
Abstract
Background:
Biomechanical factors, such as spinal deformities can result in balance control disorders.
Objectives:
The purpose of this study was to examine the effect of bracing on static and dynamic balance control of hyperkyphotic female adolescents.
Study Design:
Clinical trial.
Methods:
A force platform was employed to record center of pressure (COP) parameters. Ten adolescents undergoing Milwaukee brace for hyperkyphosis and 14 normal subjects participated in the study. The COP data were collected with and without brace immediately on first day and after 120 days of continuous brace wear.
Results:
No significant difference was found in dynamic and static balance tests with and without brace on the first day (P > 0.05). After 120 days, the values of COP displacement in functional reach to the right and left for the hyperkyphotic adolescents when performing without brace enhanced significantly compared to the first day. The forward reach distance was not significantly different between the normal and hyperkyphotic subjects (P = 0.361); however, hyperkyphotic participants had significantly smaller reach distance in the functional reach to the right (21.88 vs. 25.56cm) and left (17.04 vs. 21.25cm).
Conclusion:
It might be concluded that bracing had a possible effect on improvement of dynamic balance performance, because the subjects could reach the target in dynamic reach tests with higher displacement in sagittal plane without losing their balance control.
Clinical relevance
Little is known about the biomechanical aspects of brace wear in individuals with hyperkyphosis. This study investigated balance differences between the healthy and hyperkyphotic individuals, and outcomes of Milwaukee brace wear. It might provide some new insight into the conservative treatment of hyperkyphosis for clinicians and researchers.
Keywords
Background
Postural stability during quiet standing and balance performance may be altered by different spinal deformities, such as scoliosis and hyperkyphosis.1,2 Normal curvature of spine keeps the head over the pelvis and acts like a shock-absorber in order to distribute the mechanical forces during movements. 3 These curves become abnormal in scoliosis and hyperkyphosis. Small alteration in body upright alignment requires corrective torques to maintain the balance and stability. Human upright posture is adjusted through continuous reactions to sensory information from the proprioceptive, visual and vestibular systems. 4 When the vertical vector of the body’s center of mass (COM) is positioned within the base of support (BOS), static balance is achieved and maintaining dynamic balance requires sufficient torques to keep COM motion exactly over the BOS. 5 Several temporal and spatial parameters have been used to assess the stability control during quiet standing and functional tasks. Some of them are maximum, minimum, peak-to-peak and mean displacements of centre of pressure (COP), COP excursions, velocity, standard deviation of COP displacement (root-mean-square) and time-frequency.6.7 Functional reach is the main part of most activities of daily living (ADL). It is said to reflect balance ability and is related to risk of falling and performance in functional tasks. It is performed in multi directions as forward, backward and lateral reach. 8 During the task, one is required to move the body’s center of mass toward the front, back or lateral edges of the base of support in a well-controlled manner. Therefore, it is often considered an indicator of boundary of stability. 9
Bracing is usually recommended for the treatment of hyperkyphosis if the patient is skeletally immature for a kyphotic deformity of 40–45 degrees or greater.10,11 The most common type of hyperkyphosis treated with orthosis is Scheurmann’s disease. The goal of this treatment is not only to arrest progression but also to achieve permanent improvement in the thoracic kyphosis.12-14
Postural control disorders and gait stiffness have been reported in adolescents with spinal deformities, such as scoliosis, especially when visual and somatosensory systems are challenged simultaneously.15-19 Lateral stability of these patients also has been shown to be poorer compared with normal subjects.20,21 External factors, such as spinal bracing and backpack weight can further increase the load on the balance system and have adverse effects on control of balance.21,22 Sales De Gauzy et al. 23 compared static balance of subjects with adolescent idiopathic scoliosis (AIS) with and without brace and reported significantly poorer static balance performance with brace. Research studies suggest that both bracing and backpack carriage independently can result in inferior balance performance. Chow et al. 22 showed that bracing might not have an instant effect on a balance control system, unless somatosensory input is impaired. Lamantia et al. 24 found immediate increase in cerebellar feedback due to bracing in scoliotic patients, and improved central brainstem (oculomotor) function in the cases studied. They concluded that bracing affects the central nervous system, causing brainstem and cerebellar functional improvement, but they suggested further research in order to prove the idea of positive effect of bracing as an outcome of central neurological rehabilitation.
On the other hand, Konz et al. 25 noted that thoracolumbosacral orthosis (TLSO) altered the gait pattern of healthy subjects since it restricted the spinal motion which is said to contribute considerably to maintain the balance. A recent study by Sadeghi et al. 26 found less control in the medio-lateral (ML) axis and augmented rigidity in the antero-posterior (AP) direction for standing balance of in-brace compared with out-of-brace conditions.
However, to the authors’ knowledge, no study has been done on the effect of bracing on balance control of hyperkyphotic adolescents. The purpose of this study was, therefore, to examine the effects of long-term brace wear during 120 days on static and dynamic postural balance parameters in hyperkyphotic female adolescents. Our hypothesis was that bracing will deteriorate the balance of hyperkyphotic subjects in immediate and long-term usage. We also hypothesized that functional reach will be restricted by the brace so that the reach distance will be reduced as compared to performance without brace.
Methods
Ten female adolescents with hyperkyphosis (mean Cobb angle 53), between ages 10 and 18 (mean: 13.03; SD 1.3) with an average height of 161 cm (SD 6.2), and an average mass of 51.75 kg (SD 9.0) were selected to participate in this study through convenient sampling. The inclusion criteria for hyperkyphotic subjects were as follows:
• No previous operative treatment • Cobb angle between 40° and 70° • No history of brace wear • Milwaukee brace was prescribed as conservative treatment • No other known musculoskeletal disorder including scoliosis.
Fourteen healthy controls also volunteered to participate in the study upon an orthopedic surgeon approval of normal spine curvature. Their mean age, mass and height of the control group were 14.86 years (SD1.5), 55.68 kg (SD5.3) and 160.21 cm (SD10.6), respectively. There were no significant differences (P > 0.05) between the age, height and weight of the two groups. All the participants and their parents were asked to give an informed consent prior to taking part in the experiment. Ethical approval was obtained from the ethics committee of Tehran University of Medical Sciences.
To ensure technical consistency, 10 Milwaukee braces were fabricated for hyperkyphotic subjects by one certified orthotist according to the orthopedic specialist prescription. All the Milwaukee braces required to have a cowhorn outrigger, which is used to encourage shoulder retraction through kinesthetic response (Figure 1). The orthosis check-out was performed based on the guideline of Scoliosis Research Society (manual of bracing for Scheuermann’s kyphosis) 27 and the orthopaedic specialist criteria for brace approval. The participants were required to wear the brace 23 hours per day.

Front (right) and lateral (left) views of the Milwaukee brace for hyperkyphosis used in this study.
Clear explanation of the experiments was provided for each subject. Data collection was conducted at the Rehabilitation Research Center of Tehran University of Medical Sciences, Biomechanics Laboratory.
Following the orthotic check-out by one certified orthotist and the specialist, each subject was referred to the Biomechanics Laboratory of Rehabilitation Research Center, Tehran University of Medical Sciences, for the experiments. Each participant stood barefoot on a force platform (Bertec Load Transducer Force Plate, AM-6700), with arms relaxed at the sides, a comfortable stance, 28 an angle of 14 degrees between the long axes of the feet and shoulder-width distance between the feet. 29 Standing balance is frequently measured by single-limb and double-limb timed stance tests with eyes open and with eyes closed. 30 The COP data were recorded in single and double upright positions, in and out of brace for each subject. The experiments in single upright position were repeated with open and closed eyes. For single upright balance evaluation, the subjects were required to stand on the dominant limb with their arms relaxed at the sides. The sampling rate was 200 Hz and the duration of each test was 20 s.
Functional reach was also tested in three conditions of forward reach and lateral reach (with right and left hand), both in and out of brace. The test has reportedly good validity and can be used as a reliable method to identify individuals who are at risk of falling. 9 Functional reach was measured as follows: a yardstick was attached to a metal telescopic stand at the level of a subject’s shoulder (Figure 2). The subjects then flexed their shoulders 90° forward and lateral with the elbow in full extension while standing comfortably. The starting position at the third finger tip was recorded on the yardstick. Next, the subjects were asked to reach forward and lateral as far as possible and displace a moveable marker on the yardstick. The location of the third finger tip was recorded again. The reach distance was calculated in centimeters as the difference between the start and end position.9,31 Taking a step or losing the balance were considered trial failure and needed to be repeated. The participants performed the functional reach tests in double upright position on both feet. Three trials were carried out for each condition. 22 In order to minimize the learning and fatigue effects, the tests were carried out randomly with a one-minute rest between trials.

The front (right) and lateral (left) views of the device used for functional reach test.
The most reproducible method to compute standing balance is based on COP. The COP motion parameters were recorded as mean total velocity (TV), path length (PL), maximum AP COP displacement (MCOPAP) and ML COP displacement (MCOPML). 30 These parameters were computed by Pro-vec software (1996 MIE Medical Research Ltd; Pro-vec 5.0) and used for further statistical analysis. The maximum reach distance (RD) was also calculated for each dynamic test and recorded for all the subjects. Both hyperkyphotic and healthy subjects returned after 120 days and the balance tests were repeated.
The normal distribution of all variables was tested by Kolmogorov-Smirnov test. Since the parameters had a normal distribution, the parametric statistical test was adopted. Independent-samples t-tests were used to compare the mean COP values between the normal and hyperkyphotic subjects. The difference in performance of hyperkyphotic subjects in day 120 compared to day 0 was obtained by paired-sample t-test. Repeated measures ANOVA was employed to analyze the mean value of each variable, with within-subjects factors of bracing (with and without), time (day 0 and 120), vision (eye open and closed) and stance condition (single or double limb support). All analyses were performed by SPSS 16 (SPSS Inc.). The level of statistical significance was set at 0.05.
Results
Immediate
Some significant differences were seen between the normal participants and the hyperkyphotic subjects (Table 1). On the first day of experiments, significant differences were noted in mean total velocity (TV), MCOPAP, MCOPML and COP path length (PL) in static balance tests, unilateral stance with eyes closed compared to eyes open in both braced and non-braced conditions. Brace had no immediate effect on static balance performance; however, some COP parameters were significantly different in braced and non-braced performance in functional reach tests (Table 2). A summary of the levels of significance between the mean values of COP parameters in static balance Tests in the hyperkyphotic subjects is presented in Table 3.
Results of static and dynamic performance of the hyperkyphotic (without brace) and normal subjects on the first day.
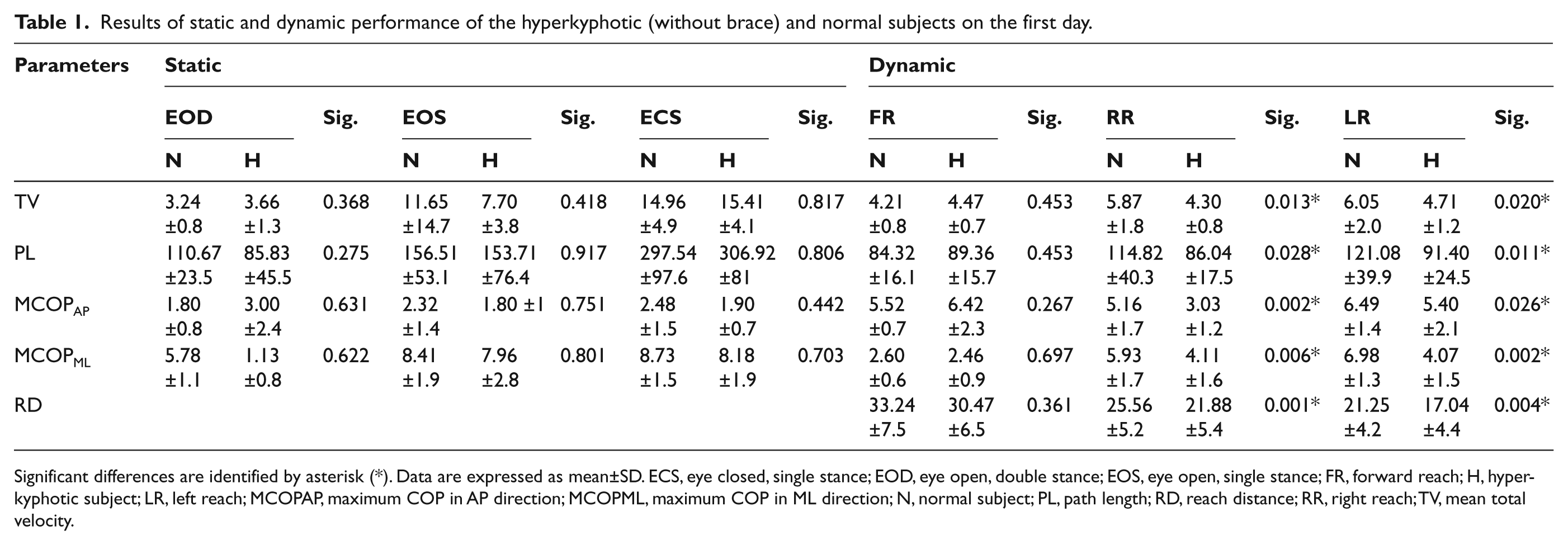
Significant differences are identified by asterisk (*). Data are expressed as mean±SD. ECS, eye closed, single stance; EOD, eye open, double stance; EOS, eye open, single stance; FR, forward reach; H, hyperkyphotic subject; LR, left reach; MCOPAP, maximum COP in AP direction; MCOPML, maximum COP in ML direction; N, normal subject; PL, path length; RD, reach distance; RR, right reach; TV, mean total velocity.
The comparison between static and dynamic performance with and without brace in the hyperkyphotic subjects on the first day.
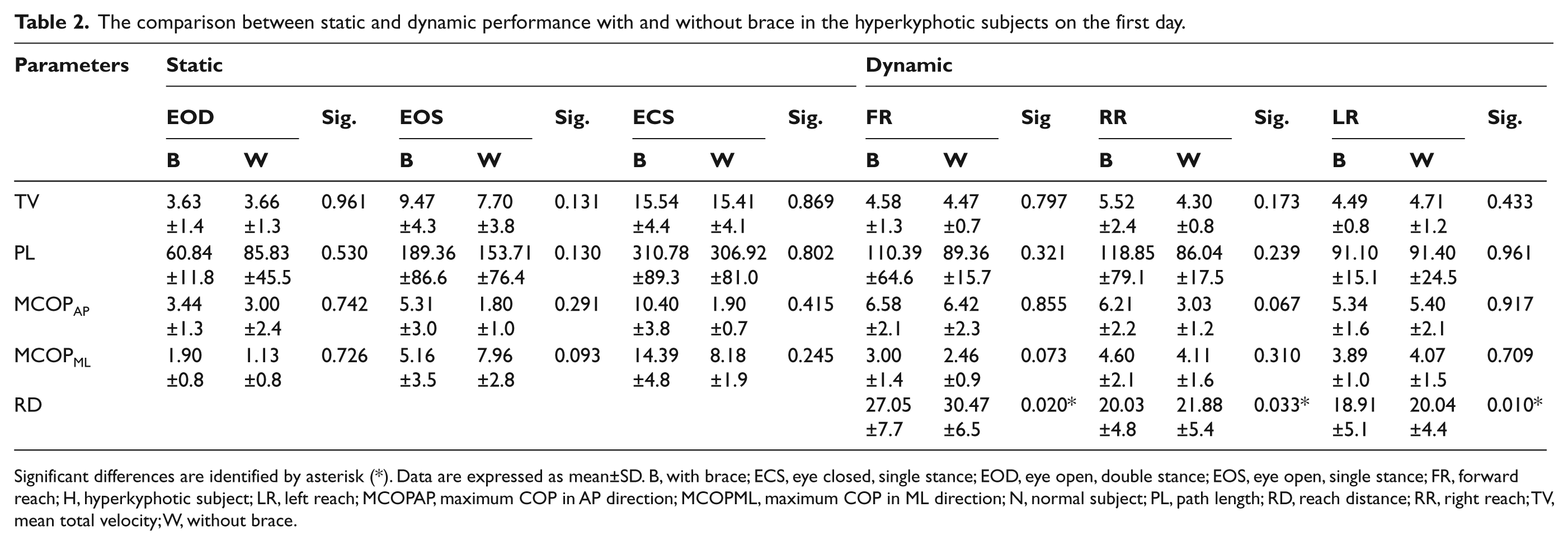
Significant differences are identified by asterisk (*). Data are expressed as mean±SD. B, with brace; ECS, eye closed, single stance; EOD, eye open, double stance; EOS, eye open, single stance; FR, forward reach; H, hyperkyphotic subject; LR, left reach; MCOPAP, maximum COP in AP direction; MCOPML, maximum COP in ML direction; N, normal subject; PL, path length; RD, reach distance; RR, right reach; TV, mean total velocity; W, without brace.
Effects of vision, stance condition and brace on the COP parameters in static balance tests for day 0 and after 120 days in hyperkyphotic subjects (n = 10).
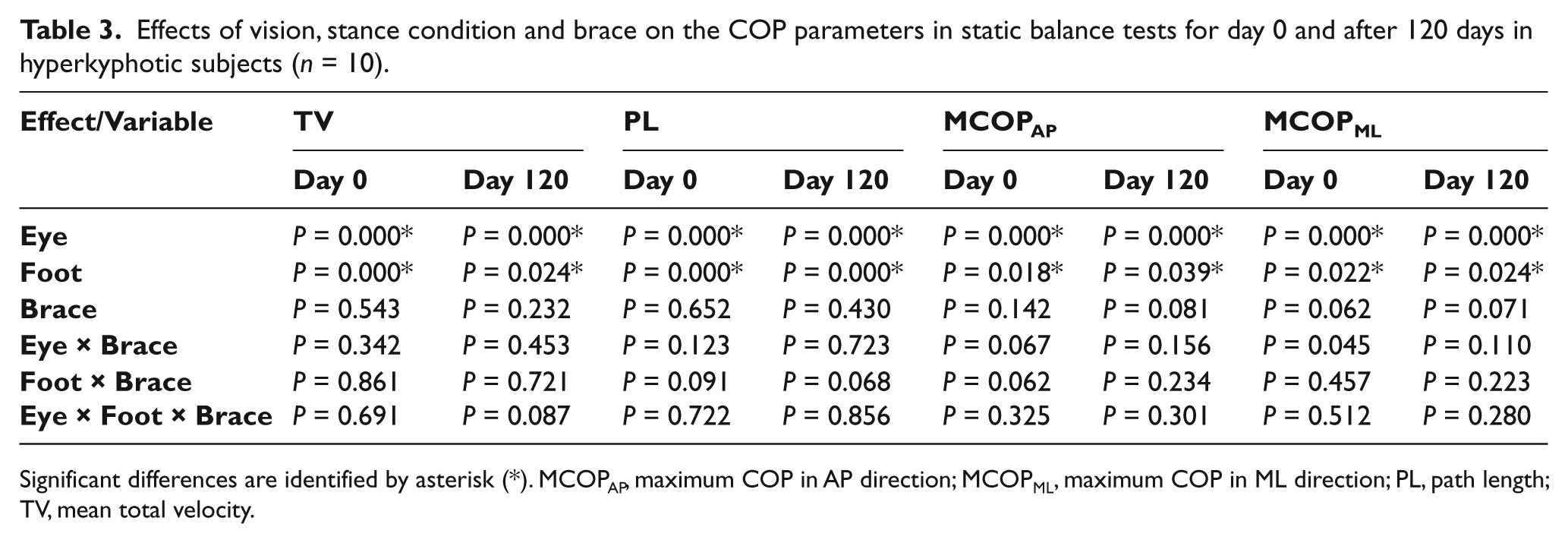
Significant differences are identified by asterisk (*). MCOPAP, maximum COP in AP direction; MCOPML, maximum COP in ML direction; PL, path length; TV, mean total velocity.
Long term
After 120 days, significant differences were found in all COP parameters during the static balance tests. These significant values were associated with unilateral stance and closed eyes both with and without the brace (Table 3). The values for all the variables were higher when participants performed the task with closed eyes (P < 0.05). However, the brace did not cause significant difference in the COP parameters in static tests.
The effect of brace on dynamic balance performance was not proved on the day 120. Nevertheless, the subjects demonstrated significant increase in the mean TV, PL, MCOPAP, MCOPML and RD without brace in dynamic balance tests during right and left reach as compared with the day 0 (all P-values < 0.05). Interestingly, it was also noted that the above-mentioned mean values had become closer to the values of the normal subjects after 120 days (Table 4).
Comparison of variables between the hyperkyphotic subjects without brace after 120 days and the normal participants.
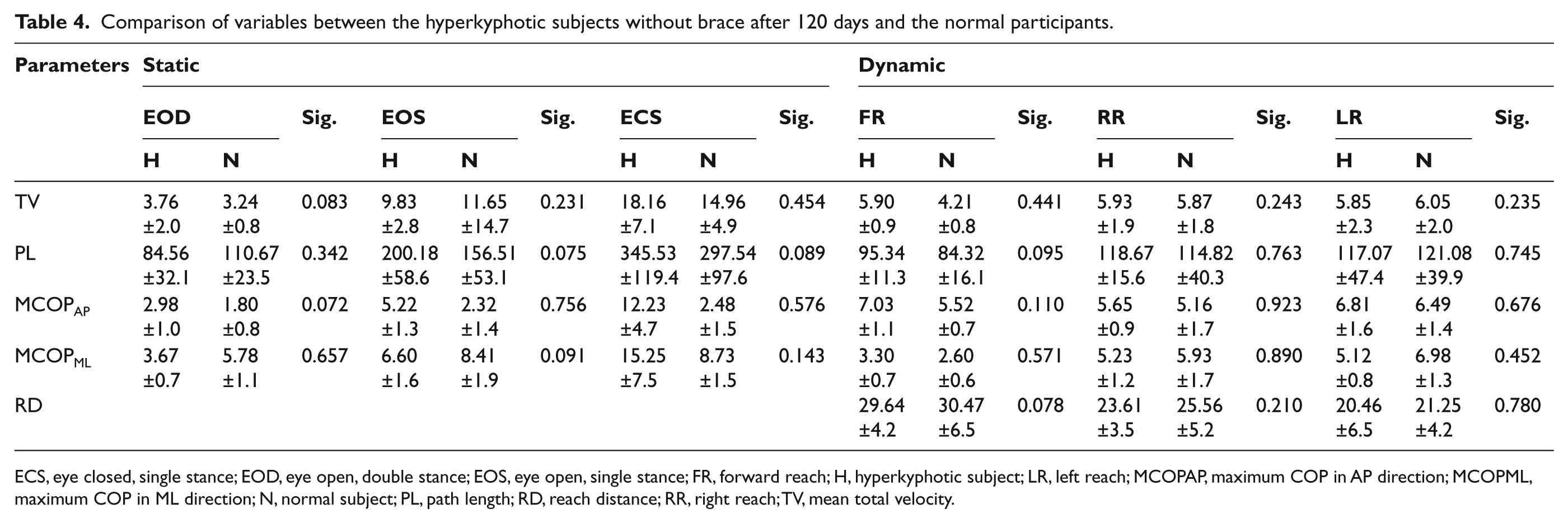
ECS, eye closed, single stance; EOD, eye open, double stance; EOS, eye open, single stance; FR, forward reach; H, hyperkyphotic subject; LR, left reach; MCOPAP, maximum COP in AP direction; MCOPML, maximum COP in ML direction; N, normal subject; PL, path length; RD, reach distance; RR, right reach; TV, mean total velocity.
Discussion
Bracing has been shown to improve the hyperkyphosis during treatment. 12 Few studies have addressed the effect of a brace on balance in patients with AIS, but to our knowledge there is no study regarding hyperkyphotic patients. This study aimed to assess the effect of bracing (Milwaukee brace) on static and dynamic balance parameters of female adolescents with hyperkyphosis. To this end, both immediate (day 0) and long-term (after 120 days) effects of bracing on COP displacements during quiet standing and functional performance were assessed.
Immediate effect
Over many years of study, COP displacements have been considered as a fair way to evaluate the human postural stability. 32 Several studies have shown that asymmetrical weight distribution, and forward or backward leaning could result in larger COP displacements along the AP and ML axes, respectively. 33 Understanding the COP displacements helps in detecting the instability during quiet standing or walking.
Although it seems that limitation of the spinal and pelvic motion by bracing may impose restriction on the ability of the spine as a contributor to the balance function, our hypothesis that the brace would have immediate effect on balance parameters was not supported. Under normal conditions, balance is maintained by an ‘ankle strategy’ that helps maintaining the balance to keep the COP within the base of support. 34 As such, it might be consistent with a previous study that indicated bracing affects the balance function of adolescents with idiopathic scoliosis, only under concurrent challenge of the proprioceptive (on foam base) and visual systems. 22 Nevertheless, another study showed deterioration of balance performance in quiet standing by brace wear, even though the proprioceptive system was not challenged. However, the authors did not report the experimental procedures and results in detail. 14 It might also be concluded that even in dynamic balance tests which increased the challenge to balance, the strategy did not shift to motion of the spine and pelvis and the participants relied on ankle strategy or they compensated the trunk limitation by relying more on ankle strategy.
The findings of this study showed that the normal and hyperkyphotic subjects performed similarly in static balance tests (Table 1). As expected, a significant increase in COP parameters was observed in the static balance tasks following the visual challenge. Furthermore, both normal and hyperkyphotic subjects showed significant increase in COP parameters when standing on one leg compared to the bilateral stance. No interaction was found between bracing and visual conditions.
The hyperkyphotic participants could not perform in functional reach tests comparable to the normal subjects, particularly in lateral reach to right and left. It might be associated with the imbalance in the supporting anterior and posterior soft tissues and musculature. 35 Patients with Scheuermann’s disease usually have a rigid hyperkyphosis in the thoracic spine and a compensatory hyperlordosis of the cervical and/or lumbar spine. Intervertebral range of motion (ROM) is dependent upon intervertebral ligamentous length. All the posterior intervertebral ligaments are stretched toward their limits as the forward flexion limit is approached. If the spine is then flexed leftward, this motion tends to require lengthening of all the ligaments on the right side of the vertebrae. However, the ligaments of the right posterior quadrant are already stretched from forward flexion so that will limit leftward ROM. Therefore, it might be concluded that reduced lateral ROM in hyperkyphotic spine may lead to weak performance in functional reach.
The smaller COP path length demonstrated by subjects with hyperkyphosis in functional reach tests suggests that our subjects were less willing and/or able to deviate from their initial COP position when compared to our sample of normal individuals, indicating a voluntary or involuntary self-limiting strategy.
Reach distance during functional reach test is employed in research and clinical practice to assess the ability to control balance. Several studies have shown it to be related to the ability to perform functional tasks and the risk of falling. 8 The reach distance in forward reach did not differ significantly between the normal and hyperkyphotic subjects (P = 0.361); however, hyperkyphotic participants had a significantly smaller reach distance in the functional reach to the left and right than the normal individuals. The rigidity of spine in lateral bending might explain the significant difference.
Our other hypothesis was that the cowhorn outrigger might limit the forward functional reach. The findings supported out hypothesis as the reach distance in forward reach with brace was less than the value while not wearing the brace in hyperkyphotic subjects (Figure 3).
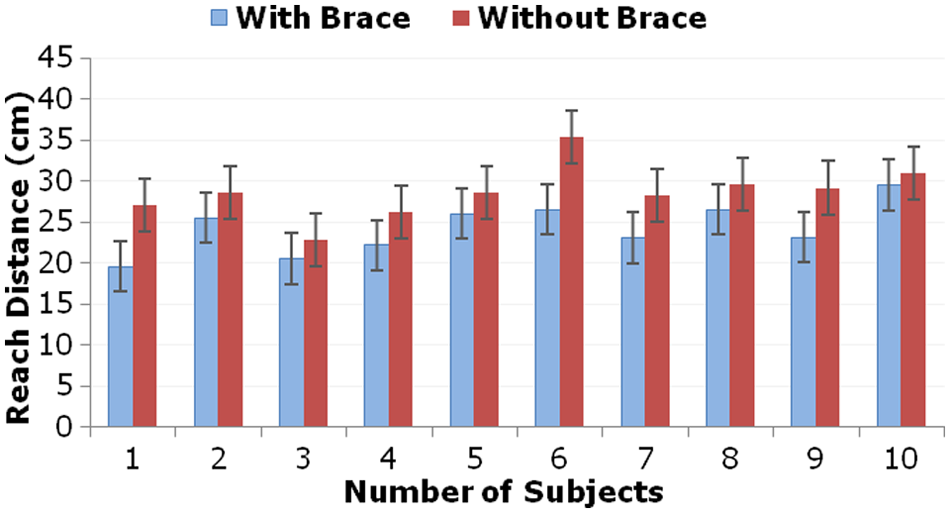
The maximum reach distance (RD) in functional forward reach for each of the hyperkyphotic subjects (n = 10) on the first day.
Long-term effect
While bracing had no immediate effect on stability in static and dynamic circumstances, after 120 days of brace wear the participants performed considerably better in balance tests compared to day 0, when they performed the tests without wearing the brace. The brace might compensate for balance disorder in patients with hyperkyphosis by its therapeutic effect, as the subjects not only performed better than day 0, but also the mean value of some of the balance parameters in right and left reach tended to be more similar to the values of the normal participants (Table 4).
The hyperkyphotic participants showed no significant difference in static and dynamic performance when performing with the brace compared to without. This is consistent with the findings of Sadeghi et al. 26 that brace had no effect on standing balance in schoolgirls with idiopathic scoliosis.
Proprioception has a significant role in standing stability as it permanently regulates the COP displacements. It is also claimed to improve while wearing a brace for musculoskeletal disorders. 36 Our findings do not support this statement as the performance of hyperkyphotic subjects was not significantly altered when they accomplished the tests with the brace compared to without.
After 120 days, the reach distances (forward, right and left) without brace in hyperkyphotic subjects were higher than the first day, but were not significantly different from the values of the normal participants (P > 0.05). It was mainly seen in COP and reach distance variables during the functional reach to right and left. Thus, it might be concluded that the brace may cause the improvement of balance function in the long term. That is what Adler et al. 34 and Chow et al. 22 called therapeutic and training effect, respectively. The participants could reach the object in dynamic reach tests without brace with higher displacement in sagittal plane after 120 days, without losing their balance (taking a step or bringing their foot up the floor).
A limitation of our study was that we could not obtain the real-time kinematic data of subjects during walking. Also, since gender differences have been found in balance control measurements, 37 the results cannot be generalized to the male hyperkyphotic patients. The interpretations are limited to the comparisons between the small sample of the hyperkyphotic and normal participants of this study.
Further longitudinal prospective studies with larger sample size and in various time intervals would be helpful to discover the long-term effect of bracing on balance function. Future research needs to be carried out to examine the effect of bracing on dynamic balance of hyperkyphotic subjects during walking and other functional tasks. Furthermore, we only included Milwaukee brace in our study. Effects of other low-profile brace types are also needed to be investigated.
Conclusions
Overall, the results of this study showed that bracing had no immediate effect on the performance of hyperkyphotic subjects in static balance tests. Bracing might result in enhanced balance in the long term. It is hoped that the study provided some new insights into the conservative treatment of hyperkyphosis for clinicians and researchers.
Footnotes
Acknowledgements
Kind assistance of Mr Atshani and Safayi at Payvand Orthotics & Prosthetics Center is appreciated. The authors wish to extend their gratitude to Mrs Seyed Mohseni at the Biomechanics Laboratory of Tehran University of Medical Sciences. Special thanks go to J Martin Carlson, CPO, FAAOP whose invaluable experience in the field was incredibly helpful to our work.
Funding
The financial support of Tehran University of Medical Sciences is gratefully acknowledged.
Conflict of interest
The authors have no conflict of interest.