
Abstract
Background:
The Hawthorne effect, a subcategory of reactivity, causes human behavior to change when under observation. Such an effect may apply to gait variation of persons with prosthetics or orthotics devices.
Objectives:
This study investigated whether the presence of observers directly affects the gait pattern of users of lower limb prostheses.
Study design:
Within-subject intervention study.
Methods:
Primary outcome measures were gait parameters of initial double support time and upper body lateral tilt angle, which were collected with a mobile sensor attached to the subjects’ back. To make subjects feel unwatched, a certain amount of deception was necessary, and two different conditions were created and statistically compared against each other: one in which the subjects were initially unaware of the attention of observers and another one in which the same subjects were aware of a group of observers.
Results:
Data from two subjects using trans-femoral prosthesis are reported. Findings included a change in step initial double support percentage by up to 14.2% (p = 0.019). Considerable changes were also noted in secondary outcome measures including speed, stride length, and stride symmetry.
Conclusions:
A reactivity effect of observation exists in prosthetics gait analysis. More comprehensive studies may be motivated by these preliminary findings.
Clinical relevance
Results of this study suggest that users of lower limb prostheses walk differently when their gait is being assessed (e.g. in the prosthetist’s office) than in situations without observers. This may in part explain the clinical experience that modifications of prosthetic fit or alignment provide only short-term betterment.
Keywords
Background
The aim of this research was to investigate possible limitations of the current process of gait analysis in prosthetics and orthotics (P&O). Previous research has challenged the assumption that the gait that is assessed in the laboratory or office is identical to the gait in real-life environments. 1 This poses the risk that any interventions with respect to prosthetics alignment and adjustment that are based on gait assessments during a fitting session are less effective in real life than they could be.
Prosthetic alignment optimization is generally based on the analysis of a patient’s gait by the prosthetist, which may be aided by instrumentation (e.g. force plates and motion capture systems) and by subjective feedback provided by the patient. The interpretation of this information is guided by the professional training and experience of the prosthetist who pursues the goal of reducing gait inefficiencies, asymmetries, and instabilities. Objectifiable measures of alignment quality, such as the roll-over-shape method, 2 have been proposed to improve this process. However, irrespective of which particular method is being utilized, the patient’s gait will always be assessed in a laboratory environment while the patient is aware of the observation.
Several of the differences between laboratory environments and real-life environments have the potential to cause differences in prosthesis gait when walking in these environments. They include differences in surface smoothness, lighting, distracting stimuli, and subjects’ exertion. 3 This pilot study explores the hypothesis that the presence of dedicated observers causes prosthesis users to walk differently in their daily lives than they do during prosthesis fitting sessions.
The Hawthorne Effect, a psychological phenomenon under the umbrella concept of reactivity, states that people will act differently when they are aware of being observed. 4 The hypothesized presence of a reactivity effect in the context of rehabilitation technology would imply that prosthesis users aware of observers may not walk their habitual stride. 5 Expecting, or even telling, subjects to “walk normally” may cause them to make an effort to attain what they perceive as “normal gait,” which could result in a pattern quite different from their actual normal gait. 6
No previous research on the reactivity effect on prosthetic gait could be identified. Past reactivity research in different populations, 7 however, supports the notion that a prosthetist’s or a scientist’s mere presence may affect a subject’s gait pattern. If this is the case, then current gait assessment in P&O could be less accurate than commonly assumed.
Methods
The study was approved by the University of Pittsburgh institutional review board after full board review, necessary because of the intentional deception of subjects. The risks of participation were considered acceptable, as subjects walked in their original prosthesis without modifications and the protocol did not require any activity that exceeded subject’s normal activities of daily life.
Three subjects were recruited for the pilot data collection here presented. Inclusion criteria were an age of 18 years or older, use of a trans-femoral prosthesis for at least 6 months prior to the data collection, 8 and the ability to walk without any assistance for the 30 minute duration of the experiment. Exclusion criteria were any medical conditions that would limit safe operation of the prostheses or that would prohibit proper attachment of the data collection equipment belt around the subject’s waist.
Data were collected for one subject at a time. A certain amount of deception was necessary 9 to conceal the real purpose of the experiment (Figure 1). Upon providing informed verbal consent to serve as a patient model for the testing of different gait assessment formats, subjects were asked to wear the mobile sensor and undergo a calibration procedure in one laboratory of the research facility. Subsequently, subjects were asked to walk down an empty hallway to another room for the testing session while study personnel stayed behind under a pretense. Traversing the hallway constituted the control condition, “A,” when subjects needed to feel that they were not being watched and that no data were being collected. Once a subject arrived in the second laboratory, the observed phase of data collection, condition “B,” commenced.
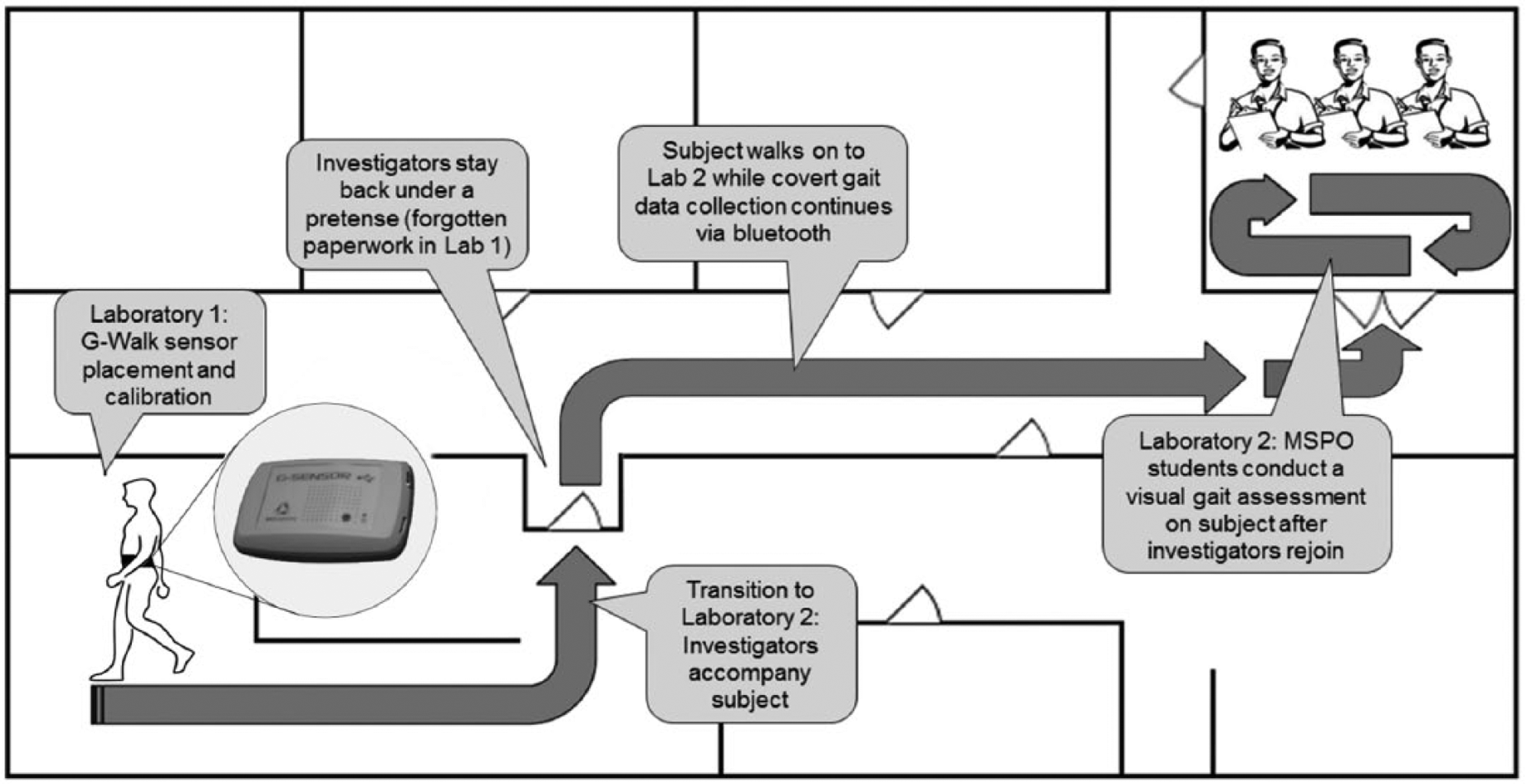
Illustration of the data collection protocol with deception (adapted from the study by Malchow and Fiedler 5 ).
In condition A, subjects’ gait data were collected for a distance of approximately 10 m, limited to the range of the sensor’s Bluetooth connection. Condition B was a classroom containing several students of the institution’s P&O program who conducted a visual gait analysis on the subjects. Subjects walked an average of 350 m while in condition B. Unlike in condition A, where they were not given attention from any observers, the students were there to make the subjects feel scrutinized in condition B. For that purpose, every subject was asked to walk normally up and down the length of the room, allowing the students to observe their gait pattern and to complete standardized gait assessment forms based on their observations. Floor surfaces, lighting, and absence of handrails or other assistive technology were kept identical between conditions A and B.
Once segment B was completed, subjects were informed about the true purpose of the study, and were asked for permission to use the gait data that had continuously been collected throughout the session.
The equipment consisted of a mobile sensor that was able to collect spatial–temporal gait data even when subjects were out of sight of the investigators (G-Walk; BTS Bioengineering, Milano, Italy). The device contains three different sensors that provide data on gait cycle durations and several kinematic parameters. It was placed in a special waist belt that kept the sensor in place on the subject’s back. Data were transmitted to a laptop computer via Bluetooth connection.
Variables of initial double support time as a percentage of the gait cycle and upper body lateral tilt angles were compared across conditions. These two factors have been used previously to determine a difference in gait pattern.10,11
In post-processing, step data were manually sequenced and the variables of body sway and initial double support time were compared across conditions by independent samples t-test, using statistical software (IBM SPSS Statistics for Windows, Version 21.0; IBM Corp., Armonk, NY). A critical alpha of 0.05 was defined prior to analysis.
Results
Three participants were recruited for this pilot data collection, of which two completed the protocol. Technical difficulties with the Bluetooth connection during data collection on the third subject prevented a proper transmission of the G-Walk data. The nature of the experiment disallowed for a repetition of the data collection with the same subject after the issue was recognized, as the necessary deception could not be replicated. Consequently, only data from two participants could be used for analysis (Table 1).
Subject information.

Samples of between 5 and 10 steps per condition were statistically compared within every subject. In either case, initial double support percentages were less symmetrical in the control trial than the observed condition (Table 2).
Initial double support percentages during unobserved (A) and observed (B) gait of trans-femoral prosthesis users.
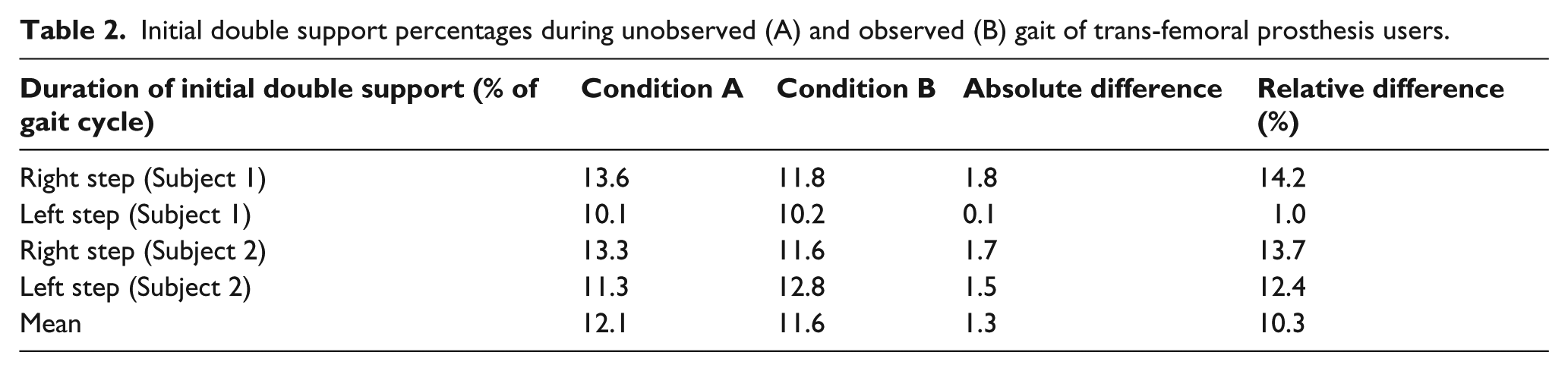
In both subjects, initial double support duration as a percentage of the gait cycle decreased substantially between conditions A and B for the right (prosthesis) step. The same variable increased for the left (sound leg) step in Subject 2, but remained essentially unchanged in Subject 1. Differences between conditions for this variable were significant (p = 0.019) for the respective right-legged steps, whereas the differences for the left-legged steps were less pronounced (p = 0.160). Average differences in initial double support duration across conditions were not significant at the 0.05 threshold.
Condition A produced an average lateral tilt angle of 4.9° while condition B produced an angle of 5.5° over the sampled steps. Only average values across the entire step samples were available as output for the tilt angle; therefore statistical comparison was not possible.
Secondary outcome measures of speed, stride length, and stride symmetry were also collected (Table 3). Differences in average stride length did not prove to be significant, although the right leg stride length showed a notable difference of 7.4% between the two conditions. Self-selected walking speed increased to 1.07 m/s in condition B from 1.01 m/s in condition A.
Secondary gait variables during unobserved (A) and observed (B) gait of trans-femoral prosthesis users. Differences are not significant at the 0.05 level.

Discussion
The analysis of gait parameters shows that there is a significant difference between the two investigated conditions. This provides evidence that subjects were affected by the observers’ attention, and thus confirms the study hypothesis. Every studied variable changed a noticeable amount from the control to the observed trial. The prosthesis side stride especially showed a shorter percentage of time in initial double support. This could mean that any limping was less pronounced in the presence of observers. The baseline (unobserved condition) initial double support times were much less symmetric between legs when compared to the observed condition.
Even though not part of the investigated hypothesis, other variables collected by the G-Walk sensor were analyzed to inform possible subsequent studies. The observed differences in gait speed and stride length may be of clinical significance as they are closely correlated to prosthesis fit, alignment, and adjustment.
Generally, it appears likely that many of the measurable gait variables are correlated. A change in gait speed may have an impact on stride lengths, trunk tilt, inter-leg symmetry, and other parameters. However, the exact mechanisms that lead to the eventually assessed changes are of minor consequence for the purposes of this investigation; as long as prosthesis gait is affected by observation, laboratory-based gait assessments and alignment changes are limited in their applicability to authentic user environments.
Our findings are in line with previously reported results of reactivity studies in different populations.12,13 It should be noted that the prosthetic limb potentially contributed to the expected effect in different ways. Use of a prosthesis could possibly induce feelings of insecurity and reduce feelings of self-affirmation, which has been shown to increase reactive behavior. 14 It is important to consider that reactivity effects may be different in able-bodied subjects and in users of limb prostheses.
The utilized protocol was based on the assumption that subjects do not believe that data are being collected as they make their way through the empty hallway. This assumption may have been violated as one subject mentioned during the debriefing that he had become suspicious when he was fitted with the sensor in a different room than the testing room.
Another limitation of the study was that steps in the control trial (A) were not independent of each other. When walking continuously, one step will to some extent affect the next consecutive one. The hallway was too short to produce enough data for a random step selection in condition A. Instead, all available consecutive strides were analyzed for this condition. While this is a violation of the assumption of independence of the sample, it may be argued that data from several steps are still preferable over a single data point. Furthermore, it has been argued that “paired samples t-test is an appropriate statistical analysis as long as the pairs of observations are independent” in cases of non-independence of a sample. 15 Steps recorded during condition B were sampled randomly from the collected data that were more extensive than in condition A. For future studies, it is recommended to devise a protocol that allows the collection of a larger step sample in the unobserved condition, for instance, by means of mobile data logger equipment.
Even though an effort was made to control for environmental variables, such as flooring and lighting between interventions, the circumstance that data were collected in two different sites (the hallway and the classroom) may have affected subjects’ gait beyond the effects of observation. This limitation is not expected to diminish clinical significance, however, as prosthesis users generally spend most of their time ambulating in different environments than the prosthetist’s office where the gait assessment takes place.
Conclusion
Users of lower limb prostheses evidently appear affected by the presence of observers analyzing their walking pattern. The results of this pilot study provide some indication that clinical gait analysis procedures in P&O have an undesirable effect on the walking pattern of prosthesis users. The clinical significance of such an effect is that it could lead to the misalignment and maladjustment of lower limb prostheses. Results also seem to support the occasionally reported clinical finding that users of newly fitted artificial legs often demand additional alignment optimization after having used the device in their own habitat (and unaffected by observation), even though their gait pattern appears satisfactory in the prosthetist’s office.
Based on the preliminary results of this research, further work should investigate the reactivity effect of observation on other gait variables. The magnitude and quality of the effects found should be confirmed by an expanded study with more subjects in a true clinical setting.
Footnotes
Acknowledgements
The authors thank Judith Navratil for her advice on the study design and the students of PITT MSPO class of 2015 for their help with data collection.
Author contribution
Study design, data collection, processing, analysis, literature review, and manuscript draft—Connor Malchow.
Study design, supervision, subject recruitment, institutional review board (IRB) oversight, manuscript revision, and editing—Goeran Fiedler.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this research was supported by ASPIRE grant no. 1262670 and VA Center grant no. B6789C.