
Abstract
Background:
Orthotic treatment of idiopathic toe walking is complicated by the lack of a known etiology. This study compared control of toe walking using an articulated ankle–foot orthosis versus a rigid carbon fiber footplate attached to a foot orthosis.
Objectives:
Ascertain differences between two orthoses in the control of idiopathic toe walking.
Study design:
Randomized controlled trial.
Methods:
A total of 18 children with idiopathic toe walking were randomized to either the ankle–foot orthosis or foot orthosis treatment group in a Parallel Randomized Controlled Trial with no blinding. Prior to and after 6 weeks of treatment, participants completed three-dimensional gait assessment and the L-test of Functional Mobility. Parents completed a satisfaction survey and a subset of the Orthotic and Prosthetic User Survey after treatment.
Results:
Nine participants were analyzed in each group. Both groups showed significant improvement in kinematics versus baseline with orthoses; however, when the orthoses were removed, the ankle–foot orthosis group did not immediately sustain this improvement, while the foot orthosis group did. Parents preferred the foot orthosis for donning and appearance.
Conclusion:
The ankle–foot orthosis controls idiopathic toe walking, but subjects may revert to earlier patterns following treatment. The foot orthosis does not control idiopathic toe walking as well but is less restrictive and more accepted by children and their parents, with similar out-of-brace effects.
Clinical relevance
This study suggests that sequential orthotic treatment for children with idiopathic toe walking (ITW) may be beneficial. Initial treatment could include a less restrictive orthosis like a foot orthosis (FO); if this is unsuccessful within a set time frame, then the patient may require a more restrictive form of treatment such as an ankle–foot orthosis (AFO).
Keywords
Background
Idiopathic toe walking (ITW) is a common pediatric diagnosis for which there is no orthopedic, neurologic, or psychiatric causality. 1 ITW is a diagnosis of exclusion, given when other diagnoses like cerebral palsy, myopathy, neuropathy, and autism are ruled out.2–4 Classic presentation of ITW is a healthy child with normal muscle strength and control who chooses to walk on his or her toes. 4 Current etiological theories of ITW include increasing sensory stimulation to increase support tone in the lower limbs during walking and/or clinically undetectable neural impairments.5,6 Westberry et al. 4 argue that if a child diagnosed with ITW can achieve normalization of gait, he/she has been given an accurate diagnosis. Another definition is the absence of a heel rocker.6–8
Approximately 30% of patients have a family history of toe walking with greater incidence in boys than girls.6,9,10 Toe walking is considered abnormal when it persists beyond the age of 2 years and usually begins when the child starts to walk, which occurs at a normal time developmentally.9,11
Instrumented three-dimensional (3D) gait analysis showed ITW can be characterized by a short-lived dorsiflexion during initial contact followed by progressive plantarflexion throughout the rest of the stance and swing phase.4,7 Although ITW is characterized by a persistent tiptoe gait pattern, many children diagnosed with ITW can walk with a heel-to-toe gait pattern if they are asked or being watched.1,4,5 Furthermore, passive dorsiflexion range in idiopathic toe walkers was sufficient for ambulation. 7
ITW has both short and long-term impacts. Negative impacts on spatiotemporal gait parameters include decreased walking velocity secondary to decreased stride length and cadence. 4 ITW puts a child at greater risks for falling and requires greater effort than normal gait.7,11 ITW can lead to future orthopedic problems including contracted Achilles tendon, equinus position of the foot/ankle complex, lumbar spine hyperlordosis, deformities of bones and soft tissues in the feet, and abnormal adult gait.8,9,11,12 Consequently, early prevention of ITW may be important for development of a normal gait pattern and energy expenditure. 8
There is a lack of comprehensive information documenting outcomes for the orthotic treatment of ITW. 13 However, orthotic treatment exists as a conservative treatment method, along with passive stretching, serial casting, and botulinum toxin.10,13 Studies have investigated treatment of ITW using habit reversal and auditory feedback, Achilles tendon lengthening, and serial casting.8,9,11,14 One study deemed surgical intervention led to no better outcomes than orthoses for the treatment of ITW, but this study did not detail the types of orthoses used or compliance of wear by patients. 6
No randomized controlled studies have been conducted on orthotic treatment of ITW. At the study center, the standard treatment for ITW is an articulated ankle–foot orthosis (AFO) with a plantarflexion stop which blocks ankle plantarflexion and resists toe flexion. The biomechanics of this orthosis inhibit toe walking altogether. Clinicians are beginning to use less restrictive orthoses for ITW, such as supramalleolar orthoses and rigid footplates (B Veldman, 2010, personal communication). These orthoses are less biomechanically oriented to impede the toe walking and designed on the premise that ITW may have a sensory component5,6 that may not respond well to a motion-restricting orthosis. In essence, the premise of the AFO is to treat a purely mechanical equinus while the foot orthosis (FO) is treating a sensory-perceptual equinus. We aim to objectively compare outcomes between the AFO and FO with an attached rigid carbon fiber footplate in children with ITW.
Methods
We recruited children with ITW from area physical therapists and physicians. Subjects who met the following inclusion criteria were included in the Institutional Review Board (IRB)-approved study: diagnosis of ITW, between the ages of 2 and 8 years, and determined by their physician to be a candidate for orthotic intervention. The convenience sample was based on recruitment over a limited time frame. Exclusion criteria were diagnosis of any neurologic conditions, previous treatment for Achilles tendon contractures (including serial casting and surgery), or presence of a plantarflexion contracture that would prevent achieving a 90° ankle angle alignment. Following informed consent, we obtained a baseline gait assessment while the patients wore their own standard athletic shoes, as well as a medical history, measurement of ankle range of motion (ROM), instrumented 3D gait analysis, parental satisfaction survey, and L-test of Functional Mobility. 15
We conducted instrumented motion analysis at 100 Hz using a 7-camera Vicon Nexus System (Oxford, England) at the Georgia State University Biomechanics Laboratory. Following measurement of anthropometrics, we attached 15 reflective markers to lower extremity skeletal landmarks according to the Vicon Plug-in-Gait Sacrum model. We instructed subjects to walk at their normal pace along a 10-m walkway for five trials while gait kinematics were recorded.
After completion of the baseline assessment, subjects were randomly assigned to either the AFO or FO group (Figure 1) for a Parallel Randomized Controlled Trial (RCT). Blocked randomization with a computer random number generator and a 1:1 allocation ratio was used with approximately equal group sizes. Allocation was concealed until interventions were assigned. Allocation, enrollment, assignment, casting, modification, and fitting of the assigned orthosis were performed by the same orthotist so that consistency was maintained across all subjects. Device fabrication was standardized so that each AFO was fabricated from 1/8″ polypropylene with a 90° plantarflexion stop, free dorsiflexion, Tamarack joints, a full heel posting to give a neutral hindfoot alignment, a layover style calf strap, and a chafe and loop strap at the ankle. Trimlines were midline at the calf and foot with a full length toe plate with medial distal footplate trimlines proximal to the metatarsophalangeal joint at the first and fifth metatarsal heads. The custom FOs with attached carbon fiber footplates were fabricated from a full-length firm carbon fiber footplate from Otto Bock (Minneapolis, MN) attached to a cork base, layered with 1/8″ poron and 1/8″ puff. Because of practical difficulties caused by the appearance of the devices, no blinding was implemented.
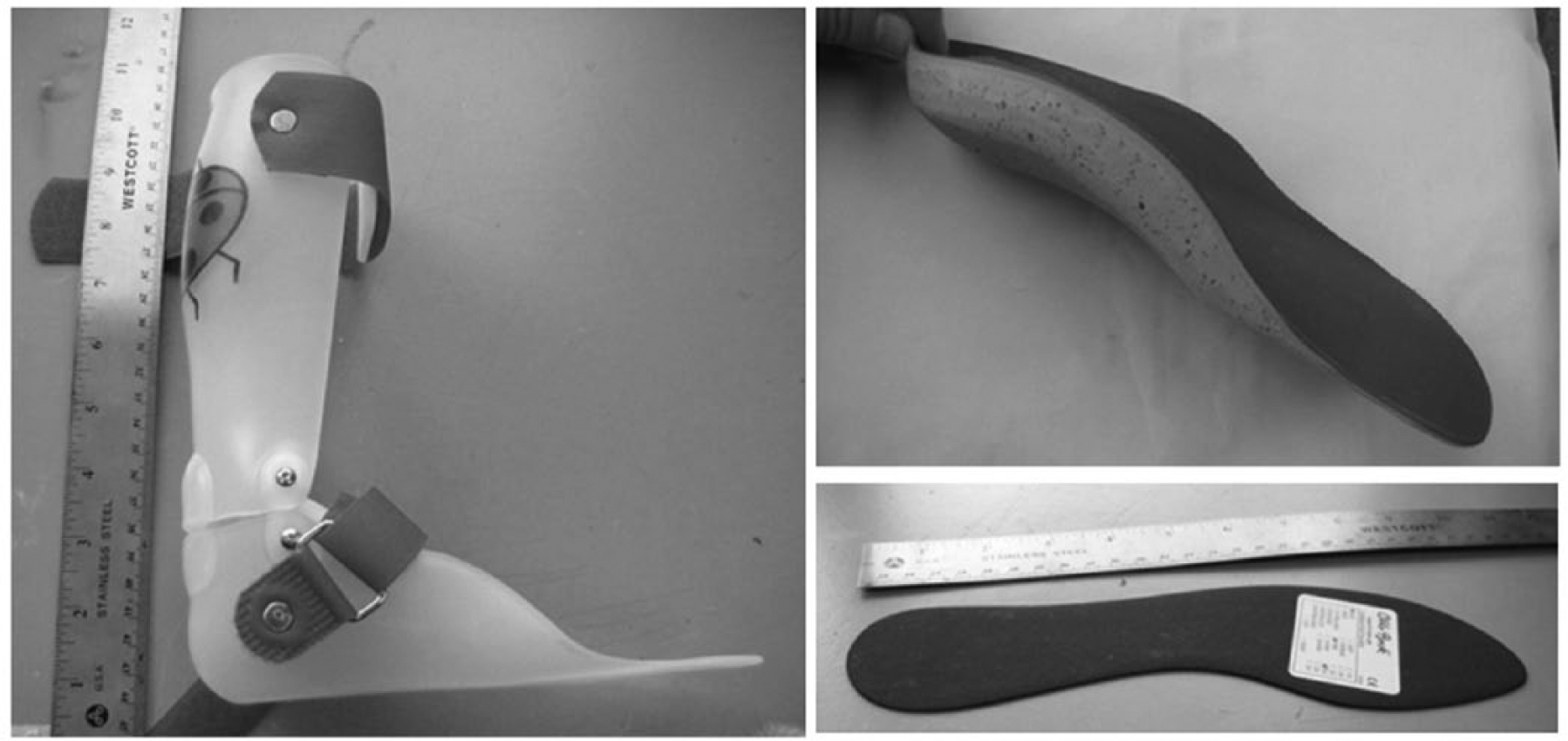
Orthoses. Photographs of articulated ankle–foot orthosis (left), foot orthosis (right top), and rigid carbon fiber footplate (right bottom).
At the fitting appointment, each child’s guardian was instructed to have the participant wear the device at all times except for sports activities and sleeping. Subjects wore the device for 6 weeks and then returned for a second assessment, which consisted of the same measurements and tests recorded for the initial baseline gait assessment, along with a subset of the Orthotic and Prosthetic User Survey (OPUS). 16 The 6-week treatment time was chosen to maintain a recruitment goal of 20 subjects (18 completed our study) within the single year duration of the study provided by the funding source. The 3D gait analysis and L-test were each conducted for two shod conditions: with and without orthosis.
Marker coordinate data were filtered using a Woltring spline filter with a predicted mean square error value of 10 mm 2 . Toe walking was defined according to Alvarez et al. 17 as initial contact with the forefoot or presence of early third ankle rocker. The latter was defined as the heel rise event occurring earlier than 30% of the gait cycle, which is one standard deviation less than the mean of 40%, when heel rise typically occurs. 17 Initial contact was determined by visual observation of the reconstructed foot segment in Vicon Polygon (v.4.0.1) software. Heel rise was determined using the Z (vertical) coordinate of the heel marker. The heel rise event was defined as a 1-cm increase in the Z-coordinate beyond the steady-state marker height at foot-flat.
Statistical analysis was conducted using Statistical Analysis System (SAS) 9.2 (Cary, NC); significance was assessed at the 0.05 level. Patient demographic and parental feedback data were compared between groups using two-sample t-tests for continuous measurements and Chi-square tests for categorical measurements. Cadence, step length, walking speed, and heel rise time taken from each trial for each participant were summarized within each condition (baseline shod, 6-week follow-up with shoes and orthosis, and 6-week follow-up with shoes only) and group (AFO vs FO) using means and standard deviations. Because the number of trials differed by subject, the number of observed data points also varied by subject. Thus, data were analyzed using a nested repeated measures analysis. The first repeated factor, trial, was nested within the second repeated factor, condition. The compound symmetric correlation matrix was used because the measurements were assumed to be uniformly correlated from trial to trial. Initially, all models included a treatment by condition interaction term; however, if the interaction term was nonsignificant, it was removed from the model.
Results
A total of 10 participants were assigned to the AFO group and 9 were assigned to the FO group. No subject was treated previously with an orthosis. Nine were analyzed in each group due to unavailability of one subject. Reported initial average walking age and initial average toe walking age were 12.1 ± 2.5 months and 17.9 ± 13.4 months, respectively (Table 1). A total of 11 participants began toe walking at the same time they began walking. Average passive dorsiflexion (DF) was 3.75° at initial entrance into the study. All subjects enrolled in the study had full plantarflexion ROM. There were no differences observed between groups when plantarflexion and dorsiflexion ROM were compared (p = 0.50). All parents of subjects involved in this study affirmed that their child could walk normally if asked to do so.
Participant characteristics.
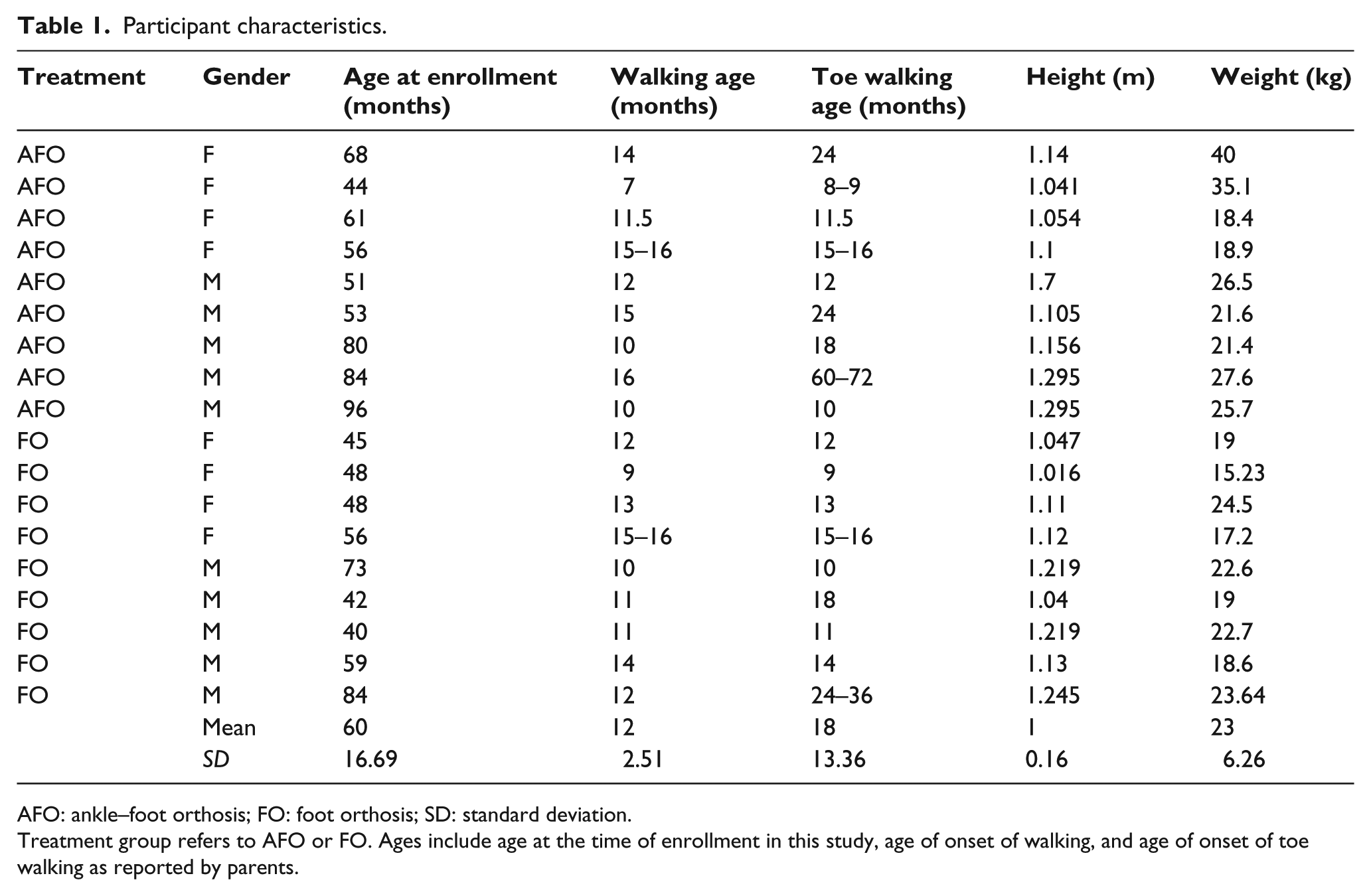
AFO: ankle–foot orthosis; FO: foot orthosis; SD: standard deviation.
Treatment group refers to AFO or FO. Ages include age at the time of enrollment in this study, age of onset of walking, and age of onset of toe walking as reported by parents.
Results of the parental satisfaction survey were mixed. No differences were seen between groups for parental report of time spent toe walking while wearing the orthosis (p = 1.0) or parental satisfaction with gait after treatment with either orthosis (p = 0.38) (Figure 2(a)). No differences were seen between the groups when parents were asked to rate the effectiveness of the orthosis (p = 0.73) (Figure 2(b)).
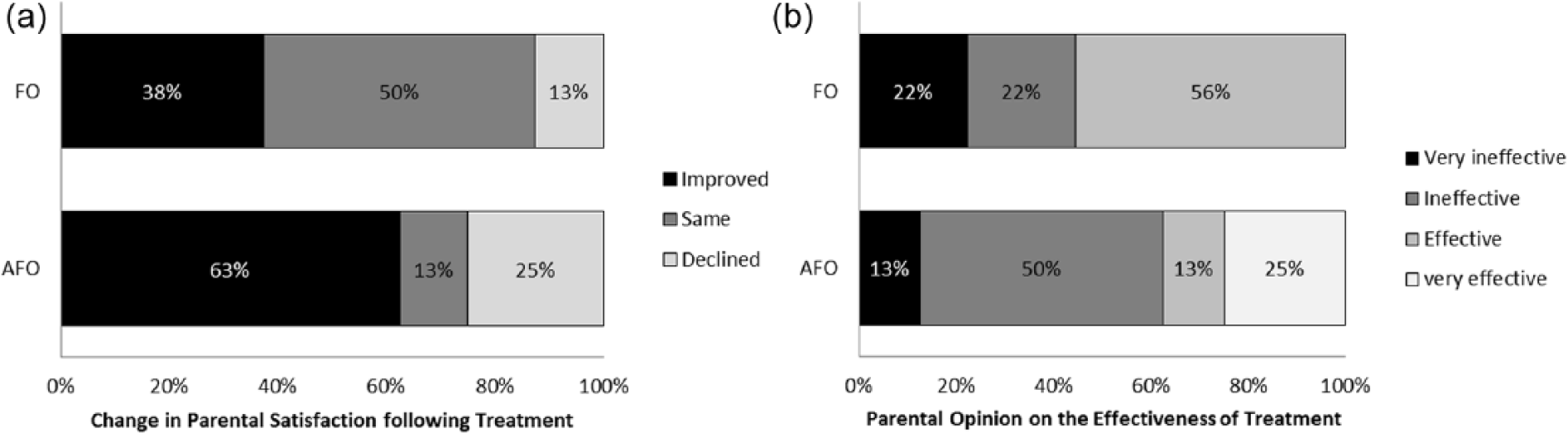
Parental satisfaction with orthoses and treatment outcomes: (a) change in parental satisfaction with the FO and the articulated AFO following treatment for each group and (b) parental opinion on the effectiveness of treatment with the FO and the articulated AFO following treatment for each group.
When answering the OPUS, significantly more parents felt donning the FO was easier than the AFO (p = 0.049). Although not significant, more parents felt the FO was more aesthetically appealing and less likely to cause skin breakdown than the AFO (p = 0.053 and 0.070, respectively). Although not statistically different (p = 0.23), compliance was reported in the OPUS survey as 9.7 ± 1.48 h/day and 11.33 ± 2.44 h/day for the AFO and FO groups, respectively.
No statistical differences were seen between groups or conditions in time to complete the L-test (p = 0.62 at baseline, p = 0.55 at follow-up with orthoses and shoes, and p = 0.92 at follow-up with shoes only).
Temporal and spatial parameters and heel rise timing showed no significant difference between groups at baseline (cadence p = 0.854, step length p = 0.430, walking speed p = 0.551, and heel rise time p = 0.853). Mean walking speed across all steps and subjects was 1.27 m/s. The AFO group walked significantly faster (1.36 ± 0.25 m/s, p = 0.006) than the FO group (1.22 ± 0.19 m/s) at follow-up when the orthosis was worn (Figure 3(a)). Cadence and step length showed no differences between treatment groups (p = 0.286 and 0.194, respectively). The AFO group showed slightly higher results in cadence and step length at both follow-up conditions (Figure 3).
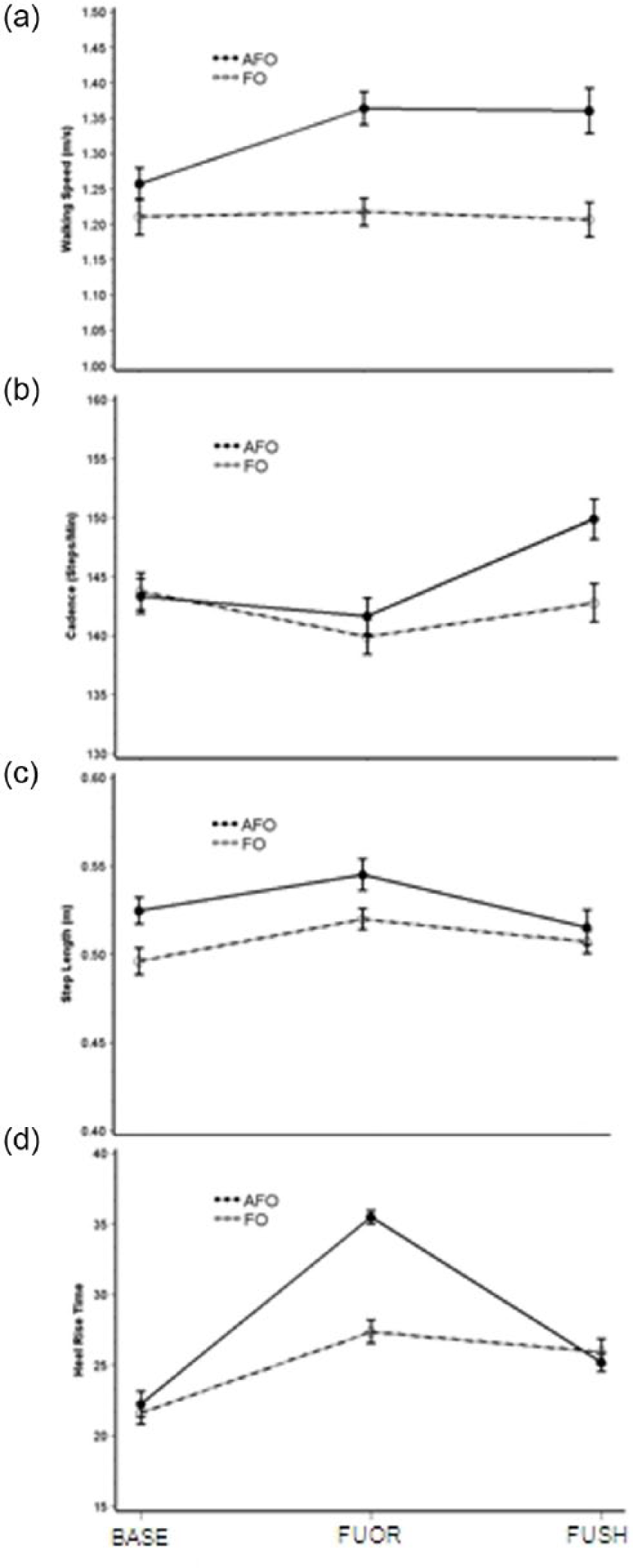
Kinematic results by group. Results from each group at three conditions for walking speed (m/s), cadence (steps/min), step length (m), and timing of heel rise event (% of gait cycle). AFO group is represented by a solid line and FO group by a dashed line. BASE = baseline condition with shoes only; FUOR = follow-up following 6 weeks of treatment tested with shoes and orthoses; and FUSH = follow-up with shoes only and no orthoses.
Out of 1682 steps assessed across all subjects at baseline, 20% showed initial contact with the forefoot, while 80% showed initial contact with the heel or with a flat foot. At follow-up, when 1495 steps were assessed in the in-orthosis condition and 1461 were assessed in the shoes-only condition, some differences between the treatment groups emerged (Figure 4). AFOs were 100% effective at preventing initial contact with the toe, while in the FO group, 13% of the steps with the orthoses showed either flat-footed or toe contact.
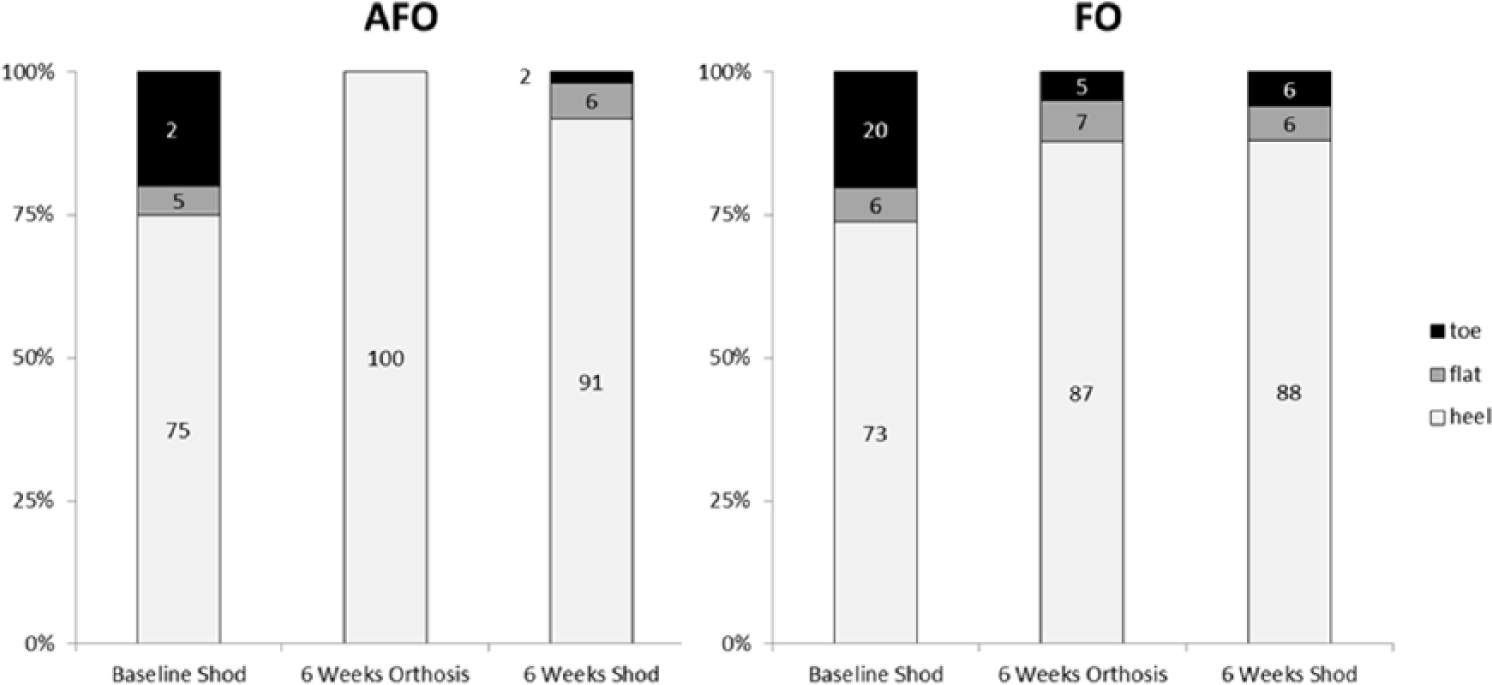
Initial contact results. Percent of steps at each condition with initial contact at the heel, on the flat foot, or at the toe. Baseline Shod = baseline condition with shoes only; 6 Weeks Orthosis = follow-up following 6 weeks of treatment tested with shoes and orthoses; and 6 Weeks Shod = follow-up with shoes only and no orthoses.
Despite the presence of initial heel contact, the majority of flat-footed or heel contact steps showed an early occurrence of the heel rise event. In fact, the only mean result for heel rise timing within normal limits was in the AFO group at follow-up while wearing the orthosis (mean heel rise at 35.5% ± 5.2% of gait cycle). All other groups and conditions showed mean heel rise earlier than 30% of the gait cycle.
Heel rise time was significantly different (p = 0.008) between groups when the orthosis was worn, but was not significantly different (p = 0.734) at follow-up in the shoes-only condition. Within each group, follow-up was compared to baseline. The AFO group showed significant improvement versus baseline (p < 0.001) while wearing AFOs, but did not sustain this improvement in the follow-up condition with shoes only (p = 0.175). The FO group also showed significant improvement versus baseline (p < 0.001) while wearing FOs; however, this group was able to maintain this improvement when the orthoses were removed (p < 0.001) (Figure 2).
Discussion
This study evaluated the effects of two different orthoses on the gait of children with ITW revealing multiple effects. The AFO group walked faster, through a combination of increased cadence and increased step length. While constraint of additional joints can lead to decreased walking speed, the opposite occurred in this case since step length is arrested when the toe contacts the ground first. Furthermore, typical swing phase propulsion via the A2 power burst18,19 that is based on a full range of triceps surae contraction is compromised when ROM is limited following toe contact or through early heel rise. Early plantarflexion tends to raise the height of the body center of mass as opposed to providing swing phase propulsion. Consequently, elimination of all toe contact is expected to improve walking speed in otherwise typically developing populations.
It is difficult to compare results of the study to existing literature as few studies systematically examine orthotic intervention in this population. Other studies have examined the effects of orthoses but for various treatment lengths and in combination with other modalities.20,21
The results for heel rise time in particular support the philosophical basis for the hypotheses of this study. It is apparent that 100% control of toe walking through the prescription of an AFO is not always sustained when the AFO is not worn, at least within the confines of this study (6 weeks of wear and assessment of immediate carryover effect). This finding is consistent with other studies which see regression of toe walking when not wearing AFOs. 20 This is important because the long-term goal of orthosis prescription in ITW is to train children toward a more typical heel-to-toe gait pattern. Orthotic treatment is intended to be short term. So, while the AFOs performed significantly better than the FOs when the orthosis was being worn, subjects reverted to their familiar ITW gait when the AFO was removed. This result underscores the need to assess both proper length of treatment and outcomes following the cessation of orthotic intervention. Although this study did not assess long-term carryover, the FO group, not the AFO group, showed significant improvement over baseline in the shoes-only follow-up. Minimizing invasive treatments such as surgery and Botox injections for this diagnosis is a theme in current literature which is highlighted in the findings of this study. 22 Consequently, less intrusive orthoses should also be considered in future studies of longer term interventions and carryover effects.
In the clinic, statistical differences were seen for very few of the measures. This finding might highlight limitations in some clinical outcome measures. The fact that neither orthosis appeared to limit the child’s function during the L-test of functional mobility indicates that laboratory testing might be required to identify the more subtle features of toe walking such as early heel rise. These findings might suggest new interpretation of other studies22,23 that reported a treatment’s ability to resolve toe walking but did not include instrumented 3D gait analysis. Given that all children in our study could achieve normal ankle ROM (which is consistent with the literature report of typical ITW presentation), 7 the sit-to-stand and stand-to-sit features of the L-test do not discriminate, and since time is the only outcome, toe walkers of different severities could have achieved similar results.
The fact that parents of children in either group did not report noticing a difference in time spent toe walking, compared to opposite observations made in the laboratory, may be explained by the environment in which the parent observed the child the majority of the time. It would be an oversight to disregard the contrast between the laboratory environment and a participant’s home/school environment when analyzing data for a population with a poorly understood pathology such as ITW. It is likely that participants in this study may have walked differently within the clinic/laboratory than they did while at home. 24 Early heel rise therefore becomes a potentially valuable clinical measure, as it indicated altered gait even when children with ITW adopted a heel-to-toe gait pattern. Use of early heel rise as an indicator of ITW is based on the assumption that initial heel contact with early heel rise in the laboratory is correlated with initial toe contact elsewhere.
One result from parental feedback is particularly surprising. There were no significant differences between groups for parental report of time spent toe walking while wearing the orthosis (p = 1.0). Mechanically, the AFOs prevent initial toe contact without gross adaptation in proximal joints, such as excessive hip and knee flexion, whereas the FOs would require less adaptation for the child to achieve initial toe contact. Our laboratory results corroborated this. Anecdotal evidence strongly suggests that if there is a difference in gait in this population between home and the laboratory, toe walking will be observed more at home than in the lab. However, this parental report would appear to contradict this result. Given the mechanical basis for the difference between the orthoses, this result might call into question the reliability of parental feedback in this study.
There are several limitations associated with the study. In addition to the aforementioned issues associated with clinical outcome measures and parental feedback, the time participants spent wearing orthoses was limited by the recruitment schedule and the term of grant funding. Given that many published studies use a variety of treatments in combination for various lengths of time, it has been difficult to establish the minimum required time of orthosis wear based on the current literature. 21 Some anecdotal observation and subjective parental feedback suggested that a longer time span of orthosis use, on the order of several months, might have changed the results. While this is likely, the study did demonstrate relatively rapid results, and given that orthosis wear in this population is meant to be temporary, additional research is warranted to determine appropriate wear duration.
In addition, the study population had a broad age range (3.3–8 years of age) and likely represented different gait patterns. The randomization scheme resulted in an older mean age at enrollment in the AFO group (65 months) versus the FO group (55 months), but the difference was not significant (p = 0.17). In addition, as previously stated, temporal and spatial parameters and heel rise timing showed no significant difference between groups at baseline.
The sample size is relatively small for a RCT, such that the project might be viewed as a pilot. Nonetheless, post hoc power analysis showed that group sample sizes of 9 and 9 are only slightly underpowered at 76% power to detect a difference of 9.0 between the null hypothesis that both group heel rise time means are at 36.0% of the gait cycle and the alternative hypothesis that the mean of the FO group is 27.0% of the gait cycle with estimated group standard deviations of 5.0 and 8.0 (AFO and FO, respectively) and with an alpha level of 0.05 using a two-sided two-sample t-test.
Naturally, these results are measured across multiple subjects, and individual results varied. Clinicians involved in the study observed that some subjects within both groups seemed better suited for their prescribed orthosis than others. Consequently, it is unwise to interpret these data to mean that a certain orthosis type is better in all cases. Future research should consider identification of additional indicators to predict effectiveness of certain treatments for particular patients.
Conclusion
Both orthoses affected gait in children with ITW. While the orthosis was being worn, the AFOs had a greater effect at reducing indicators of toe walking, including initial contact with the toe and early heel rise. Following orthosis removal, only the FO group showed significant improvement versus baseline. The rigid FO was generally preferred by children and parents.
Footnotes
Acknowledgements
The authors acknowledge the valuable assistance from Karl Barner, CPO, Children’s Healthcare of Atlanta Orthotics and Prosthetics Department; Courtney McCracken, PhD; Bernie Veldman, CO; and Hsin-Chen FanChiang, PhD.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
None declared.
Funding
This research was supported by a grant from the Orthotic and Prosthetic Education and Research Foundation (OPERF-2011-SGA-1). The funding agency was not involved in study design, data collection, data analysis, manuscript preparation, and/or publication decisions.