
Abstract
Background:
Lower limb amputees are at higher risk of cardiovascular disease compared to non-amputees. Dietary intake, a major determinant of cardiovascular disease risk, has not previously been studied in this group.
Objective:
The aim of this study was to investigate dietary intakes and prevalence of overweight/obesity in adult lower limb amputees.
Study design:
A cross-sectional survey was used to investigate the dietary intake and prevalence of overweight/obesity in adults with lower limb amputations living in the United Kingdom.
Method:
Dietary intakes of male adult lower limb amputees (n = 46, non-dysvascular) were assessed using food frequency questionnaires and results were compared to dietary reference values in the United Kingdom. Prevalence of overweight/obesity was assessed through body mass index and waist-to-hip ratio and compared to the general population according to the Health Survey for England 2011.
Results:
Dietary intake risk factors for cardiovascular disease such as sugars (22.01%), total fat (34.87%), saturated fat (12.72%) and sodium (2660.10 mg/day) were significantly higher (p < 0.001, p < 0.001, p = 0.043, p < 0.001; p < 0.001; respectively) than the dietary reference values. A high prevalence (82.8%) of overweight/obesity was found with a significantly higher body mass index and waist-to-hip ratio (p = 0.027; p = 0.001; respectively) compared to the Health Survey for England 2011.
Conclusion:
High intakes of sugars, dietary fats, sugars and salts, combined with high prevalence of overweight/obesity observed in lower limb amputees are concerning. These findings suggest that greater emphasis on dietary intakes should be considered for rehabilitation programmes.
Clinical relevance
Findings highlight poor dietary habits in lower limb amputees with respect to fat, sugar and salt intake, also high levels of overweight/obesity. Considering greater emphasis on dietary intake and including lifestyle changing interventions in rehabilitation programmes for lower limb amputees may lower the risk of obesity and CVD.
Keywords
Background
Having to undergo a lower limb amputation (LLA) is a life-changing experience, and the degree to which a patient’s health and quality of life is affected depends on a combination of physical, psychological and social factors including the patient’s age, cause and level of amputation, comorbidities (such as cardiovascular disease (CVD), diabetes mellitus or arthritis), depression, anxiety or social isolation.1,2
LLAs are often categorised as vascular related (dysvascular) and non-dysvascular. Peripheral arterial disease in association with type 2 diabetes mellitus is the main cause of dysvascular LLA, 3 whereas non-dysvascular LLAs are mainly due to trauma or malignancy. 4 The main risk factors commonly described to increase the risk of CVD in dysvascular amputees include older age and male gender combined with a low physical activity level and comorbidities such as diabetes, hypertension, obesity and hyperlipidaemia.5–7 In addition, several factors have been suggested to have an effect on the arterial system leading to obstructed arterial flow that potentially results in CVD in non-dysvascular amputees, these include age at amputation, psychological stress, hemodynamic consequences in association with level of amputation, hyperinsulinaemia and a sedentary lifestyle and obesity.8–12
It was suggested that obesity increases the risk of LLA and potentially increases the risk of additional weight gain post-amputation which may result in further comorbidities, and LLA may also lead to obesity post-amputation in patients with a healthy weight pre-amputation. 13 In general, individuals with physical disabilities are at higher risk of obesity and subsequently at increased risk of additional comorbidities and lower limb amputees are no exceptions.13–17 The relationship between obesity and physical impairment may also impose a vicious cycle on the disabled individual and therefore further reduce the physical functioning and independence. 16
Previous research gave convincing evidence that lower limb amputees are at increased risk of obesity and CVD.5,10,14,17,18 However, to the authors’ knowledge, no research has been carried out on the dietary habits within this population and a subsequent link to the increased risk of obesity and CVD.
The aim of this study was to investigate the dietary intakes and the prevalence of overweight/obesity as potential risk factors for increased risk of CVD within the adult population with LLAs with the following hypotheses: (1) dietary intakes in amputees are not in line with recommended dietary reference values (DRVs) in the United Kingdom and (2) the prevalence of overweight/obesity in lower limb amputees is higher compared to the general population.
Methods
Study design
This was a cross-sectional survey investigating dietary intake and prevalence of overweight/obesity in adults with LLAs living in the United Kingdom.
Recruitment of participants
A convenience sample was recruited from amputee charity events (LimbPower and Limbless Association), both of which promote sport and fitness to the limb-loss community and one NHS Outpatient Rehabilitation Centre for amputees (Bowley Close Rehabilitation Centre). Participants were approached in person and instructions were given on how to complete the food frequency questionnaire (FFQ) independently. Inclusion criteria for major LLA were transtibial amputation, transfemoral amputation and knee-disarticulation due to any cause. Exclusion criteria were (1) minor amputations such as toes, partial foot or foot, because these were not previously reported to be associated with increased risk of CVD; (2) pregnancy; and (3) participants who suffer from a health condition that may necessitate a specific diet such as the exclusion or severe restriction of particular nutrients (i.e. coeliac disease or Phenylketonuria). Participants were offered free nutritional advice by a nutritionist registered with the Association for Nutrition.
Ethical approval
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Ethic Committee of the University of Roehampton (reference no. LSC 14/099), the NHS Research Ethics Committees (REC, reference no. 14/NS009) and the NHS Research and Development department at Guy’s and St Thomas’ NHS Foundation Trust (registration no. RJ114/N196). Written informed consent was obtained from all participants.
Survey design
The questionnaire was divided into three sections. The first section addressed the participants’ demographics and questions in relation to their amputation/disability. The second and third sections consisted of a physical activity questionnaire and an FFQ, respectively. The physical activity questionnaire was assessed in accordance with the guidelines published by the Department of Health for the General Practice Physical Activity Questionnaire 19 taking into account work and leisure time activity, and also non-work-related screen time; data were categorised as follows: (1) inactive, (2) moderately inactive, (3) moderately active and (4) active. The FFQ was a copy of the semi-quantitative FFQ used in the ‘European Prospective Investigation of Cancer’ (EPIC) Norfolk study 20 consisting of 130 items commonly consumed in the United Kingdom and was based on medium servings or standardised units (i.e. pints and teaspoon).
Anthropometric measurements of waist and hip circumferences were taken using a non-stretchable tape measuring around their waist and hips while wearing thin clothing and the tape pulled tight enough to compensate for the added girth of clothing. For those participants who were not able to remove their prosthetic limb, hip circumferences were taken including the socket of a prosthetic limb (i.e. transfemoral amputation or knee disarticulation) and adjusted by a subtraction of 4.5 cm. This value was derived from a pilot study measuring transfemoral amputees with and without wearing their prosthetic limb (socket). For those amputees, the values were between 4.2 and 4.6 cm and the mean was 4.5 cm. All measurements were taken twice and the mean was used for data analyses.
The body mass index (BMI) (body weight in kilogrammes divided by height in metre squared (kg/m2)) was calculated using touchcalc®, an online tool 21 that adjusts BMI according to the level of amputation. The formula applied by Fadern 21 was adapted from a formula for correcting body weight in amputees used by several previous studies.22–24 Overweight and obesity were categorised as BMI of 25–29.9 kg/m2 and BMI ⩾30 kg/m2, respectively. Levels of waist-to-hip ratio (WHR) and waist circumference (WC) published in the Health Survey for England 2011 (HSE) 25 were used as reference values; WHR levels as indicator for increased risk of CVD were set at 0.9 for men and 0.8 for women. WC levels as indicator of abdominal obesity and high risk of CVD were categorised for men as 94.0–101.9 cm and for women as 80.0–87.9 cm, and abdominal obesity and very high risk of CVD were categorised for men as >102.0 cm and for women as >88.0 cm. 25
The physical activity questionnaire was assessed in accordance with the guidelines published by the Department of Health and Social Care 19 taking into account work and leisure time activity, and also non-work-related screen time. Data were categorised as (1) inactive, (2) moderately inactive, (3) moderately active and (4) active.
The FFQ was analysed using the FETA (Φετα) software. 26 DRVs were used as reference values for the analyses of estimated dietary intakes, such as the reference value for total energy published by the Scientific Advisory Committee on Nutrition (SACN), 27 the reference values for macro- and micro-nutrients published by the Department of Health 28 and the World Health Organization (WHO) 29 recommendation for fruit and vegetable intake.
Statistical analysis
Statistical analyses were performed using SPSS 21 software. Descriptive statistics were used to test for frequencies such as numbers (n), valid percentages (%) and descriptive characteristics in the form of mean and standard deviation (SD); data were tested for normality using Kolmogorov–Smirnov test. One-sample and paired-sample t-tests were performed to compare the dietary intakes of the study population with the DRVs and to compare the participants’ level of overweight/obesity with the means of the general population according to the results published in the HSE. 25 Pearson’s correlation coefficient statistics were used to assess the association between BMI, WC, WHR, time since LLA, self-reported duration of prosthetic limb use in hours per day and estimated mean dietary intakes per day. The level of significance was set at p < 0.05.
Results
Study sample characteristics
A total of 63 participants were recruited, but due to limited numbers in dysvascular and female participants (Figure 1), further data analyses were performed on data of male non-dysvascular amputees only (n = 46) (Supplementary Tables 1–3).
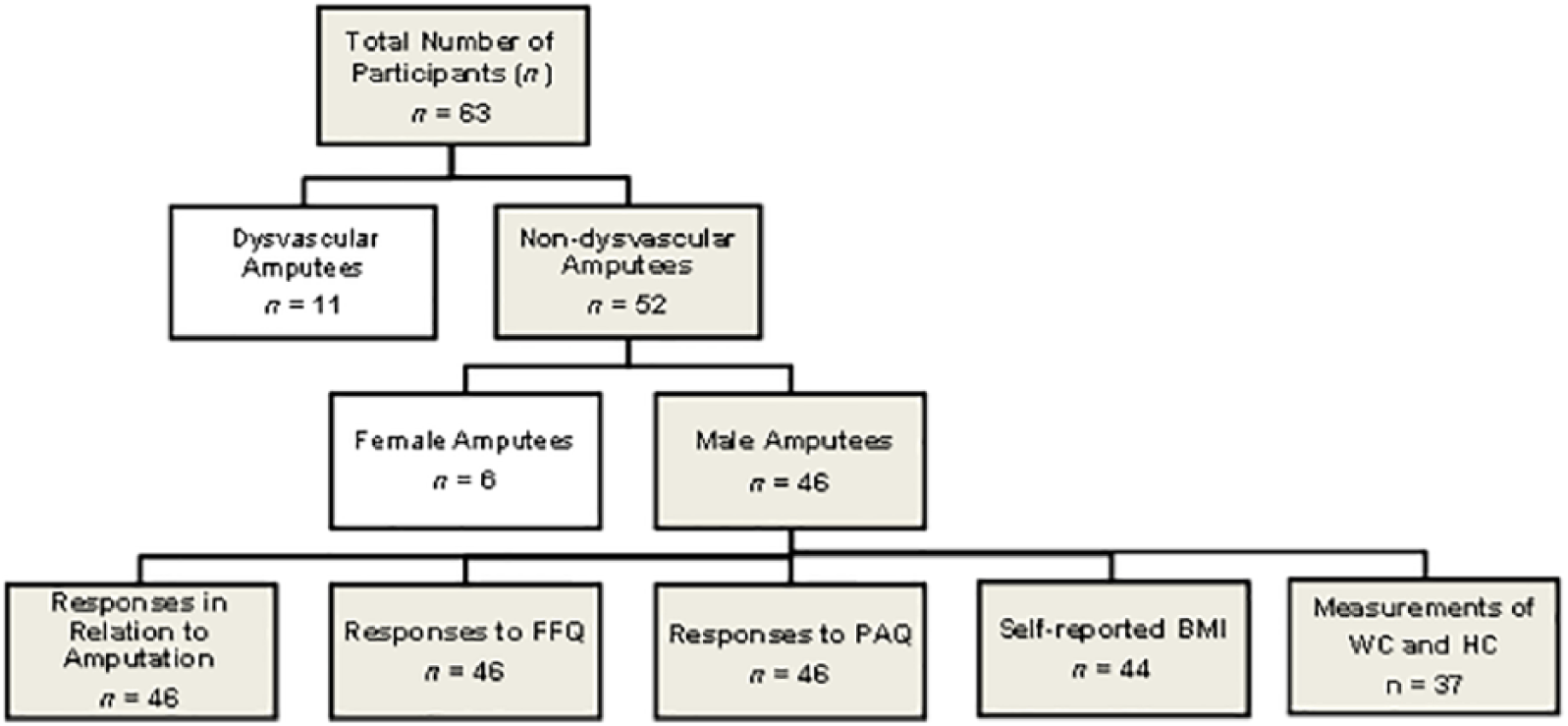
Recruitment numbers and number of participant responses to individual sections of the survey. Dysvascular and female amputees excluded from further data analyses due to low number of participants.
The majority of participants reported a white ethnic background (80.4%) with a mean age of 46 (SD = 14.57) years. Further descriptive characteristics (Table 1) include the following: participants were predominantly unilateral amputees (93.5%) and the average time since participants became amputees were 14 (SD = 14.58) years. The reported average daily use of a prosthetic limb was 13.3 (SD = 3.48) hours per day.
Descriptive characteristics of whole sample (n = 46) with majority of responses in frequency of valid responses, percentage of number of respondents to individual question and valid percentage.
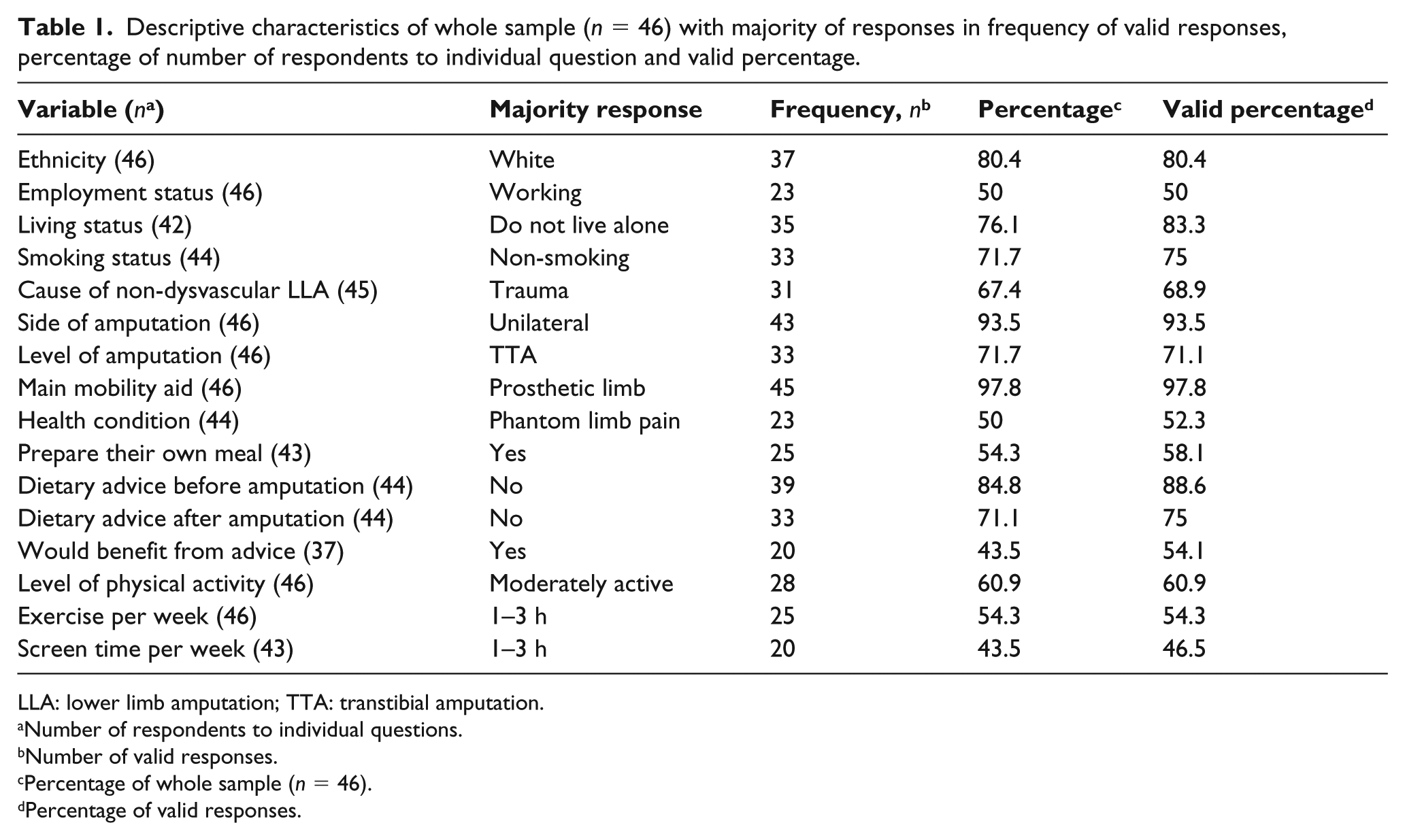
LLA: lower limb amputation; TTA: transtibial amputation.
Number of respondents to individual questions.
Number of valid responses.
Percentage of whole sample (n = 46).
Percentage of valid responses.
Dietary intakes
Dietary intakes of the participants differed significantly from the DRVs (Table 2). The estimated mean daily intakes of carbohydrates (43.35%) and non-starch polysaccharides (15.29 g) were significantly lower than the estimated average requirements. In contrast, the daily intakes of non-milk extrinsic sugars (NMES, 22.01%), total fat (34.87%) and saturated fatty acids (SFA, 12.72%) were significantly higher than the estimated average requirements. The estimated intakes of protein (84.16 g) and sodium (2660.10 mg) were also significantly higher than the recommended nutrient intake. The daily consumption of fruit and vegetables showed no significant difference to the recommendation for the United Kingdom.
Differences of estimated mean dietary intakes (total energy (MJ), macro-nutrients (g or %), fruit and vegetable (g) and sodium (mg)) per day (d) between whole sample (n = 46) and the DRVs in the United Kingdom; statistical test included paired-sample and one-sample t-tests.
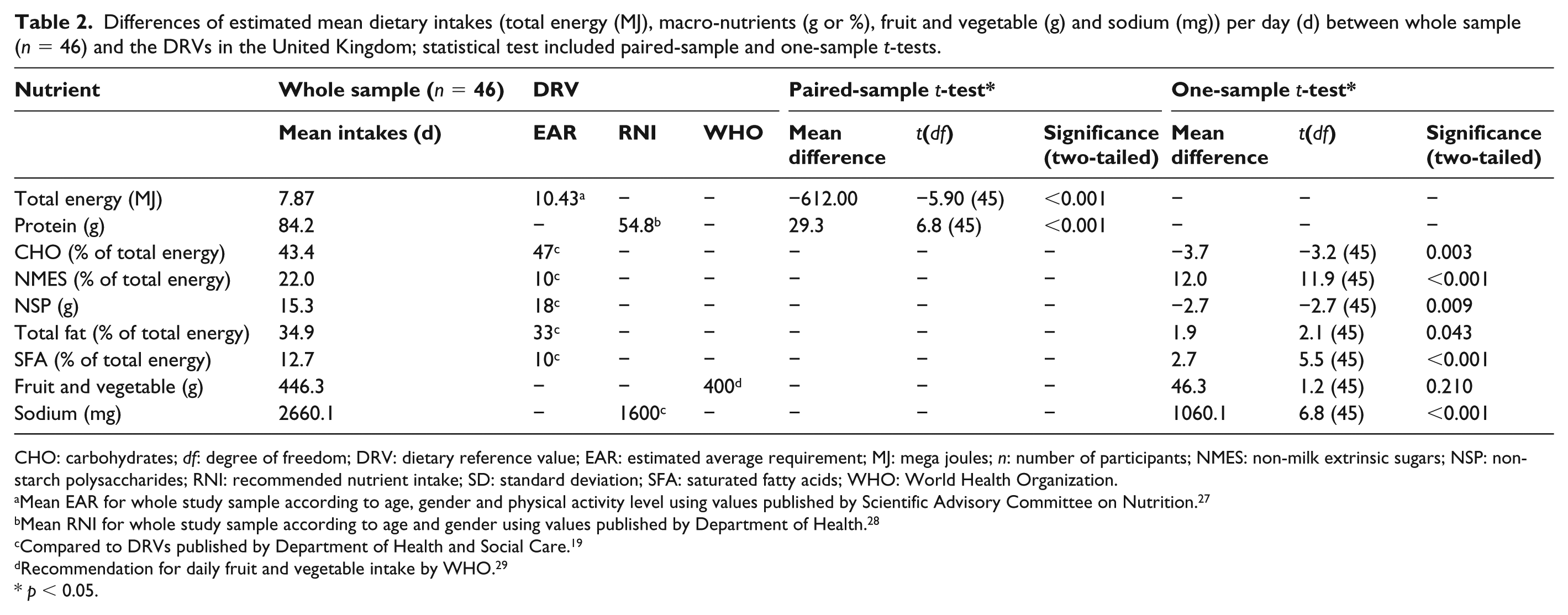
CHO: carbohydrates; df: degree of freedom; DRV: dietary reference value; EAR: estimated average requirement; MJ: mega joules; n: number of participants; NMES: non-milk extrinsic sugars; NSP: non-starch polysaccharides; RNI: recommended nutrient intake; SD: standard deviation; SFA: saturated fatty acids; WHO: World Health Organization.
Mean EAR for whole study sample according to age, gender and physical activity level using values published by Scientific Advisory Committee on Nutrition. 27
Mean RNI for whole study sample according to age and gender using values published by Department of Health. 28
Compared to DRVs published by Department of Health and Social Care. 19
Recommendation for daily fruit and vegetable intake by WHO. 29
p < 0.05.
Prevalence of overweight/obesity
The mean BMI was 28.81 (SD = 5.15) kg/m2, the mean WC was 96.42 (SD = 14.28) cm and the mean WHR was 0.96 (SD = 0.10). Results showed that 54.5% of the participants fell within the overweight BMI category and 29.5% within the obese category. Analysis of WC revealed that 27.0% fell within the high risk and 35.1% within the very high-risk category for CVD and abdominal obesity; the analysis of the WHR showed that 75.7% were within the high-risk category of CVD. The comparison of the participants’ body composition with the mean values taken from HSE 25 (Table 3) revealed that the participants’ average BMI and WHR were significantly higher than the mean for the general male population; however, no significant difference was found in WC.
Differences of mean BMI (kg/m2), waist circumference (cm) and WHR between the study sample and the HSE. 25
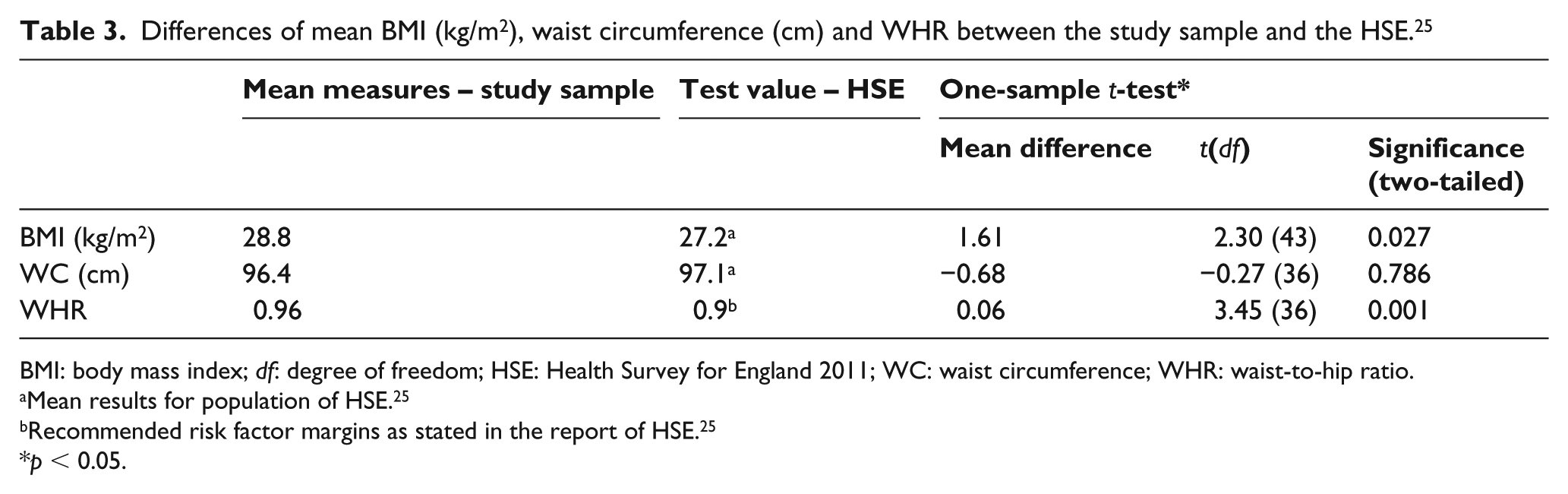
BMI: body mass index; df: degree of freedom; HSE: Health Survey for England 2011; WC: waist circumference; WHR: waist-to-hip ratio.
Mean results for population of HSE. 25
Recommended risk factor margins as stated in the report of HSE. 25
p < 0.05.
The results of Pearson’s correlation coefficient (r) test indicated a significant positive correlation between BMI and WC (r = 0.667, n = 37, p < 0.01), between BMI and WHR (r = 0.333, n = 37, p < 0.05) and between WC and WHR (r = 0.592, n = 49, p < 0.01). Moreover, a significant positive correlation was found between BMI and estimated total fat intake (r = 0.310, n = 44, p = 0.041). However, no further correlations were found between markers of obesity and dietary intakes.
Discussion
The aim of this study was to investigate the dietary intakes and the prevalence of overweight/obesity as potential risk factors for increased risk of CVD within the adult population with LLAs. Previous research suggested that amputees with major LLAs are at greater risk of developing CVD compared to the general population5,10,14,17,18 and it is believed that the current study is the first to focus on the dietary intakes of lower limb amputees. The key findings of the study are as follows: (1) male non-dysvascular amputees had higher than recommended intake of dietary fats, sugars and salts and (2) had a higher prevalence of overweight/obesity than the UK general population.
Dietary intakes in amputees
The dietary intakes of male amputees in the current study are not in line with the DRVs for the United Kingdom. The estimated daily intakes of carbohydrates and non-starch polysaccharides were significantly lower than the DRVs, whereas the daily intakes of protein, NMES, total fat, SFA and sodium were significantly higher; these results give sufficient reason for concern in terms of increased risk of CVD.30,31 However, the estimated daily consumption of fruit and vegetable showed no significant difference to the current recommendation for the United Kingdom.
The current study revealed that NMES intakes were more than double the DRV (22.01% vs 10%). High sugar intake is associated with increased prevalence of overweight/obesity and CVD; a systematic review showed a positive association between intakes of dietary sugars and change in body weight. 32 Recent research assessing the sugar intakes in the US population showed an increased risk of CVD mortality of 38% with added sugar intakes of 17%–21% compared to intakes of 8%, and with an intake of more than 21%, the risk of CVD mortality increased more than double. 31 There is evidence of an association between intakes of added sugars and changes in lipid profiles associated with an increased risk of CVD. 33 The current study also found high intakes of total fat and saturated fat in amputees indicating a further increased risk of CVD. Previous research found an increased risk of CVD associated with hypercholesterolaemia and/or dyslipidaemia in patients with LLA; a study comparing 68 male lower limb amputees with non-disabled matched controls reported significant higher low-density lipoprotein cholesterol in the amputees. 14 A systematic review by Hooper et al. 34 investigating 27 randomised controlled trials revealed that a reduction or change in dietary fat intakes led to decreased risk of CVD. Given previous evidence suggests participants under rather than over estimate intake of fats and sugars, 35 the authors are confident that their data have correctly highlighted poor dietary habits in this population.
A further concern that arose from the current findings was the significantly higher dietary sodium intakes of 2660.1 mg/day; high dietary sodium intakes were found to be positively associated with hypertension which in turn is linked to increased risk of stroke and CVD.36,37
In contrast to the rather concerning results of estimated sugar, fat and sodium intakes were the estimated intakes of fruits and vegetables (446.31 g/day) which were higher than the recommended minimum of 400 g/day, although this was statistically not significant. Nevertheless, this is still a higher estimated intake than the general population which on average consume less than 400 g/day and previous research associated a high consumption of fruits and vegetables with reduced risk of all-cause mortality and particular CVD.38–41
Diet as a whole is a modifiable risk factor which plays a major part in CVD prevention.42,43 Overall, the dietary guidelines for the prevention and management of diabetes may also be recommendable for lower limb amputees, and considering these guidelines is also intended to reduce the risk of obesity and CVD. 44 These guidelines do not refer to a specific type of diet; however, they do suggest a healthy balanced diet including low intakes of total fat, saturated fat, sugar and sodium and high intakes of fruits and vegetables. 44
Prevalence of overweight/obesity
Levels of overweight and/or obesity were higher in the current study population when compared to the general male population. When evaluating the BMI, WC and WHR, a very high prevalence of overweight/obesity was found and the majority of participants were at high or very high risk of developing CVD. The results of this study population demonstrated that a mean BMI was significantly higher than the general male population and the mean WHR was significantly higher than the recommended risk factor margin published in the HSE. 25 Although no significant difference was found between the study population and the general public, the mean WC of the participants was within the high-risk category of developing CVD. Furthermore, a significant positive correlation was found between BMI and WC, between BMI and WHR and also between WHR and WC. Of particular interest, BMI was positively correlated with total fat intake which could suggest a link between the poor dietary habits and the levels of overweight/obesity found in this study. However, it must be noted that correlations with other measures of obesity and total fat intake were not significant; therefore, the association of total fat intake with BMI is an area requiring further study before coming to the conclusion that there is a robust association.
The current findings with respect to overweight/obesity levels are in accord with previous studies which also found very high levels of obesity in lower limb amputees.13,18 Shahriar et al. 18 reported 82.5% obesity in bilateral male non-dysvascular lower limb amputees according to their WHR being greater than 0.9, and Rosenberg et al. 13 found 84% overweight/obesity 1 year post-amputation in dysvascular amputees, but they also described a pre-amputation overweight/obesity prevalence of 81.2%. Overall, the current study and previous research suggest an increased risk of overweight/obesity in amputees. There is some evidence that the level of overweight/obesity is associated with the level of LLA as described by Kurdibaylo, 14 who found in patients with unilateral non-dysvascular TTA 37.9% were obese. Obesity prevention and weight management play a major role in reducing the risk of CVD, but it is also important in terms of a good fitting prosthetic limb which in turn is associated with the amputees’ mobility and quality of life. 3 Obesity itself may limit the amputees’ mobility and/or ability to be physically active. The physical activity results in this study revealed 60.9% of moderate activity and 37.0% of moderate inactivity; this may be due to the young mean age of 46 years and 71.1% of LLAs were unilateral transtibial amputees. Also, the charity events chosen for the recruitment of participants were mostly attended by amputees who potentially have a higher level physical activity and are aware of the health benefits associated with increased physical activity. The good level of physical activity in this group may suggest that dietary intake is the more likely cause of overweight/obesity; however, historical levels of physical activity need to be considered before drawing a firmer conclusion.
The current study is not without its limitations; in particular, an additional comparison to a matched non-amputee control group, with data collected using an identical protocol, rather than comparing to DRV and HSE data, not collected by the same protocol, would significantly strengthen our findings. Furthermore, we only analysed non-dysvascular amputees’ data, and this cannot be generalised to all amputees. We also had no historical data available with regard to pre and post-amputation BMI.
All dietary analyses have limitations. We chose the self-reported EPIC FFQ as it has the advantage of reflecting habitual dietary habits of the study population, as opposed a single dietary recall which may not represent participants’ general diet. However, this dietary assessment method may have led to intentional or unintentional misreporting. Had we had access to our participant group for longer than a single occasion, multiple dietary recalls or several food diaries may have led to more accurate results.
Conclusion
This study focused on the dietary intakes in lower limb amputees and highlights poor dietary habits with respect to fat, sugar and salt intake which may pose an increased risk of CVD. Due to lack of sufficient research within this area, particular attention need to be paid to dietary habits, including food choices and eating patterns and how they may be affected by the disability (i.e. ability of food shopping or meal preparation).
Future research would ideally include much larger studies (i.e. multi-centred) in order to achieve a more representative sample of individuals with non-dysvascular and dysvascular LLAs and to explore whether lifestyle changing interventions would improve their health status and overall quality of life.
Supplemental Material
823118_supp_mat – Supplemental material for Dietary intakes and prevalence of overweight/obesity in male non-dysvascular lower limb amputees
Supplemental material, 823118_supp_mat for Dietary intakes and prevalence of overweight/obesity in male non-dysvascular lower limb amputees by Elke A Westerkamp, Siobhan C Strike and Michael Patterson in Prosthetics and Orthotics International
Footnotes
Acknowledgements
The authors would like to express their gratitude to Alan McDougall (Prosthetist at Blatchford) for his help and support at the Bowley Close Rehabilitation Centre. They also like to thank Kiera Roche from the LimbPower charity and Dean Heffner from the Limbless Association.
Author contribution
Elke A Westerkamp formulated the research question and undertook the data collection. All three authors contributed to study design, data analyses and writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Ethic Committee of the University of Roehampton (reference no. LSC 14/099), the NHS Research Ethics Committees (REC, reference no. 14/NS009) and the NHS Research and Development (R&D) Department at Guy’s and St Thomas’ NHS Foundation Trust (registration no. RJ114/N196).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from all participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.