
Abstract
Background:
For transfemoral amputations, the residual femoral length is critically important to prosthetic function. The aim of this report is to describe a novel method of extending femoral length and to assess its stability over time.
Case Description and Methods:
A 57-year-old woman with recurrent parosteal osteosarcoma was treated with above-knee amputation. A portion of the distal femoral endoprosthesis, which included uncemented fixation with a Compress® stem, was retained in an effort to extend the short femoral remnant and maximize stump length.
Findings:
At 3 years follow-up, the Compress stem remained well-fixed, and there was no soft tissue breakdown over the implant. The patient ambulated with a prosthetic limb and no external support.
Outcomes and Conclusion:
To the best of our knowledge, this is the first report of using the Compress device as a means to maintain stable fixation and extend residual femoral length following above-knee amputation.
Clinical relevance
Extension of residual bone length in amputated limbs can help improve prosthetic fitting and function. The Compress device may be useful in this application as a means of secure fixation for a modular metallic prosthesis.
Keywords
Background
Despite amputation being one of the oldest known operations, improvements in surgical technique are still vitally needed. For transfemoral amputations, the fitting of the socket and the function of the limb are dependent upon the length of the residual limb. 1 A variety of methods to extend bones and lengthen stumps have been described in the past.2–5 We report here a novel application of the Biomet Compress® device, previously developed for endoprosthetic limb salvage surgery, as a means of augmenting a short residual femur and maximizing the length of the residual lower limb. This strategy may have some potential advantages in the realm of reconstructive surgery for amputees. The aim of this report is to describe this novel method of extending femoral length and to assess its stability over time.
Case description and methods
A 26-year-old woman with parosteal osteosarcoma on the posterior aspect of the distal femur (Figure 1) underwent wide excision of the tumor and knee arthrodesis. After 5 years, the tumor recurred in the vastus lateralis, and this was removed by wide excision. A second soft tissue recurrence arose 9 years after, and it was also excised. Finally, at the age of 54 years, she presented to our clinic with a third recurrence, this time involving a long portion of the distal femur. We performed a distal femoral resection and endoprosthetic reconstruction, which included the Biomet Compress device for stem fixation (Figure 2). The patient did well initially and regained full active knee extension. However, she developed acute vascular insufficiency a month later and underwent emergent above-knee amputation. The anchor plug and spindle were left in place to maximize stump length. This provided a 10 cm extension of the short proximal femur. Following surgery, there was prolonged drainage at the stump. She underwent debridement of the wound and placement of a round methyl methacrylate cap on the metallic segment. The wound healed thereafter, and she could be fitted with an external prosthesis. The patient was followed radiographically and examined clinically for 3 years after this last operation. Radiographs were inspected for signs of loosening or instability of the prosthetic extension. Guidelines for patient consent have been met, and the report has been prepared in accordance with the rules of Institutional Review Board.

Lateral view of the right knee showing parosteal osteosarcoma in the distal femoral region prior to the initial operation.
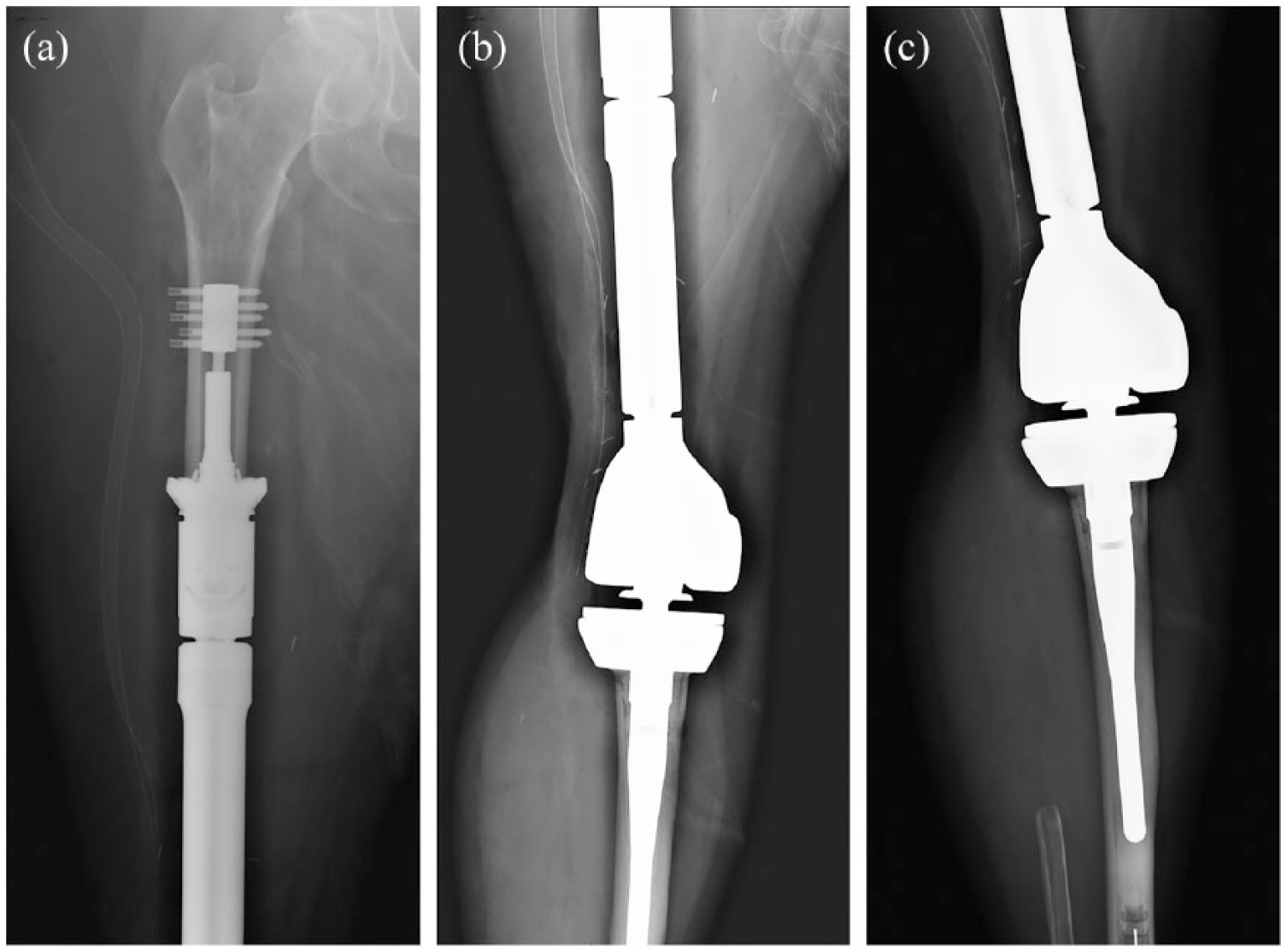
Anteroposterior views of the (a) femur, (b) knee, and (c) distal tibia showing the femoral endoprosthesis and hinged arthroplasty reconstruction of the knee after resection of recurrent disease.
Findings and outcomes
At her last follow-up (3 years after amputation), the skin showed no areas of erythema or breakdown. The patient ambulated with a prosthetic leg and did not use a cane or external support. X-rays showed stable stem fixation and no evidence of local recurrence, loosening, or loss of fixation (Figure 3).
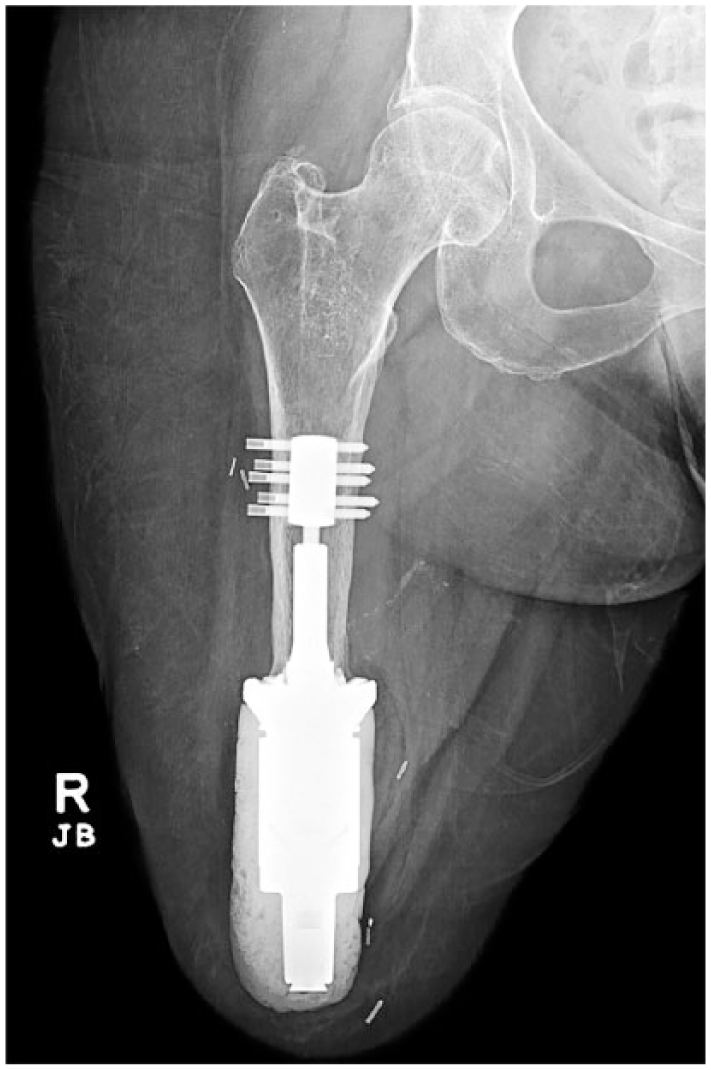
Anteroposterior view of the amputated limb with the Biomet Compress® implant and methyl methacrylate cap 3 years after amputation. The thickness of the diaphyseal bone has not diminished compared to the immediate post-operative radiograph (Figure 2). The anchor plug remains in stable configuration and position relative to the spindle.
Discussion and conclusion
For transfemoral amputation, an adequate residual limb length is important for prosthetic fitting and function. 6 Maximizing stump length can be challenging. In our patient, there was a paucity of normal bone relative to the amount of soft tissue at the time of amputation. The Compress anchor plug and spindle were retained in an effort to achieve the longest stump possible. The construct has remained stable and well-tolerated for 3 years now. The smooth methyl methacrylate cap seems to provide a suitable interface between the metal implant and the soft tissues of the stump.
The indications for extending femoral length after amputation include a number of clinical scenarios in oncologic surgery. Patients who might benefit are those undergoing amputation after prior distal femoral replacement, either for local recurrence or failure of the implant. There may also be the rare patient needing amputation with a skip metastasis that forces the level of osteotomy to be substantially higher than the soft tissue resection. Infection or repeated attempts at revision for aseptic loosening could result in a situation where there is little bone remaining but substantial viable soft tissue. If a well-fixed stem is present, it may be reasonable to retain this, but if the entire prosthesis must be removed, a metallic femoral extension with a Compress anchor may be a viable option.
The uncemented Compress device prevents stress shielding and promotes cortical bone hypertrophy. 7 It is worth noting that femurs tend to become osteopenic after above-knee amputation. The experience with our patient suggests that the Compress device maintains stability in the femoral diaphysis after amputation despite the tendency toward osteopenia. For segmental endoprosthetic fixation, the rate of aseptic loosening of the Compress device appears to be favorable.8,9 Another important feature of the Compress device is its short intramedullary length (8 cm or less), and its ability to achieve stable fixation when there is little diaphyseal bone remaining. 7
It is worth noting that a number of other methods have been described for lengthening residual limbs after amputation. The Ilizarov external ring fixator with distraction osteogenesis has been successfully used for lower limb lengthening. 3 The reverse flap method was reported by Pant and Younge 4 to attach the proximal to the distal tibia in five patients. Fibular allografts and autografts have also been reported. 5
The Compress stem might be pertinent to amputation surgery of the future since it offers an alternative means of osteointegration for an external prosthetic leg. There are certain theoretical advantages of Compress fixation compared to current methods of osteointegration. As mentioned before, the Compress stem can be applied to short residual bones, and it increases bone mineral density at the bone end. Moreover, it is easier to extract compared to porous ingrowth stems. These considerations may be especially relevant to treating infected stems, which is a difficult problem with current techniques of osteointegration. 10 Extraction of an infected, porous-ingrown stem could result in severe bone loss, and this may have serious consequences if there is not much diaphyseal bone to begin with. However, much work and research would be needed to determine whether the Compress stem is suitable for osteointegration.
In summary, we report the use of the Compress device to maximize residual limb length by addition of an endoprosthetic segment to a short proximal femur. At 3-year follow-up, the implant appears stable radiographically, and the patient continues to function well in terms of ambulation with a prosthetic limb. To our knowledge, this is the first report of using the Biomet Compress device for maximizing bone length after above-knee amputation. We suggest that the application of the Compress device for femoral fixation is suitable for the purpose of maximizing femoral length in patients undergoing transfemoral amputation, particularly in situations where there is greater bone loss compared to soft tissue loss. Whether the Compress concept may have applicability in the broader realm of osteointegration for prosthetic limbs remains to be determined.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.