
Abstract
Background: Optoelectronic motion capture may provide a platform for the development of objective biomechanical outcome measures applicable to the young, active individual with lower limb loss. In order to create valid and robust tools, the modelling strategy applied must adequately represent both natural and prosthetic segments and joints.
Objectives: To explore existing usage of optoelectronic motion capture and modelling strategies for the analysis of amputee function.
Study design: Literature review.
Methods: Systematic search of Medline (OVID) and keyword search of the Journal of Prosthetics and Orthotics.
Results: Over 60% (n = 32) of the 51 studies extracted adopted a conventional three degree-of-freedom modelling approach. Linear segment representation (15%) and six degree-of-freedom techniques (19%) were employed in the remaining papers. Prosthetic modelling strategies were poorly reported. Landmarks were estimated from corresponding positions on the contralateral intact limb, mechanical joint centres and regression equations. No model defined the residuum and socket independently.
Conclusions: In the absence of a definitive solution, it is essential that the limitations of any model are understood in the development and establishment of reliable outcome measures for this population using motion capture technology. Poor reporting and a lack of consistency make comparison of results between studies and institutions impractical.
Standard modelling techniques may not consistently represent the body and prosthesis adequately to produce valid results for the analysis of function of persons with lower limb loss. Variation in modelling techniques limits the utility of findings reported in the literature. Development and application of a uniform, robust modelling strategy would benefit research and clinical practice.
Keywords
Introduction
Following lower limb amputation, regaining function with the aid of a prosthesis involves substantial motor learning in light of the loss of natural joints, musculature and proprioceptive feedback, 1 which are fundamental in the movement and stabilization of the body.
For all persons with limb loss, continual evaluation during rehabilitation is critical in developing and consolidating efficient movement patterns, avoiding detrimental compensatory motions and optimizing the alignment and configuration of the prosthetic limb.
Standard measures of amputee function include gait velocity and analysis of temporal and spatial stride parameters, 2 – 5 functional assessments such as the timed walk test 6 and the timed up-and-go (TUG) test, 7 and subjective approaches such as questionnaires and functional rating scales. 8 These are simple to perform and require little specialized equipment; however, they have largely been designed to assess basic functional capabilities, quality of life and health status. 9 As such, they can measure only limited aspects of mobility 8 and thus may have insufficient sensitivity at higher levels of function. 10
Recent statistics show that the national average age of referrals to UK civilian prosthetics centres is 65 years for males and 69 years for females, 11 with over 70% of amputations of dysvascular aetiology. In contrast, with 84% of UK regular forces below the age of 40, 12 the military amputee population is significantly younger, and limb loss is predominantly a result of trauma sustained on military operations.
For a young, previously active patient without cardiovascular compromise, the potential demands of prosthetic use are greater, with many individuals expecting to perform at a high level in employment and sport. 13 Consequently, greater versatility is required of outcome measures used to evaluate this group, where the context of application may range from early gait re-education to movement refinement and performance optimization.
Applied as a basis for gait and functional movement assessment, biomechanical analysis can provide a means to understand adaptations that have occurred with respect to the integration of the prosthesis into the dynamic system of the individual. 14 It can also offer additional information about functional status and prosthetic performance, 10,13,15 inform appropriate patient management 16 and establish the efficacy of a rehabilitation programme. 17
Marker-based motion capture is a tool commonly used to track and describe the movement (kinematics) of the body in three dimensions. The output additionally forms a key component in more complex analyses that combine motion, force and muscle activity data to gain further insight into interactions, motor strategies and energy transfer mechanisms.
Optoelectronic motion capture systems enable the acquisition of kinematic data in three dimensions via the detection of a configuration of skin-mounted markers positioned at bony landmarks and/or segment midsections by a system of cameras.
Two-dimensional (2D) marker coordinates from each camera are amalgamated in order to establish a set of position coordinates for each marker in the three-dimensional (3D) measurement volume. This is performed for each frame of captured data during activity. Central to the use of this technique for human functional measurement is the employment of a biomechanical model that simplifies the complex anatomy of the individual under investigation.
Conventionally, each segment of the body, for example the thigh and shank, is assumed to be a rigid body. 18 The model dictates the placement of the markers and relates their position to the geometry of the underlying segment. With reference to this model, the coordinate data of each detected marker may be translated into meaningful information about the position and movement of the body upon which the marker or markers are placed. The extent to which useful information may be extracted thus depends on the extent to which the system is adequately represented by the markers.
Modelling strategies
Modelling strategies vary in complexity and affect the number of degrees of freedom (DOF) that may be reported between anatomical segments, e.g. foot, thigh, trunk. In simplest form, the motion of a single marker may be used to describe the displacement of an anatomical landmark or segment relative to which it has been applied. The application of two or more markers on each segment enables the angular motion of a segment to be described. Linear segment representation, as employed in the link model described by Winter,
19
requires landmarks at single proximal and distal segment endpoints (Figure 1a). The line between these points, commonly defined via the 2D or 3D coordinates of laterally attached markers, is used to represent the segment. Relative segmental motion may be defined locally in 1DOF by the minimum inclusive angle between the two lines in 3D space, or globally with respect to the plane of progression or laboratory coordinate system.
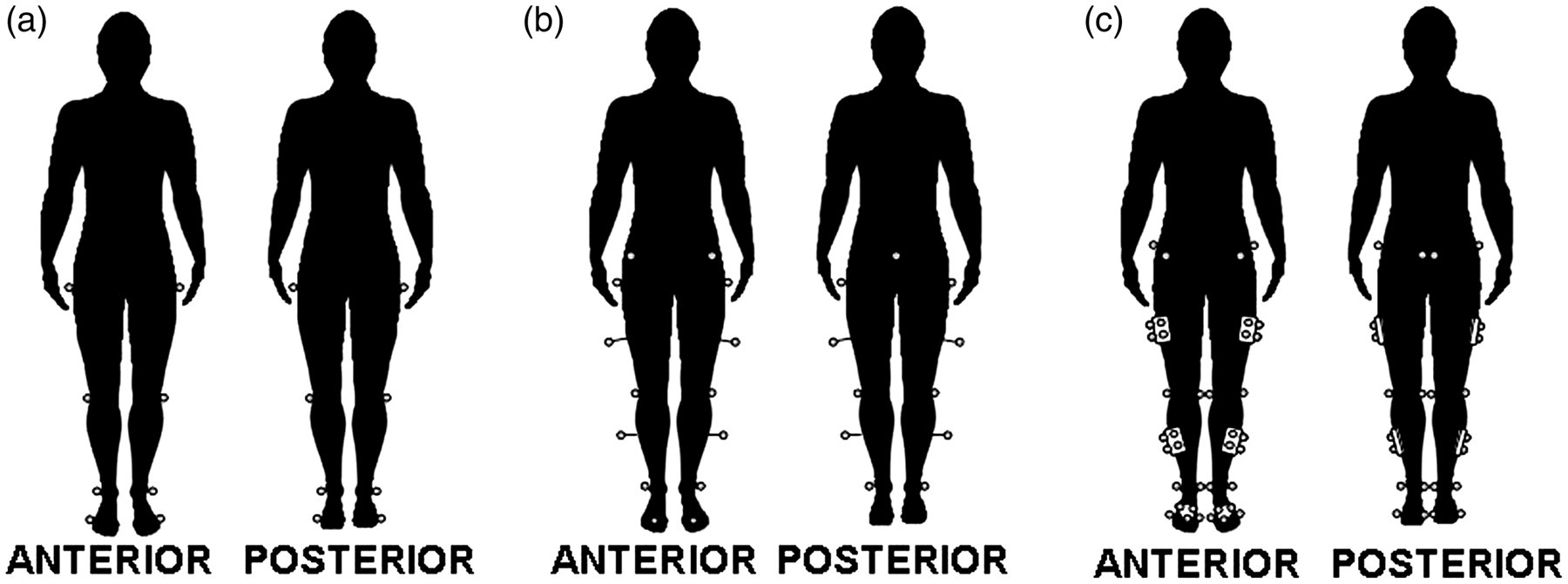
Early published works by Kadaba et al. 18 and Davis et al., 20 describing protocols developed at Helen Hayes and Newington hospitals, respectively, are the foundation of many models used in gait and movement analysis. 21 Three markers are employed in the definition of the shank, thigh and pelvic segments. Attached laterally on the segment at the tip of a wand, the third marker enables a plane to be defined from which 3D segment-embedded local coordinate systems are built 18,20 (Figure1b). Knee and ankle joint centres are estimated from laterally placed markers and anthropometric measurements. The hip joint centres are estimated via regression equations based on pelvic geometry as a function of leg length. With the exception of the foot, which is tracked by only two markers, the 3D modelling of each segment enables sagittal, coronal and transverse joint rotations, i.e. motion in 3DOF, to be described. This modelling approach, commonly referred to as ‘historical’ or ‘conventional’, forms the basis for protocols within the dedicated clinical software packages provided with a number of motion capture systems, 22 e.g. Vicon Plug-In Gait (Vicon Motion Systems, Oxford), and the Codamotion Gait Package (Codamotion, Charnwood Dynamics Ltd, Leicestershire).
Using 6DOF modelling enables the description of three rotational components and three translational components of motion between two segments. This requires segmental independency that may be achieved when there are at least three real markers unique to each segment. 23,24 Examples include the Cleveland Clinic set within the Orthotrak software supplied with Motion Analysis systems (Motion Analysis Corporation, California) and the calibrated anatomical systems technique (CAST) described by Cappozzo et al. 23 In both of these methods the motion of each segment is tracked by an independent group of three or more markers in close proximity (‘triad’ or ‘cluster’) applied at the segment midsection, unconstrained to the adjacent segments. Within a static trial an ‘anatomical’ configuration based on real markers and/or landmark digitization is used to define the geometry of each segment and the position of the marker group relative to the segment (Figure 1c). In the subsequent movement trials any anatomical markers, including those that may hinder movement such as those placed medially at the knee and ankle, may be removed. 22
Limitations of the various modelling strategies are widely acknowledged. Soft tissue artefact arising from uncontrolled skin and subcutaneous tissue movement, 22,25 – 28 and marker placement imprecision, 29– 31 for example, are commonly cited sources of error in all marker-based protocols.
Repeatability has been investigated by several authors; 22,23,30,32 – 36 however, aside from marker placement discrepancies between sessions, variability in data may also be attributed to natural variation in both non-pathological and pathological movement. 22,31,37 – 39 Validity is more difficult to establish in the absence of a suitable gold standard measure. 35
Hybrid protocols based on conventional and 6DOF strategies have evolved with the aim of improving validity or optimizing the method for a specific assessment environment or patient population. For example, more complex foot models have been developed and evaluated. 40 This increased focus on the foot may be attributed to the extensive use of motion capture for the analysis of children with cerebral palsy, for which foot function is frequently of clinical importance. Functional methods of estimating joint centres of rotation during movement trials have been explored and implemented as an alternative to anthropometrics and reliance on regression-based joint centre estimations inestablishing local segment and joint coordinate systems. 29,38,41,42
In describing the kinematics of a person with limb loss where motion at, and distal to, the level of amputation is under investigation, the model configurationadopted must also take the prosthetic limb into account.
Scope
This review was conducted to investigate the use of motion capture, biomechanical models and marker sets for the motion of individuals with lower limb loss as described in the existing literature, with the aim of establishing an appropriate model and marker configuration for this patient cohort. Such a model is required as a foundation for the development of robust, objective biomechanical outcome measures for rehabilitation and performance optimization for this group.
Methods
A search of the MEDLINE (OVID) database was conducted on 15 April 2010 to obtain papers published after 1950 that describe the use of a marker-based approach for analysis of lower limb amputee kinematics. The search strategy used is defined in Figure 2. The Journal of Prosthetics and Orthotics (unlisted by Medline) was searched separately with the keywords ‘kinematic’, ‘kinematics’, ‘kinetic’, ‘kinetics’ and ‘biomechanics’, and the results added to the primary search prior to filtering and study selection.
Search strategy and study selection.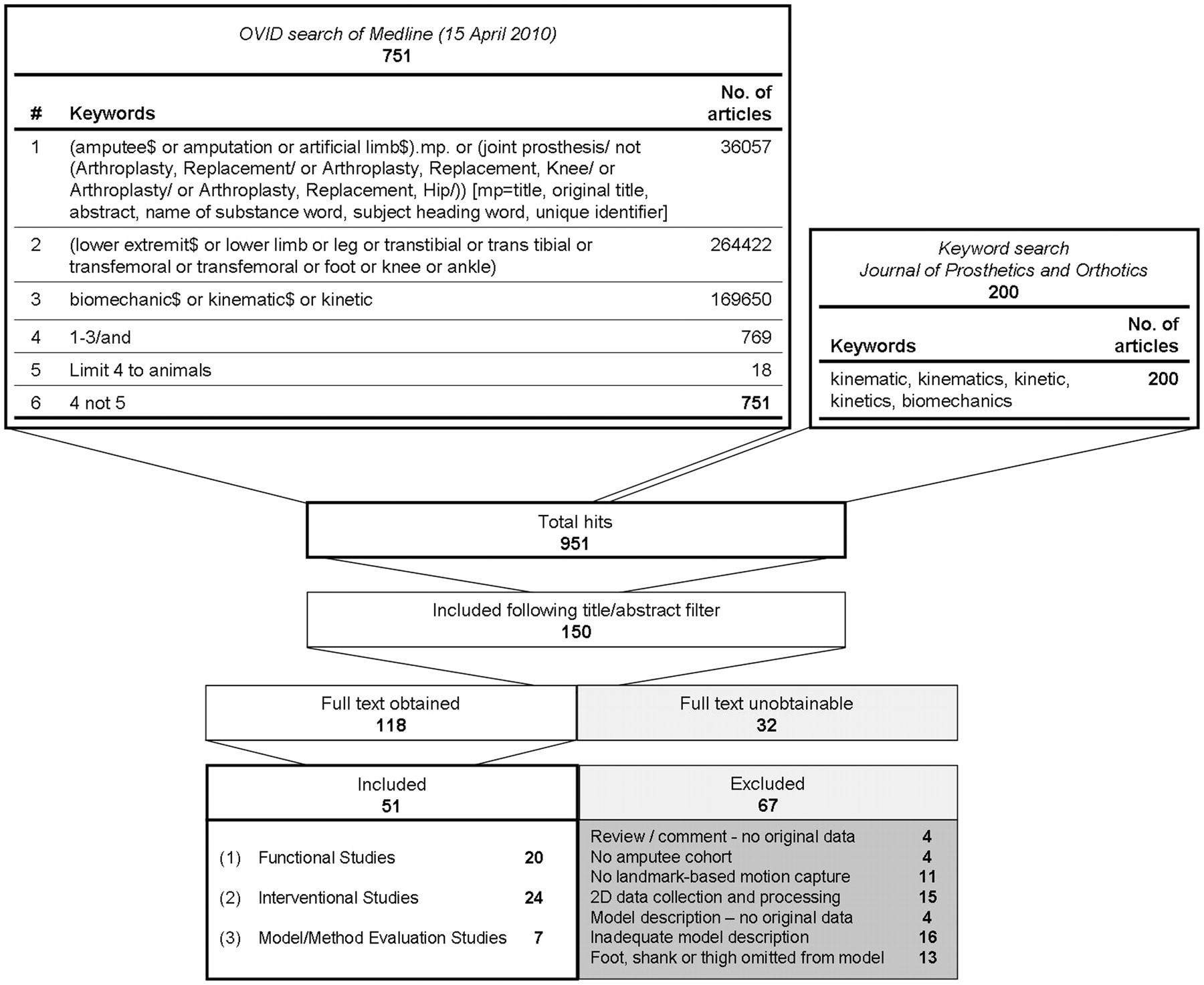
Study selection
Papers were selected for inclusion based on the following criteria:
Use of 3D motion capture using a marker or landmark-based model; Digitized or marker-derived landmarks; Analysis of at least one subject with single or multiple amputations, including at least one lower limb amputation at any level from foot to hip disarticulation; Application or evaluation of a biomechanical model for full lower limb analysis, including segmental definition of foot, shank and thigh; English language.
Dual-planar video analyses were accepted if direct linear transform conversion was applied to obtain 3D coordinates of digitized landmarks.
Papers were excluded if detail regarding the marker set and model presented in the described method or obtainable cited references were insufficient to establish the landmark location and segment definition strategy of the model. Literature reviews were excluded. Where application of a named or referenced model was applied in the study method, full implementation of the model protocol was assumed, including marker placement, segment definition and calibration, unless explicitly stated otherwise. Studies were separated into three groups by focus:
Functional: observation and description of function of amputee cohorts performing a specified task or activity; Intervention: investigation of the effect of an intervention on amputee function; Model/method evaluation: utilization of kinematic data from an amputee subject or cohort to evaluate a method or modelling technique or for simulation purposes.
Results
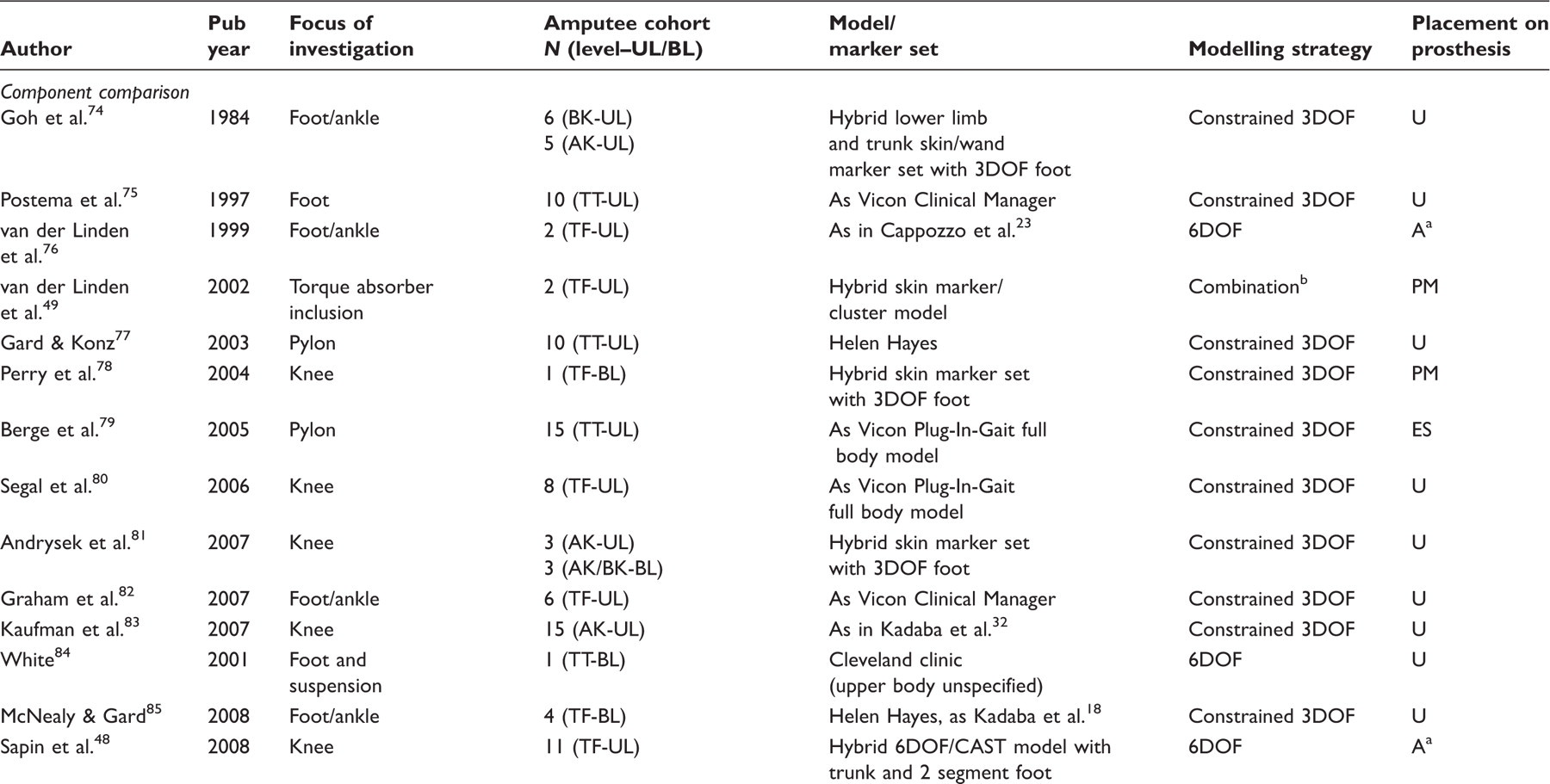
Functional studies: analyses of data collected from a defined amputee population performing a specific motion, task or activity.
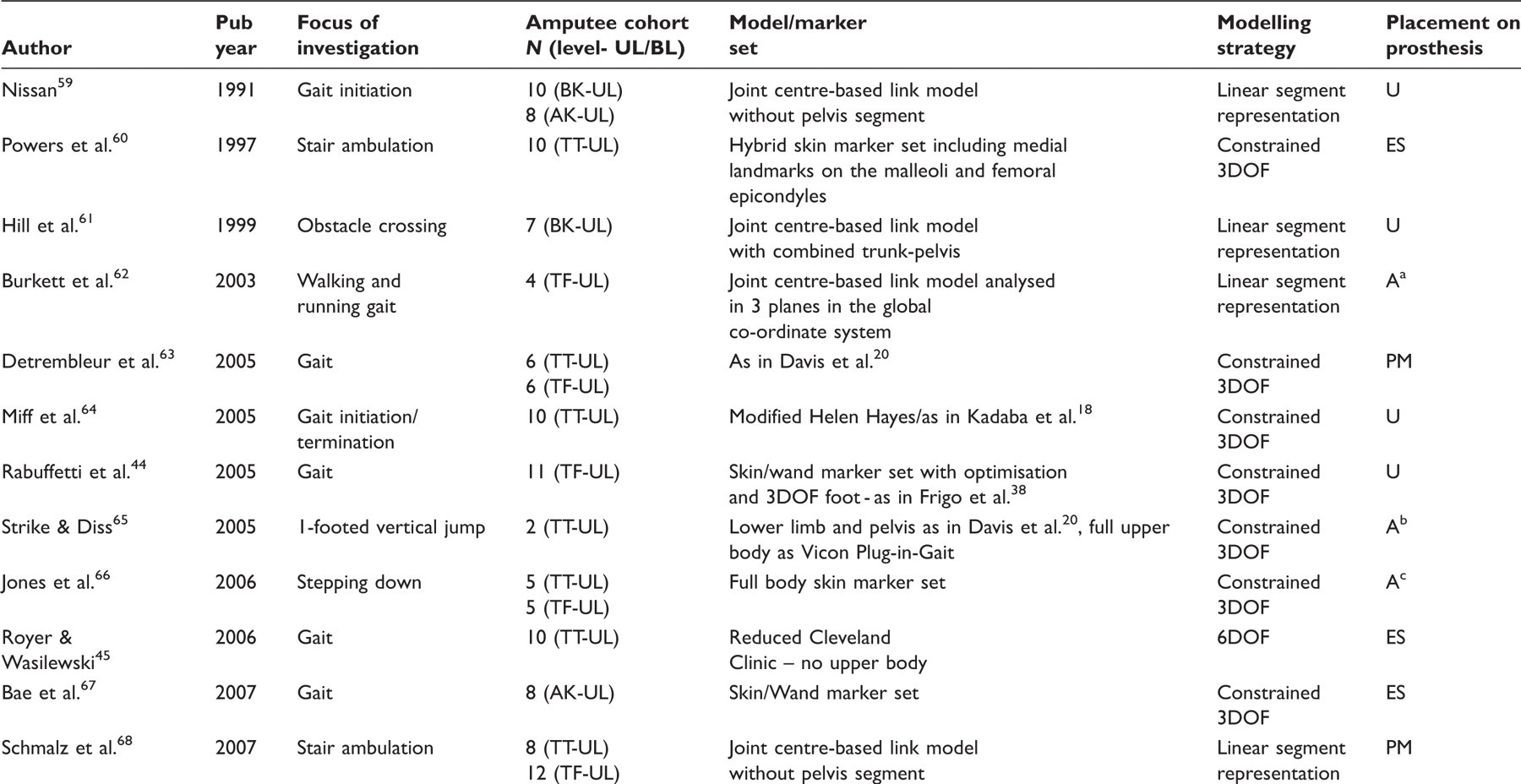
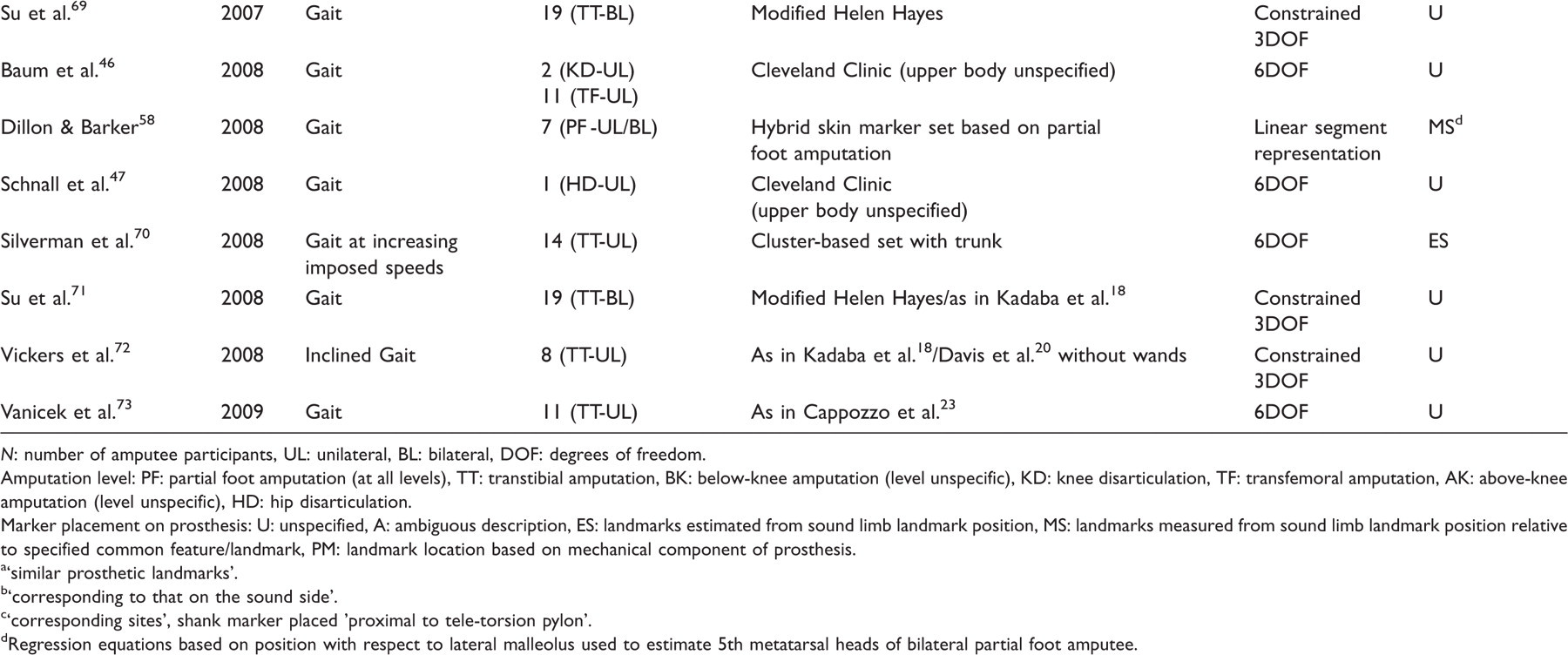
N: number of amputee participants, UL: unilateral, BL: bilateral, DOF: degrees of freedom.
Amputation level: PF: partial foot amputation (at all levels), TT: transtibial amputation, BK: below-knee amputation (level unspecific), KD: knee disarticulation, TF: transfemoral amputation, AK: above-knee amputation (level unspecific), HD: hip disarticulation.
Marker placement on prosthesis: U: unspecified, A: ambiguous description, ES: landmarks estimated from sound limb landmark position, MS: landmarks measured from sound limb landmark position relative to specified common feature/landmark, PM: landmark location based on mechanical component of prosthesis.
‘similar prosthetic landmarks’.
‘corresponding to that on the sound side’.
‘corresponding sites', shank marker placed 'proximal to tele-torsion pylon’.
Regression equations based on position with respect to lateral malleolus used to estimate 5th metatarsal heads of bilateral partial foot amputee.
Interventional studies: analyses of more than one prosthetic component or configuration, or rehabilitation method with respect to effects on amputee function.
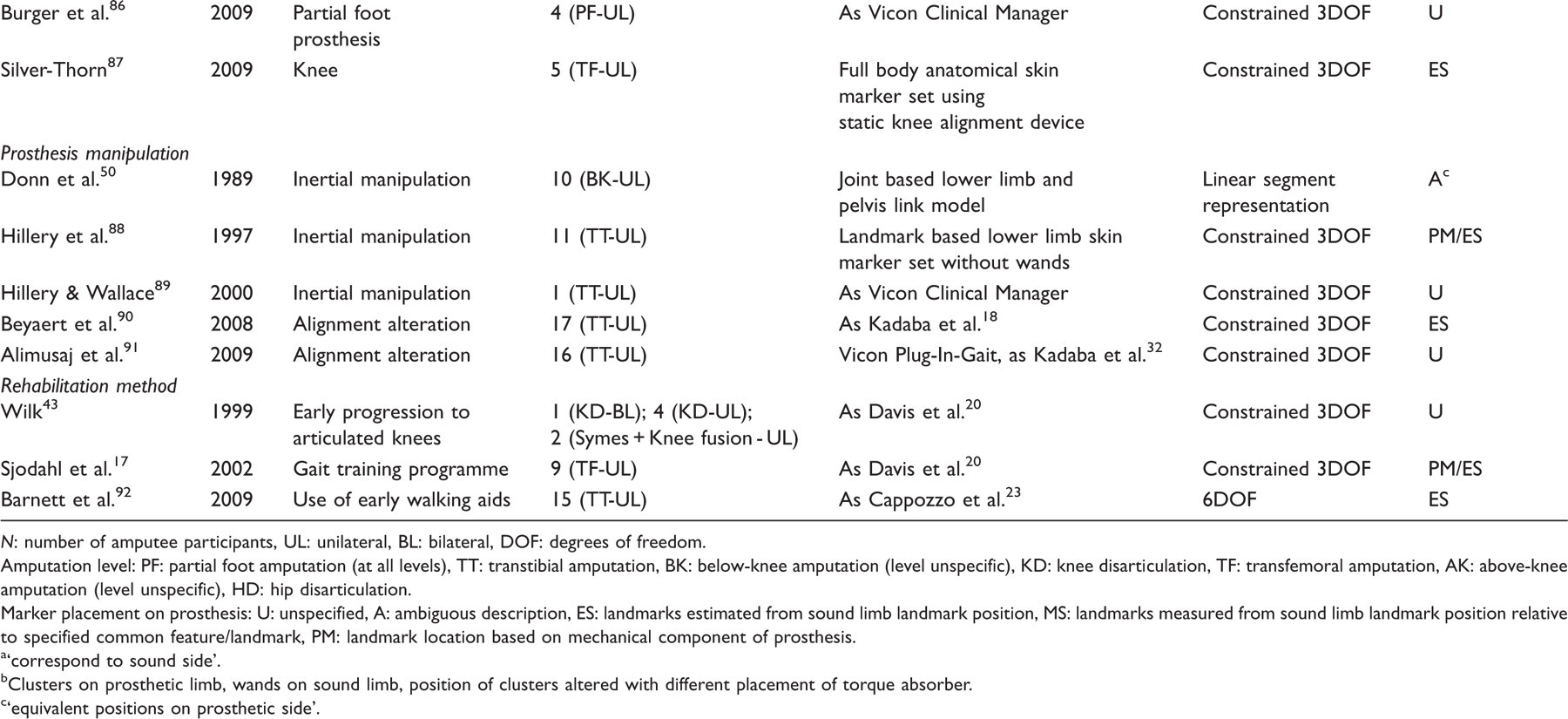
N: number of amputee participants, UL: unilateral, BL: bilateral, DOF: degrees of freedom.
Amputation level: PF: partial foot amputation (at all levels), TT: transtibial amputation, BK: below-knee amputation (level unspecific), KD: knee disarticulation, TF: transfemoral amputation, AK: above-knee amputation (level unspecific), HD: hip disarticulation.
Marker placement on prosthesis: U: unspecified, A: ambiguous description, ES: landmarks estimated from sound limb landmark position, MS: landmarks measured from sound limb landmark position relative to specified common feature/landmark, PM: landmark location based on mechanical component of prosthesis.
‘correspond to sound side’.
Clusters on prosthetic limb, wands on sound limb, position of clusters altered with different placement of torque absorber.
‘equivalent positions on prosthetic side’.
Model/method evaluation studies - evaluations of models and outcome measures for amputee/prosthesis functional analysis.
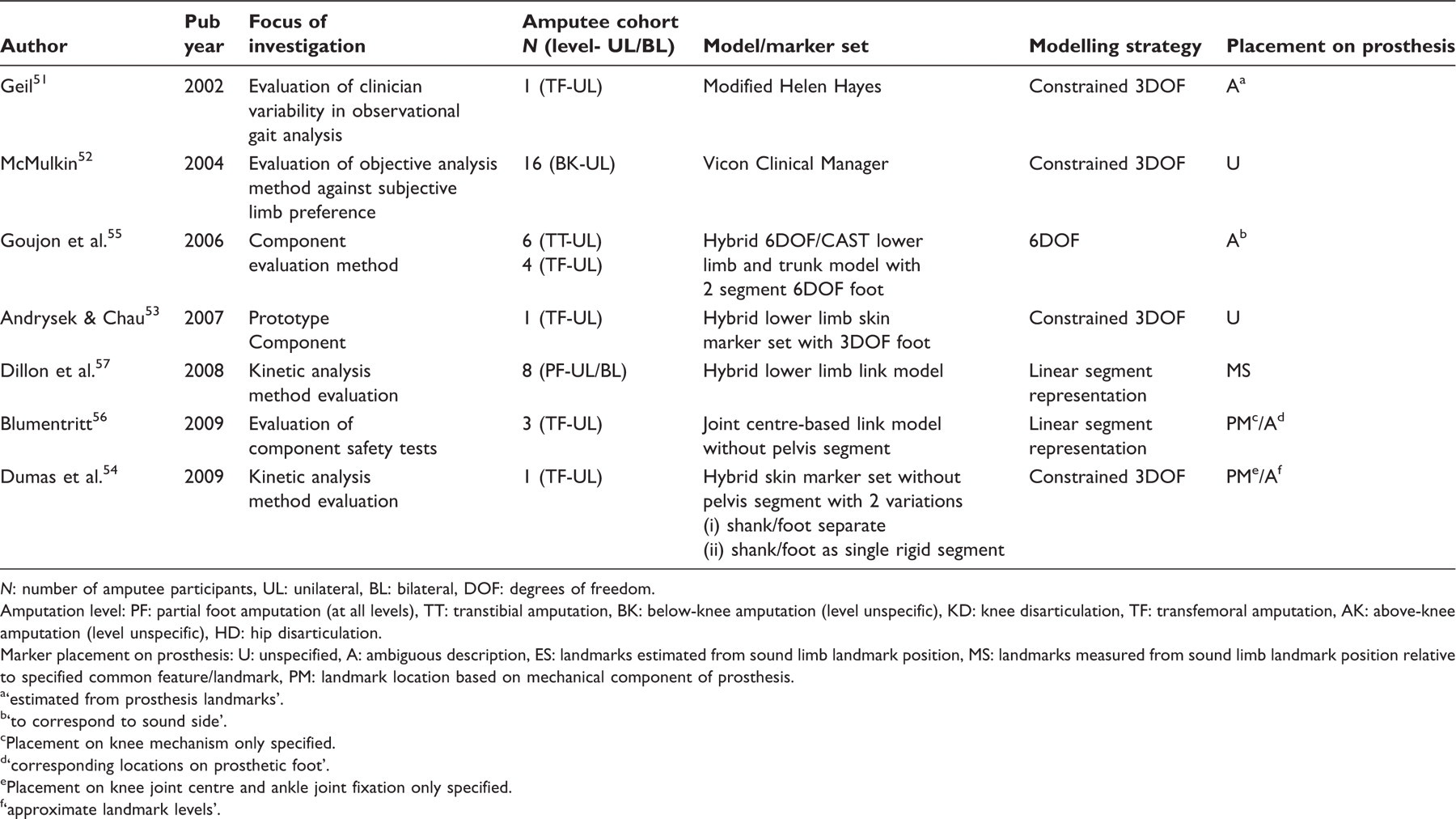
N: number of amputee participants, UL: unilateral, BL: bilateral, DOF: degrees of freedom.
Amputation level: PF: partial foot amputation (at all levels), TT: transtibial amputation, BK: below-knee amputation (level unspecific), KD: knee disarticulation, TF: transfemoral amputation, AK: above-knee amputation (level unspecific), HD: hip disarticulation.
Marker placement on prosthesis: U: unspecified, A: ambiguous description, ES: landmarks estimated from sound limb landmark position, MS: landmarks measured from sound limb landmark position relative to specified common feature/landmark, PM: landmark location based on mechanical component of prosthesis.
‘estimated from prosthesis landmarks’.
‘to correspond to sound side’.
Placement on knee mechanism only specified.
‘corresponding locations on prosthetic foot’.
Placement on knee joint centre and ankle joint fixation only specified.
‘approximate landmark levels’.
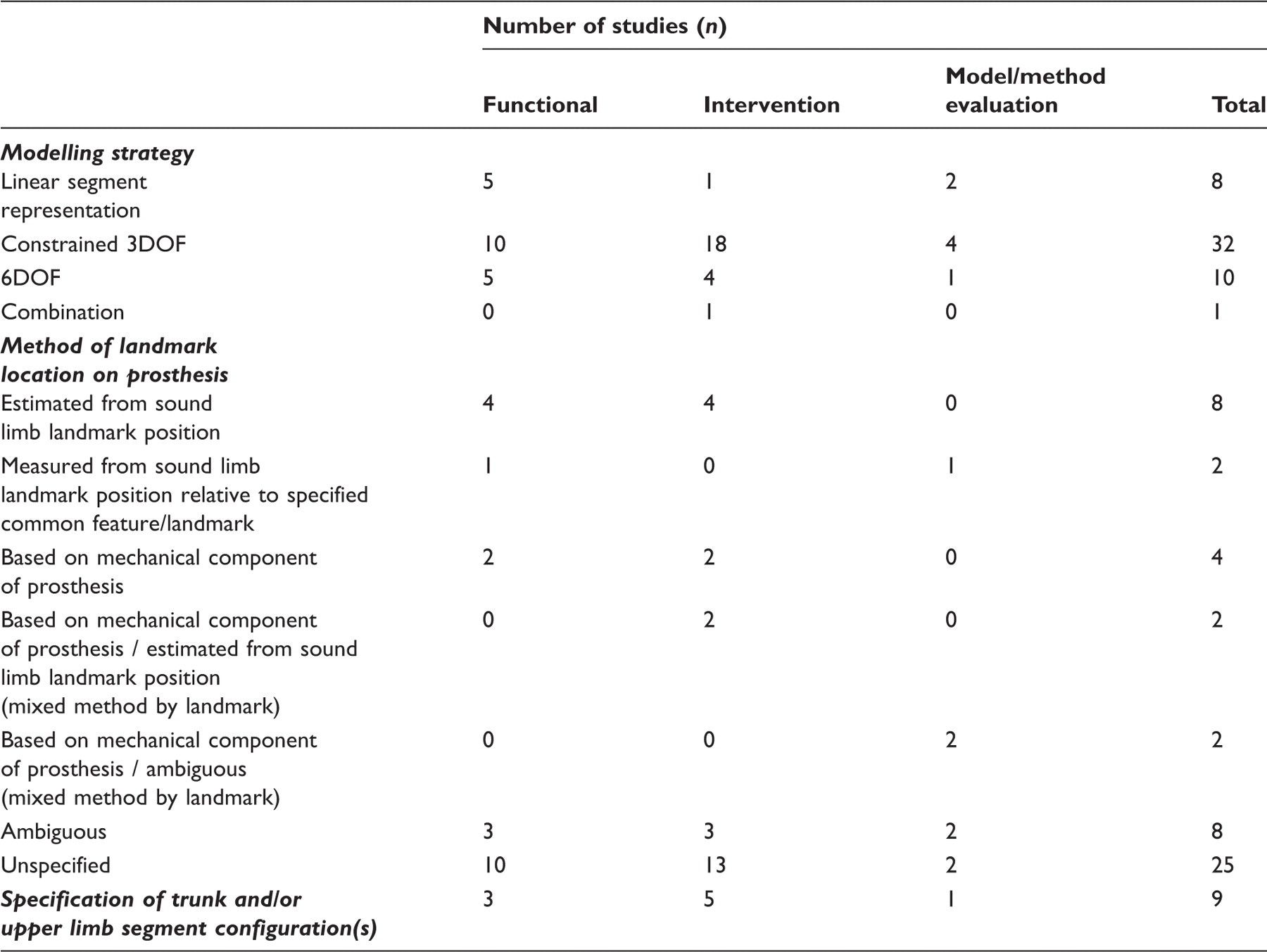
Modelling strategies of included studies.
Functional studies
The 20 studies in the functional group explored a range of activities within the laboratory environment (Table1), the most common of which was walking at a self-selected speed.
Half of the studies (n = 10) utilized derivatives of the ‘conventional’ approach. One of these adopted an ‘optimization’ model as described by Frigo et al. 38 with a 3DOF single segment foot model and optimization of the hip and knee joint centre definitions by a functional approach. 44 Another 25% of the studies (n = 5) implemented a 6DOF approach, three of which used the Cleveland Clinic model. 45 – 47 The remaining 25% (n = 5) utilized a joint centre-based linear modelling approach.
Intervention studies
The 24 intervention studies were further grouped by intervention type (Table 2). Sixteen studies investigated the effect of a specific prosthetic component on amputee function. Five studies investigated the effect of different prosthetic adjustments, namely rotational alignment manipulation (n = 2) and inertial manipulation (n = 3), and three studies evaluated the efficacy of rehabilitation methods.
A derivative of the conventional approach was used in 75% of intervention studies (n = 18). Four studies employed 6DOF modelling, one of which included a two-segment foot model. 48 One study mounted clusters on the prosthetic limb and a conventional anatomical configuration on the sound limb. 49 Donn et al. employed a linear model. 50
Model/method evaluation studies
Four of the seven studies that fell within the model/method evaluation category (Table 3) employed a 3DOF approach. Geil evaluated the variability of observational gait analysis amongst clinicians 51 while McMulkin et al. investigated the agreement of instrumented performance analysis and subjective preference for prosthetic components. 52 Andrysek & Chau evaluated the energy transfer mechanisms of a swing phase controlled knee joint using a hybrid version of the conventional approach with a 3DOF foot. 53 Dumas et al. compared the results of inverse dynamic calculations of loads at the knee joint with direct measurements via a transducer incorporated into the prosthetic structure. 54 Calculations were based on a hybrid 3DOF model with the foot and shank modelled both separately and as a single rigid structure.
Goujon et al. investigated potential kinematic and kinetic parameters to be used for the evaluation of prosthetic feet using a 6DOF model with a two-segment foot, as utilized in a later study from the same group also included in this review (intervention studies group – Sapin et al. 48 ). 55 Blumentritt et al. used a joint centre-based linear model to analyse a series of devised tests designed to evaluate the safety of prosthetic knee joints. 56 Dillon et al. 56 investigated the effect of employing a standard link model 19 for calculating inverse dynamics in partial foot amputees, and evaluated an adaptation to the model designed to account for the loss of a portion of the extremity, 57 as utilized in a study that falls within the functional studies group of this review. 58
Discussion
Successful biomechanical modelling requires the anatomy of the individual to be adequately described geometrically, and with sufficient degrees of freedom to capture motion of interest in all relevant planes, with respect to the activity under investigation. Fundamental to the utilization of marker-based models are assumptions that anatomical segments are rigid and that there is negligible movement between the markers and the underlying skeleton. 23 The ability to extract meaningful data depends on the extent to which the requirements are met and these assumptions hold, and this may vary for an individual or population cohort. 31 In the context of clinical prosthetics, the introduction of an artificial limb poses new challenges in segment definition and tracking as well as in the reporting of meaningful kinematic information.
A standard model developed based on an intact human musculoskeletal system may be appropriately applied should it adequately represent the combined biological-prosthetic system, given the parameters under investigation. However, differences in the positioning of relevant functional landmarks, differences in joint behaviour, non-anatomical movement of prosthetic components and the introduction of an additional segmental interface between the socket and residual limb, amongst other factors, may increase the scope for misrepresentation and subsequent misinterpretation of data. This is undesirable for outcome measure data that are to be used as the basis for a clinical judgement, and also limits the applicability of the method in the assessment of prosthetic component function, 93 particularly when the data are combined with kinetic measurements in order to calculate joint forces, moments and powers, and energy mechanisms.
The results of this search indicate that there is currently no established model for the analysis of lower limb amputees. There was no obvious correlation between the focus of the existing literature and the choice of model. Over 60% (n = 32) of the 51 studies adopted a conventional 3DOF approach, either with direct application of the models described by Kadaba et al. 18 (Helen Hayes model) or Davis et al. 20 (Newington model), or in a derivative or hybrid form. This approach is limited by the sharing of common landmarks in the definition of adjacent segments, which promotes error propagation between segments and constrains the reported movement to three degrees of rotational motion about a single point, with implications for the adequacy of system representation and accuracy. 21,93
In many institutions, preference for the conventional approach may be due to the appeal of few markers, ease and speed of implementation, availability of established and well-published protocols, and support within dedicated clinical gait packages that are supplied with several motion capture systems. Within established laboratories, a change of capture protocol would demand the compilation of new normative and group datasets in light of the redundancy of the data collected with the previous configuration, which could no longer be assumed to provide a suitable comparative control in an assessment scenario. 35
Landmark location and definition
Treatment of the prosthesis within the biomechanical models employed is poorly reported in the literature. In approximately 50% (n = 25) of the 51 study protocols retrieved in this review, including 10 of the 16 studies evaluating prosthetic components, the placement of markers or location of landmarks on the prosthetic side was unspecified. It is possible that this aspect was not considered or that the detail was omitted in favour of text regarded as more relevant to the main focus of the study.
Of the studies that provided a description of the treatment of the prosthetic limb in the model, position was most frequently described ambiguously (n = 8) or estimated from corresponding positions on the contralateral intact limb (n = 8). This estimation method has the advantage of simplicity; however, such placement may be misleading or irrelevant considering the structure and function of the prosthetic component. In the modelling of a solid ankle cushioned heel (SACH) foot, for example, a marker placed at the cosmetic lateral malleolus is essentially redundant beyond the description of the geometry of the component in the zero condition, as there is no articulation at this point. Selection of an appropriate location may also be confounded by cosmetic coverings that obscure the position of relevant landmarks.
Placement of markers based on the geometry or functional mechanisms of the prosthetic component may lead to a more representative description of the system, although this may be complicated by components that produce non-anatomical movement, such as running blades. 94 However, only eight studies adopted this approach for any landmark within the model.
Joint origin and axis definition
Differences in limb geometry or functional prosthetic joint behaviour as well as alterations in limb alignment, such as anterior or posterior translation of the foot with respect to the shank pylon, inherently affect the joint definition within the model. 95 This complicates analysis when examining different components and the effects of adjustments to limb alignment.
Arguably, 6DOF methods are more appropriate for describing the motion of non-uniaxial prosthetic joints such as polycentric knees, as they do not impose a single centre of rotation between segments. However, where a component violates the rigid body assumption, for example a foot with a deformable keel, an alternative modelling approach may be required, 58,94 particularly where this aspect of the design is responsible for joint functionality. In assuming segmental rigidity and a single axis of rotation at the ankle, significant error has been demonstrated in the calculation of joint moments and energy storage and transfer mechanisms, for example in assessment of foot and ankle components. 96,97
Residuum–socket interface
Any relative movement at the interface between socket and limb will also counter the rigid body assumption of a standard model and affect results. 17 Where this relative movement may vary in severity between two cohorts under comparison, for example primary and established amputees, or where the socket fit itself is under investigation, it may be more appropriate to model the residual limb and socket as two segments. Only two studies acknowledged the residuum and socket as independent segments. 57,58 These publications were from the same institution and investigated only partial foot amputation. In both studies, the anthropometric models required for inverse dynamics were adapted to account for the prosthesis; however, both residuum and prosthesis were modelled as a single rigid foot segment within the kinematic link model.
Trunk and upper limb movement
Profound compensatory movement strategies may be developed following the loss of a limb, and therefore significant functional variables may be overlooked by neglecting trunk and upper body movements in biomechanical analyses. 98 The present review included only nine studies that specified inclusion of configurations for any independent segments above pelvic level in addition to the lower limb (Table 4).
Ensemble data
Factors including age, 99 aetiology of amputation, 14,99 experience ambulating with a prosthesis, 100 complications with the residual limb 101 and differences in prosthetic components 14,102 are all associated with functional ability post amputation, and may result in a high degree of inter-subject variability within an amputee cohort. Averaging such data with the aim ofproducing a representative mean for a sample may conceal important events, 76 reduce the magnitude of results 102 or create anomalies, and ultimately lead to the generation of profiles that do not reflect the movement of any subject. 69 The majority of observational studies extracted for this review evaluated single cases or small heterogeneous cohorts, with low control for confounding factors.
Given geometric, structural and functional differences between limbs, components and their natural counterparts, direct comparisons of individual or grouped motion data should always be conducted with care. Selection of appropriate parameters to compare requires an understanding of the deficiencies of the model, so that the accuracy of the representation of each separate human or prosthetic system or condition (e.g. alignment) under investigation can be judged. Differences between limb or component alignment, rigidity, rotational or translational axes, and the presence or lack of soft tissue artefact, for example, may affect the integrity of inter-limb comparisons. When the model favours either of the limbs in terms of applicability of imposed constraints and measurable degrees of freedom, or describes neither limb adequately for the movement under investigation, an alternative modelling strategy may be required.
The relevance of conducting comparative analyses of the motion of two systems that are by nature or design geometrically or functionally different, for example single axis and polycentric or natural knee joints, should also be questioned.
Conclusion
Optoelectronic motion capture may provide a means to objectively measure function across the wide range of abilities that may be demonstrated by a young, active population with lower limb loss. The extraction of representative and meaningful data relies upon (1) the selection of outcome variables that are functionally relevant to the individual or population under investigation, and (2) a model that is sufficiently representative of the system or systems to enable accurate computation of these variables. There is no definitive marker set in the literature that is appropriate for the analysis of this population in all contexts. Few centres have published work describing attempts to develop marker-based models specifically to incorporate prosthetic components. Further efforts are warranted to quantify potential error in applying standard models, as the literature is lacking in this area. In the absence of a definitive solution, it is essential that the limitations of any applied model and associated landmark configuration are understood, in order for appropriate, informed conclusions to be reliably drawn from the data. 31
Knowledge transfer across institutions requires explicit method description for validity to be established, and is facilitated by the use of common approaches to motion capture, modelling and analysis. The development of more robust modelling strategies for individuals with limb loss would be worthwhile, enabling standard motion analysis techniques to provide reliable data to monitor ability, enhance treatment and aid prosthesis optimization for the maximization of function and performance throughout the rehabilitation pathway and beyond.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors alone are responsible for the content and writing of the paper.