
Abstract
Background:
The Intrepid Dynamic Exoskeletal Orthosis is a custom-made dynamic response carbon fiber device. A heel wedge, which sits in the shoe, is an integral part of the orthosis-heel wedge-shoe system. Because the device restricts ankle movement, the system must compensate to simulate plantarflexion and allow smooth forward progression during gait.
Objectives:
To determine the influence of wedge height and durometer on the walking gait of individuals using the Intrepid Dynamic Exoskeletal Orthosis.
Study design:
Repeated measures.
Methods:
Twelve individuals walked over level ground with their Intrepid Dynamic Exoskeletal Orthosis and six different heel wedges of soft or firm durometer and 1, 2, or 3 cm height. Center of pressure velocity, joint moments, and roll-over shape were calculated for each wedge.
Results:
Height and durometer significantly affected time to peak center of pressure velocity, time to peak internal dorsiflexion and knee extension moments, time to ankle moment zero crossing, and roll-over shape center of curvature anterior-posterior position. Wedge height had a significant influence on peak center of pressure velocity, peak dorsiflexion moment, time to peak knee extension moment, and roll-over shape radius and vertical center of curvature.
Conclusion:
Changes in wedge height and durometer systematically affected foot loading. Participants preferred wedges which produced ankle moment zero crossing timing, peak internal knee extension moment timing, and roll-over shape center of curvature anterior-posterior position close to that of able-bodied individuals.
Clinical relevance
Adjusting the heel wedge is a simple, straightforward way to adjust the orthosis-heel wedge-shoe system. Changing wedge height and durometer significantly alters loading of the foot and has great potential to improve an individual’s gait.
Keywords
Background
Severe lower limb injuries can limit physical function and thereby affect many aspects of an individual’s life. Studies in service members 1 and civilians2–4 have shown that severe lower limb injuries may lead to depressive symptoms, pain interfering with daily activities, psychological distress, and low rates of returning to work. The Intrepid Dynamic Exoskeletal Orthosis (IDEO) was designed to restore function often lost after severe lower limb injury.
The IDEO is a custom-made dynamic response device which consists of a rigid carbon fiber supramalleolar footplate connected to a proximal cuff with carbon fiber struts (Figure 1). The struts deflect under load to store energy during midstance, which is released later in the gait cycle as the device is unloaded, similar to energy storage and return prosthetic feet. Studies have shown the IDEO to be effective in treating a wide variety of severe lower extremity injuries.5–7 In conjunction with a physical therapy training program tailored to IDEO users, the IDEO has improved functional outcomes such as self-selected walking velocity and timed stair ascent,6,8 reduced pain, 6 and allowed individuals to return to athletic activities. 9 Although the IDEO has documented benefits, it does not fully restore gait biomechanics.10–12
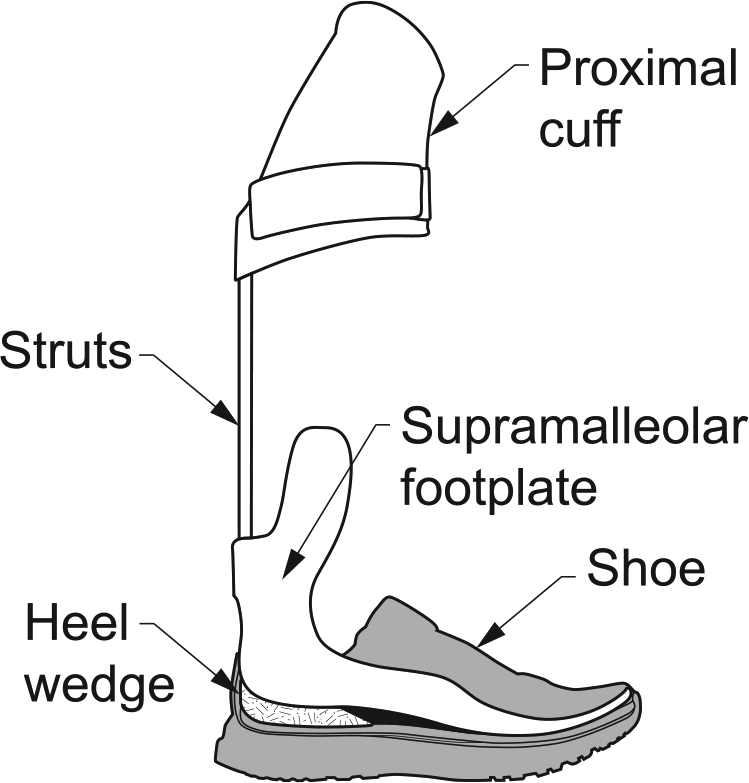
IDEO–heel wedge–shoe system. The heel wedge, shown in hash mark fill, sits in the shoe under the IDEO.
In able-bodied gait, the ankle rapidly plantarflexes during loading response, as the foot and ankle provide shock absorption, stability, and facilitate forward progression. 13 However, the design of the IDEO does not allow plantarflexion motion. Without a compressible heel wedge under the IDEO, it would function in a manner analogous to a ski boot in which the lower leg pivots about the heel resulting in an abrupt transition from the heel to forefoot. The heel wedge, while not physically part of the IDEO, is an integral part of the IDEO-heel wedge-shoe system (Figure 1). The wedge is made of urethane foam and is shaped to fit in the heel of the shoe. The height and durometer of the wedge are chosen based on patient weight and the plantarflexion angle which is built into the IDEO footplate. As a starting point, the clinician’s goal is a slightly inclined shank to vertical angle during standing. The choice of durometer is empirically determined based on patient weight, as one role of the heel wedge is shock absorption. After initial fitting, the heel wedge may be adjusted based on observational gait assessment and patient feedback. Wedge properties are thought to play an important role in allowing a smooth roll-over, although their effects on gait are not well understood.
Several approaches can be used to evaluate the effect of heel wedge properties on lower limb loading. The movement of the center of pressure (COP), the weighted average location of all ground reaction forces (GRF), can provide information on the position and timing of limb loading, and more specifically the rate at which force shifts from the proximal to distal foot. For example, COP progression has been used to demonstrate that a hydraulic prosthetic ankle allowed a smoother transition from heel to toe, 14 and COP displacement data have proved useful in comparing prosthetic feet with intact feet to better understand gait asymmetry with a transfemoral prosthesis. 15
The roll-over shape (ROS) is a graphical representation of the position of the COP from the point of initial contact to contralateral initial contact when viewed relative to a fixed vertical shank coordinate system. 16 The rocker-like pattern is highly consistent in able-bodied individuals and is a useful comparator because it is not affected by walking speed, 17 shoe heel height, 18 loads carried, 19 or shoe rocker radius. 20 Ankle foot orthoses (AFOs) have been evaluated to determine the effect of articulated AFOs on ROS radius of curvature 21 and to determine if clinically prescribed AFOs restored ROS to that of able-bodied individuals. 22 It has been proposed that knowledge of a prosthetic foot’s ROS could be used to align prostheses. 16 Likewise, analyzing IDEO ROS with heel wedges of different height and durometer may help us understand the effects of these wedge properties on lower limb loading.
An improved understanding of how heel wedge properties such as durometer and height affect gait, specifically during loading response, could provide a basis for selecting the most appropriate wedge or optimizing the design of the wedge. Therefore, the purpose of this study was to determine the influence of heel wedge properties on the walking gait of individuals using an IDEO. Specifically, we aimed to determine whether wedge height or durometer affects COP velocity, joint moments, or ROS during gait while using an IDEO.
Methods
A total of 12 IDEO users and 12 individuals with no lower extremity injury provided written informed consent prior to participation. This study was approved by the Brooke Army Medical Center Institutional Review Board. All participants were between the ages of 18 and 55 years. IDEO users had unilateral foot or ankle weakness or pain, had worn the IDEO for at least 2 weeks, and were able to walk without any other assistive devices. Exclusion criteria included neurologic or musculoskeletal disease in the contralateral leg, spinal cord injury, or central nervous system pathology. Able-bodied control participants had no injuries or pathologies affecting gait.
A fully replicated repeated-measures crossover design with six heel wedge conditions was used to assess the effects of height and durometer. Heel wedges, made from blocks of soft or firm Kingsley Heel Cushion Material (Kingsley Manufacturing Co., Costa Mesa, CA), were used. Durometer was tested using a Digital Durometer Type OO mounted on a Dampened Operating Stand (models DD-4-OO and OS-4H, Rex Gauge Company, Inc., Buffalo Grove, IL). The OO scale was chosen based on ASTM D2240-05:2010. 23 All soft wedges were between 50.0 and 57.0 on the OO scale, while firm wedges were between 75.0 and 78.0 on the OO scale. Wedges were cut to 1.0, 2.0, or 3.0 cm in height.
A target walking speed was calculated for each subject based on their leg length and a Froude number of 0.16. The Froude number is a dimensionless number defined as velocity squared divided by the gravitational constant times leg length.24,25 Subjects were given verbal feedback when necessary, encouraging them to walk faster or slower to ensure they were within 10% of their target speed. Controlling gait speed reduces inter-subject variation, thereby improving the ability to identify biomechanical differences between groups, 26 and improves reliability. 27 Biomechanical data were collected as participants walked over level ground at their controlled speed. All participants wore a similar brand and style of shoe (Rhino Runner (men), Reina Runner (women), Apex Foot Health and Wellness, Teaneck, NJ). Kinematic data were collected with an optoelectronic motion capture system (Motion Analysis Corp, Santa Rosa, CA) with 27 cameras recording at 120 Hz, while GRFs were recorded at 1200 Hz via five force plates (Advanced Mechanical Technology Inc., Watertown, MA) embedded in a walkway. In total, 19 reflective markers were used to track the position of the foot, shank, thigh, and pelvis in a manner consistent with published methods. 28 Markers were only placed on the side of the IDEO for the IDEO group and randomly assigned to either the right or left side for the control group. One marker was placed on the C7 vertebra to track walking velocity. IDEO users walked with each of the six different heel wedges in randomized order, until six successful trials were collected with each wedge. Control group participants wore the same standardized shoes and walked at the controlled speed until data were collected for six successful trials as described above.
After walking with each wedge, participants were asked to rate their experience walking with that wedge in terms of foot and ankle pain, comfort of the IDEO, and perceived smoothness of gait. Pain was assessed using an 11-point numerical pain rating scale, in which 0 = no pain and 10 = worst pain imaginable. Comfort and smoothness were reported using modified versions of the Socket Comfort Score. 29 Scores were from 0 = most uncomfortable to 10 = most comfortable, and from 0 = least smooth to 10 = most smooth.
Data were processed with Visual3D software (version 5, C-motion, Inc., Germantown, MD). A fourth-order low-pass Butterworth filter was applied to all data, with a 6 Hz cutoff for kinematic data and 50 Hz cutoff for GRF data. Kinematic and GRF data were synchronized and heel strike and toe off events were defined based on force plate data. Three primary outcome variables were assessed: COP velocity, joint moments, and ROS. COP velocity in the plane of the force plate was determined based on the 1200 Hz GRF data. Through inverse dynamics, joint moments were calculated. The peak internal knee extension moment, peak internal ankle dorsiflexion moment, and the time the ankle moment crossed zero, going from a dorsiflexion to plantarflexion moment, were determined.
ROS was plotted as the COP vertical position versus the COP forward position in the shank coordinate system. The shank coordinate system was defined based on the ankle joint center, knee joint center, and lateral malleolus, following previously described methods. 21 Data were not collected to determine the time of contralateral heel strike, so ROS was calculated from the point of continuous forward progression to the point at which the plot began to move downward or backward. The best-fit radius of curvature and center of curvature were determined for each ROS using a non-linear fitting algorithm 17 in MATLAB (R2015b, The MathWorks, Inc., Natick, MA).
Prior to study initiation, a power analysis was performed. Given the use of multiple dependent measures, with each considered to be of equal importance, a generic power analysis with an alpha of 0.05 and power of 0.8 was used to determine sample size. It was determined that when using a 2×3 repeated-measures analysis of variance (ANOVA), a sample size of 11 would be sufficient to detect an effect size of one standard deviation for each dependent measure.
A two-factor (height × durometer) repeated-measures ANOVA was used to evaluate interactions and main effects for each primary outcome variable (SPSS, Version 22, IBM Corporation, North Castle, NY). All data were checked for normality and data with non-normal distributions were transformed using the inverse of the data. Friedman tests were used to compare differences between wedges for self-reported outcomes. Significant outcomes (p < 0.05) of the ANOVA and Friedman tests were analyzed with post hoc paired t-tests with Bonferroni–Holm corrections.
Results
Subjects
A total of 12 IDEO users and 12 individuals with no lower extremity injury participated in the study. In the IDEO group, there were 11 men and 1 woman of age 23–44 years (mean ± standard deviation, 32.1 ± 7.5 years). Mean height for this group was 1.84 ± 0.10 m and mean body mass was 96.7 ± 23.3 kg. There was a wide range of injuries among subjects: fracture, nerve damage, tendon rupture, arthritis, fusion, and volumetric muscle loss.
The reference control group had 10 men and 2 women of age 23–45 years (33.7 ± 6.7 years), height of 1.76 ± 0.08 m, and body mass of 79.2 ± 14.4 kg. This group was significantly shorter (p = 0.048) and had a lower body mass (p = 0.040) than the IDEO group; however, body mass index was not significantly different between the two groups (p = 0.153). The age difference between the groups was not significant (p = 0.590).
COP velocity
Time to peak COP velocity had significant main effects for durometer (p = 0.002) and height (p < 0.001) (Figure 2(a)). Height was found to have a significant main effect on peak COP velocity magnitude (p = 0.039) (Figure 2(b)).
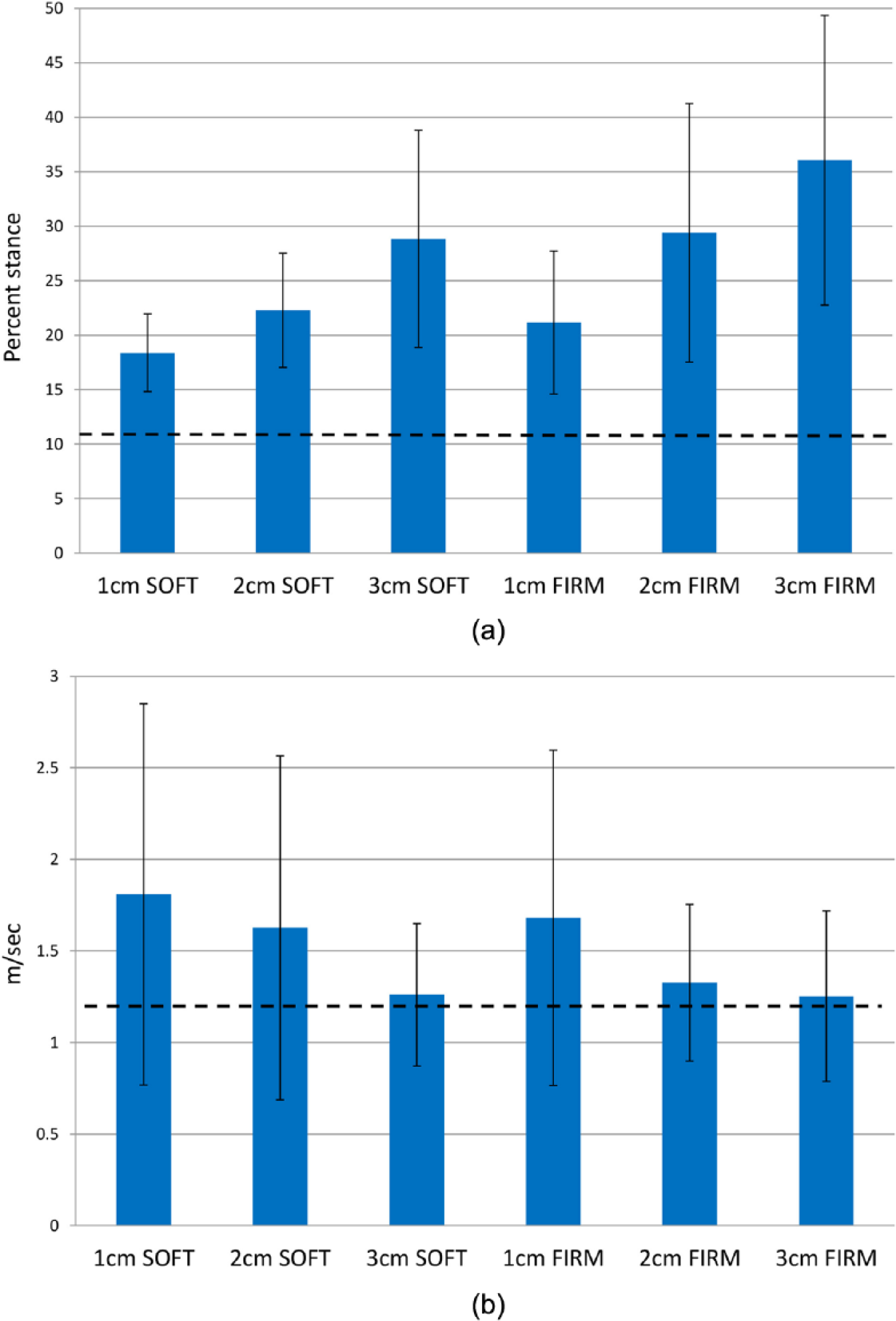
(a) Time (percent stance) to peak center of pressure (COP) velocity. The able-bodied control group is shown as a dashed line for reference. Time to peak COP velocity was significantly earlier for 1 cm heel wedges (19.8% ± 5.3% stance) compared to 2 cm wedges (25.8% ± 9.7% stance) (p < 0.001), 1 cm wedges compared to 3 cm wedges (32.4% ± 12.1% stance) (p < 0.001), and 2 cm wedges compared to 3 cm wedges (p = 0.003). Soft wedges produced peak COP velocities that were significantly earlier (23.2% ± 7.9% stance) than firm wedges (28.9% ± 12.3% stance) (p < 0.001). (b) Peak center of pressure (COP) velocity. The able-bodied control group is shown as a dashed line for reference. Peak COP velocity was significantly greater for 1 cm heel wedges (1.74 ± 0.96 m/s) than 3 cm wedges (1.26 ± 0.42 m/s) (p = 0.008).
Joint moments
There was a significant interaction of heel wedge height and durometer on time to peak internal dorsiflexion moment (p = 0.012) and time of ankle moment zero crossing (p = 0.033) (Figure 3(a), Table 1). There was a significant main effect for wedge height on peak dorsiflexion moment (p < 0.001). Peak internal knee extension moment had a significant interaction effect of height and durometer (p = 0.037) and the time to the peak knee extension moment had a significant main effect for height (p = 0.002) (Figure 3(b), Table 1).
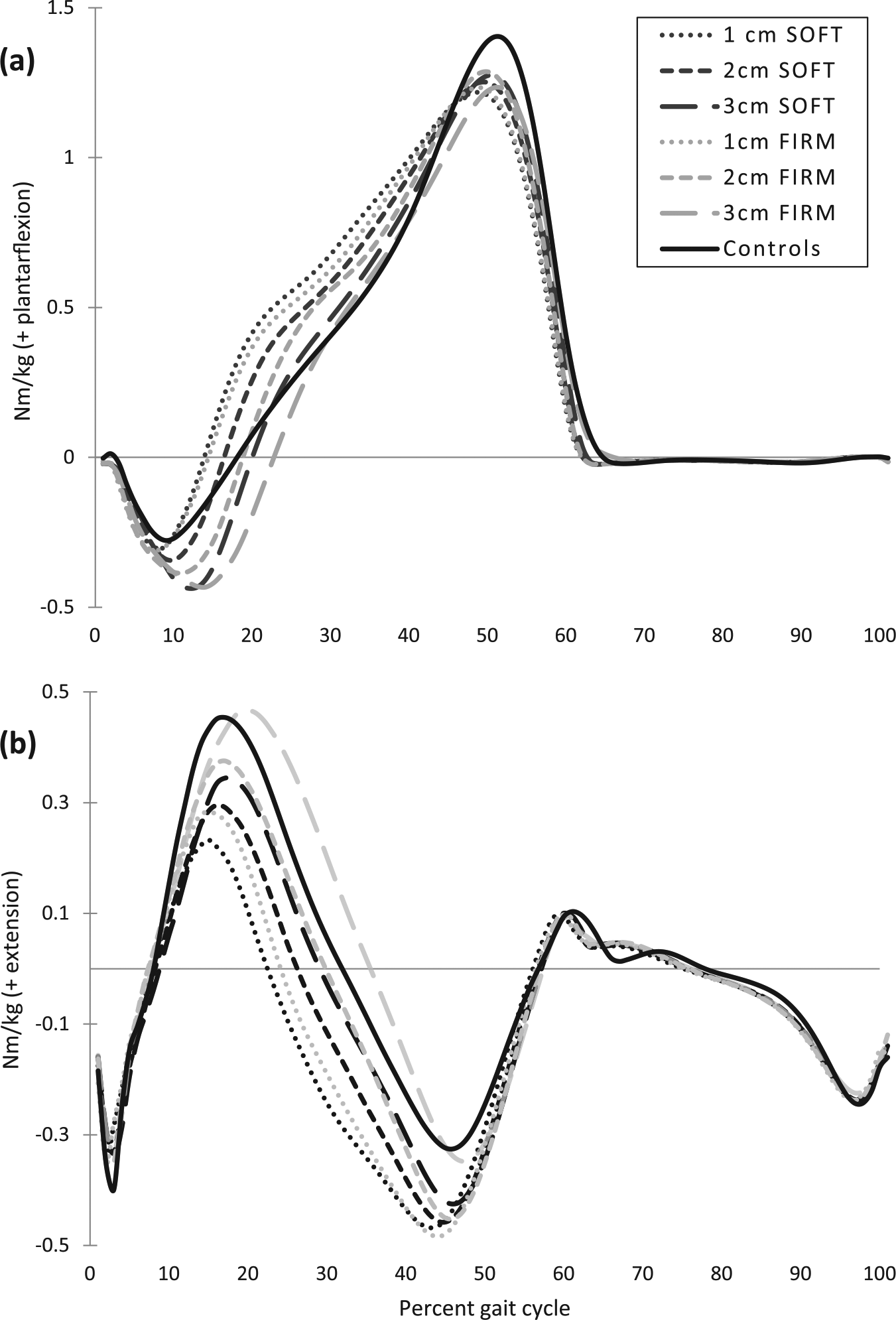
Average internal ankle (a) and knee (b) moments, normalized to body mass. The able-bodied control group is shown for reference.
Internal moment events for 12 IDEO users.
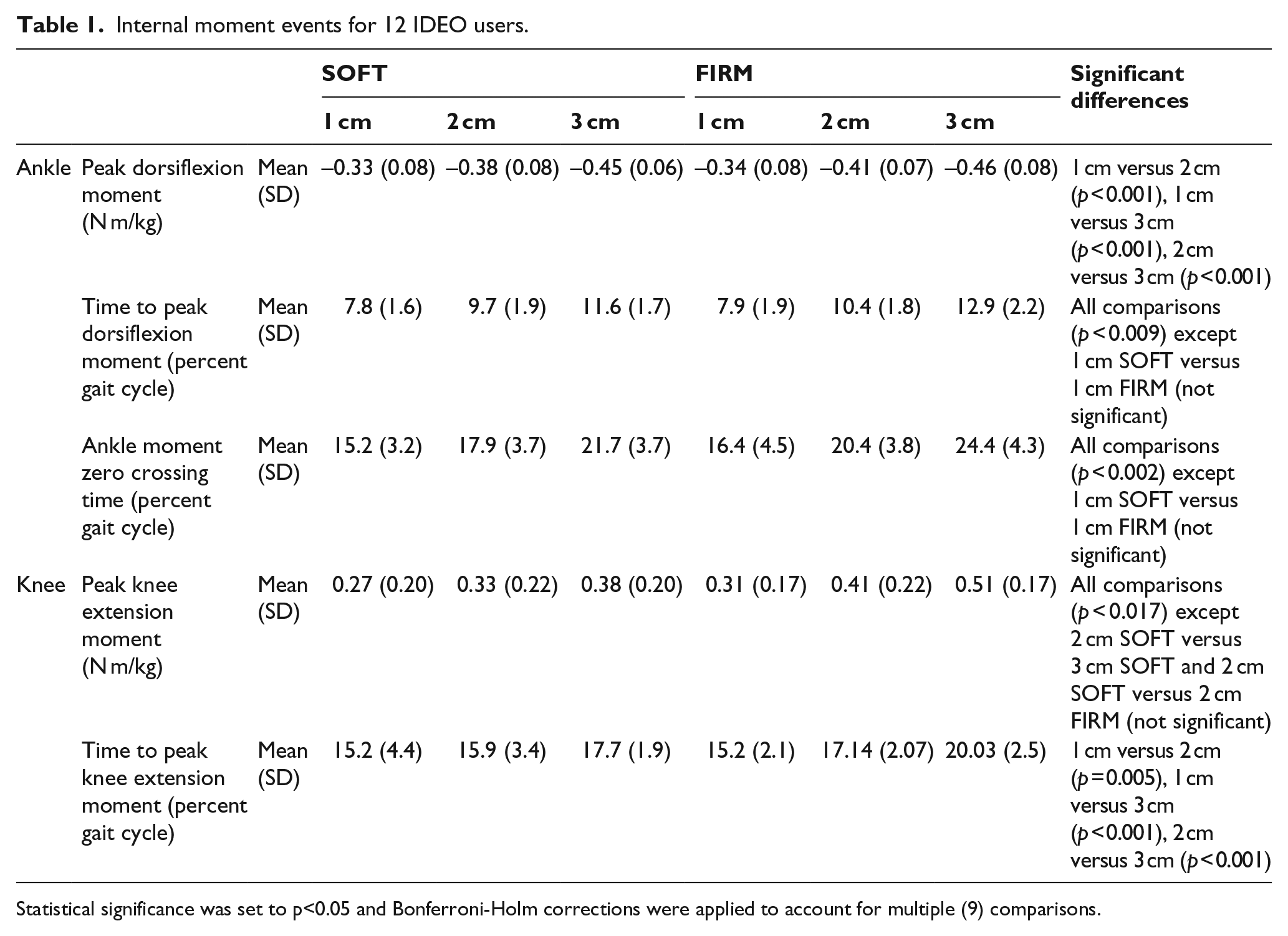
Statistical significance was set to p<0.05 and Bonferroni-Holm corrections were applied to account for multiple (9) comparisons.
ROS
There was a significant main effect for heel wedge height on ROS radius of curvature (p < 0.001) (Figure 4) and ROS center of curvature vertical position (p < 0.001), as well as a significant interaction of height and durometer for center of curvature anterior-posterior (A-P) position (p < 0.001) (Figure 5).
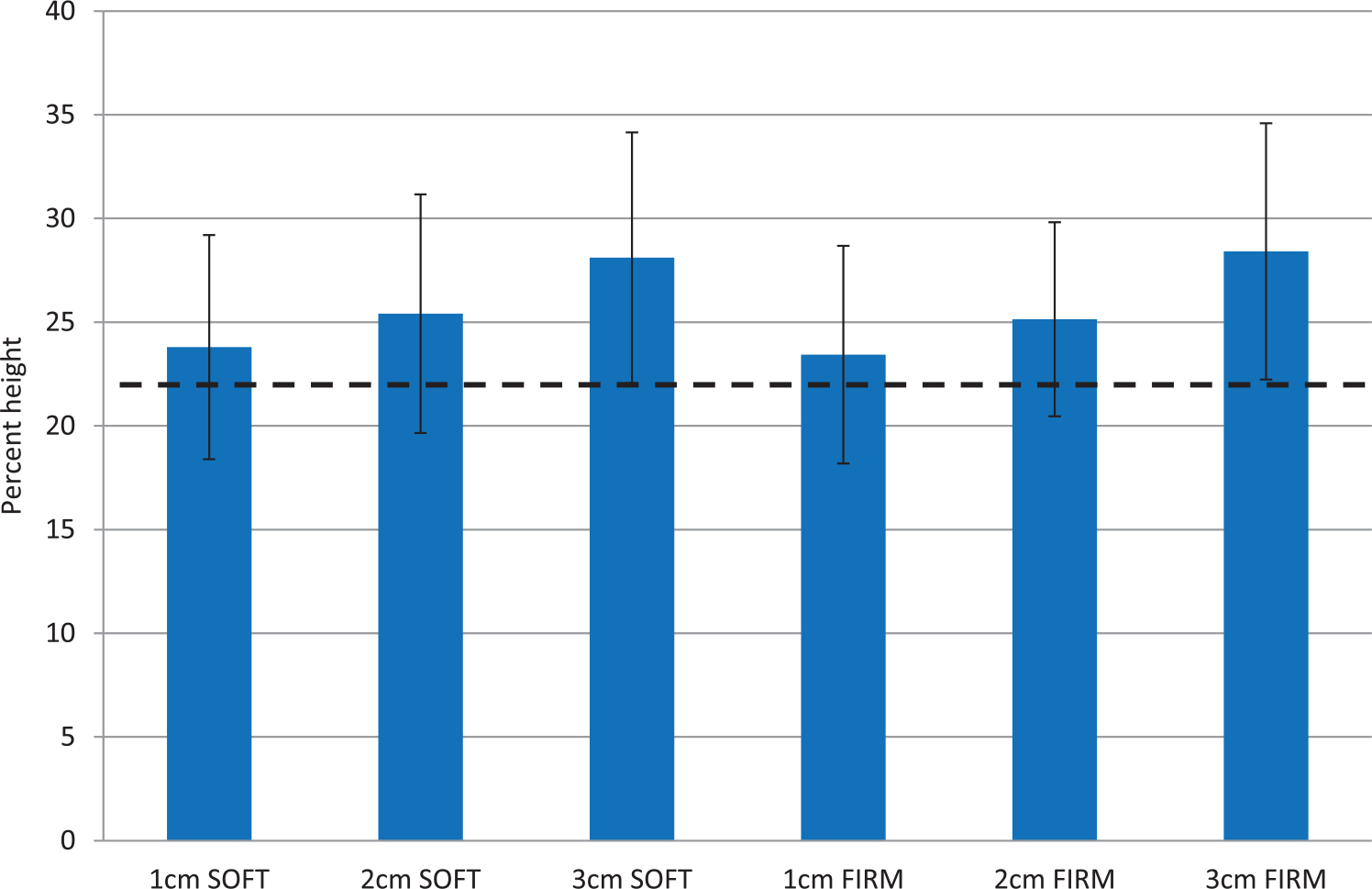
Roll-over shape (ROS) radius of curvature normalized to body height. The able-bodied control group is shown as a dashed line for reference. Collapsing across durometers due to lack of a main effect for durometer, radius of curvature for 3 cm wedges (27.9 ± 5.9% height) was significantly greater than 1 cm wedges (23.6 ± 5.1% height) and 2 cm wedges (25.2 ± 5.2% height) (both p<0.001). Two cm wedges also produced greater radius of curvature than 1 cm wedges (p<0.001).
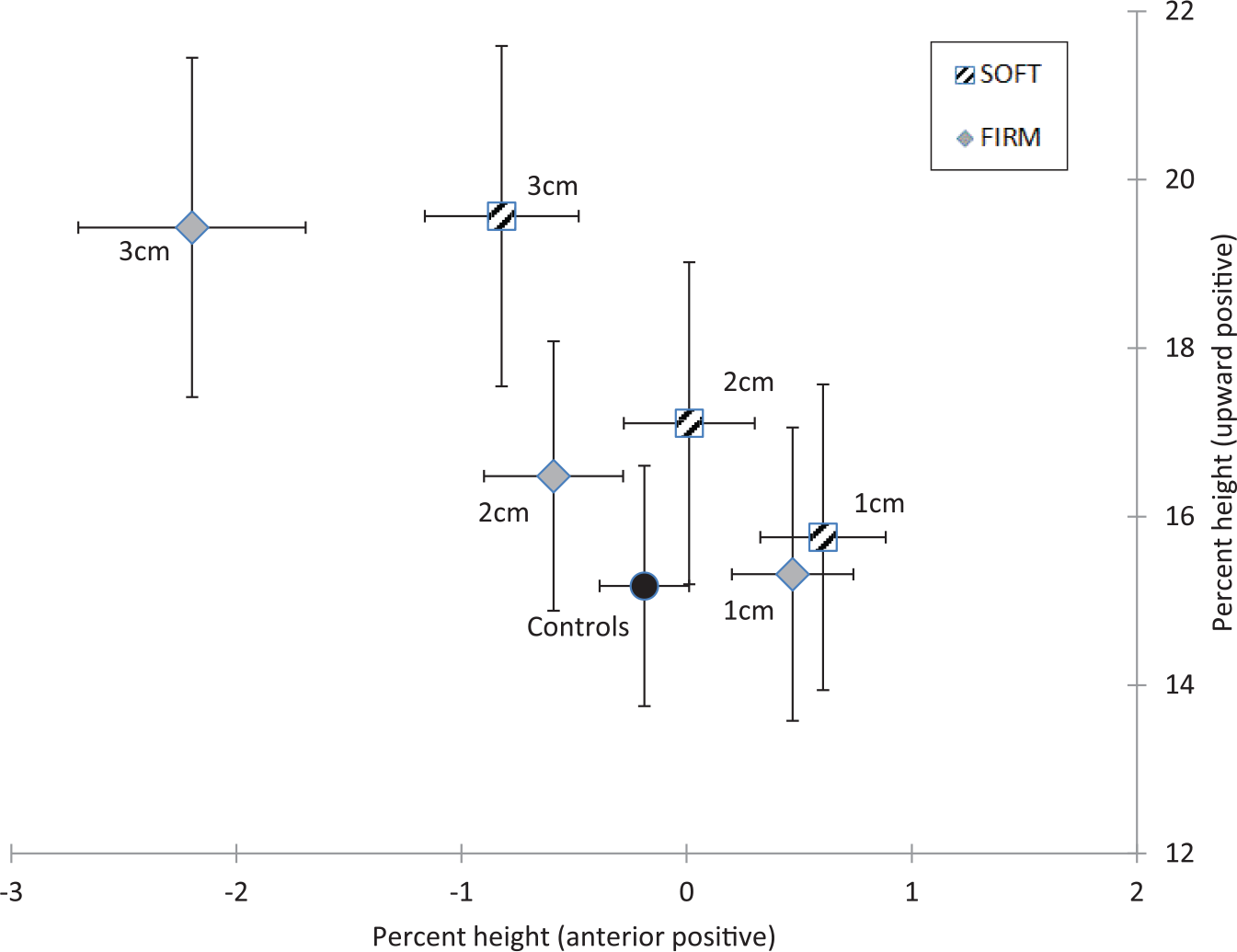
Roll-over shape (ROS) center of curvature position relative to ankle joint center, normalized to body height (mean with SEM). The able-bodied control group is shown for reference. Post hoc comparisons for anterior-posterior position revealed that all differences within height and within durometer were statistically significant (p<0.001), except 1 cm firm vs. 1 cm soft (p=0.052). For vertical position there were significant differences between all conditions (all p<0.001).
Self-reported outcomes
Comfort and smoothness showed similar trends with the 2 cm soft, 3 cm soft, and 2 cm firm wedges receiving the highest ratings in both of these categories; although with the Bonferroni–Holm correction applied, not all differences were statistically significant (Table 2). Pain ratings were also best for these three wedges, although overall pain ratings were very low and no differences in pain between wedges were statistically significant (Table 2).
Self-reported outcomes for 12 IDEO users.
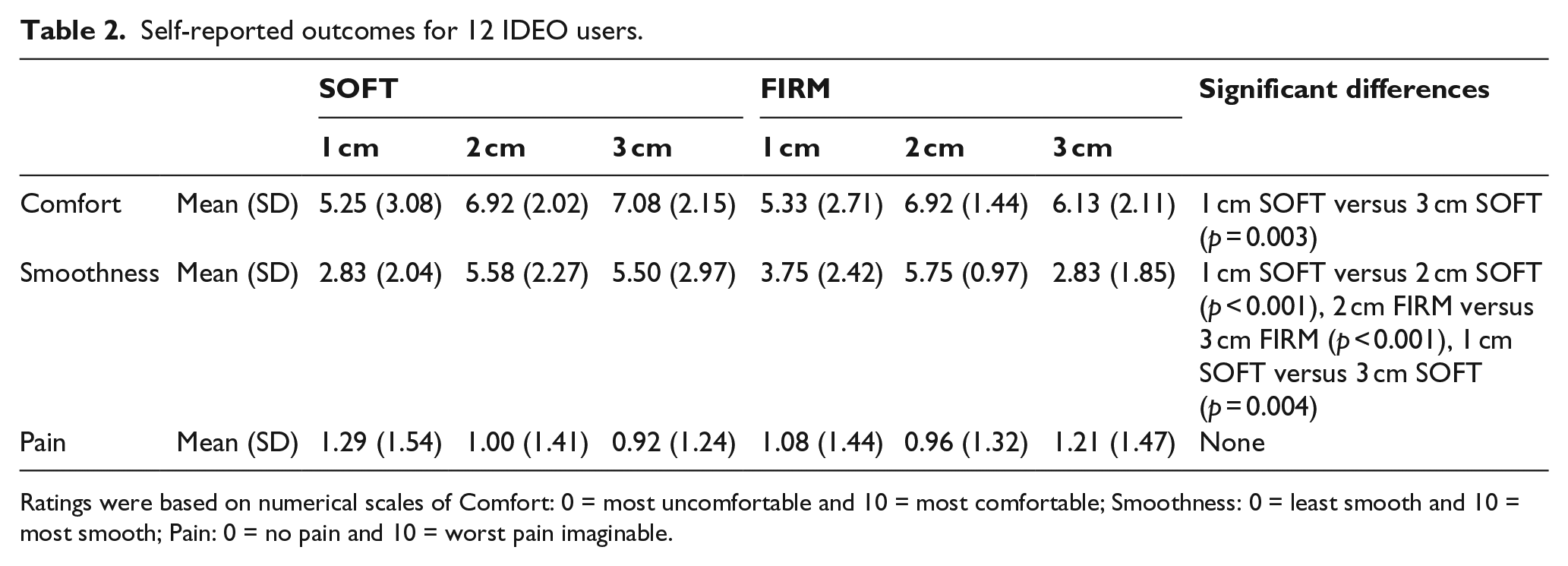
Ratings were based on numerical scales of Comfort: 0 = most uncomfortable and 10 = most comfortable; Smoothness: 0 = least smooth and 10 = most smooth; Pain: 0 = no pain and 10 = worst pain imaginable.
Discussion
The purpose of this study was to determine the influence of heel wedge properties on the walking gait of individuals using an IDEO. The results demonstrate that wedge height and durometer have direct effects on measures of limb loading and patient perception and are important to consider when adjusting an IDEO-heel wedge-shoe system. During able-bodied gait, the ankle plantarflexes to bring the forefoot into contact with the ground and initiate controlled progression of the COP under the foot. With the IDEO, compression of the heel wedge is required to simulate plantarflexion, allowing gradual lowering and loading of the forefoot, and associated COP progression. As the wedge compresses, the IDEO pivots forward rotating about the heel resulting in forefoot loading and forward movement of the COP.
The timing of peak COP velocity was affected by both wedge durometer and height. Peak COP velocity occurred earlier with shorter and softer heel wedges (Figure 2(a)), and in general, the magnitude was greater with shorter (and a non-significant trend for softer) wedges (Figure 2(b)). In theory, a large peak COP velocity represents a somewhat abrupt transition of the COP from the heel to the forefoot. The greater the peak, the more abrupt the transition. The abrupt transition with 1 cm wedges likely contributed to these wedges being rated as the least comfortable and tied for least smooth among all wedges (Table 2).
The ankle moment timing and magnitude data are consistent with the COP velocity timing and magnitude results. Peak dorsiflexion moments were greater and later in the gait cycle for taller heel wedges and the time of moment zero crossing was later for taller and firmer wedges (Figure 3(a), Table 1). This may be due to the taller and firmer wedges taking longer to compress, resulting in a more posterior position of the COP and a larger distance from the COP to the ankle joint center. Smoothness ratings were best for 2 cm firm and 2 cm soft wedges, which were the closest in timing to the able-bodied ankle moment zero crossing (19.2% ± 2.8% gait cycle). This may suggest a preference for heel wedges, which result in a transition from a dorsiflexion to a plantarflexion moment at about the same point in the gait cycle as able-bodied gait.
Knee moment data showed systematic trends in response to heel wedge changes. Peak knee internal extension moments were greater for taller and firmer heel wedges and occurred later in the gait cycle for taller wedges (Figure 3(b), Table 1). This is consistent with an earlier study in which insole wedges were used to change heel height for healthy adults wearing rigid AFOs and found increasing heel height led to greater knee extension moments. 30 The timing of the peak extension moment for the 2 cm firm heel wedge was closest to the timing for the able-bodied control subjects (16.9% ± 1.5% gait cycle). This may indicate that perceived smoothness of gait is influenced by peak knee extension moment timing and a peak time similar to able-bodied gait is desirable, as the 2 cm wedges were highest ranked in smoothness.
Although able-bodied individuals have been shown to adapt their kinematics to maintain a consistent ROS, 20 ankle motion is restricted for individuals wearing an IDEO and therefore ROS was dependent on heel wedge properties. In this study, taller wedges produced ROS radii that were significantly larger (Figure 4). Additionally, ROS centers of curvature for taller and firmer wedges were significantly further posterior (Figure 5). Generally, IDEO users gave the best smoothness ratings to wedges with ROS centers of curvature closest in A-P position to those of able-bodied individuals. Recognizing that the alignment of the IDEO-heel wedge-shoe system is defined by the angle of the shank relative to the foot, 30 taller and firmer wedges are conceptually similar to dorsiflexed prosthetic feet, which also have larger ROS radii and more posterior centers of curvature. 31 This is consistent with our supposition that changing the IDEO heel wedge is analogous to changing prosthetic alignment. Likewise, changing the heel wedge can be viewed in terms of tuning the AFO footwear combination (AFOFC) which involves adjusting the heel sole differential of the AFOFC to obtain the desired shank to vertical angle at midstance. 32 In this study, the heel sole differential of the IDEO-heel wedge-shoe system was manipulated by changing heel wedge height and durometer. Tuning has been shown to be beneficial in stroke rehabilitation with solid AFOs, 33 to produce improvements in gait over time in hemiplegia as compared to an untuned AFOFCs, 34 and to have potential benefits for children with cerebral palsy. 35
Future research to determine optimal heel wedge configurations, including alternate materials or designs, is warranted. The findings from this study suggest that simple, low-cost solutions may allow a steadier forward progression of the COP when walking with an IDEO. It may be possible to implement the use of heel wedges to other types of orthoses as well, extending these findings to an even wider range of patients.
Limitations of this study include the relatively small sample size, heterogeneity of participants, and limited mechanical testing. Although the study was sufficiently powered, the overall sample size was relatively low and future studies including more participants may provide additional sensitivity to detect the effects of heel wedge properties. Although the variety of pathologies and injuries exhibited by the IDEO users increased external validity, participants may have employed slightly different strategies to compensate for the effects of the different wedges. Furthermore, mechanical testing was limited to durometer testing of the wedge alone. Assessing the combined hardness of the heel wedge-shoe combination and examination of the interaction between wedge height and durometer on the resultant compressed height may have further clarified results.
Conclusion
Changes to heel wedge height and durometer can be used to easily and inexpensively change limb loading with the IDEO. Systematic changes in height and durometer clearly affected the loading of the foot, as indicated by the COP position and velocity, which in turn influenced ankle and knee moments and ROS. Participants tended to prefer heel wedges which produced ankle moment zero crossing timing, knee peak extension moment timing, and ROS center of curvature A-P position which were close to that of able-bodied individuals. Selecting the most appropriate wedge height and durometer has great potential to improve an individual’s gait.
Footnotes
Acknowledgements
The views expressed herein are those of the authors and do not reflect the official policy or position of Brooke Army Medical Center, the US Army Medical Department, the US Army Office of the Surgeon General, the Department of the Army or the Department of Defense, or the US Government.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.