
Abstract
Background:
Flexor tendon repair in the hand remains challenging in avoiding tendon rupture and adhesion formation. Post-operative mobilization has been shown to be critical in regaining functional range of motion.
Objectives:
The objective of this study is 2-fold: to assess the influence of wrist position on maximum grip force generated in a post-operative orthosis and to determine the correlation between this maximum grip force and an individual’s grip strength.
Study design:
Clinical measurement
Methods:
A total of 30 uninjured wrists of right-handed men were given a post-operative orthosis with an incorporated Caroli-hinge. The maximum grip force was measured according to a different wrist position ranging from −30° extension until 80° of flexion using a 10° interval. These measurements were plotted out on a graph for regression analysis. A correlation was determined between measurements in a neutral wrist position and maximum grip strength generated without an orthosis. To assess the coherence of the measurements, a mean intraclass correlation coefficient was used.
Results:
The maximum grip force values were statistically significantly different in every wrist position and decreased progressively with an increasing flexion angle (p < 0.05). This relationship is expressed in a logistic regression curve f(x) = −4.98 + 16.92/(1 + (x/8.59))2.24. A wrist position of 4.4° of flexion was derived from this function to cause a maximum grip force reduction of 33%. Further analysis showed a force decrease of 50% at 23.2° and 66% at 51.8° of wrist flexion. The grip strength measured without an orthosis showed a positive correlation with previous measurements (Spearman’s correlation coefficient = 0.74 for the right hand and 0.72 for the left hand (p < 0.001)).
Conclusions:
The obtained logistic function allowed to derive the wrist position needed in a post-operative orthosis to obtain a desired amount of maximum grip force reduction.
Clinical relevance
Measuring a high grip force in a clinical setting of flexor tendon repair on the contralateral non-affected hand could indicate the use of an increased flexion angle in a post-operative orthosis. This reduces the load transferred on the tendon repair when involuntary contractions take place, for example, during sleeping when positioned in a post-operative orthosis.
Background
Flexor tendon repair in the hand remains challenging. 1 A recent meta-analysis has shown rates of re-operation of 6%, rupture of 4%, and adhesions of 4%. 2 Post-operative treatment has been shown to be critical to regain functional range of motion, even after a state-of-the-art tendon repair.1,3–5 A recent systemic review analyzing all flexor tendon zones showed a higher risk of rupture in early active motion protocols and a higher risk of decreased digit range of motion in the passive motion protocols. 5 These results indicate the difficulty in finding the ideal balance between achieving enough tendon excursion to prevent adhesion formation without creating profound tensional stress that would compromise the repair. Stress reduction is therefore particularly important in the first weeks when the sutured tendon is changing from a cellular to a fibrous healing response.6,7
A high grip force has been shown to correlate with an increased load transferred on the flexor tendons and could therefore cause early rupture when appearing after a sudden involuntary contraction. 8 Early biomechanical studies already showed that a wrist positioned in flexion causes a lower maximum grip force when compared to a wrist left in neutral or positioned in extension.9,10 However, these studies lack a clear mathematical relationship between those different wrist positions and the extrapolation toward a possible use in clinical practice.
We hypothesized that there would be a mathematical relationship between wrist position and maximum grip force in a post-operative orthosis that could be of use in clinical practice. Therefore, the objective of this study was 2-fold: to determine graphically the influence of these different wrist positions on maximum grip force generated in a post-operative orthosis and to assess whether a person’s maximum grip strength as measured in clinical setting concords with a maximum grip force measured in a post-operative orthosis.
Methods
Study population
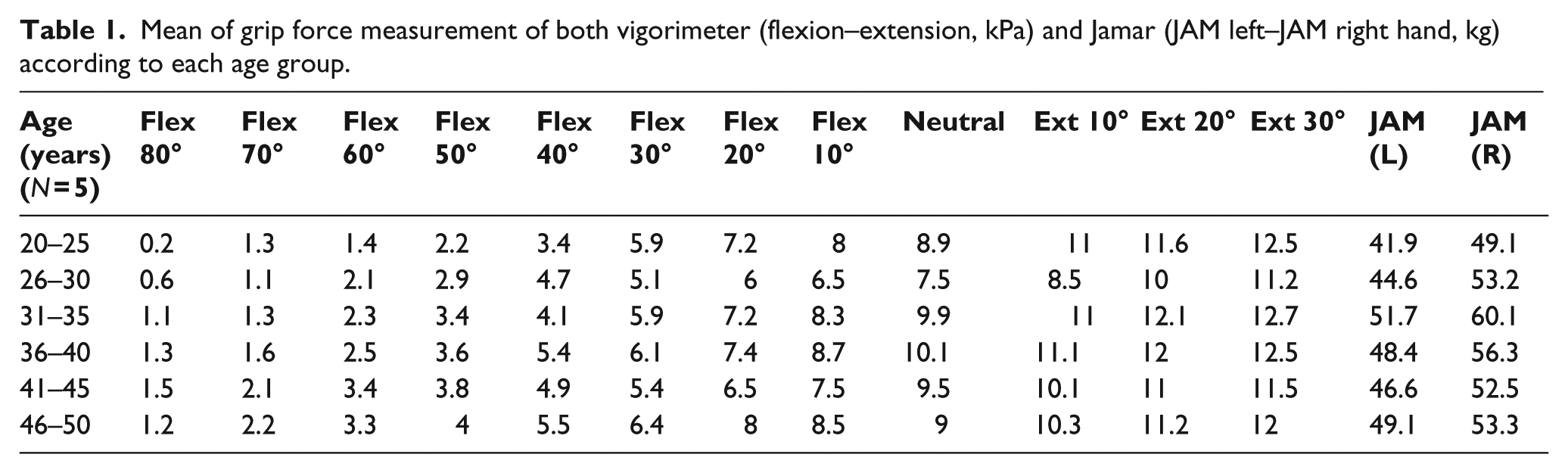
A total of 30 male, right-handed, orthopedic technicians (mean age: 38.4 ± 5.1 years; range: 20–50 years) participated in this study. Age distribution was equimodal with N = 5 in every 5 years of age interval (Table 1). The subjects had no known trauma or neuropathy in the hand or upper extremity that would affect the grip strength. All participants read and signed an informed consent. The research was performed and approved at the Thomas More University College, Geel, Belgium, by their ethical commission guidelines.
Mean of grip force measurement of both vigorimeter (flexion–extension, kPa) and Jamar (JAM left–JAM right hand, kg) according to each age group.
Study design
Subjects were fitted on the dominant (right) hand an orthosis made out of low-temperature thermoplastic (LTTP) material and constructed as described by Kleinert with metacarpophalangeal (MCP) joints blocked in flexion. 11 An MCP angle of 90° was used to neutralize the influence of the intrinsic hand muscles. 12 A Caroli-hinge was incorporated, allowing to set different wrist angles ranging from 80° of flexion until 30° of extension.
The maximum grip strength was measured using a Martin vigorimeter (Martin; Elmed, Addison, IL, USA), because it fitted the orthosis as opposed to the Jamar dynamometer. Although the Martin vigorimeter is a pressure measure (grip strength expressed in bars (1 bar = 105 Pa = 1 N/m2)), implying a dynamic movement in contrary to the static strength measure of the Jamar dynamometer, the results indicate a high correlation between both measurements. 13
Each subject was seated in a chair with both feet on the floor, allowing the hips, knees, and ankles to be positioned at approximately 90°. On the upper limb, the shoulder was positioned according to a neutral posture, the elbow in 90° flexion, and the forearm with 0° of pro-supination. In response to a standard verbal order, subjects were instructed to exert a maximal grip.
In the first part of the study, the maximum grip in a post-operative orthosis according to each different wrist position was measured. The measurements started with a wrist position of 30° of extension, and from this point on repeated at a 10° interval until 80° of flexion was reached (Figure 1). A set of three consecutive measurements for each wrist position was used with 1 min of rest between each set.
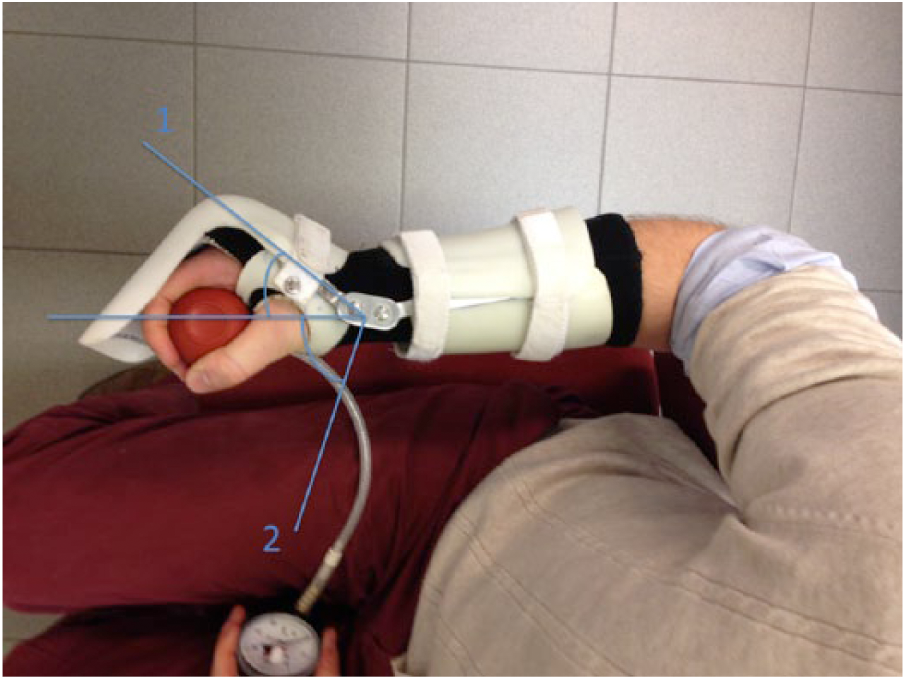
Maximum grip force was measured on a 10° interval starting in position 1 and ending in position 2 when seated in a neutral posture.
The mean out of three measurements for each wrist position was calculated and used for further analysis. The second part of the study investigated whether the grip strength of the non-affected hand without an orthosis can be used to have an estimation of the grip force expressed in a post-operative orthosis.
For this, the maximum grip strength was determined on both left and right hands without an orthosis using the Jamar dynamometer in a neutral position as proposed by the American Society of Hand Therapists (ASHT). 14 As in the first part of the study, the mean out of three measurements was used for further analysis. Resting time of 1 min was used between measuring the right and the left hands.
The obtained grip strength measurements without an orthosis were subsequently compared to the maximum grip force value obtained from the fixed neutral position in the orthosis. A correlation analysis was performed to investigate this relationship. In clinical practice, this setting could be of use because the generated grip force will determine the force transmitted on the finger flexors and hence on the sutured tendon. 8
Statistical analysis
The maximum grip force measurements observed in the first part of the study were plotted in a graph chart and curve analysis was performed by SigmaPlot software (release 12.5; Systat Software, Inc., San Jose, CA, USA). Analyzing normality was performed using the Shapiro–Wilk test. This could not point out the presence of a normal distribution in all the obtained data; further analysis was therefore performed using non-parametric tests.
Comparison of mean maximum grip force measurements between each different wrist position in an orthosis was performed using the Mann–Whitney U test. Their ranks were analyzed using the Kruskal–Wallis test. The correlation between the maximum grip force measured in an orthosis and without an orthosis was assessed by the calculation of the Spearman’s coefficient and visualized by a corresponding scatterplot.
To assess the coherence of three subsequent grip force measurements, an intraclass correlation coefficient (ICC) was used for each wrist position. The SPSS (release 20.0.0, standard version; SPSS, Inc., Chicago, IL, USA) statistical package was used to analyze the results. A probability level of p < 0.05 was considered significant.
Results
Assessment of grip force generated in an orthosis
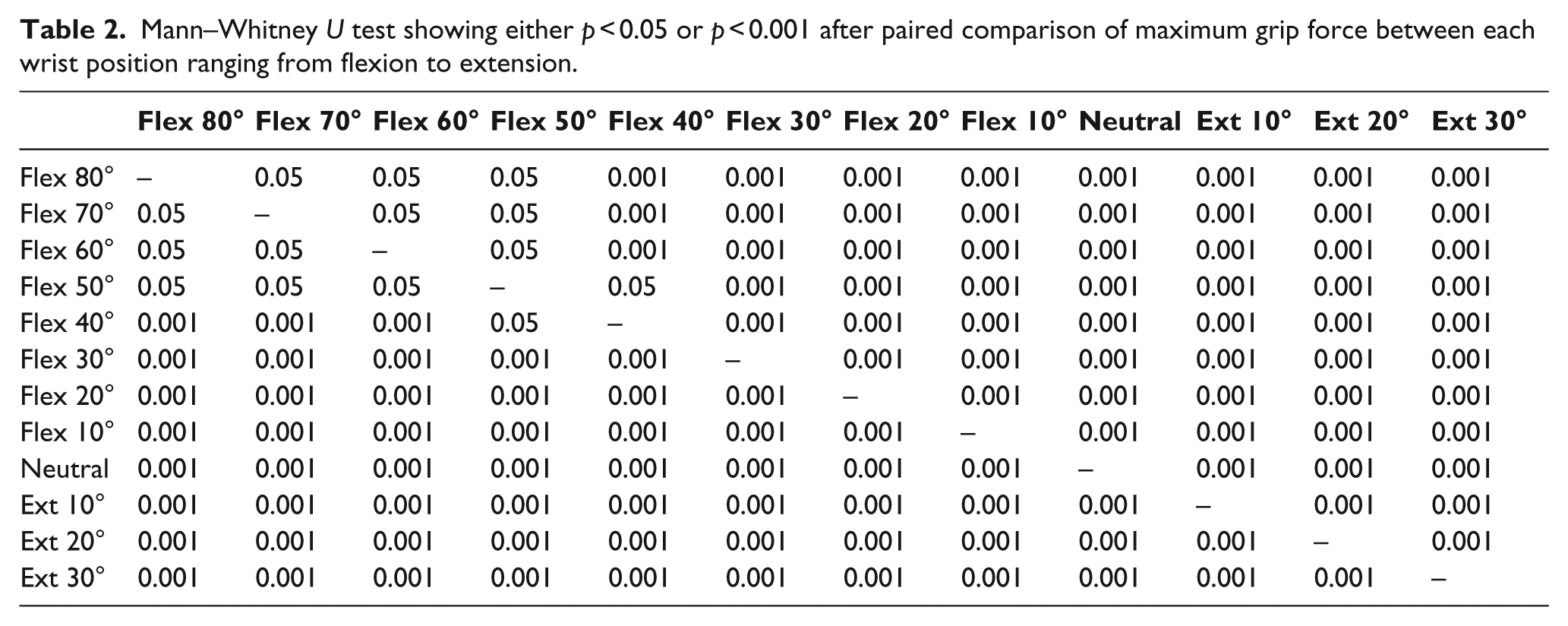
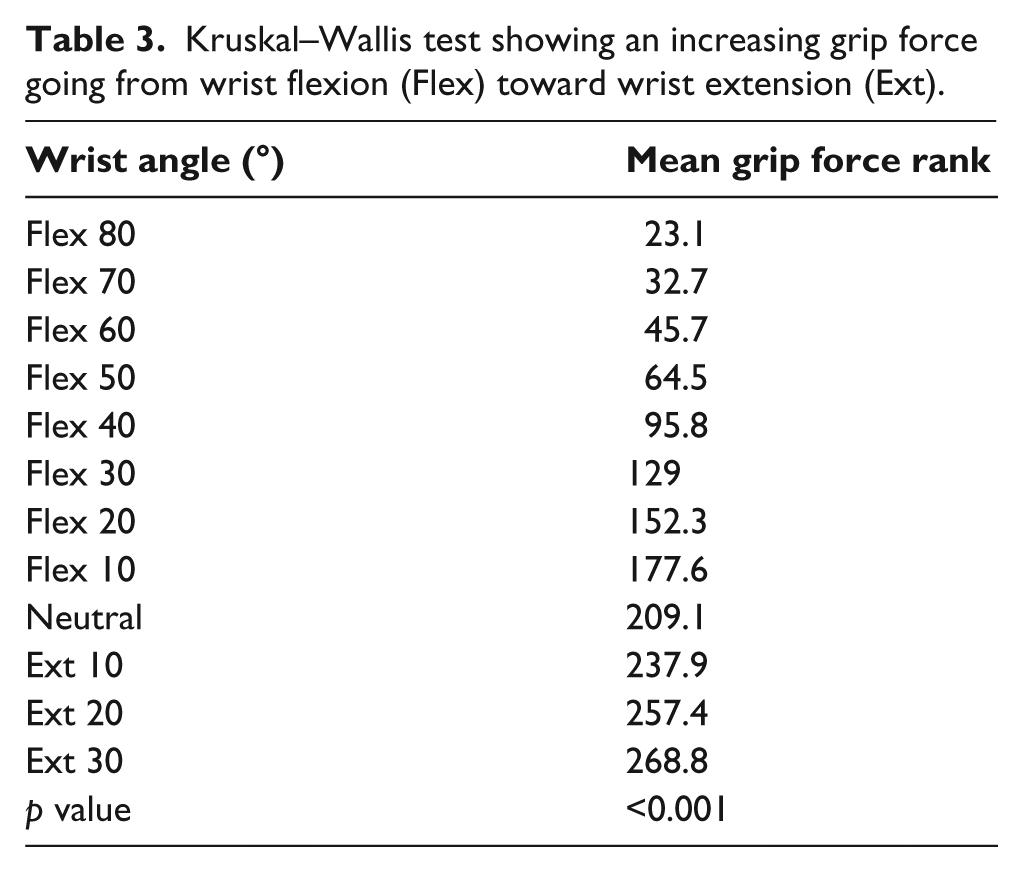
The maximum grip force values (kPa) are shown according to a different wrist position (Table 1 and Figure 2(a)). Paired comparison of grip force measurement showed a statistically significant difference between each wrist position (p < 0.05) (Table 2). This difference showed a significant progression in maximum grip force going from flexion to extension (Table 3). The decrease in maximum grip force accorded to a logistic function f(x) = −4.98 + 16.92/(1 + (x/8.59))W2.24.
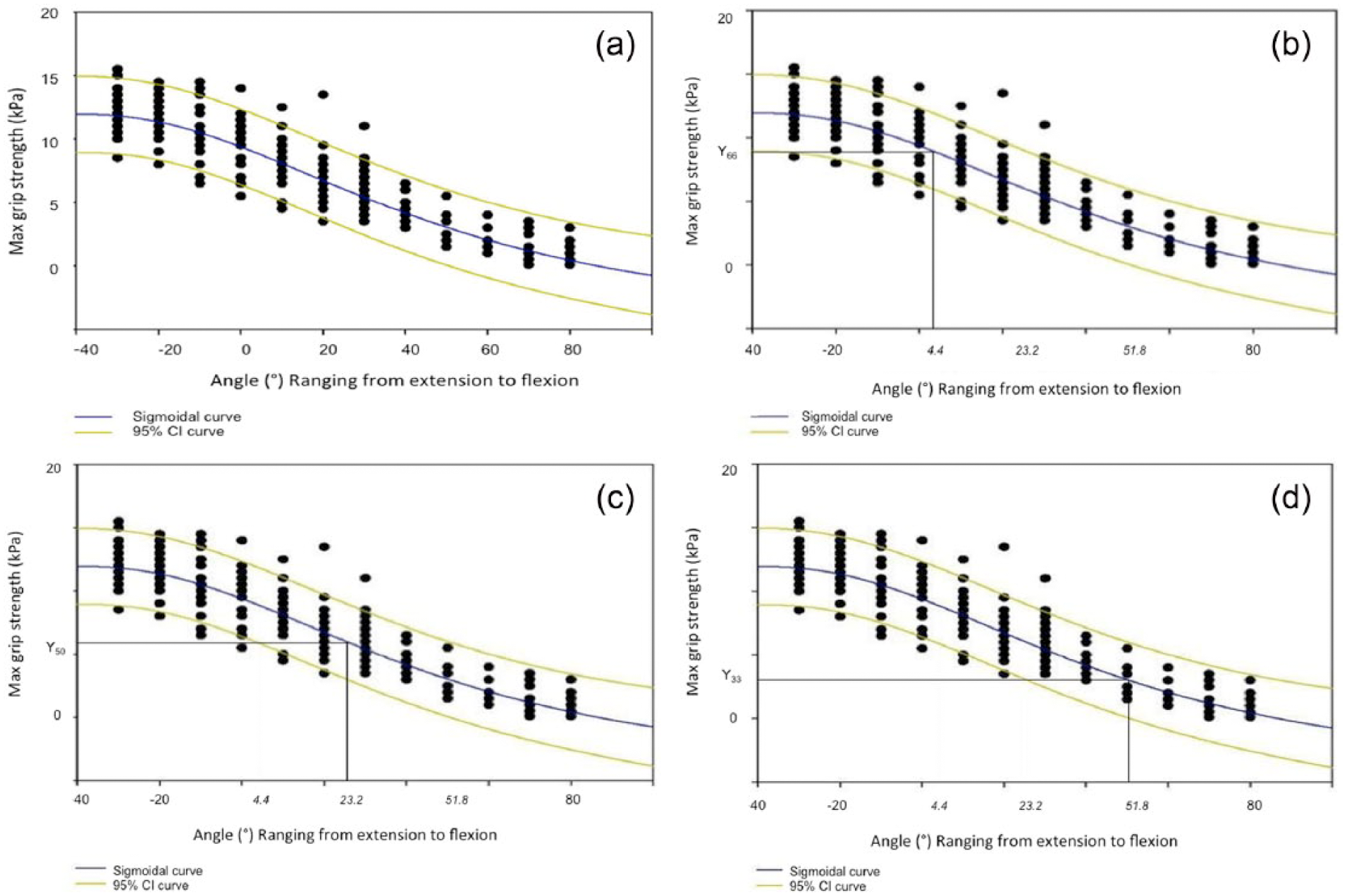
(a) Logistic regression curve according to different wrist positions (b) to (d). Wrist position necessary to achieve a maximum grip force reduction (MGR) of 33%, 50%, and 66%.
Mann–Whitney U test showing either p < 0.05 or p < 0.001 after paired comparison of maximum grip force between each wrist position ranging from flexion to extension.
Kruskal–Wallis test showing an increasing grip force going from wrist flexion (Flex) toward wrist extension (Ext).
A wrist position of 4.4° flexion was derived from this function to cause a maximum grip force measurement (MGM) reduction of 33% (Figure 2(b)). Further analysis showed a MGM decrease of 50%, MGM50 = 23.2° and MGM66 = 51.8° of wrist flexion (Figure 2(c) and (d)). The mean of the ICCs for each different wrist position equaled 0.92 (Table 4).
ICC according to each different wrist position going from wrist flexion (Flex) toward wrist extension (Ext).
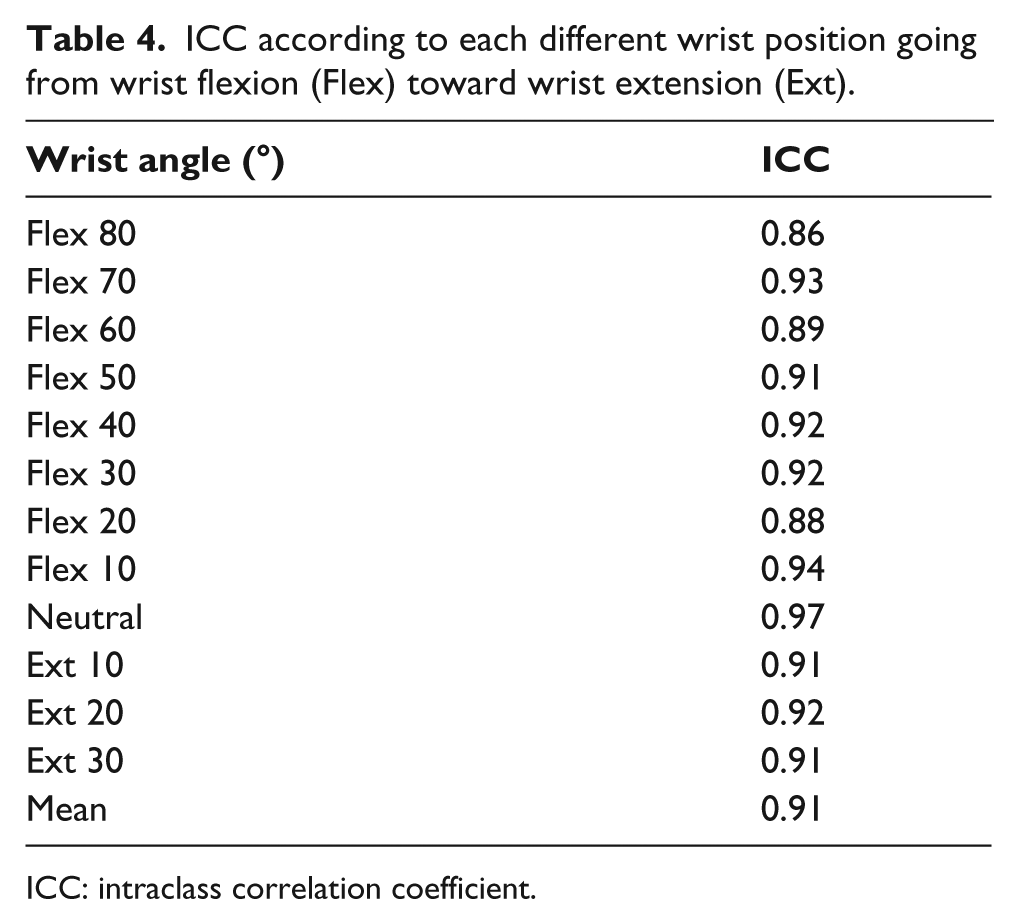
ICC: intraclass correlation coefficient.
Assessment of grip force generated without an orthosis
The mean maximum grip force values (kg) of both the left (non-dominant) hand and the right (dominant) hand measured without an orthosis are positively correlated to the concomitant wrist positions in an orthosis according to a Spearman’s correlation coefficient of 0.72 for the left hand and 0.74 for the right hand (p < 0.001) (Figure 3). The mean of the ICCs for each different wrist position equaled 0.87.
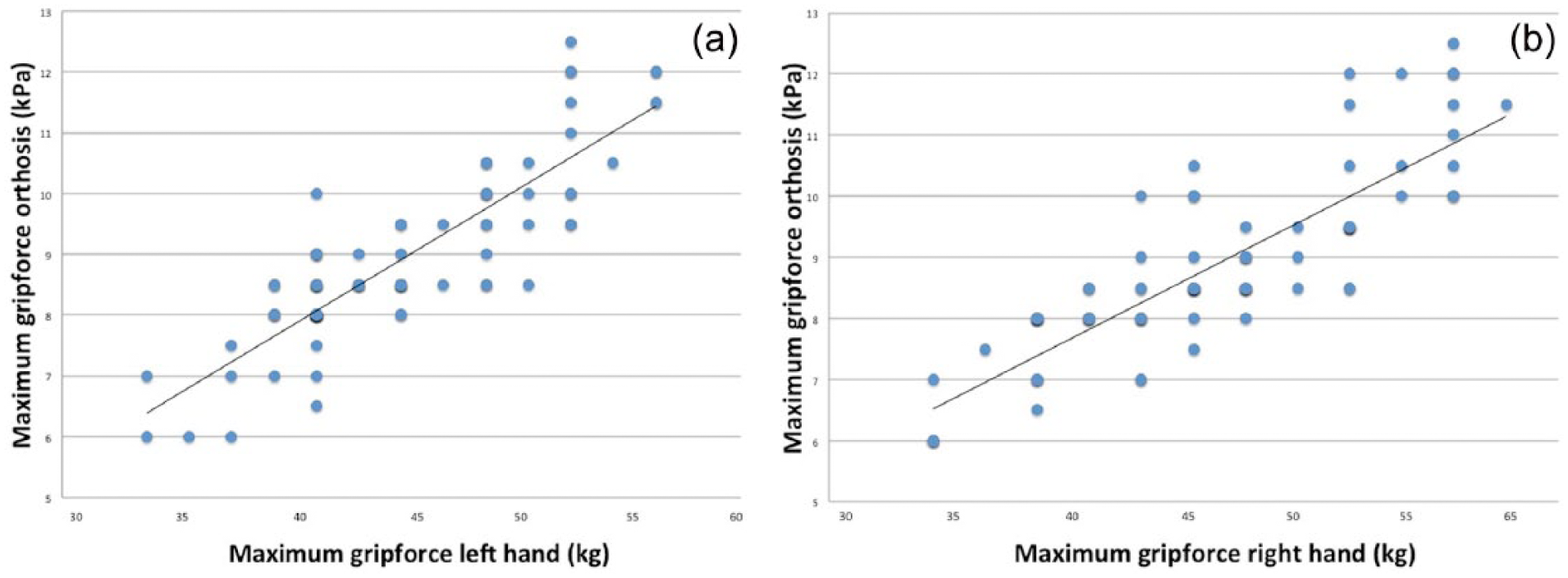
Positive correlation between grip force measured in a neutral position free-handed (a) left and (b) right compared to the concomitant position in an orthosis.
Discussion
The first part of the study showed a logistic regression between the maximum grip force and wrist position in a post-operative orthosis. The peak values of maximum grip force were observed with a wrist positioned in extension, progressively decreasing with an increasing flexion angle. This is a known phenomenon reported in previous studies and is attributed to an increased length of the flexor muscle sarcomeres, thereby causing an increased contraction force.8,10,15–17
This study attributes a logistic function which allowed to derive the wrist position necessary to achieve a desired amount of grip force reduction with an MGR50 occurring at 23.2° of wrist flexion. Two factors could be influencing the obtained results: muscle tiredness and contribution of the intrinsic muscles.
However, the subjects were given 1-min resting time, which is considered enough time to restore phosphocreatine levels and not to reduce maximum grip force in consecutive measurements.18,19 In addition, other studies measuring grip strength in different orders of wrist position or with a limited amount of measurements reported similar findings.9,16
The intrinsic muscles have shown to contribute for almost 50% to the maximum grip force in some studies. 20 Theoretically, the intrinsic muscles are neutralized by positioning the metacarpals in 90° of flexion. 12 However, past research highlighted the influence of wrist position on the intrinsic both in flexion and extension with only the adductor pollicis being independent from wrist position. 21
This study only investigated the cumulative result on the maximum grip force and therefore could not rule out a possible influence of the intrinsic muscles on the observed grip force reduction. Further research is needed to investigate their role/contribution during various wrist positions in post-operative orthosis to obtain the isolated force generated on the flexor tendons.
Another limitation from this study can be attributed to the absence of measuring the force transferred on each finger separately. Finger force distribution has been shown in previous studies to be relatively constant regardless of hand size, hand dominance, force magnitude, and wrist position.9,22
In contrast to these findings, Li 8 found that force sharing with each different finger flexor was significantly affected by wrist position, attributing this to a different moment arm expressed with regard to the axis of movement. 23 This could be of clinical importance due to a changing location of flexor tendon injuries presented by each individual patient. Altering the wrist position according to the affected finger could therefore reduce the load transferred on the repaired flexor tendon injury.
The second part of the study showed a positive correlation between the maximum grip force measured in an orthosis and subsequently free-handed for the same wrist positions. These findings are in accordance to a positive correlation found between the maximum grip strength of the dominant and non-dominant hand. 24 A limitation could be attributed to the use of only the neutral wrist position for correlation with the maximum grip force values measured in a post-operative orthosis.
Difficulties in obtaining reproducible measurements were encountered, because the maximal grip force could not be accurately measured without creating some movement in wrist position. However, a neutral position is used as a standard approach to obtain maximal grip force by the ASHT. 14
Conclusion
This study showed how a different wrist position alters the maximum grip force expressed in a post-operative orthosis according to a logistic equation, correlating positively with the contralateral (free)hand. Involuntary contractions (e.g. during sleep) can generate this maximum grip force post-operatively in an orthosis and increase the risk for rupture at the repair site. 25 Reducing the maximum grip force in a clinical setting could be of use because the generated grip force will determine the force transmitted on the finger flexors and hence on the sutured tendon. 8
Further clinical studies are needed to point out whether a patient with a high maximum grip force measured in the non-injured hand could benefit from an increased flexion angle in reducing rupture rate. Further experimental studies can be aimed at incorporating various wrist positions in a post-operative orthosis and analyzing the force reduction achieved on the flexor tendons of each finger separately. By this, the most appropriate position for a patient in a post-operative orthosis can be determined depending on the injured flexor tendon.
Footnotes
Acknowledgements
This manuscript contains original research. Preliminary results were shown on the 22th International Hand Symposium, Genval/Brussels, Belgium, as listed below: Burssens A, Schelpe N, Vanhaecke J, Dezillie M and Stockmans F. Effects of wrist position on maximum flexion force during mobilization in a Kleinert orthosis. In: 22th international hand symposium, Genval/Brussels, Belgium, 2014 (Burssens A—Oral Presentation).
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.