
Abstract
Background:
Many individuals with cerebral palsy wear ankle foot orthoses during daily life. Orthoses influence joint motion, but how they impact muscle remains unclear. In particular, the gastrocnemius is commonly stiff in cerebral palsy. Understanding whether orthoses stretch or shorten this muscle during daily life may inform orthosis design and rehabilitation.
Objectives:
This study investigated the impact of different ankle foot orthoses on gastrocnemius operating length during walking in children with cerebral palsy.
Study design:
Case series, within subject comparison of gastrocnemius operating length while walking barefoot and with two types of ankle foot orthoses.
Methods:
We performed gait analyses for 11 children with cerebral palsy. Each child was fit with two types of orthoses: a dynamic ankle foot orthosis (Cascade dynamic ankle foot orthosis) and an adjustable dynamic response ankle foot orthosis (Ultraflex ankle foot orthosis). Musculoskeletal modeling was used to quantify gastrocnemius musculotendon operating length and velocity with each orthosis.
Results:
Walking with ankle foot orthoses could stretch the gastrocnemius more than barefoot walking for some individuals; however, there was significant variability between participants and orthoses. At least one type of orthosis stretched the gastrocnemius during walking for 4/6 and 3/5 of the Gross Motor Functional Classification System Level I and III participants, respectively. AFOs also reduced peak gastrocnemius lengthening velocity compared to barefoot walking for some participants, with greater reductions among the Gross Motor Functional Classification System Level III participants. Changes in gastrocnemius operating length and lengthening velocity were related to changes in ankle and knee kinematics during gait.
Conclusion:
Ankle foot orthoses impact gastrocnemius operating length during walking and, with proper design, may assist with stretching tight muscles in daily life.
Clinical relevance
Determining whether ankle foot orthoses stretch tight muscles can inform future orthotic design and potentially provide a platform for integrating therapy into daily life. However, stretching tight muscles must be balanced with other goals of orthoses such as improving gait and preventing bone deformities.
Keywords
Background
Ankle foot orthoses (AFOs) are commonly used to improve ambulation for individuals with cerebral palsy (CP). Many types of AFOs are available and are prescribed for different gait patterns and musculoskeletal deformities. AFOs are designed to improve gait, reduce energy costs, prevent bone deformities, provide stability, and achieve other patient-specific goals.1–8 The majority of these goals focus on improving function, and prior research has indicated that if properly prescribed, AFOs can improve gait and other activities of daily living. 9 Since AFOs are worn daily, this research also suggests that AFOs may provide a tool for extending therapy and rehabilitation into daily life.
CP is caused by a brain injury at or near the time of birth; 10 however, secondary musculoskeletal impairments such as bone deformities, contracture, and weakness commonly develop. 11 AFOs have been designed to help prevent bone deformities, 12 but their impact on muscle is not as well understood. In particular, the gastrocnemius is a complex multi-articular muscle, which is commonly impaired among individuals with CP and may be influenced by AFO prescriptions.13,14 Stretching has commonly been prescribed for individuals with CP, and repetitive stretching has been shown to increase gastrocnemius fascicle length and reduce passive force. 15 Since muscles adapt to the stretched or shortened positions experienced during daily life, understanding how AFOs influence gastrocnemius length could be important for optimizing AFOs. If an AFO can stretch the gastrocnemius with every step, AFOs may help prevent contracture and improve long-term muscle function. Conversely, if an AFO decreases the gastrocnemius operating length, it may further exacerbate contracture.
Musculotendon operating length is defined as the length of the muscle–tendon unit from origin to insertion during movement. Prior studies have indicated that individuals with CP often have a shortened gastrocnemius operating length compared to unimpaired individuals, which can contribute to excessive ankle plantarflexion and knee flexion in stance.16,17 Spasticity, defined as a velocity-dependent resistance to stretch, 18 is also common in individuals with CP and can contribute to increased ankle plantarflexion during gait. 19 However, quantifying musculotendon operating length and velocity during movement can be challenging because it requires information about an individuals’ joint kinematics, musculoskeletal geometry, moment arms, and muscle paths. Gait analysis and musculoskeletal modeling can be used to quantify these parameters and estimate musculotendon operating length and velocity. 20 For example, musculoskeletal modeling has been used to evaluate hamstring operating length and velocity during crouch gait of children and adolescents with CP. These studies have demonstrated that hamstring operating length and velocity are related to outcomes after surgery and can be used for treatment planning.21,22 A prior study also evaluated the impact of AFOs on hamstring operating length and demonstrated increased operating lengths with rigid AFOs compared to barefoot walking. 23 In a case study of an adult stroke survivor, a rigid AFO was also shown to decrease the operating length of the gastrocnemius during gait compared to barefoot walking. 14 Musculoskeletal modeling has also shown that in CP, gastrocnemius length and velocity differ in children with spasticity and are dependent on walking speed. 24 Evaluating the impact of AFOs on musculotendon operating lengths and velocities may have important implications for rehabilitation and long-term use of AFOs.
The goal of this study was to evaluate how AFOs impact gastrocnemius musculotendon operating length and velocity during gait among children with CP. We evaluated gastrocnemius operating length and velocity during walking with two different types of AFOs: Cascade dynamic ankle foot orthoses (DAFOs) and Ultraflex adjustable dynamic response ankle foot orthoses (ADR AFOs). We sought to determine whether currently available AFOs and prescription procedures tend to stretch or shorten the gastrocnemius during gait compared to barefoot walking and whether responses are dependent upon impairment level or type of AFO.
Methods
This study reports a secondary analysis of data from a trial comparing two types of AFOs and barefoot walking in children with CP. Details and results of the main study appear in a previous publication. 25 This study extends that work by examining the effects of different types of AFOs on medial gastrocnemius (MG) operating length and velocity.
Participants
Data were analyzed for 11 children with CP, including 6 individuals in Gross Motor Function Classification System (GMFCS) Level I (mean ± standard deviation, height: 120.6 ± 15.2 cm, mass: 23.9 ± 9.6 kg, age: 7.9 ± 2.4 years) and 5 individuals in GMFCS Level III (height: 116.1 ± 10.7 cm, 23.5 ± 5.7 kg, age: 7.4 ± 2.2 years). Three hemiplegic, five diplegic, and two quadriplegic participants were included in this study. All participants had crouch and/or equinus gait patterns, as evaluated by the physical therapists’ visual observations. 26 Participants were not excluded based upon prior surgical or pharmaceutical treatment (Table 1). Children’s Hospital Los Angeles Institutional Review Board approval was obtained for this study and participants and their guardians gave written informed assent and consent.
Participant information and prescribed AFOs.
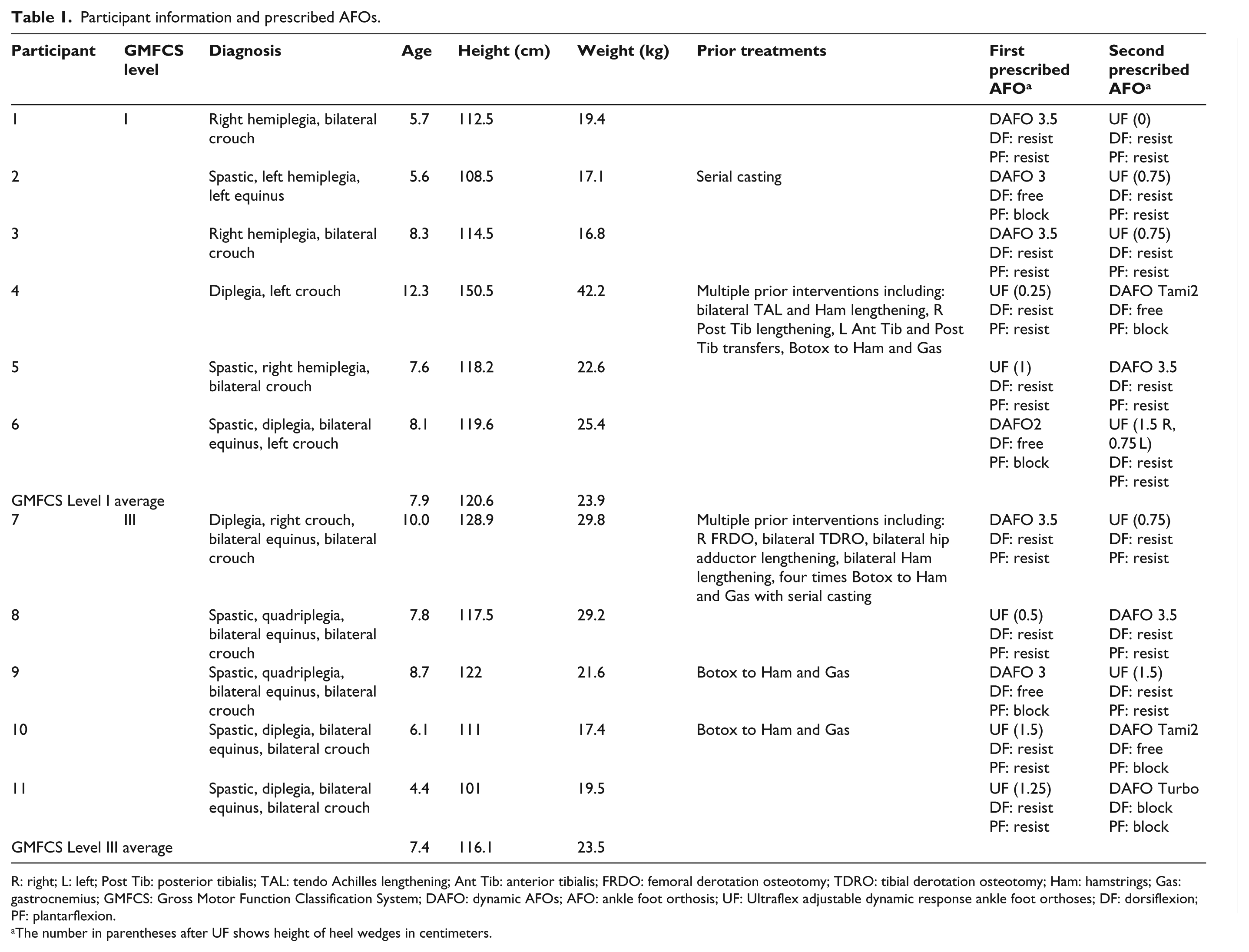
R: right; L: left; Post Tib: posterior tibialis; TAL: tendo Achilles lengthening; Ant Tib: anterior tibialis; FRDO: femoral derotation osteotomy; TDRO: tibial derotation osteotomy; Ham: hamstrings; Gas: gastrocnemius; GMFCS: Gross Motor Function Classification System; DAFO: dynamic AFOs; AFO: ankle foot orthosis; UF: Ultraflex adjustable dynamic response ankle foot orthoses; DF: dorsiflexion; PF: plantarflexion.
The number in parentheses after UF shows height of heel wedges in centimeters.
Orthotic conditions
Each participant was prescribed two different types of AFOs: DAFOs and Ultraflex ADR AFOs. Participants wore each AFO for 4 weeks, and the order of AFOs was randomized for each participant. The AFO prescriptions were determined by manufacturer recommendations based on range of motion, muscle tone, and observational gait analysis (barefoot and wearing the participant’s current AFOs) performed by a physical therapist. Fitting was performed by a certified pediatric orthotist.
Due to the heterogeneity in walking patterns among individuals with CP, the DAFOs and ADR AFOs prescribed varied between participants (Table 1). For example, DAFO 3.5 provides moderate dorsiflexion resistance and aggressive plantarflexion resistance. DAFO 2, DAFO 3, and DAFO Tami 2 provide free dorsiflexion motion and limited plantarflexion motion. DAFO Turbo provides aggressive plantarflexion resistivity and limited plantarflexion motion. The ADR AFO uses elastomers to provide resistance and store energy, including four adjustment channels: anterior and posterior elastomers to resist dorsiflexion/plantarflexion (0–27.1 N m/0–40.7 N m) and anterior and posterior stops to limit dorsiflexion/plantarflexion. Table 1 provides the order of AFO prescription, dorsiflexion/plantarflexion resistance, heel wedge height, and DAFO type for each participant. The goal of this research was to determine, given the current standards of prescription, whether these different AFOs tend to stretch or shorten the MG during gait in children with CP.
Gait analysis procedure
Each participant visited the gait analysis laboratory three times over a 2-month period for initial testing and testing with the two types of AFOs. During the first visit, the participant’s gait was assessed without AFOs, in the barefoot condition. The participants were randomly assigned one type of AFO. The participants wore the first AFO for 4 weeks and then returned for gait analysis. Each participant was then fit with the other type of AFO and returned 4 weeks later for gait analysis. The same shoes were worn with both AFOs (Apis Answer2 Shoes; Apis Footwear Company, South El Monte, CA, USA).
For gait analyses, an eight-camera infrared motion-capture system (Vicon Motion Systems Ltd., Oxford, UK) was used to acquire three-dimensional marker data at 120 Hz. Markers were placed on each participant based on a modified Helen-Hayes marker set. 27 At each visit, a minimum of 10 gait cycles was collected. Each participant’s kinematic data were averaged over all gait cycles to compare the different conditions.
Musculoskeletal modeling
OpenSim, an open-source musculoskeletal modeling software, 28 was used to calculate joint angles and estimate musculotendon operating length of the MG. A generic musculoskeletal model with 19 degrees of freedom (DOFs) and 92 musculotendon actuators was scaled to each participant based upon anatomical landmarks: 20 three rotational and translational DOF at the pelvis, a ball-and-socket joint between the pelvis and torso, ball-and-socket joints at each hip, and a single DOF at each knee and ankle. Inverse kinematics was used to calculate joint angles by minimizing the distance between experimental marker trajectories and virtual markers in OpenSim. The MG operating lengths were calculated along the musculotendon path from origin to insertion in the musculoskeletal model during the gait cycle.
For each individual, we evaluated musculotendon operating length from the scaled model over a gait cycle. The MG’s peak operating length during gait was compared to each individual’s passive threshold, which was defined as the length of the MG at maximum ankle dorsiflexion with the knee fully extended from physical examination. To compare between participants, MG operating length and passive threshold were normalized to the length of the MG when the musculoskeletal model was positioned in anatomic position, similar to previous studies.22,29 Musculotendon velocity was calculated by numerically differentiating the normalized MG length with respect to time.
Since joint and musculotendon kinematics depend on walking speed, 29 each participant’s walking speed was calculated from the horizontal position of the sacrum marker. The walking speed of the GMFCS Level I and III participants were most similar to the slow and very slow walking speeds, respectively, of a group of typically developing children analyzed in a prior study (N = 8, data available at: http://simtk.org/home/mspeedwalksims), 30 and the average kinematics and MG operating length and velocity for the slow and very slow speeds from these children were used for comparison. Figure 1 shows an example of the average MG operating length for one participant over a gait cycle with each of the tested conditions.
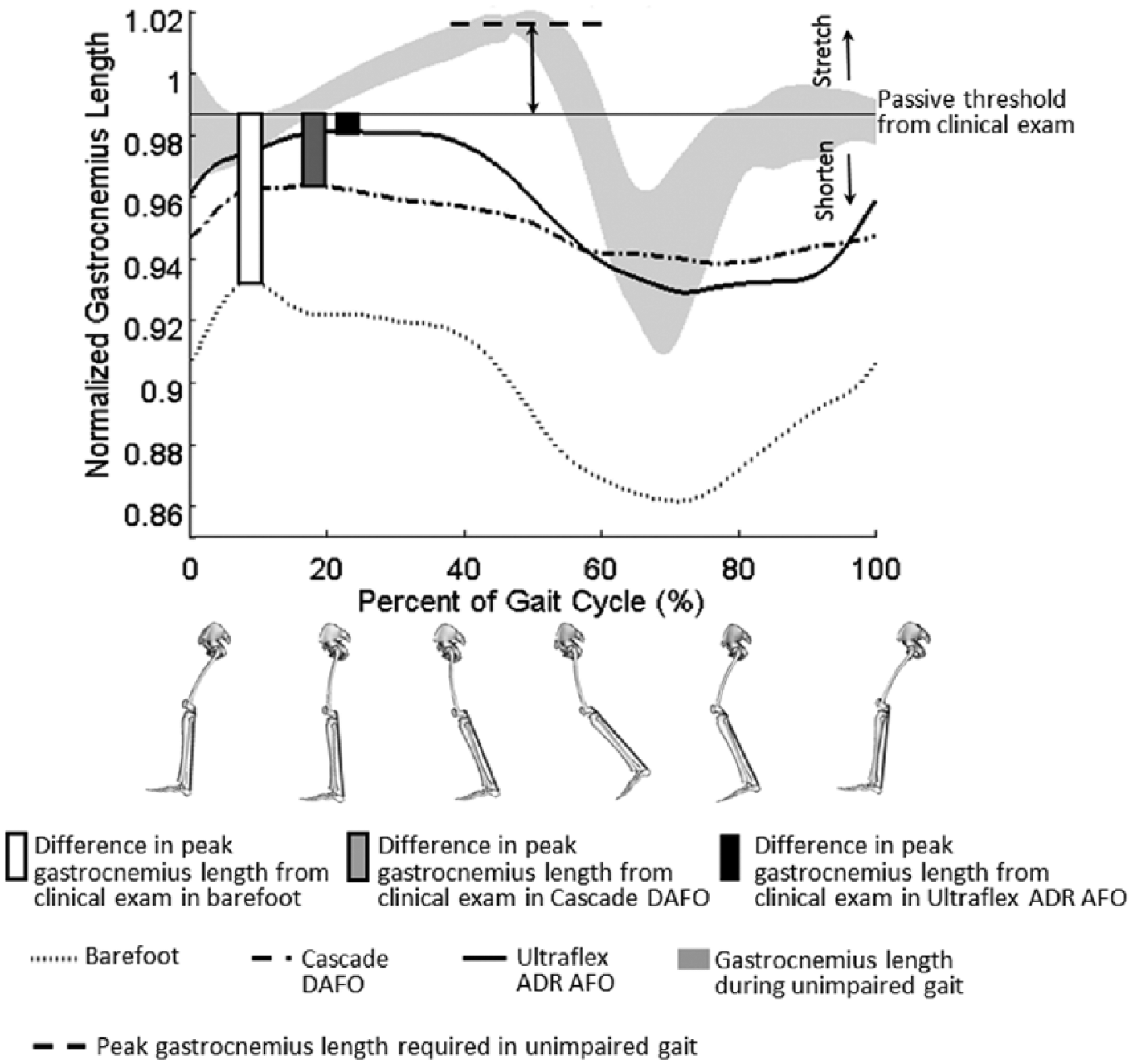
The average medial gastrocnemius operating length over a gait cycle across all conditions for one participant (P09, left limb). For each condition, the relative difference between peak gastrocnemius operating length and the passive threshold from physical exam was calculated (bars). The difference in the passive threshold and the peak gastrocnemius operating length required during unimpaired gait was also calculated (arrow). The gray shaded curve represents the average ±1 standard deviation in gastrocnemius operating length for unimpaired individuals walking at a very slow speed, similar to the speed of this participant. Thus, this participant’s passive threshold was less than the peak length required during unimpaired gait. Furthermore, when walking barefoot or with either AFO, this participant did not stretch the gastrocnemius beyond the passive threshold measured by the physical therapist during the physical exam.
Results
Barefoot walking
We first evaluated whether, during barefoot walking, the MG was stretched or shortened relative to the passive threshold measured from physical examination. For all but one participant (P04), the MG operated at a shorter length than the passive threshold during barefoot walking (Figures 2(a) and 3(a), white bars are less than 0). These results indicate that when walking barefoot, the MG was generally not stretched beyond the maximum length measured during passive stretching of the ankle by a therapist.
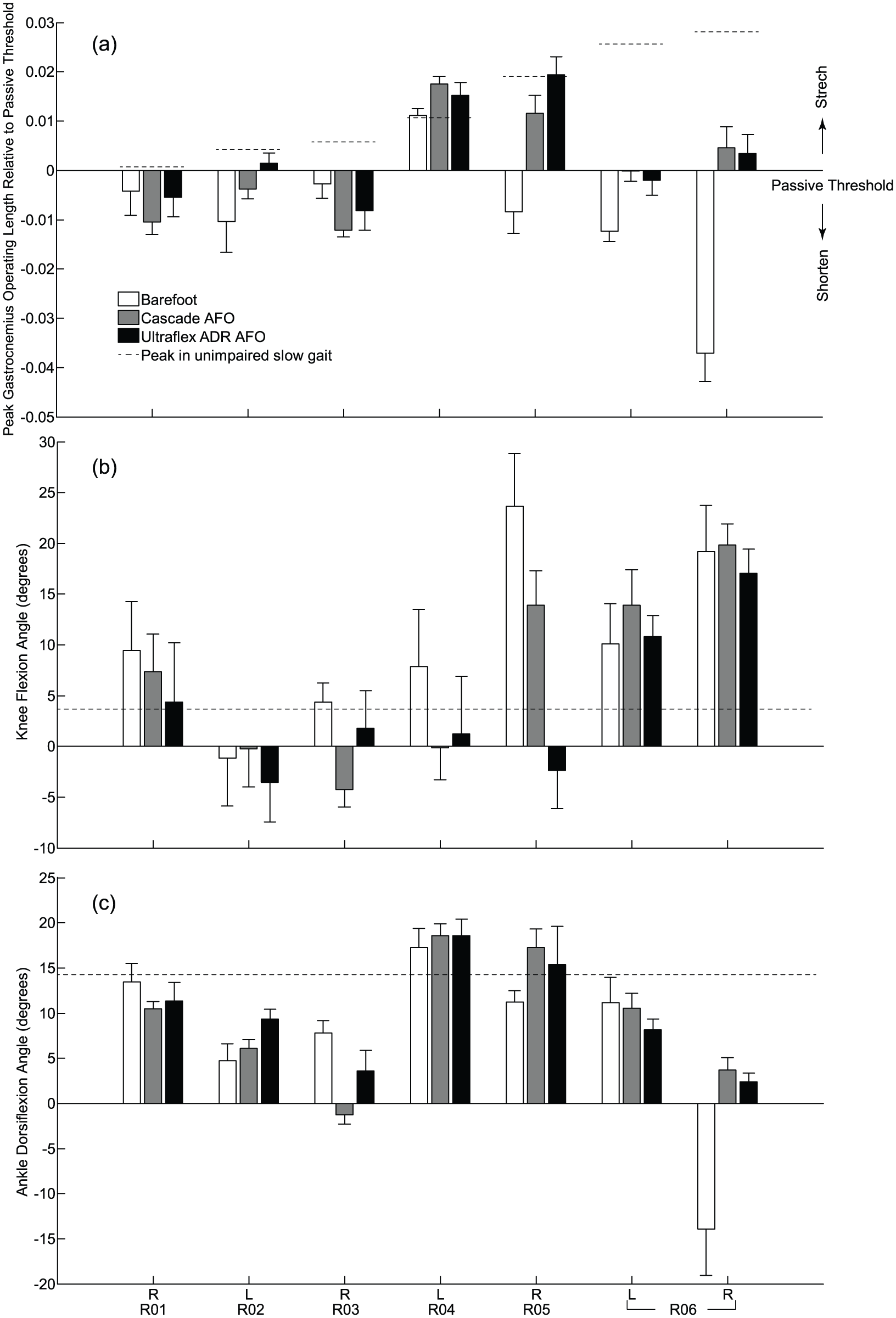
GMFCS Level I results: (a) average normalized peak medial gastrocnemius operating length during gait compared to each individual’s passive threshold from physical exam and sagittal plane kinematics at the (b) knee and (c) ankle at peak gastrocnemius operating length for all limbs that wore AFOs. Comparisons are shown during walking barefoot (white bars), with DAFOs (gray bars), and with ADR AFOs (black bars). Error bars describe 1 standard deviation across multiple gait cycles for each gait condition. Positive values of gastrocnemius length suggest stretching relative to the passive threshold and positive values of knee and ankle angles indicate flexion and dorsiflexion, respectively. Dashed lines depict the (a) peak operating length, (b) minimum knee flexion, and (c) maximum dorsiflexion during unimpaired gait at slow speeds. A dashed line in (a) greater than zero indicates that the participant’s passive threshold measured from physical exam was lower than the operating length required during unimpaired gait.
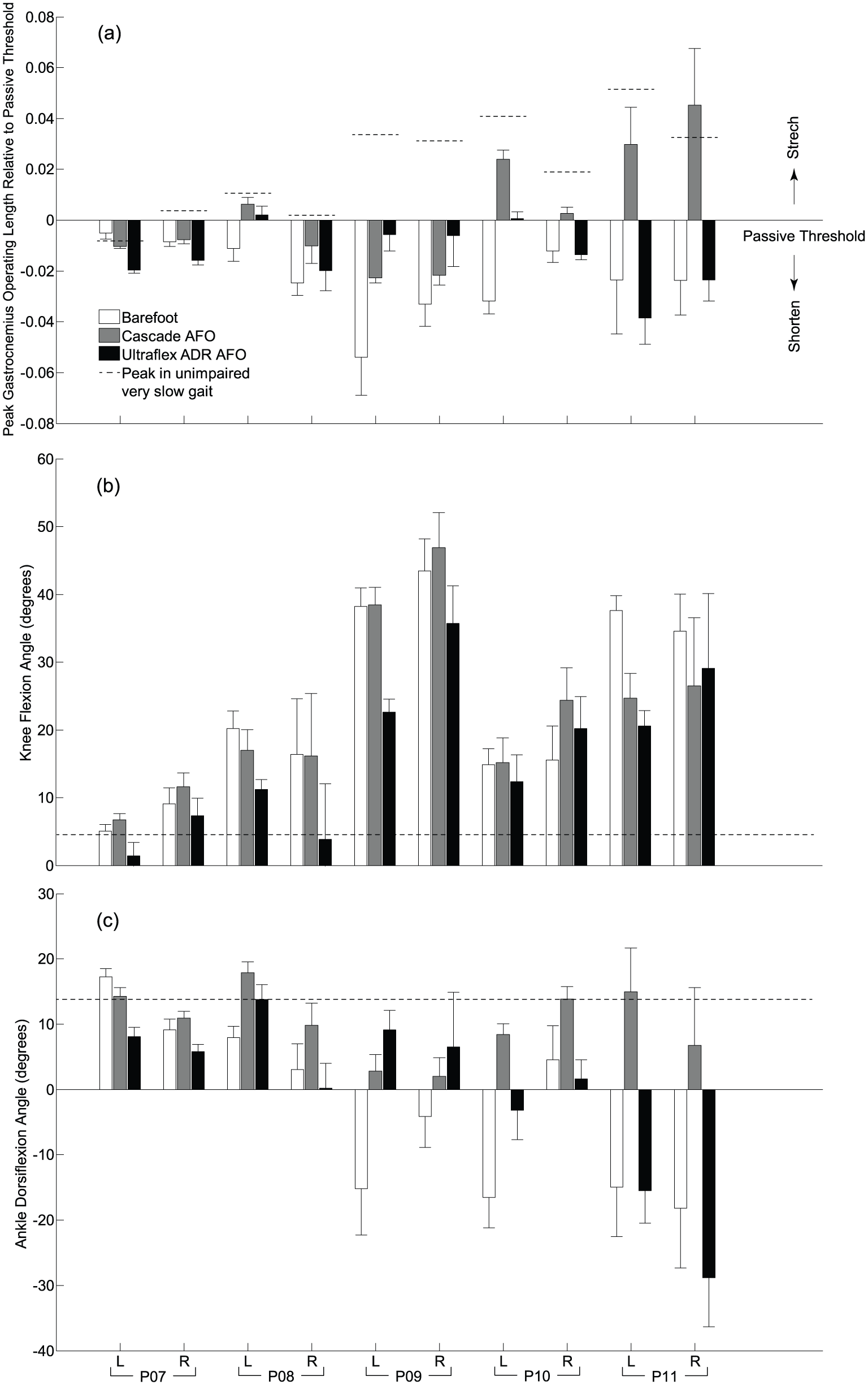
GMFCS Level III results: (a) average normalized peak medial gastrocnemius operating length during gait compared to each individual’s passive threshold from physical exam and sagittal plane kinematics at the (b) knee and (c) ankle at peak gastrocnemius operating length for all limbs that wore AFOs. Comparisons are shown during walking barefoot (white bars), with DAFOs (gray bars), and with ADR AFOs (black bars). Error bars describe 1 standard deviation across multiple gait cycles for each gait condition. Positive values of gastrocnemius length suggest stretching relative to the passive threshold and positive values of knee and ankle angles indicate flexion and dorsiflexion, respectively. Dashed lines depict the (a) peak operating length, (b) minimum knee flexion, and (c) maximum dorsiflexion during unimpaired gait at slow speeds.
We next evaluated whether each participant’s passive threshold was sufficient to achieve normal walking kinematics (i.e. the ankle dorsiflexion and knee extension required during unimpaired gait). The dotted lines in Figures 2(a) and 3(a) indicate the peak MG operating length required during unimpaired walking relative to each participant’s passive threshold. The MG’s passive threshold was less than the peak MG operating length required during unimpaired walking for all participants, except the left limb of P07 (Figures 2(a) and 3(b), dotted lines greater than 0). As a result, participants walked with either increased knee flexion (Figures 2(b) and 3(b)) or decreased ankle dorsiflexion (Figures 2(c) and 3(c)) in stance during barefoot walking compared to unimpaired gait. Both knee and ankle kinematics showed a linear relationship with the difference between the MG passive threshold and the MG length required for unimpaired gait (Figure 4). This demonstrates that a short and stiff MG contributes to altered knee and ankle kinematics.
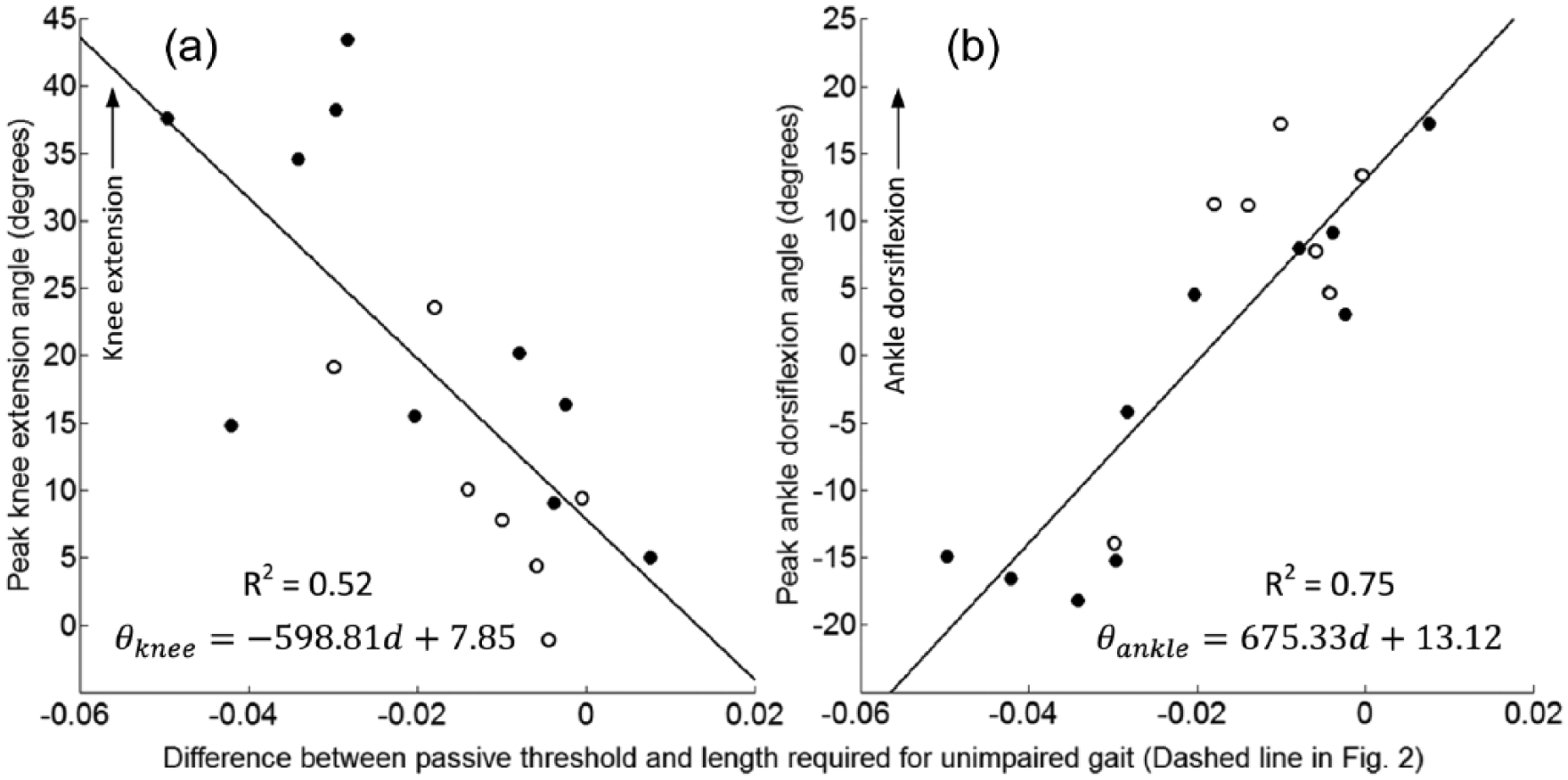
Correlation of (a) peak knee extension angle,
AFO: GMFCS Level I
The DAFOs increased peak MG operating length during gait compared to barefoot walking for 4/6 GMFCS Level I participants (Figure 2(a), gray bars). For three of these participants (P04, P05, and P06) the MG was stretched beyond the passive threshold measured during physical exam due to increased knee extension or ankle dorsiflexion in stance (Figure 2(b) and (c), gray bars). There were variable changes in kinematics and MG operating length between the different types of DAFOs. Of the participants who had posterior leaf spring DAFOs that aggressively resisted plantarflexion and moderately resisted dorsiflexion (DAFO 3.5—P01, P03, and P05), all had increased knee extension in stance (one into hyperextension). For the participants who had hinged or solid DAFOs that only blocked plantarflexion (DAFO 2, 3 or Tami2—P02, P04, and P06), all had increased MG operating length compared to barefoot walking. This suggests that aggressively resisting plantarflexion with a DAFO may play a role in increasing MG operating length. The ADR AFO increased peak MG operating length during gait compared to barefoot walking for the same 4/6 GMFCS Level I participants. For three of these participants (P02, P05, and P06) the MG was stretched beyond the passive threshold (Figure 2(a), black bars) due to increased knee extension and ankle dorsiflexion (Figure 2(b) and (c), black bars). However, two of the participants had knee hyperextension (P02 and P05) with the ADR AFO (Figure 2(b), black bars). The other two participants (P01 and P03) had similar or slight decreases in MG operating length compared to barefoot walking. Peak MG velocity during gait for the GMFCS Level I participants was relatively similar to slow unimpaired gait (6.81 × 10−4 normalized length/second, Figure 5(a), dashed line) and was consistent across conditions. Only one participant (P05) had a large decrease in peak velocity with the DAFO and ADR AFO, while the other participants had similar or increased lengthening velocity with both types of AFOs.
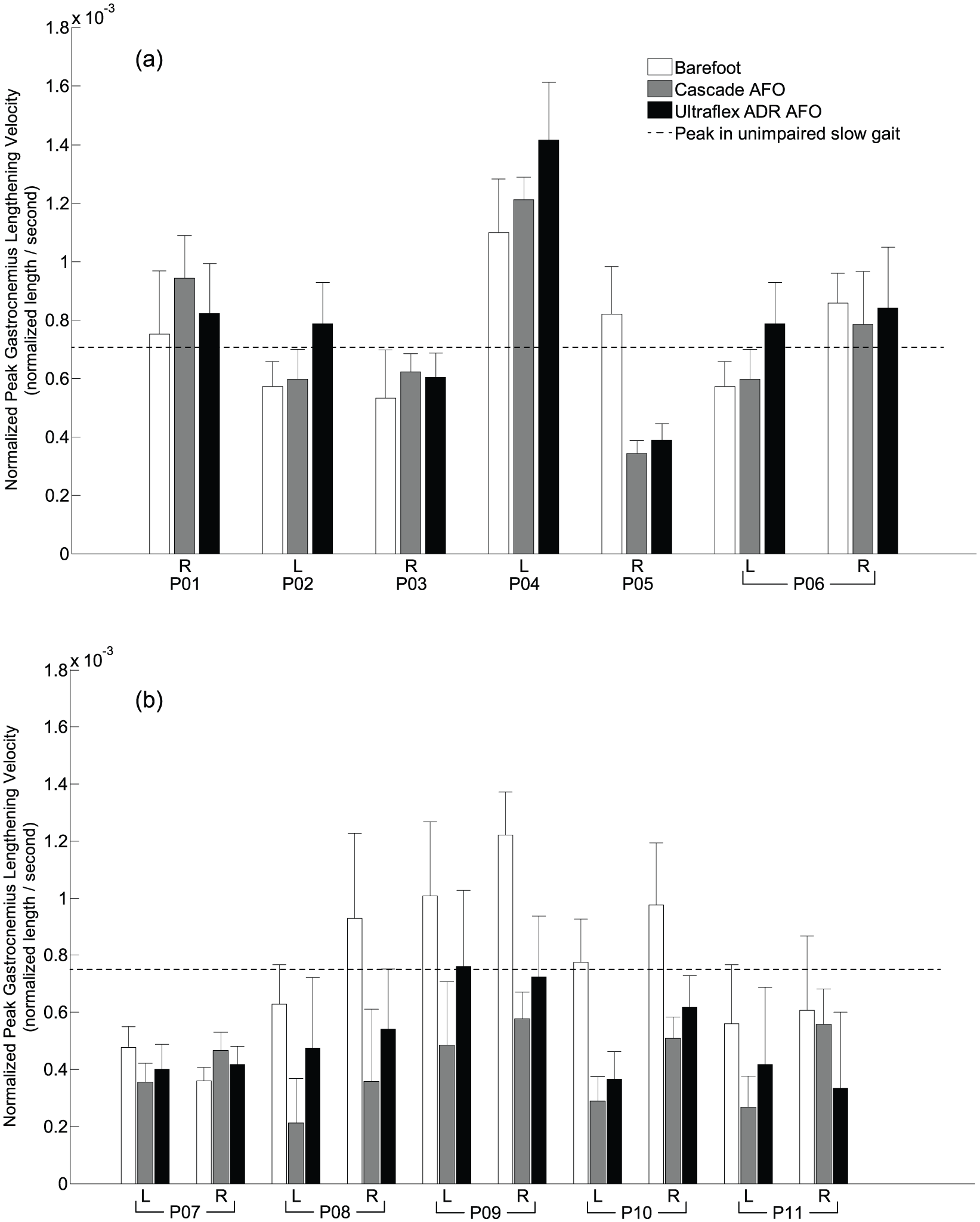
Average normalized peak medial gastrocnemius lengthening velocity during gait for the (a) GMFCS Level I and (b) GMFCS Level III participants. Comparisons are shown during walking barefoot (white bars), with DAFOs (gray bars), and with ADR AFOs (black bars). Error bars describe 1 standard deviation across multiple gait cycles for each gait condition. Dashed lines depict the peak medial gastrocnemius lengthening velocity during unimpaired gait at (a) slow speeds and (b) very slow speeds.
These results with the DAFO and ADR AFO demonstrate that AFOs could stretch the MG length for some GMFCS Level I participants, although sometimes with undesirable changes in kinematics (i.e. knee hyperextension). GMFCS Level I participants generally demonstrated similar changes in MG operating length and kinematics with the two different AFO prescriptions.
AFO: GMFCS Level III
The DAFOs increased peak MG operating length during gait compared to barefoot walking for all GMFCS Level III participants (Figure 3(a), gray bars), except P07 who already had a passive threshold similar to the peak length required during unimpaired gait. Changes in MG operating length with the DAFOs were primarily driven by increased knee extension or ankle dorsiflexion (Figure 3(b) and (c), gray bars). Unlike the GMFCS Level I participants, none of the GMFCS Level III participants had knee hyperextension with either AFO. Although MG operating length increased with the DAFOs, it only stretched the MG beyond the passive threshold for three of the participants (P08, P10, and P11). P11 had the greatest increase in MG operating length during gait with the DAFOs due to increases in both knee extension and ankle dorsiflexion. This participant had the most rigid DAFO, the Turbo, which likely contributed to the greater changes in kinematics and MG operating length.
The ADR AFOs increased peak MG operating length during gait compared to barefoot walking for 3/6 of the GMFCS Level III participants (Figure 3, black bars). However, only one participant (P09) had a greater increase in MG operating length and improvements in knee extension and ankle dorsiflexion with the ADR AFO compared to the DAFO. With the ADR AFO, none of the participants had an MG operating length significantly greater than the passive threshold on both limbs, suggesting the MG was operating in a shortened state during gait with this AFO. Both DAFOs and ADR AFOs decreased peak MG lengthening velocity during gait compared to barefoot walking, except for the right side of P07 (Figure 5(b)). MG lengthening velocity was generally slightly greater with the ADR AFO compared to the DAFO, except for P07 and P11 right sides.
These results demonstrate that the MG length was generally short during gait relative to its passive threshold and MG lengthening velocity tended to decrease for GMFCS Level III participants with both types of AFOs.
Discussion
In this study, we used musculoskeletal modeling to evaluate the influence of different types of AFOs on MG operating length, lengthening velocity, and gait kinematics for individuals with CP. Our results demonstrate that current AFO prescriptions can stretch the MG during gait for some individuals with CP. However, changes in MG operating length and velocity were variable between participants and types of AFOs. The heterogeneity among participants in this study reflect the clinical reality faced by practitioners prescribing AFOs. These results illustrate the variability in response to different types of AFOs, emphasizing the need to understand the underlying mechanisms by which muscle function changes with AFOs. Stretching of the MG was driven by increases in knee extension and ankle dorsiflexion in stance. However, in some participants, although the MG was stretched during gait with the AFOs, the participants had excessive knee hyperextension.
The AFOs used in this study were prescribed according to current clinical recommendations, but these results highlight the interplay of potential competing priorities in orthotic prescription. While an orthosis may stretch the MG during gait, this stretching may be due to undesirable changes in kinematics. Balancing improvements in kinematics, metabolic costs, and other therapeutic goals is a continuing challenge.
There was a difference in the response between GMFCS Level I and III participants to the different AFOs. While GMFCS Level I participants had similar changes in MG operating length and gait kinematics with the DAFOs and ADR AFOs, the GMFCS Level III participants often exhibited different responses to the two types of AFOs. The DAFOs provided more rigid resistive support than the ADR AFOs, which may contribute to the greater change in ankle dorsiflexion with the DAFOs for the GMFCS Level III participants. ADR AFOs allow orthotists to tune the stiffness of the AFO; however, a quantitative measure of the stiffness set for each participant was not available. The reported peak plantarflexion and dorsiflexion torques of ADR AFOs (40.7 and 27.1 N m, respectively) may not be sufficient for some GMFCS Level III participants. Furthermore, GMFCS Level III individuals generally have less strength, 31 and these individuals may put more of their body-weight on external walking aids, impacting changes in kinematics and MG operating length with AFOs. 32
Across GMFCS Level I and III participants, the passive threshold of the MG was less than that required for unimpaired gait. Unless individuals with CP have sufficient MG operating length, they will not be able to achieve the knee extension and ankle dorsiflexion required during unimpaired gait. During barefoot walking, the MG operating length was less than the passive threshold for all but one of the participants in this study, highlighting that the short and stiff MG is not stretched during barefoot walking. The fact that the MG operating length remained below the passive threshold suggests two alternatives for the impact of a short and stiff MG on gait kinematics. First, the passive threshold measured from a slow stretch in physical exam may over-estimate the range of motion possible during dynamic motion due to spasticity or other dynamic constraints. Second, other factors beyond MG contracture may contribute to an individual’s increased knee flexion and ankle plantarflexion during gait, including weakness, spasticity, 31 or adopting a crouched posture for stability. 33
Evaluating the rate of change in musculotendon length (i.e. velocity) can also be useful for evaluating points in the gait cycle where spasticity or other velocity-dependent effects may influence muscle function and motion. Among the GMFCS Level III participants, the peak MG lengthening velocity was less than that during unimpaired gait for the majority of the subjects. Both the ADR AFOs and DAFOs tended to further decrease MG lengthening velocity for this group, which could reduce the impact of spasticity during gait. Reducing MG lengthening velocity by constraining the ankle joint could improve knee joint kinematics by preventing excessive muscle activity. 34 However, if a participant has hamstring spasticity, a knee extension angular velocity could also trigger inappropriate muscle activity and limit improvements in knee kinematics during gait. Future studies that use quantitative assessments of spasticity 35 and monitor spastic thresholds could assist in understanding the role of spasticity on musculotendon dynamics with and without AFOs.
The variety of AFOs and pathological gait patterns in this study allowed us to evaluate how current AFO prescriptions may influence stretching or shortening of the MG during daily life. This variety introduced limitations, but also reflects the heterogeneity among individuals with CP and the diversity of AFO options currently available. We were unable to precisely quantify the stiffness of each AFO, which could provide valuable insight into the differences in response between individuals.36,37 Musculoskeletal modeling lets us evaluate the overall operating length of a muscle during movement; however, this reflects changes in length of both the muscle and tendon. An advantage of these methods is that they can be obtained from standard clinical gait analysis methods. To investigate whether AFOs can stretch muscle fascicles, leading to long-term improvements in function, future studies should incorporate techniques such as ultrasound to evaluate relative stretching of muscle and tendon.
The musculoskeletal model used in this study was a generic model based on the anatomy of unimpaired adults. This model assumes no bone deformities such as femoral anteversion or tibial torsion, which are common in children with CP and may influence the results of modeling studies.38,39 Among these bone deformities, tibial torsion could have an impact on gastrocnemius operating length. However, Hicks et al. 39 in 2007 demonstrated that tibial torsion deformity did not significantly affect gastrocnemius moment arms, which would suggest minimal effects of tibial torsion on the gastrocnemius musculotendon operating length estimated in this study. However, magnetic resonance imaging–based methods to create patient-specific musculoskeletal models for children with CP may enhance future research, although they are time and resource intensive.40,41 In this study, we were limited in our ability to statistically compare changes in MG operating length with kinematics due to the heterogeneity of participants AFO prescriptions. However, this heterogeneity demonstrates the “real-life” clinical situation and highlights the challenge for clinicians and orthotists to make patient-specific treatment decisions.
Muscles respond to the demands experienced in daily life, and this study represents a first investigation into whether AFOs may be able to help address short and stiff muscles among individuals with CP. Children with CP take fewer steps per day compared to typically developing peers; however, even GMFCS Level III children with CP take over one thousand steps per day. 42 If AFOs can help stretch short or stiff muscles, this may provide another tool for improving long-term function.
Conclusion
We found that the MG was stretched when walking with AFOs for some individuals. Whether this stretching is beneficial and could assist in rehabilitation during daily life will require further investigation. Furthermore, potentially stretching tight muscles with AFOs would need to be balanced with other purposes of orthoses such as reducing energy costs, improving gait kinematics, and preventing bone deformities. Since muscle impairments contribute to pathologic gait in CP and are a common target of more invasive treatments, we should consider changes in muscle operating length and long-term adaptations in future orthotic design and prescription.
Footnotes
Acknowledgements
The authors wish to thank James Dryden, CPO, for his orthotic expertise in this study; Sandra Dennis, PT, Susan Rethlefsen, DPT, Bitte Healy, PT, and Nicole Mueske, MS, for data collection and processing; and Keshia Peters for assistance with data analysis and interpretation.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Science Foundation under Grant No. CBET 1452646 and a research contract from Ultraflex Systems, Inc.