
Abstract
Study design:
Retrospective cohort study.
Background:
Persons with a lower limb amputation can regain mobility using a prosthetic device. For fast and adequate prescription of prosthetic components, it is necessary to predict the mobility outcome early in rehabilitation. Currently, prosthetic prescription is primarily based on empirical knowledge of rehabilitation professionals.
Objective:
In this study, we explored motor ability tests, to be completed without a prosthetic device, which have predictive value for mobility outcome at the end of rehabilitation.
Methods:
For this study, data of 82 patients with a lower limb amputation were included. The Single-limb standing balance test (Balance test), the Lower-Extremity Motor Coordination Test and the Amputee Mobility Predictor Assessment Tool (AMPnoPRO) were used as measures for motor ability. Mobility outcome was measured using the Timed Up and Go Test, the Two-Minute Walking Test and K levels were used.
Results:
The explained variance of the Balance test, the Lower-Extremity Motor Coordination Test and the AMPnoPRO was, respectively, 0.603, 0.534 and 0.649 on the Two-Minute Walking Test (linear regression); 0.597, 0.431 and 0.624 on the Timed Up and Go Test (linear regression); and 0.432, 0.420 and 0.526 on the K levels (logistic regression).
Conclusion:
The AMPnoPRO predicted mobility outcome statistically (largest amount of explained variance).
Clinical relevance
This study explored the possibility of statistically predicting mobility outcome in lower limb amputees at the end of rehabilitation, using motor ability tests conducted in early rehabilitation. This study suggests the use of the AMPnoPRO to predict mobility outcome in lower limb amputees.
Keywords
Background
Approximately 3300 lower limb amputations are performed in the Netherlands annually. 1 The incidence of a lower limb amputation in the Netherlands is approximately 20 per 100,000; of which 60% is performed on males, 80% of the patients are older than 65 years and 90% of the amputations are the result of vascular causes. 1 A lower limb amputation reduces mobility and can make persons with a lower limb amputation dependent on assistive devices like crutches or a wheelchair. 2 A prosthetic device can help persons with a lower limb amputation to regain mobility and independence in daily living.3,4
The prediction of walking ability with a prosthetic device for persons with a lower limb amputation in the early stages of rehabilitation is important because walking ability influences the choice of prosthetic device and components most suitable for the amputee. 5 Tests, which statistically predict mobility outcome at the end of rehabilitation, that can be performed prior to prosthesis fitting may facilitate the choices regarding device and components. Currently, prosthetic prescription is primarily based on clinical expertise and empirical knowledge, which can lead to variations in prosthetic prescription, lack of transparency for patients and health insurance companies and the incorrect provision of prostheses to persons who are not able to use them. It has been shown that 30% of amputees were prescribed prosthetic feet from a lower functional category than their functional capabilities demonstrated. 6 Rehabilitation professionals require objective tests to make an informed choice on which prosthetic device should be prescribed and what rehabilitation programmes the amputee should follow. 7 It is known that the level of mobility that can be achieved by persons with a lower limb amputation is influenced by multiple variables like age,7–10 level of amputation10–12 and the cause of the amputation.13,14 In some studies, gender also influenced mobility outcome,5,10 but in most research, no influence of gender was found.3,15–17
During the rehabilitation process, multiple tests are available that help physicians to determine both motor ability and mobility in amputees. Tests that determine motor ability are the Single-limb standing balance test (Balance test), the Lower-Extremity Motor Coordination Test (LEMOCOT) and the Amputee Mobility Predictor without prosthesis (AMPnoPRO).18–20 Several tests that assess mobility outcome are available for example the Two-Minute Walking Test (2-MWT), the K levels, also known as Medicare Functional Classification Level, the Timed Up and Go (TUG) Test and the SIGAM-WAP, the Dutch translation of a single item scale of amputee mobility, which was described by the Special Interest Group in Amputee Medicine (SIGAM).21–25 The goal of this research was to identify the strongest predictor (largest explained variance) for mobility outcome.
The main question of this study was as follows: which motor ability test is the best statistical predictor for mobility outcome when corrected for the effect of secondary variables? We hypothesised that the AMPnoPRO is the best statistical predictor for mobility outcome since the AMPnoPRO is specifically designed for determining motor ability without the use of a prosthesis. Furthermore, the AMPnoPRO consists of more facets of motor ability compared with the LEMOCOT and the Balance test.
Methods
Data of patients with a unilateral lower limb amputation (transtibial, knee disarticulation or transfemoral) who were admitted between July 2011 and December 2014 to the Center for Rehabilitation of the University Medical Center Groningen were included in this retrospective cohort study. The time between amputation and admission to the rehabilitation centre displayed a median of 3 (interquartile range (IQR) = 1.7–6 weeks). Data of patients who underwent a bilateral amputation or who did not receive a prosthetic device or died during rehabilitation were not included in this study. Three motor ability tests were conducted at admission to rehabilitation: the Balance test, the LEMOCOT and the AMPnoPRO. For the performance of the AMPnoPRO, the patient must be able to make a few hops on one leg, and therefore, the tests could not be performed at admission since sometimes delayed wound healing did not allow hopping. Training in the rehabilitation centre focussed on improving physical fitness, balance control and muscle strength. After prosthetic prescription, patients started with basic gait training, followed by walking and standing using their own prosthesis during different activities. Duration of training with the prosthesis was 6–8 weeks. At the end of rehabilitation, two tests were conducted, the TUG Test and 2-MWT. Three physiotherapists of the rehabilitation centre conducted all tests and determined K level at the end of rehabilitation. The physiotherapists are experienced in testing the patients (evaluation of usual care) and were not blinded for the test results. Within the analysis, it was verified whether the secondary variables were associated with the outcome variables at the end of rehabilitation. These secondary variables were age, gender, level of amputation and cause of amputation. All data were extracted from the medical records and entered in SPSS. Missing cases in the data set were replaced with the median of the specific variable looking at all participants. For this study, permission was granted from the medical ethical commission of the University Medical Center Groningen (METC 2014/071).
Motor ability tests
The Balance test assesses balance while standing on the non-affected limb. The patient has to stand upright and perform a series of tests (e.g. balancing with eyes closed). As soon as the patient fails a test, the score for that test is the end score (ranging from 0 to 6 in which 0 is poor standing balance and 6 is good standing balance). 20 The Balance test has been found to be a decent outcome predictor for functional outcome (32% of the amputees were correctly predicted).18,19
The LEMOCOT measures motor coordination of the lower extremity. The patient moved the non-affected leg between two points as fast and precise as possible while being seated. 19 The number of on-target touches in 20 s is counted. A higher score suggests better motor coordination. The LEMOCOT showed considerable construct validity (r: 0.62–0.79) and test–retest reliability (intraclass correlation coefficient (ICC): 0.83–0.88). 17
The AMPnoPRO measures mobility before the patient starts to walk with a prosthetic device. It consists of 21 small assignments. The assignments are scored varying between 0 and 2 for test items and 0 and 3 for the use of an assistive device. 18 The total possible score across the 21 test items is 39. The AMPnoPRO showed considerable construct validity (r: 0.69) and excellent intra-rater (ICC: 0.96–0.97) and inter-rater reliability (ICC: 0.99). 18
Statistical analysis
Linear regression (stepwise) analyses were performed with the scores of the Balance test, the LEMOCOT and the AMPnoPRO and the secondary variables as predictors and the scores of the 2-MWT and the TUG Test as response variables. R2 (range 0–1) was used as measure for explained variance. A higher value corresponds to a larger amount of explained variance. A binary logistic regression was performed to explore the predictive value of the Balance test, the LEMOCOT and the AMPnoPRO on the K levels. The measure used for explained variance was Nagelkerke R2. Furthermore, the correctly predicted K levels were extracted from the classification tables. Before regression analyses, the secondary variables were dichotomised. Cause of amputation was dichotomised into vascular (0) and other causes (1). Lower limb amputations are most frequently performed due to a vascular cause, 1 and the frequency of other causes was expected to be small. 1 Age was dichotomised into younger than 65 (0) and 65 and older (1) years of age. Level of amputation was dichotomised into the categories transtibial (0) and transfemoral including knee disarticulation (1). K levels were dichotomised into 1 and 2 (0) and 3 and 4 (1). Gender was specified as males (0) and females (1). At the start of the statistical analysis, all secondary variables were entered stepwise and were included in the regression model if p ⩽ 0.05. Following this stepwise inclusion, the respective predictive test was entered in the equation, which was followed by a backward removal of the non-significant secondary variables from the model which had a p ⩽ 0.1. p-values ⩽0.05 were considered statistically significant.
A box-and-whisker plot was created for the best predictor with the K levels, as the K levels are used in an amputee rehabilitation setting for prescribing the correct prosthetic components.
To see whether this research corresponded with a previous study done by Gailey et al., the results were compared with the range of AMPnoPRO variables for each K level according to their research (http://assets.ossur.com/lisalib/getfile.aspx?itemid=31999).
Results
The database consisted of 87 patients; of which 5 were excluded due to a second amputation (n = 2), unsuccessful prosthesis fitting (n = 2) and death during rehabilitation (n = 1). This resulted in data of 82 patients available for analysis. Mean age was 59.2 years (standard deviation (SD): 13.3 years), 51 patients were younger than 65 years, 56 were male, 45 patients had a transtibial amputation and 52 patients had been amputated due to a vascular cause, of which 50% were older than 65 years. From the group with an amputation due to other causes, 17% were older than 65 years. The descriptive statistics of the three motor ability tests and the three mobility outcome tests can be found in Table 1.
Descriptive statistics of the test scores on the three motor ability tests and the three mobility outcome tests.
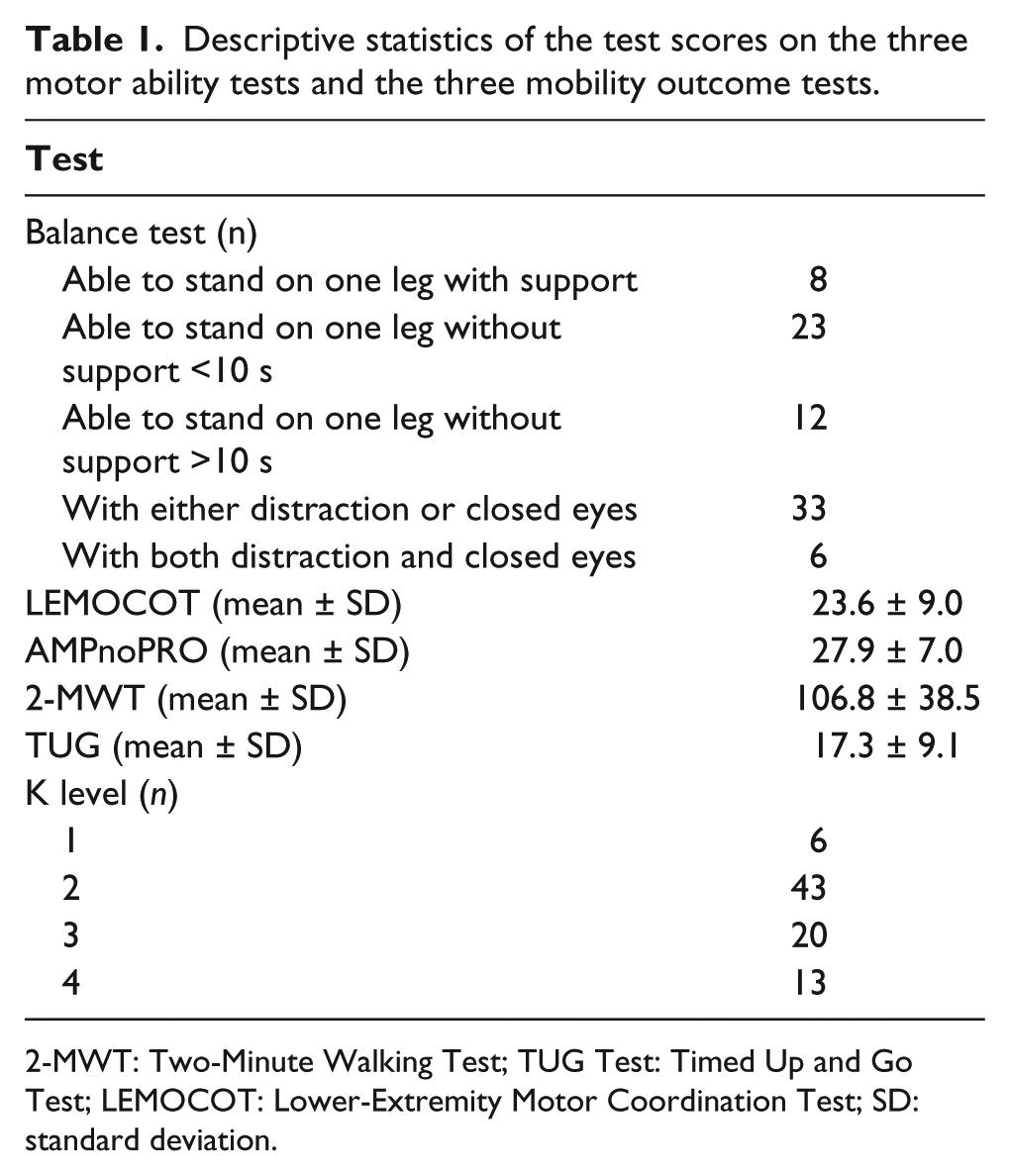
2-MWT: Two-Minute Walking Test; TUG Test: Timed Up and Go Test; LEMOCOT: Lower-Extremity Motor Coordination Test; SD: standard deviation.
For the 2-MWT, addition of the Balance test gave an R2 change of 0.120, addition of the LEMOCOT gave an R2 change of 0.051 and addition of the AMPnoPRO gave an R2 change of 0.213 (Table 2).
Results of linear regression analysis to predict the 2-MWT with the balance test (Balance), LEMOCOT and AMPnoPRO as predictors.
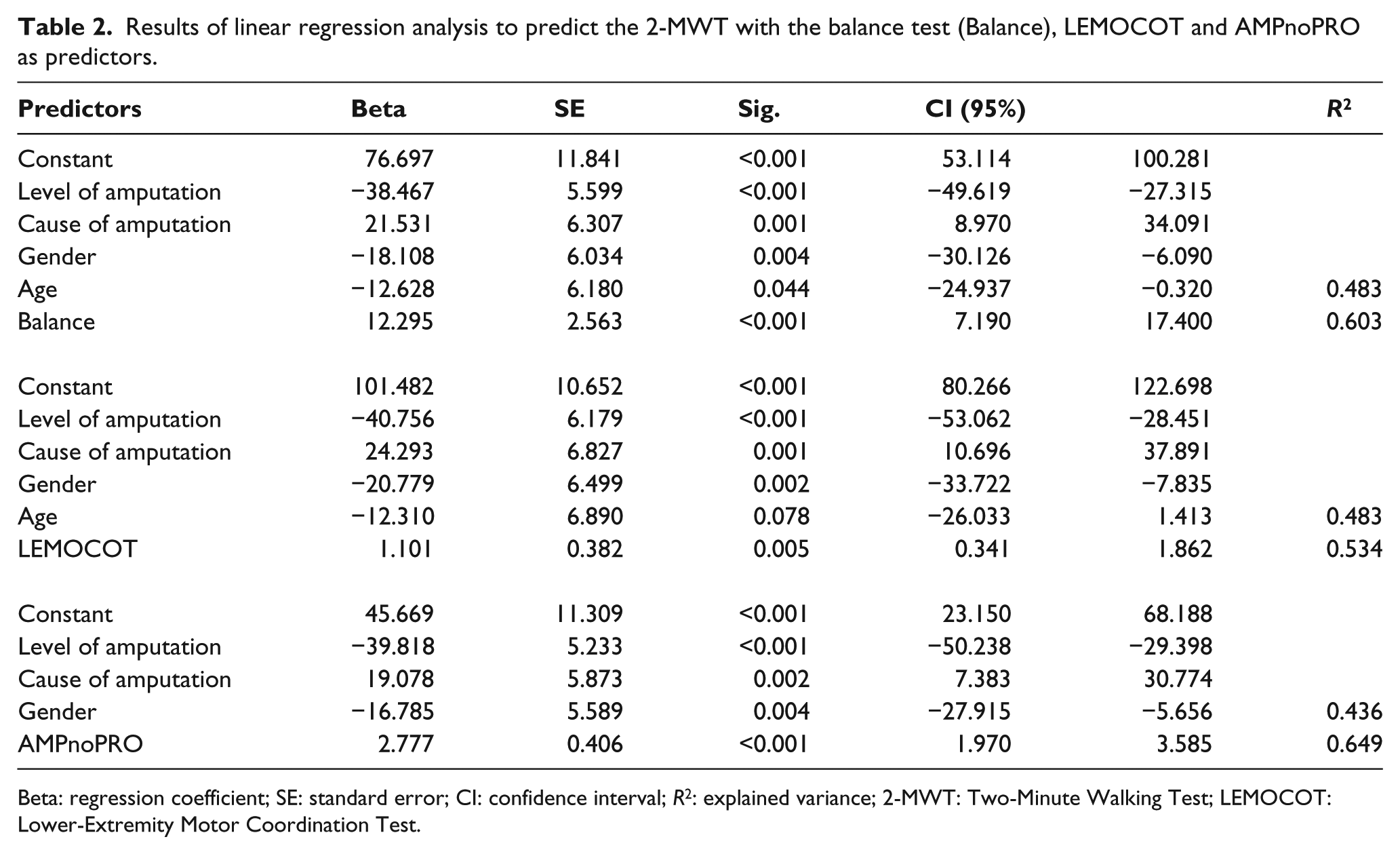
Beta: regression coefficient; SE: standard error; CI: confidence interval; R2: explained variance; 2-MWT: Two-Minute Walking Test; LEMOCOT: Lower-Extremity Motor Coordination Test.
For the TUG Test, addition of the Balance test gave an R2 change of 0.205, addition of the LEMOCOT gave an R2 change of 0.039 and addition of the AMPnoPRO gave an R2 change of 0.232 (Table 3).
Results of linear regression analysis to predict the TUG Test with the balance test (Balance), LEMOCOT and AMPnoPRO as predictors.
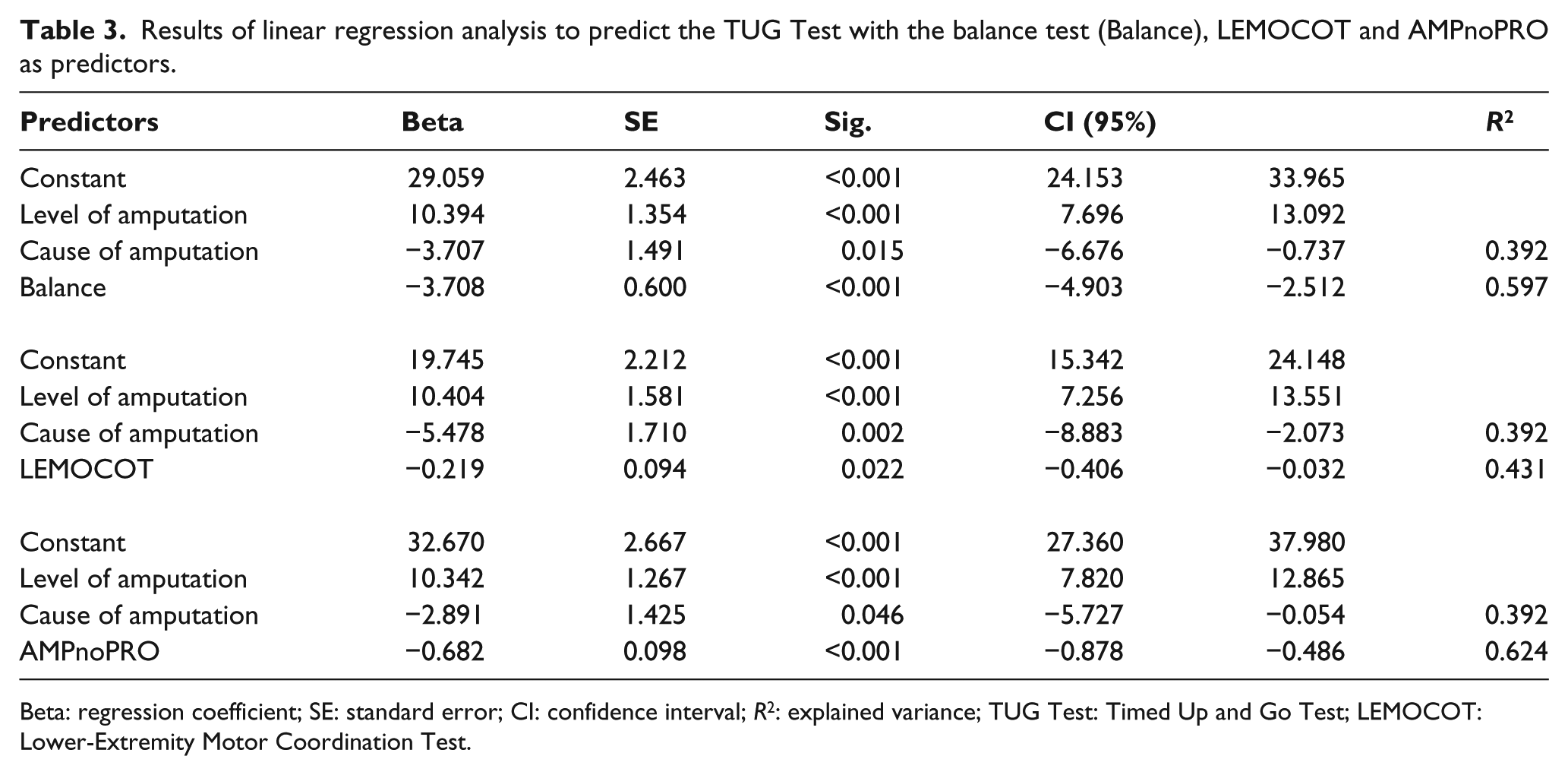
Beta: regression coefficient; SE: standard error; CI: confidence interval; R2: explained variance; TUG Test: Timed Up and Go Test; LEMOCOT: Lower-Extremity Motor Coordination Test.
For K levels, the addition of the Balance test gave an (Nagelkerke) R2 change of 0.088, addition of the LEMOCOT gave an R2 change of 0.076 and addition of the AMPnoPRO gave an R2 change of 0.264 (Table 4). The percentages of correctly predicted K levels for the different models were 78.0% for the Balance test, 76.8% for the LEMOCOT and 82.9% for the AMPnoPRO.
Results of binary logistic regression analysis to predict the K levels (K levels 1 and 2 = 0, 3 and 4 = 1) with the balance test (Balance), LEMOCOT and AMPnoPRO as predictors.
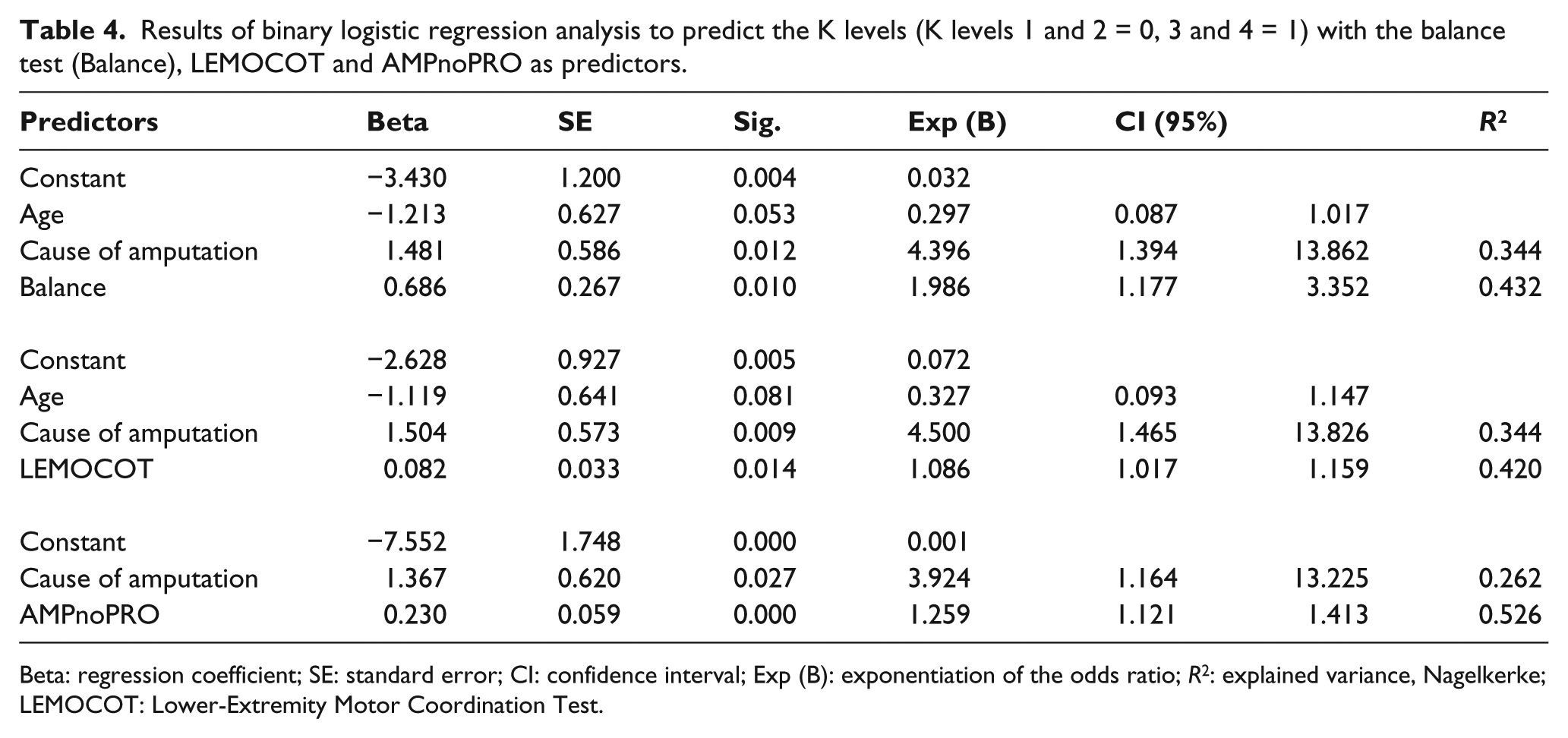
Beta: regression coefficient; SE: standard error; CI: confidence interval; Exp (B): exponentiation of the odds ratio; R2: explained variance, Nagelkerke; LEMOCOT: Lower-Extremity Motor Coordination Test.
Of the motor ability tests, the AMPnoPRO explained most variance for all outcome variables. Looking at the box-and-whisker plot (Figure 1), it can be seen that the median value of the AMPnoPRO for K levels 1 and 2 are around the same level and are both lower than the median for K level 3, which is again lower than the median for K level 4.
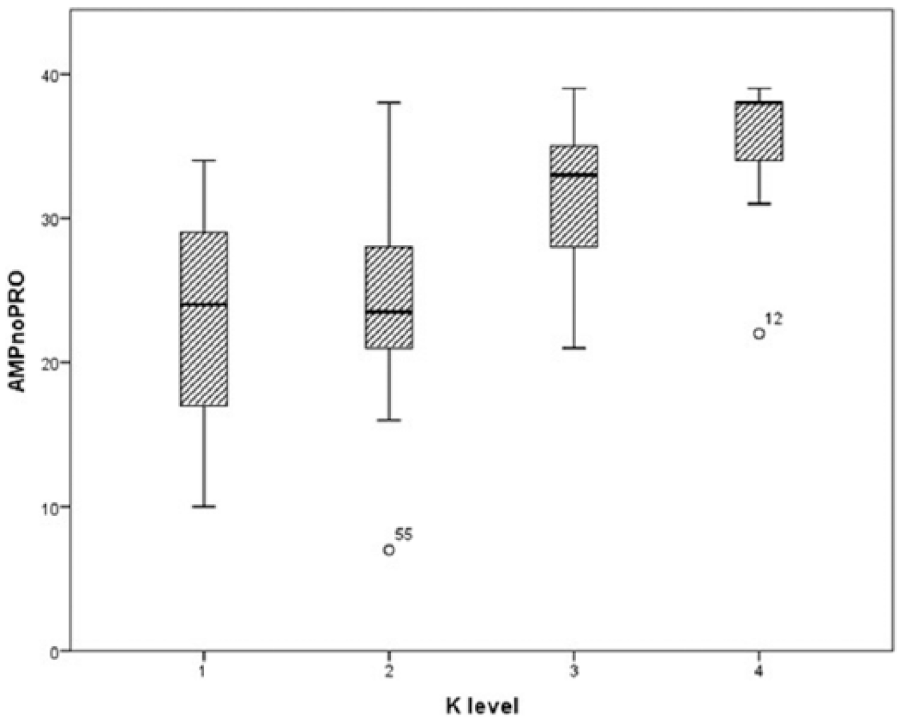
Box-and-whisker plot of the scores of the AMPnoPRO against the K levels. The points 12 and 55 are outliers.
In this research, 59.76% of all participants fell inside in range proposed by Gailey et al.
Discussion
The aim of this study was to explore whether motor ability tests (Balance test, the LEMOCOT and the AMPnoPRO) could be used to statistically predict mobility outcome at the end of rehabilitation when corrected for effects of secondary variables. These tests were performed by the amputee during the start of rehabilitation before the amputee was fitted with a prosthetic device. The AMPnoPRO was measured later in the rehabilitation process than the other two motor ability tests in multiple cases. This delay could have had an effect on the scores of the tests; however, due to the necessity of adequate wound healing to perform the items that involve hopping in the AMPnoPRO, this delay was unavoidable. Furthermore, bias may be present because the assessors, physiotherapist, evaluated usual care of the amputees, and were not blinded for previous assessment results. Outcome of mobility outcome was measured in three ways: the 2-MWT, the TUG Test and the K levels. Results show that all motor ability tests have some statistical predictive value for mobility outcome. The AMPnoPRO showed the highest explained variance followed by the Balance test and the LEMOCOT for all three mobility outcome tests, supporting the hypothesis. Looking closer at the content of the motor ability tests, these results could more or less be expected: the LEMOCOT measures the coordination of the non-affected limb while the patient is sitting on a chair, the Balance test measures balance capabilities in persons with a lower limb amputation, but only in a static standing position, whereas the AMPnoPRO measures both static and dynamic balances through an array of 21 different tests.
From the secondary variables, level of amputation had predictive value on mobility outcome. It could be assumed that the level of amputation would have a significant effect on mobility outcome, since the knee joint is retained in a transtibial amputation.11,12 Energy expenditure is higher for transfemoral amputees compared to transtibial amputees. 26 It was expected that age would have predictive value on mobility outcome in persons with a lower limb amputation, since older people normally have more problems with walking, in general, and with learning to walk with a prosthetic device, in particular.7–9 In this study, the cause of the amputation had no predictive value on mobility outcome, which was unexpected. Causes, like trauma or infection, are mostly local, whereas an amputation with a vascular cause is a comorbidity of vascular disease which has an effect on the entire body.8,13,14 In general, persons with a vascular cause of amputation are older than persons with a traumatic amputation. Therefore, the effects of cause of amputation and age may not be distinguishable in this study. Additionally, persons with a lower limb amputation because of vascular problems with a poor prognosis are mostly not admitted to a rehabilitation centre but to a nursing home. 27 In this study, gender had no predictive value on mobility outcome, except on the 2-MWT. This lack of predictive value can be explained through results of a study that found significant differences between walking speeds for males and females when not corrected for leg length. 28 Since the 2-MWT measures the distance walked in 2 min, the scores would be higher for male walkers than for female walkers, as the scores for the 2-MWT were not corrected for leg length.
In previous research, some motor function tests were evaluated for their predictive value for mobility outcome in amputee populations. The Functional Independence Measure (FIM) and Rivermead Mobility Index have shown not to be predictive for post-amputation walking.5,29,30 The Single-limb balance test is indicative for better walking potential after an amputation. 20 A combination of both mental and physical tests, 10 taking into account the ability to stand on one leg, age, gender and level of amputation, showed a significant predictive value for mobility outcome in an amputee population. These findings are in accordance with our results. The AMPnoPRO has significant correlations with the 6-minute walking test (r: 0.694). 18 This result is also in line with this study in which the AMPnoPRO showed predictive value for the three other mobility outcome tests.
The K levels are of most clinical interest since these levels are used to classify amputees for prosthetic component prescription. A motor ability test that can distinguish among the five K levels could increase accuracy in prescribing prosthetic components. In the previous study, the AMPnoPRO was able to predict the K levels. 18 For every K level, the authors stated an estimated cut score on the AMPnoPRO: K0: 0–8, K1: 9–20, K2: 21–28, K3: 29–36 and K4: 37–43 (http://assets.ossur.com/lisalib/getfile.aspx?itemid=31999). This study showed that 59.76% of the patients were correctly classified. Our data showed that the outcome of this test should be interpreted with great caution. To reduce rehabilitation costs, it might seem a good idea to exclude people from prosthetic limb training who are classified K0 during admission using the AMPnoPRO scores. However, one of our participants, who scored 7 on the AMPnoPRO (which would be K0), became a K2 prosthetic limb user at discharge.
Looking at the box-and-whisker plot (Figure 1), it can be seen that there is a distinct difference between K levels 2 and 3. There is less difference between K levels 3 and 4 and a great overlap between K levels 1 and 2. These results may be related to the small group of participants who scored in K levels 1 (n = 6) and 4 (n = 13).
In the linear regression, two ordinal scales, the Balance test and the AMPnoPRO, were used as predictors. The resulting betas should be interpreted carefully.
Since K levels are an ordinal scale, considerably larger sample sizes are required to analyse whether and which motor ability test on admission can determine the K level more precisely.
This study is a good starting point in predicting mobility outcome using motor ability tests. The AMPnoPRO consistently showed better predictive values compared to both the Balance test and the LEMOCOT. Further research should include a larger research population, as it would lead to a larger statistical power. This might lead to a better distinction between K levels.
Conclusion
This study explored the predictive values of three motor ability tests on mobility outcome in persons with a lower limb amputation in a rehabilitation setting when corrected for effects of secondary variables. AMPnoPRO was the best statistical predictor for mobility outcome. However, due to the small population, it is not possible to use these results in practice yet. Research in a larger population is required.
Footnotes
Acknowledgements
We like to thank Carine EM Goos as our contact during the research, providing us with information regarding the rehabilitation programme.
Author contribution
M.H.S., P.v.d.B., A.H.V. and H.G.v.K contributed to set-up. A.H.V. contributed to data collection supervision. M.H.S., P.v.d.B. and P.U.D. contributed to data analysis. M.H.S., P.v.d.B., A.H.V., H.G.v.K. and P.U.D contributed to the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.