft tissues due to accumulation of interstitial fluid and is 100 times greater in this population than in the general population. 7 Skin ulceration with or without osteomyelitis was the most common cause for amputation in our patients. Persistent infection, with or without osteomyelitis, refractory to conservative management is an indication to consider amputation, with the goal of maintaining reasonable mobility. Care of the foot and consideration of properly fitting footwear are likely to be very important in the prevention of foot/skin problems for these patients although research is lacking. However, parallels could be drawn with patients who have diabetes and neuropathy where footwear and footcare are recognized as essential. 8
Most of our patient groups required amputation before the age of 35 years. This is important to be aware of when counselling patients with spina bifida who are undergoing persistent foot ulceration with little or no progress in healing. In total, 15 patients had a transtibial amputation. This level of amputation will afford better function for walking as compared to a more proximal amputation. Two of the 16 patients progressed to bilateral lower limb amputation within 4–6 months of having the initial lower limb amputation. None of the patients underwent a partial foot amputation although this is sometimes performed in patients with spina bifida. 9
The neurological level of the spina bifida lesion was gleaned from the medical notes and therefore may have been reported by the patient and may not have been confirmed by physical examination. This allows for the possibility that some of the neurological levels reported by the patients in this study may not be accurate.
Younger age at amputation and the transtibial level of amputation are likely the major reasons for the relatively preserved ambulation in many of these patients.
For patients with spina bifida, who have not had a lower limb amputation, the neurological level of the spinal defect and the ability to be walking ambulant can usually be predicted.10,11 Samuelsson found that 80% of patients with L5 defects were walking ambulant and that 100% of patients with sacral defects were walking ambulant.
The ability to mobilise with a lower limb prosthesis for patients with spina bifida has not been previously recorded in literature. In our study, numbers are small but Figure 1 generally reflects that found in Samuelsson’s study with the wheelchair users having higher levels of spinal cord defect than those who could walk aided or unaided post-amputation.
In this review, all patients who progressed to amputation continued to be able to walk with prosthetic replacement or transfer, although two required more support for walking sticks or crutches. It is recognized that for patients who are wheelchair ambulant restoration of side-to-side transfers can be made easier by wearing a prosthesis, thus weight and balance are somewhat restored to what it would have been prior to amputation. 12 Two wheelchair ambulant patients with spina bifida after amputation benefited from a prosthesis: both patients found that the prosthesis restored their weight distribution when attempting to transfer.
This study is small and therefore care must be taken when drawing conclusions; in addition, it was beyond the scope of this review to investigate if there were changes in speed of walking and speed of transfers after amputation. However, as so few amputations are performed each year for this condition in the United Kingdom, this is a relatively sizeable number and it highlights some important findings.
Conclusion
Patients with spina bifida who have foot ulceration problems appear to require lower limb amputation at a younger age than patients with established peripheral vascular disease and diabetes mellitus. In almost all cases, the patients had prior chronic skin infection or osteomyelitis as precursors for amputation. The most common level for amputation was transtibial. Mobility was maintained for all patients albeit in a more supported way, for example, crutches instead of sticks. Two wheelchair users also benefited from a prosthesis for transfers.
Footnotes
Acknowledgements
The author thanks Dr Suzanne Connolly, Staff Grade in Rehabilitation Medicine who cross referenced patient names with attendees at the Regional Spina Bifida Clinic. Thanks also to Dr John McCann Consultant in Rehabilitation Medicine who’s idea stimulated this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.