
Abstract
Background:
Mortality after amputation is known to be extremely high and is associated with a number of patient features. We wished to calculate this mortality after first-time lower-limb amputation and investigate whether any population or treatment factors are associated with worse mortality.
Objective:
To follow up individuals after lower limb amputation and ascertain the mortality rate as well as population or treatment features associated with mortality.
Study design:
A prospective cohort study.
Methods:
Prospective lower-limb amputations over 1 year (N = 105) at a Regional Rehabilitation Centre were followed up for 3 years.
Results:
After 3 years, 35 individuals in the cohort had died, representing a mortality of 33%. On initial univariate analysis, those who died were more likely to have diabetes mellitus (χ2 = 7.16, df = 1, p = 0.007) and less likely to have been fitted with a prosthesis (χ2 = 5.84, df = 1, p = 0.016). There was no association with age, gender, level of amputation, social isolation, significant medical co-morbidity other than diabetes or presence of mood disorders. A multi-variable logistic regression (backward step) confirmed that diabetes (odds ratio = 3.04, confidence intervals = 1.25–7.40, p = 0.014) and absence of prosthesis-fitting (odds ratio = 2.60, confidence interval = 1.16–6.25, p = 0.028) were independent predictors of mortality.
Conclusion:
Mortality after amputation is extremely high and is increased in individuals with diabetes or in those who are not fitted with a prosthesis after amputation.
Clinical relevance
The link between diabetes and mortality after amputation has been noted by others, but this is the first study to find an effect from prosthetic limb-wearing. This requires further investigation to ascertain why the wearing of a prosthetic limb, confers an independent survival benefit that is not related to the presence of medical co-morbidity.
Background
Lower-limb amputations remain an important cause of long-term impairment and dependency. The subsequent mortality rate is extremely high but varies considerably in the literature between 39% and 68% at 5 years.1–13 This wide range of rates may reflect the difficulties in study designs as well as the use of retrospective or cross-sectional analyses which dominate the literature.
We wished to estimate this mortality rate in a cohort after lower limb amputation who attended a prosthetic rehabilitation centre. Most previous studies have been based in surgical centres and have therefore examined outcome from a surgical perspective. These studies often focus on peri-operative deaths and short-term mortality, and there is a real dearth of high-quality studies in this area based at prosthetic rehabilitation services incorporating long-term outcomes. All amputations in our region are carried out at one hospital, and all of these individuals are then transferred to the rehabilitation ward post-operatively ensuring that we have a complete, unselected population to follow-up over time from a prosthetic perspective.
Besides overall mortality, our other aim was to identify any features that may be associated with a worse outcome. A large number of demographic and treatment features have been studied after amputation, but there is still considerable disagreement as to the features that affect outcome, for example, diabetes mellitus. In general, it is acknowledged that diabetes increases vascular risk9,11,14 and most studies have indeed shown a higher mortality after amputation in individuals with diabetes.2,3,7,9 However, some have found little or no difference.1,6,12
Apart from diabetes mellitus, the other features that we wished to examine were gender, level of amputation, presence of significant medical co-morbidities, social isolation, psychological symptoms, age and prosthetic limb-fitting.
It had been observed by ourselves that patients who are fitted with a prosthetic limb often seem to fare better than those who are not. However, this may simply be attributed as a surrogate marker for the presence of medical co-morbidities. Prostheses are usually issued after the multi-disciplinary team makes an overall judgement in terms of suitability for limb-fitting based on patient goals achieved in physiotherapy and overall patient frailty. However, there is no certainty in terms of exact relationship with limb-fitting and so we decided to study this feature in the model.
Psychological symptoms are extremely common after amputation,15,16 but it is unsure as to whether there is any impact on long-term mortality. Therefore, this was also included in the study.
It is hoped that by identifying factors associated with long-term outcome, we may allow a better understanding of the condition, target any modifiable factors in high-risk patients or better allocate sparse resources in the future.
Methods
We studied admissions over a 12-month period, to a rehabilitation ward at a regional prosthetic centre after lower limb amputation. All amputations in the region (population over 1.5 million) are carried out at one surgical centre, and all of these individuals are then transferred to the rehabilitation ward within a few days for their care and discharge. Only peri-operative deaths are excluded from this population, which therefore represents the entire regional population of amputation survivors over a year. The majority of amputations are carried out for dysvascular disease with a small number of cases from trauma or oncological aetiologies. Only major lower limb amputations were considered; this is defined as amputations proximal to the ankle joint. The exclusions were lower limb amputations below the ankle or upper limb amputations and any re-amputations, for example, transtibial amputations (TTAs) converted to transfemoral.
Post-operatively, all patients have a short in-patient stay to start physiotherapy, wound-healing and arrange for discharge care. At this time, patients suitable for prosthetic limb-fitting are selected by a multi-disciplinary team approach. The team is guided by progress the individual has made in physiotherapy, safety considerations and individual patient goals. Most patients are fitted with a limb, and in general, only very frail and unsafe patients would not receive a limb. After a short in-patient stay for rehabilitation, patients were discharged after suitable modification of environment and care input. After discharge, patients were followed up by prosthetists and medical and therapy staff as was appropriate for their case. Some patients may need adjustments to the new limb or further physiotherapy sessions; others may receive only a medical follow-up to check on progress or any new problems.
The presence of significant co-morbidities was defined by the Charlson Index, which was calculated using clinical records at discharge. This has been shown to be a good predictor for significant co-morbidities and long-term outcome. 17
Social isolation was assessed by the short version of the Revised UCLA Scale. 18 This tool effectively identifies those most isolated in the community.
Psychological symptoms after amputation were evaluated by using the Hospital Anxiety and Depression Scale (HADS), which is a short questionnaire validated for assessing anxiety and depression symptoms with recommended cut-offs (score > 8) as significant. 19 These were all administered within a week of amputation.
After 3 years, all patients were followed up by detailed medical interview by the lead investigator. Using hospital records and phone calls to general practitioners, it was possible to trace all patients in the original cohort and to ascertain survival. If patients could not travel to an appointment, they were visited at their home.
Initial univariate analysis using χ2 test or t-test was used to investigate association between mortality and other factors of interest. Subsequent multi-variable logistic regression with backward step entry was applied; starting with a full model of all variables, we used a stepwise analysis to remove non-significant variables one at a time to determine the independent predictors of survival at 3 years. The criteria for entry or removal of a variable were 5% for inclusion and 5% for exclusion. All analyses were performed using SPSS version 16.0. Local Ethics Committee approval for the study was obtained for the follow-up interviews.
Results
Over a 12-month period, there were 116 admissions direct from surgical wards with primary amputation. In total, 11 of these were upper limb and forefoot amputations who were excluded. The remaining 105 were all major lower limb amputations of whom 70 were alive, on average 3.1 (standard deviation (SD) = 0.15) years after their operation. All 70 of these individuals were traced and interviewed. The mean age at amputation was 62.6 (SD = 14.6) years and median age was 66 (range = 25–91). In total, 43 amputations (41%) were transfemoral and the rest were transtibial. There were no bilateral amputations. Over the study period, four (3.8%) individuals had further amputations, three converting to transfemoral amputation (TFA) and one requiring a contralateral TTA. In terms of aetiology of amputation, 33 (31.4%) had diabetes mellitus (of whom 24 had peripheral vascular disease), 60 (57.1%) had peripheral vascular disease without diabetes, 8 (7.6%) were traumatic limb loss and 4 (3.8%) had limb loss as a result of bone tumours. Using the Charlson Index to define co-morbidities, we found that 61 (58%) fell into the higher co-morbidity group (using a cut-off > 2). In terms of initial fitting with a prosthetic limb, 65 (64%) were fitted. No further attempt was made to quantify or grade the extent of prosthesis use. Initial level of psychological symptoms using the HADS was 26 (25%) for anxiety and 28 (27%) for depression.
Differences between the surviving and non-surviving groups are shown in Table 1. On univariate analysis, we found that increased mortality was associated with diabetes (χ2 = 7.16, p = 0.007) and absence of initial prosthetic limb-fitting (χ2 = 5.84, p = 0.016). There were no differences between the two groups in terms of age, gender, social isolation, medical co-morbidities, level of amputation or presence of anxiety or depressive symptoms.
Differences between groups for survivors and deaths.
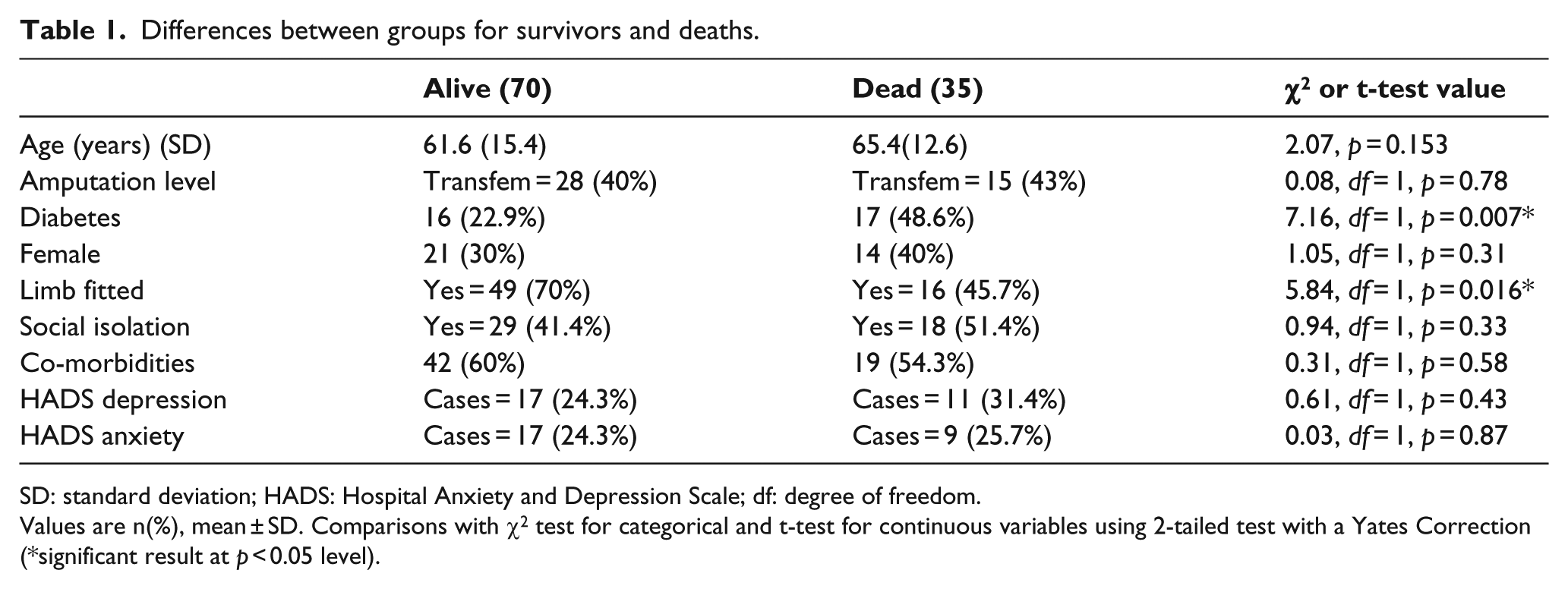
SD: standard deviation; HADS: Hospital Anxiety and Depression Scale; df: degree of freedom.
Values are n(%), mean ± SD. Comparisons with χ2 test for categorical and t-test for continuous variables using 2-tailed test with a Yates Correction (*significant result at p < 0.05 level).
Further analysis of mortality was carried out with a multi-variable logistic regression technique (backward selection). This confirmed that diabetes (odds ratio (OR) = 3.04, confidence intervals (CIs) = 1.25–7.40, p = 0.014) and absence of initial limb-fitting (OR = 2.60, CI = 1.1–6.25, p = 0.028) were independent predictors. For this analysis, limb-fitting was converted to absence of limb-fitting to make sense of the OR as limb-fitting was found to have a protective effect compared to diabetes (Table 2). Therefore, the independent predictors of mortality at 3 years are diabetes and absence of prosthetic limb-fitting.
Logistic regression analysis (backward) of mortality and clinical features after amputation.
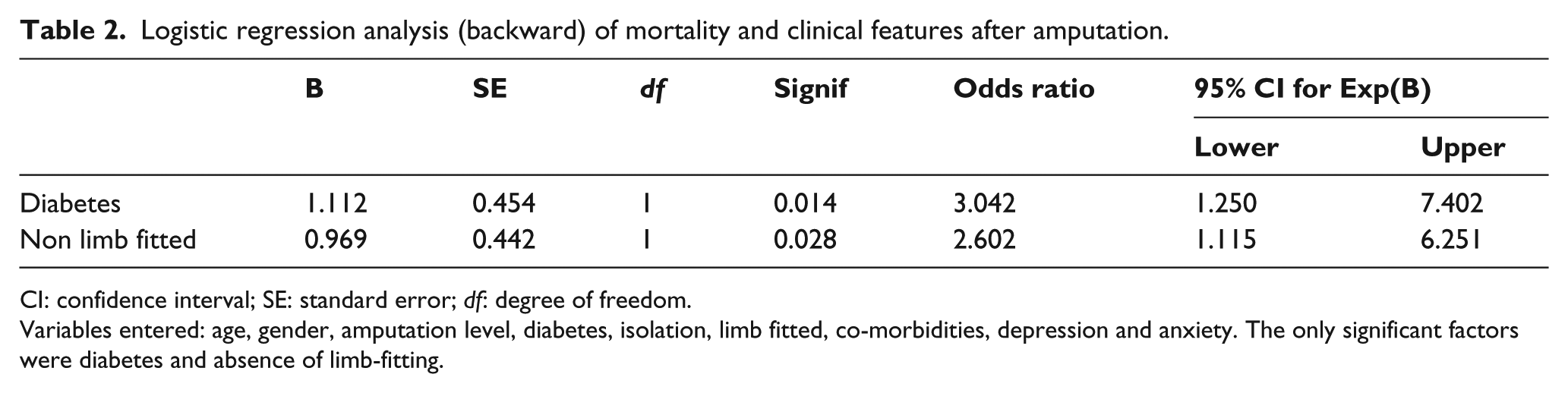
CI: confidence interval; SE: standard error; df: degree of freedom.
Variables entered: age, gender, amputation level, diabetes, isolation, limb fitted, co-morbidities, depression and anxiety. The only significant factors were diabetes and absence of limb-fitting.
Discussion
A high mortality rate after lower limb amputation is well recognised with studies reporting from 39% to 68% mortality at 5 years.1–13 These are predominantly from surgical units which include a substantial number of peri-operative deaths. Our study differs from these in that we have looked at a population after amputation who have then been referred to rehabilitation services. Our overall mortality rate was 33% at 3 years. In individuals with diabetes the mortality was 52%. Effectively, the study excluded patients who constituted peri-operative deaths which explains why the rate is at the lower end of previously published work. It is interesting that this rate is similar to a recent large retrospective study in a similar rehabilitation population attending a prosthetic service. 3 This would suggest some similarity across two similar population groups. In general, the problem that affects many other studies is that they look at single disease groups, for example, diabetes or trauma. We have tried to look at a generalised population typical of a regional rehabilitation centre with the aim of making observations that could guide practice or even target therapy. Our region has a population of 1.5 million, and this is the only regional prosthetic centre that individuals can access. Therefore, we are confident that we have a complete and valid study group from which to make conclusions particularly with regard to prosthetic practice.
From the results of recent studies including our own, compared to those some 20 years ago,1,20,21 it is possible to discern a change in the overall mortality rate associated with amputations. Larger population based studies using comprehensive disease registers have also shown a decreasing rate of amputation as well as decreased mortality thereafter.8,9,22–24 It is possible to speculate that strategies of earlier vascular intervention including radiology, better control of cardiovascular risk factors such as diabetes and lipids, good amputee rehabilitation management, smoking cessation and overall prevention strategies may be impacting on the progression of disease and the overall mortality.
We have found that diabetes was an independent predictor of mortality. Lower limb complications are a major source of morbidity in individuals with diabetes. Although reduction of amputations is often cited as an objective, 25 patients still have a high risk of complications and death compared to non-diabetics.9,11 Several studies have compared individuals with and without diabetes after amputation; the majority suggest that it is indeed a significant factor in outcome.2–5,7,9,11 However, the literature is confounded by a number of studies that have shown that diabetes may decrease the initial peri-operative mortality. 1 Others have found no long-term effect on mortality from diabetes.6,12,26–28,41 A large retrospective rehabilitation study found that individuals with diabetes had a higher rate of readmissions, re-amputation and costs associated with their care but no difference in mortality. 10
There is therefore still some uncertainty, although the bulk of studies find that diabetes worsens outlook. In our study, it was the single largest significant factor in mortality after amputation.
Apart from the presence of diabetes, we found that initial prosthetic limb-fitting was an independent predictor of mortality. The multi-variable analysis slightly attenuated the effect on mortality, but it was still highly significant. Unfortunately, we did not have a measure of the extent of functional limb use after 3 years. This may have allowed further evaluation of the possible protective effect of limb use on outcome.
The protective effect of initial limb-fitting has been noted previously in our centre and was explained as a surrogate measure of medical co-morbidities and general patient frailty. This would then result in the multi-disciplinary team deciding that patients were too frail to be fitted. However, these results have found that co-morbidities were not significant so that this explanation is not tenable. It is possible that the process of selecting patients for limb-fitting is more robust and effective than systems we have designed for picking up medical co-morbidities. Dillingham found that individuals receiving in-patient-based rehabilitation had better survival compared to community rehabilitation, 29 and others have shown that early rehabilitation improves functional outcome. 30 Hence, initial limb-fitting may be a marker for non-biological factors affecting the quantum of rehabilitation and attention received. It is possible that encouraging patients by limb-fitting, results in better mobility and health. Non-fitted patients may find it harder to get to clinics or their general practitioner. Alternatively, an individual’s coping skills may be adversely affected. All of these could affect mortality. This area is worthy of further research, and we know of no other studies that have looked at limb-fitting and mortality. Why should it confer an independent benefit for survival after correction for co-morbidities?
A number of studies have suggested that TTA cases have better survival than TFA cases.2,4–6,12,28 Only one study found the reverse with a poorer survival for TTA cases. 3 However, we did not find any difference as did two other studies.1,31 We would suggest that irrespective of the level, any amputation is a manifestation of a multi-system problem; the cardiovascular risk for any individual is clearly elevated as the amputation is a reflection of systemic atherosclerosis going on throughout the vasculature. Indeed, some studies of minor amputation (e.g. metatarsal) have similarly high mortality rates of up to 60% at 5 years which is comparable to that associated with major amputation.32–35 This may explain why we see no difference between levels of amputation as all patients carry a high risk.
We also found no effect of gender. Most studies likewise find no effect but a few have found that women have worse functional and survival outcomes than men.1,13,28,36 One study, however, was in a population of American Indians and another in Chinese ethnicity with diabetes; these may not be relevant to generalised practice.28,36 Others have found that the drop in amputation rates over recent years has been most noted in women for reasons yet to be explained. 22
It was surprising that we found no association between mortality and presence of significant medical co-morbidities excluding diabetes. We used a validated system that should be able to identify significant co-morbidity risk apart from diabetes which we wanted to examine separately. 17 Clearly, the addition of diabetes which was an independent predictor of mortality would have changed this association. Other studies have looked at medical co-morbidities combined or at single conditions. One article found no association with vascular disease 28 while others have found that co-morbidities worsen mortality, although some of these studies were only in individuals with diabetes.5,6,12,32,37
Depression and anxiety are known to affect overall outcomes, especially in individuals with diabetes, albeit these are often studies in general patients without amputation. 38 It is known that anxiety and depressive symptoms are common in patients after amputation and can affect functional outcomes.15,16 But in this study, we have shown that the presence of such symptoms shortly after amputation did not affect long-term mortality. We are not aware of any other studies that have looked at this outcome.
It has been suggested that functional outcomes for patients can be affected by the amount of relative support that individuals receive or the social isolation that is felt. 39 We are not aware of any clear scale that can measure social isolation without very detailed questionnaires, and we have settled on the use of a short item form with three short questions to identify those who experience most isolation in their community. We accept the criticisms that a longer, more detailed questionnaire may better classify individuals, but it would have greatly prolonged our assessments and was not the main aim of our study. We found that social isolation did not predict mortality, and this is the first published report that we know of that has looked at this as a feature.
The main limitations of our study are that we do not know the exact cause of death, and therefore, we have looked at all-cause mortality. While cause-specific mortality would have allowed us to examine more specific questions, it is known that cardiovascular disease is the leading cause of death in patients with amputation and it seems reasonable to make this assumption.12,14 Most other studies also use all-cause mortality. The high attrition rate of the group means that it would be difficult to follow-up this population group for much longer as numbers will become insignificant for analysis other than an overall mortality rate.
The other significant limitation is the lack of a suitable measure of limb use after amputation. We have assessed prescription of the limb after amputation but not measured the extent of limb use. If it is possible that use of a limb has a protective effect for an individual, then use of a measure such as hours of limb wear would allow better discrimination of any benefit. The unit is carrying out a further study on extent of limb-wearing in terms of hours of limb wear and functional outcome but we did not have any such measures available here. At the same time, patient reported activity level is known to poorly correlate to actual physical activity and future studies should consider the use of activity meters or pedometers to measure true activity levels and limb use. 40
A mention should be made of the population group that we have studied. A balance has to be struck between using a select, disease specific group or a population that reflects usual clinical practice. We have used a mixed population from a surgical unit who were referred for rehabilitation rather than a specific population group. This population constitutes all amputation cases in the region over a 1-year period who survived operation and were then transferred out of the surgical unit. We feel that it therefore reflects actual clinical practice for those of us working in the field rather than just an idealised population for a study. We had initially hoped that we might be able to compare different aetiologies but we had too few trauma patients. A larger study may allow us to compare different aetiologies, for example, trauma and vascular amputations. In general, it is thought that individuals with traumatic amputations fare better, but other studies have found similar 1 year mortality for all three aetiologies, namely, vascular, trauma and bone tumours.
The main strength of our study is that it is a prospective cohort and most of the published studies consist of retrospective or cross-sectional analyses. Furthermore, most studies have a surgical perspective, whereas we have looked at a rehabilitation population after the initial peri-operative period. We hope that other studies from a rehabilitation perspective will follow. We have also been able to trace and follow-up all survivors from the cohort at 3 years, representing 100% follow-up and this is an important feature.
Ultimately, understanding the features that are associated with mortality is the only way to avoid amputation or to target rehabilitation interventions. The costs associated with amputation, rehabilitation, social care and the lost employment opportunities are extremely high. Furthermore, despite our best efforts in rehabilitation, quality of life for individuals still remains poor after amputation. We hope that with this and further studies, we will better understand the features associated with amputation such that we may target our interventions better or more appropriately.
Conclusion
Our study confirmed high mortality after amputation which was associated with diabetes and absence of limb-fitting. This is the first study to find that prosthetic limb-fitting has a significant independent effect on long-term mortality.
Footnotes
Author contribution
Rajiv Kumar Singh gathered data, carried out the study and wrote the bulk of the article. Guru Prasad assisted with data collection and analysis including statistical analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.