
Abstract
Background:
The majority of lower limb amputations are undertaken in people with peripheral arterial occlusive disease, and approximately 50% have diabetes. Quality of life is an important outcome in lower limb amputations; little is known about what influences it, and therefore how to improve it.
Objectives:
The aim of this systematic review was to identify the factors that influence quality of life after lower limb amputation for peripheral arterial occlusive disease.
Methods:
MEDLINE, EMBASE, CINAHL, PsycINFO, Web of Science and Cochrane databases were searched to identify articles that quantitatively measured quality of life in those with a lower limb amputation for peripheral arterial occlusive disease. Articles were quality assessed by two assessors, evidence tables summarised each article and a narrative synthesis was performed.
Study design:
Systematic review.
Results:
Twelve articles were included. Study designs and outcome measures used varied. Quality assessment scores ranged from 36% to 92%. The ability to walk successfully with a prosthesis had the greatest positive impact on quality of life. A trans-femoral amputation was negatively associated with quality of life due to increased difficulty in walking with a prosthesis. Other factors such as older age, being male, longer time since amputation, level of social support and presence of diabetes also negatively affected quality of life.
Conclusion:
Being able to walk with a prosthesis is of primary importance to improve quality of life for people with lower limb amputation due to peripheral arterial occlusive disease. To further understand and improve the quality of life of this population, there is a need for more prospective longitudinal studies, with a standardised outcome measure.
Clinical relevance
This is of clinical relevance to those who are involved in the rehabilitation of persons with lower limb amputations. Improved quality of life is associated with successful prosthetic use and focus should be directed toward achieving this.
Keywords
Background
Peripheral arterial occlusive disease (PAOD) affects approximately 20% of adults above the age of 55 years in Europe and Northern America 1 and is a manifestation of systemic atherosclerosis, most commonly within the lower extremities. 2 Approximately 6% of the UK population are living with diabetes which increases the risk of PAOD. 3 PAOD can cause pain from ischaemia and infection of the lower limb and can be treated with wound management, orthotics or limb salvaging surgery. 4 However, between 1% and 2% of those with the most severe form of PAOD will require a lower limb amputation (LLA). 1 Those with PAOD have limited mobility pre-amputation, attributable to the existence of co-morbidities such as ischaemic heart disease and cerebrovascular disease which often co-exist with PAOD. If diabetes is also present, many will have neuropathic, visual, renal and weight-related problems. 3
There are more than 6000 primary LLAs per annum in the United Kingdom and approximately 85% are due to PAOD.1,5 Those undergoing a LLA due to PAOD are generally above 65 years old, and approximately 50% will have multi-morbidities. 6 Life expectancy post LLA is only 2–5 years. 7 This is predominately due to a 6-fold increase in mortality from coronary artery disease. 8 It is therefore imperative that quality of life (QoL) post LLA is optimised to ensure that major surgery for PAOD is not a futile intervention.
Following LLA, the focus of rehabilitation is to optimise function, especially walking. 9 Despite this, approximately 60% of people following LLA will be wheelchair-bound which may impede their physical capability, independence and thus their QoL. 6
The surgical success of a LLA is often measured in terms of survival or receiving a prosthetic limb. 10 Approximately 40% of those who undergo a LLA receive a prosthetic limb. 6 Those who have a trans-tibial amputation (TTA) have a greater likelihood of walking with a prosthesis than those with a trans-femoral amputation (TFA) or through-knee amputation (TKA). 11 The energy expenditure required to walk with a prosthesis following TFA is higher due to the loss of the knee joint. 12 Consequently, only 26% of those with a TFA will receive a prosthesis, compared to 75% of those with a TTA. 6 Successful outcome following a LLA should take into account the person’s QoL, a concept which has become increasingly more important in rehabilitation. 13 QoL is defined as ‘an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns’. 14 There are no validated QoL outcome measures for those with a LLA; therefore, generic QoL outcome measures are used. These generic measures focus on the function/disability areas of the International Classification of Functioning and Disability Framework rather than the contextual factors such as the environment.
A person who has a LLA for dysvascular reasons has a poorer QoL compared to someone who has a LLA for other reasons such as trauma or tumour. 15 To maximise rehabilitation outcomes, an understanding of the factors that influence a person’s QoL following dysvascular LLA is essential for healthcare professionals. A previous literature review assessed QoL in those with a LLA for all aetiologies, including trauma, tumour, orthopaedic complications and dysvascular causes. 16 The majority of the 26 articles included had amputee populations of mixed aetiologies such as trauma or tumour (n = 16), did not distinguish between upper limb amputation and LLA (n = 2) and compared major LLAs to other surgeries (n = 2). 16 To date, no systematic review has been undertaken on QoL in those with LLA for PAOD. The aims of this systematic review were to report the QoL of those with a LLA due to PAOD and to identify the factors that influence QoL after a major LLA due to PAOD.
Methods
Search strategy
A systematic literature review was undertaken in December 2015 using EBSCO and OVID which searched MEDLINE, CINAHL, PubMed and PsycINFO databases. Web of Science and Cochrane databases were searched separately, and all literature published from database inception to the end of 2015 were included. The search strategy included specific keywords and combined Medical Search History (MeSH) headings which were exploded for greater depth, and the following terms were used: foot or feet, ‘lower limb’, knee, leg, amput*, ‘above knee’, ‘below knee’, ‘lower extremity stumps’, ‘limb absence’, ‘limb loss’, ‘limb removal’, ‘quality of life’, quality of life, ‘Peripheral Vascular Disease’, ‘peripheral arterial occlusive disease’, ‘diabetes mellitus’, ‘diabetes’, ‘DM’, ‘type II diabetes’, ‘Activities of daily living’, ‘Physical and Rehabilitation medicine’, ‘Rehabilitation Centres’, Rehabilitation, ‘Mobility Limitation’, ‘Phantom Limb’, ‘Phantom Pain’. The use of Boolean terms ‘AND’ and ‘OR’ enhanced the search. Citations of relevant articles were also reviewed for possible inclusion.
Inclusion/exclusion criteria
Articles were included if the entire amputee study population had a LLA due to PAOD, participants were 18 years old or above, the full-text article was published in English, had a sample of more than 10 participants, reported the results of one or more QoL outcome measures and was empirical research. Articles were excluded if they were case-studies, reviews, editorial opinions, testimonies, biography/interviews, books, progress reports, conference abstracts or posters, discussion papers, guidelines, discussed other people’s QoL, for example, a carer’s or family member’s rather than a patient’s QoL, and did not use an objective outcome measure which meant all qualitative studies were excluded. Also excluded were articles that were a development or validation of an outcome measure to assess QoL, if the populations studied were of mixed aetiology or if participants underwent an amputation for reasons other than PAOD.
The literature search produced 333 articles: 201 from OVID, 122 from EBSCO, 4 from Web of Science, 1 from Cochrane and 5 from reference lists. Two systematic reviews were identified, one was not relevant 17 and the other provided back referencing of articles to include. 16 Fifty-four duplicate articles were removed. The titles of 279 articles were screened initially by one reviewer (F.C.D.-S.) which resulted in 209 being excluded. Then, two reviewers (F.C.D.-S. and E.C.) examined the abstracts of the remaining 70 articles and excluded a further 58 articles. This resulted in 12 full-text articles for review and assessment (Figure 1).
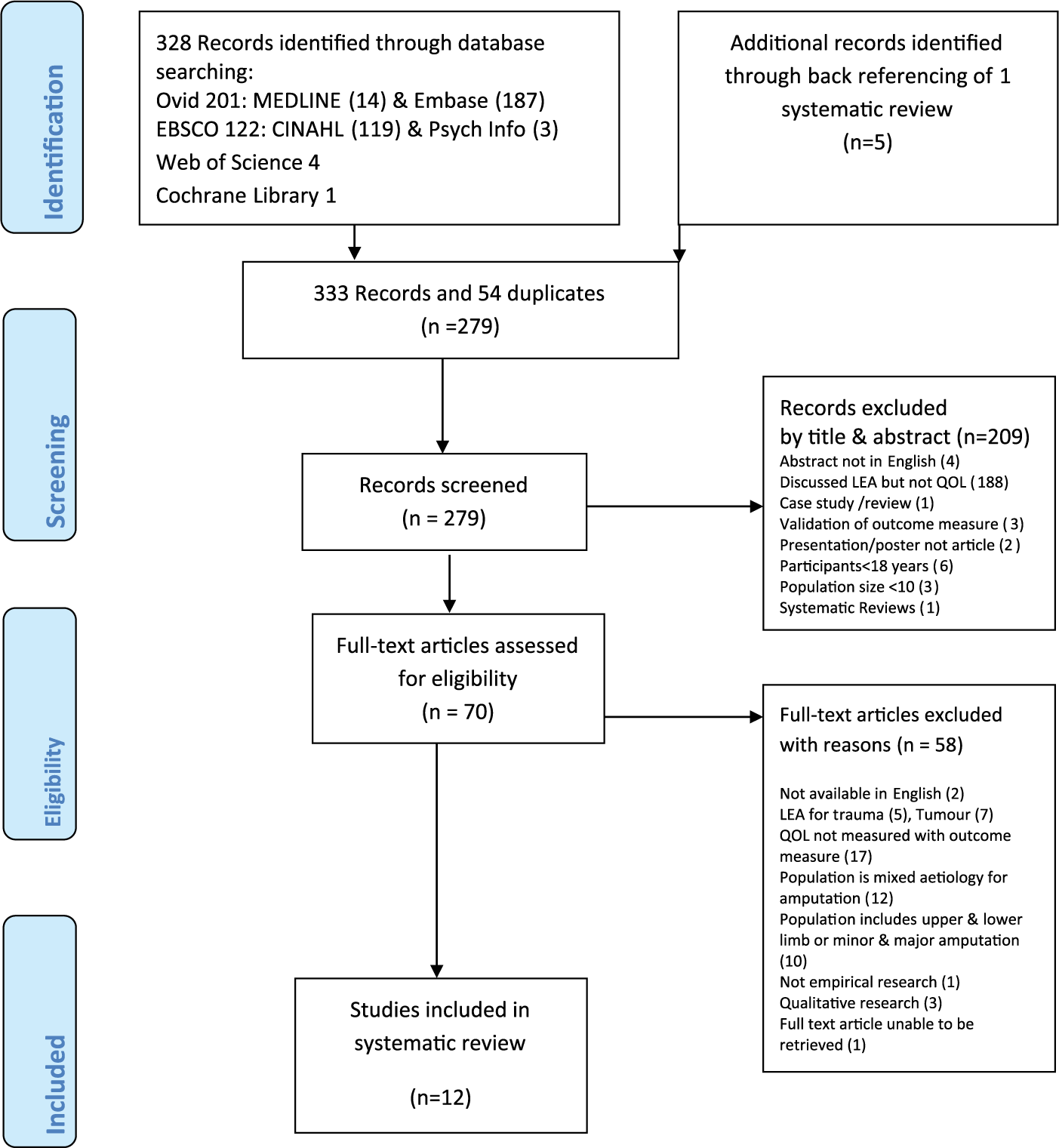
Schematic diagram of literature search when inclusion and exclusion criteria applied.
Quality assessment
The included articles were scored using a quality assessment tool with 19 criteria, adapted from a previous systematic review. 16 To bring the quality assessment in line with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, 18 one further criterion was added: evidence of limitations, creating a 20-criteria tool (Figure 2). 18 These additional criteria assessed whether the authors had accounted for potential bias and discussed any limitations of their research. The maximum quality assessment score was 38 points; this was based on three sub-categories: (1) the source population (11%), (2) study population characteristics (42%) and (3) methodological characteristics (47%). 16
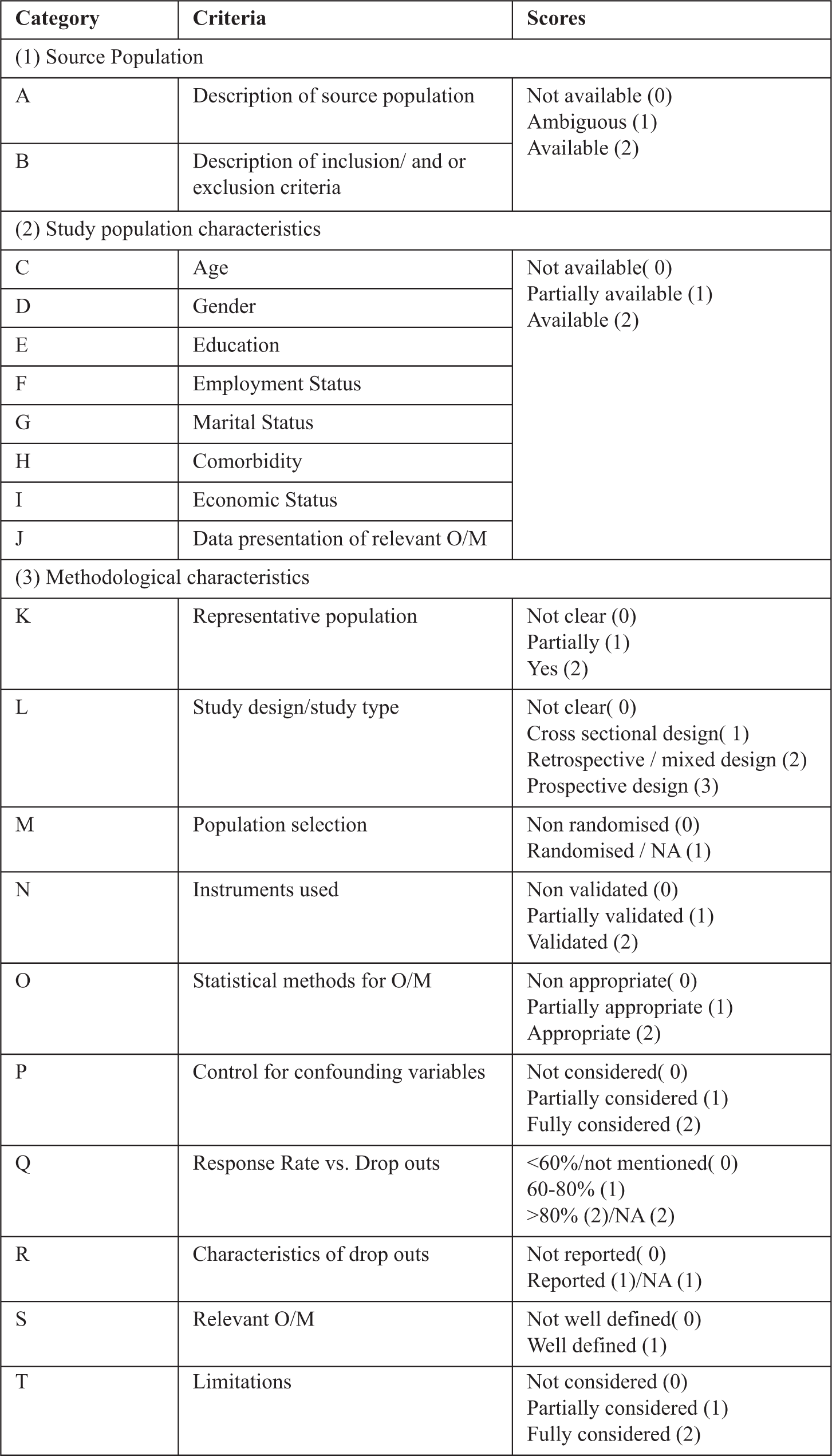
Quality assessment criteria and scores used to rate the articles.
Each article was independently scored by two of three assessors (F.C.D.-S., E.C. and L.P.), and when agreement could not be met, the third assessor was consulted to ensure consensus was reached. A pilot assessment was conducted where all three reviewers read one article independently and scored it, and then met to discuss the scoring and agreement was achieved. From this successful pilot, the remainder of the articles was scored with two assessors.
Results
The 12 studies that were eligible for inclusion are presented in Table 1. This highlights each study’s aims, population, QoL outcome measure and findings; these were grouped by methodological design (Table 1).
Evidence of literature.
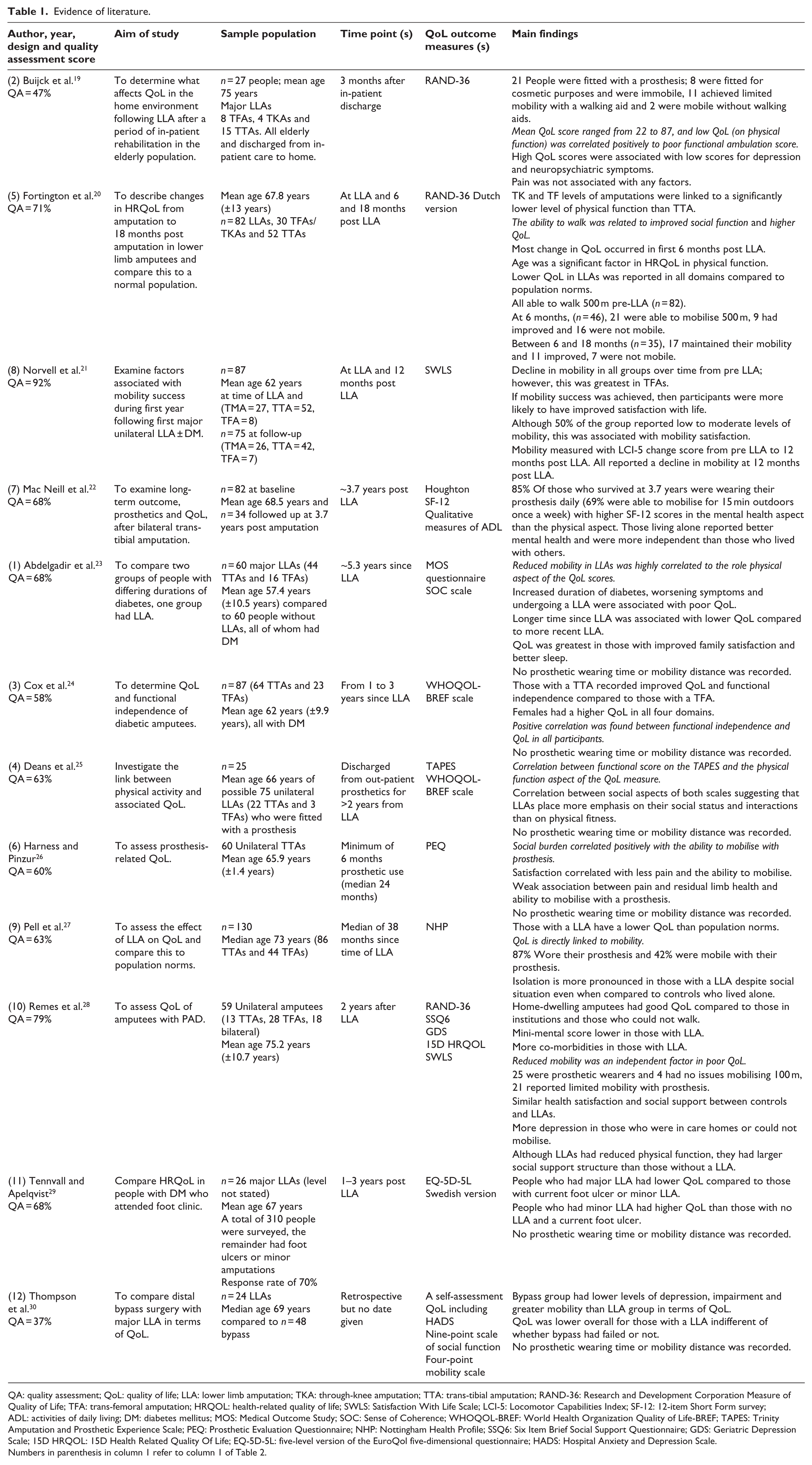
QA: quality assessment; QoL: quality of life; LLA: lower limb amputation; TKA: through-knee amputation; TTA: trans-tibial amputation; RAND-36: Research and Development Corporation Measure of Quality of Life; TFA: trans-femoral amputation; HRQOL: health-related quality of life; SWLS: Satisfaction With Life Scale; LCI-5: Locomotor Capabilities Index; SF-12: 12-item Short Form survey; ADL: activities of daily living; DM: diabetes mellitus; MOS: Medical Outcome Study; SOC: Sense of Coherence; WHOQOL-BREF: World Health Organization Quality of Life-BREF; TAPES: Trinity Amputation and Prosthetic Experience Scale; PEQ: Prosthetic Evaluation Questionnaire; NHP: Nottingham Health Profile; SSQ6: Six Item Brief Social Support Questionnaire; GDS: Geriatric Depression Scale; 15D HRQOL: 15D Health Related Quality Of Life; EQ-5D-5L: five-level version of the EuroQol five-dimensional questionnaire; HADS: Hospital Anxiety and Depression Scale.
Numbers in parenthesis in column 1 refer to column 1 of Table 2.
Scoring of quality assessment
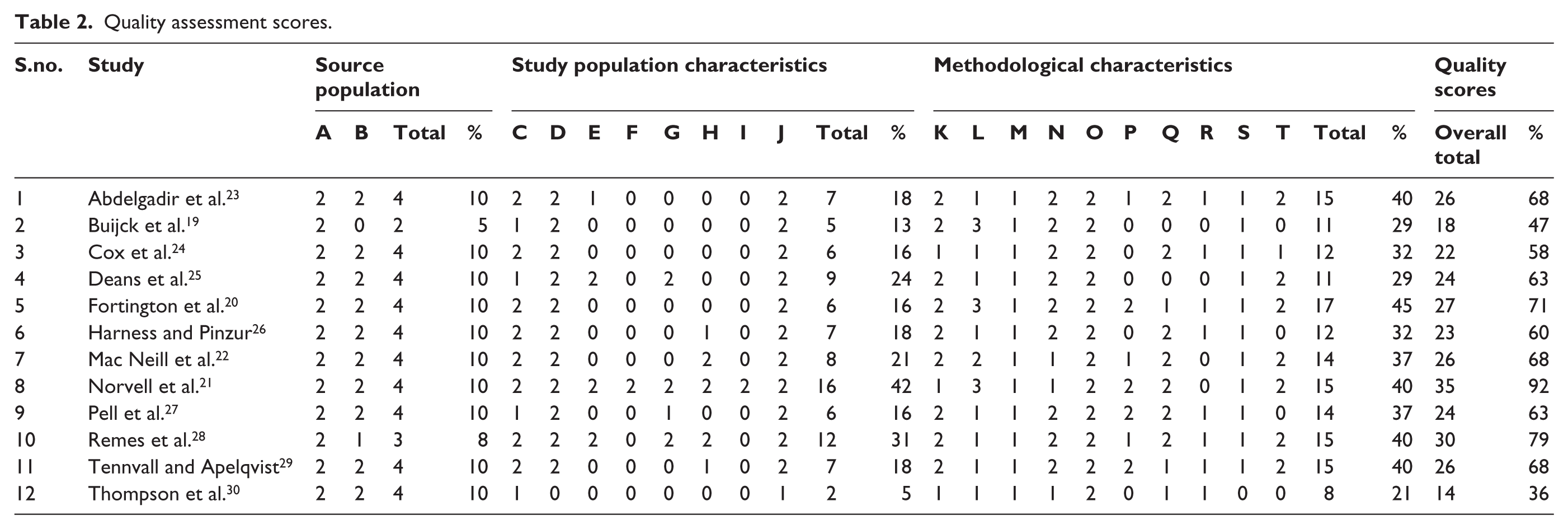
Quality assessment scores ranged from 36% to 92%. Reviewers reached agreement all final scores. The majority of the included articles were of good quality, with 10 of the 12 articles scoring more than 50%. Analysed by sub-categories, 10 of the 12 articles achieved the maximum score for source population; however, only 4 articles achieved a score more than 50% for study population characteristics. The methodological characteristics subcategory had higher quality scores, with the majority (11 of 12) scoring more than 60% (Table 2).
Quality assessment scores.
Sample populations
There was large variation in sample size, sampling techniques and comparator groups throughout the 12 studies. Sample sizes ranged from n = 24 30 to n = 130. 27 Sampling techniques included purposive,20–24,25,27–30 convenience19,22 and random sampling. 26 Comparison groups included age- and gender-matched controls,23,27,28 those with limb salvaging surgery 30 and those with foot ulcers. 29
Study designs
Study designs were cross-sectional (n = 8),23–30 prospective (n = 3)19–21 and mixed methods (n = 1). 22 The time points chosen to assess QoL ranged from 3 months after in-patient discharge 19 to 5.3 years after LLA. 23 The length of time between outcome measurements in prospective longitudinal studies also varied from date of LLA, 6 and 18 months post LLA 20 to 6 weeks and 12 months post LLA. 21
Outcome measures
A variety of generic QoL outcome measures were used across the studies: the Research and Development Corporation Measure of Quality of Life (RAND-36, n = 3);19,20,28 the World Health Organization Quality of Life scale (WHOQOL-BREF, n = 2);24,25 the 12-item Short Form survey (SF-12, n = 1) 22 and the five-level version of the EuroQol five-dimensional questionnaire (EQ-5D-5L, n = 1). 29 Although none of these measures has been validated for use with the LLA population, Sinha et al. 31 reported high internal consistency for the Short Form-36 (SF-36) in the LLA population. The same authors found a significant correlation between the Trinity Amputation and Prosthetic Experience Scale (TAPES) and the Physical and Mental component summaries of the SF-36 QoL measure in the LLA population. 31 The Prosthetic Evaluation Questionnaire (PEQ; n = 1) 26 is specific to those who have a prosthesis after LLA. Other scales such as the Satisfaction With Life Scale (SWLS; n = 2), 21 Sense of Coherence scale (n = 1), 23 Nottingham Health Profile (n = 1) 27 and a nine-point scale of social function (n = 1) 30 were also used.
Ten studies used a single measure to assess QoL,19–27,29 whereas one study used four separate measures. 28 Seven studies measured QoL alongside other factors such as physical function, depression, social support, prosthetic use and change in walking.19,21,22,24,25,28,30
Factors influencing QoL
Walking ability and use of prosthesis
Walking with a prosthesis was the most notable factor that influenced QoL and was reported by all 12 studies. The other factors that were identified that influenced QoL were gender, age, diabetes and family support (Table 2).
When comparing QoL of people after LLA to age- and gender-matched controls, after controlling for social isolation and emotional distress, the ability to walk was still found to significantly influence QoL.23,27 Norvell et al. 21 suggested that even small amounts of walking resulted in greater QoL compared to being unable to walk. In addition, Deans et al. 25 suggested that the association between QoL and walking was due to the positive influence of walking with a prosthesis on social interaction, rather than improving physical fitness.
Two cross-sectional studies compared those with a LLA to people with active foot ulcers 29 and bypass graft (limb salvaging surgery). 30 Both studies concluded that the QoL of those with a LLA was significantly poorer than those with active foot disease or surgery. Those who underwent a LLA had higher levels of depression and were less mobile than those who underwent a bypass graft. 30 Mobility was self-reported on a four-point scale and those with a LLA were significantly less mobile than those with revascularisation; however, no information about prosthetic use or distances covered was given. Although the results are as expected, this article was a retrospective study with a relatively small number of those with LLA (n = 26) compared to those with a bypass graft (n = 86), and the study’s quality assessment score was low (Table 2).
Level of LLA
Two studies of prospective design examined the effect of level of LLA on QoL,20,21 both achieving high-quality assessment scores (Table 2). Those with a TTA reported better QoL, compared to those with a TFA. 20 This was due to improved walking ability and thus greater social function in those who had a TTA. A decline in QoL and walking was observed over 12 months after LLA in all participants with LLA regardless of level; 20 however, this decline in QoL was greatest in those with a TFA. 21 In one study of people with unilateral TTA, a strong association was found between QoL and the ability to walk (n = 60); 26 however, all the sample received prosthetic rehabilitation and were therefore more likely to be mobile.
Age, co-morbidities and gender
There was a strong association between being above 65 years of age at the time of LLA and reduced ability to walk, which ultimately had a detrimental effect on QoL.20,21 With increasing age, there was a higher incidence of co-morbid disease 20 which may have affected QoL directly or indirectly through the influence of the co-morbid conditions on walking ability.
The presence of diabetes was associated with a lower QoL following LLA. Furthermore, the longer the duration of diabetes and its associated secondary complications, the poorer the QoL. 23 Other co-morbidities such as hypertension, alcohol dependence, anxiety and depression are reported to negatively influence QoL. 21 Two studies found that gender influences QoL with women having higher QoL following LLA,23,24 especially in those below 60 years old.
Social situation
Living at home and being to walk was positively associated with QoL. 28 Poor QoL and the presence of depressive symptoms were more prevalent in those living in a care home or in those who were wheelchair-bound within their home environment. 28 Mac Neill et al. 22 found that those who had bilateral TTAs and lived alone scored higher on the mental health aspect of QoL and higher on the activities of daily living on the Frenchay Activities Index, than those who lived with family. The authors also suggested that poorer QoL was attributed to social isolation, 24% of people were housebound; however, social isolation was reported to be present even if participants did not live alone. 27
Conclusion
The aims of this systematic review were to identify the factors that influence QoL after LLA for PAOD. Our findings show that the ability to walk with a prosthesis had the strongest influence on QoL. Many factors affect the ability to walk with a prosthesis such as level of LLA, co-morbid diseases, psychological motivation, living situation and social function. Although there is general agreement that those with a LLA have poorer QoL compared to their healthy peers, walking ability was the central influencing factor, which then determined the ability to live independently and participate in social activities which also impacted QoL.
Our review concurs with some of the findings of Sinha et al. 16 who also found that limited walking ability negatively influences QoL in those with a LLA. Furthermore, our review found that the ability to participate socially, perform activities of daily living and live independently influence the QoL of a person with a LLA due to PAOD. The age range of the populations studied in this review was from 56 to 75 years old. Of all the studies included in this review, only one study reported that QoL declined with increasing age, specifically above 65 years old. Our review is novel as it focuses solely on those who have a LLA due to PAOD as opposed to previous reviews which have examined heterogeneous groups of those with amputations. LLAs due to PAOD are the most common and have the greatest impact on health resources.
Factors such as advancing age and co-morbidities, notably diabetes, negatively influence the probability of successfully walking with a prosthesis and therefore QoL.20,21,23 The majority of those with a LLA due to PAOD are above 65 years old and approximately half will have diabetes. The presence of arterial disease in other organs adds to the co-morbid burden of this patient group, compounded by walking ability which may be impaired prior to LLA; 6 these factors reduce their life expectancy and ability to walk with a prosthesis. One solution to improving the QoL of non-prosthetic users may be extending rehabilitation and integration with prosthetic users to allow for improvements in morale and social integration. 27 QoL was greater in those with a TTA compared to a TFA. Those with distal amputations, for example, TTA, are more likely to have successful prosthetic management, less likely to need walking aids and more likely to engage in meaningful vocational and social activities. 11 Hagberg et al. 12 concluded that those with a TFA had poorer QoL, than those with a TTA, as they required a higher level of energy expenditure to walk, due to the loss of the knee joint. In addition, it is possible that lower mood and higher psychological burden may reduce the inclination to participate in rehabilitation which lowers the successful use of a prosthesis.
Two studies in this review examined the gender differences in QoL.23,24 Improved QoL was reported in females, compared to males, and was attributed to their higher levels of physical function. These findings conflict with previous literature, in which males were found to have greater QoL. 16 However, the review by Sinha et al. 16 included those with LLAs for non-vascular causes. Therefore, it is possible that QoL following a LLA may be greater in females when it is due to PAOD and improved in males when the LLA is due to trauma or tumour. Further research is warranted to examine these gender differences.
Although there were conflicting results regarding family support and its impact on QoL, those who live alone may be more capable, both cognitively and physically, and therefore have a better QoL. 22 Mac Neill et al. 22 also suggested a cause-and-effect relationship between QoL and living alone. More specifically, those who lived alone were more able to perform activities of daily living independently, a third engaging in social outings on a weekly basis. Consequently, they had better mental health as they felt less burdensome and relied less on others. Conversely, two studies suggested that living with family was associated with better QoL in comparison with those who lived alone.23,27 Although these studies focussed on living with family, the rating of good QoL may be replicated in a supportive environment such as residential or assisted living complex.
There are no validated QoL outcome measures available for the LLA population, accommodating both wheelchair and prosthetic mobility. The TAPES was used in one study; however, this only assesses the function of prosthetic users. 25 The PEQ, which has a sub-section that measures QoL, is the only outcome measure that has been validated for use in those with a LLA. Despite this, it is only relevant for those who receive a prosthesis and was only used in one study included within this review. 26 Developing and validating a QoL outcome measure for this population is imperative to allow for more rigorous future longitudinal studies, systematic reviews and meta-analyses.
This review has demonstrated that being able to walk with a prosthesis is the main factor affecting QoL after a LLA for PAOD. A number of factors such as age, level of amputation and the presence of co-morbidities also affect QoL in those with PAOD, but are not modifiable. It is therefore important that rehabilitation focusses on modifiable factors, particularly with regards to walking. Furthermore, LLAs due to non-vascular aetiologies have benefitted from advances in prosthetic technologies and access to rehabilitation.32,33 The improved technology may benefit amputees in prosthetic comfort, pain relief and energy conservation improving walking ability following LLA.
Study limitations
This review was limited to studies published in English. It was also limited by the heterogeneity of the study designs included. Due to the variety of outcome measures used, it was not possible to conduct a meta-analysis. Studies using qualitative methodologies were excluded from the review; however, they may have added context to the factors that influence QoL.
This review is novel in its focus on those with a LLA due to PAOD and as such has identified the factors that influence QoL in this population. Walking is the main factor that influences QoL following LLA and as such rehabilitation should focus on gait re-education with a prosthesis. To improve the QoL, there is a need for more prospective longitudinal studies with a standardised outcome measure which can examine the possible change in QoL over time.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by Diabetes UK through the Sir George Alberti fellowship.