
Abstract
Background:
In patients with lower limb amputations, gait alteration, increased loading on the intact extremity, and use of prosthesis may lead to joint degeneration.
Objective:
To explore the effects of prosthesis type on quadriceps muscle and distal femoral cartilage thicknesses in transtibial amputees.
Study design:
A cross-sectional study.
Methods:
A total of 38 below-knee amputees were enrolled in the study, of which 13 patients were using vacuum system type prosthesis and 25 patients were using silicon liner pin system prosthesis. Patients’ femoral cartilage and quadriceps muscle thickness measurements were performed using musculoskeletal ultrasound.
Results:
When compared with the intact sides, cartilage and rectus femoris, vastus intermedius, and vastus medialis muscle thickness values were significantly decreased on the amputee sides (all p < 0.05). Clinical characteristics and ultrasound measurements were similar between the two groups except the lateral and medial femoral condyle thicknesses, thinner in the silicon liner pin system users (both p < 0.05).
Conclusion:
The distal femoral cartilage and quadriceps muscle thicknesses were found to be decreased on the amputated sides, and the negative impact on the cartilage seemed to be worse in the silicon liner pin system users.
Clinical relevance
This study might provide another argument as regards the preference of vacuum system type prosthesis to prevent possible knee osteoarthritis due to cartilage thinning in adult transtibial amputees.
Background
Patients with lower extremity amputations usually suffer pain and loss of mobility in their remaining limbs.1,2 Changes in gait pattern and ground reaction forces in the intact leg have also been documented. 3 In amputees, it is believed that gait alteration, increased loading on the intact extremity, and use of prosthesis can lead to joint pain and degeneration.2,4,5 When compared with normal subjects, knee pain (intact limb) was seen nearly two times more in lower limb amputee patients. 2 Additionally, the prevalence of symptomatic knee osteoarthritis has been found to be 17 times higher than age-matched normal subjects in unilateral lower limb amputees. 1 Furthermore, it is also known that there is disparity between various prostheses. For instance, vacuum suspension systems do not inhibit wound healing, but allow early fitting of the prosthesis and provide prompt mobilization. 6
In amputees, articular degenerative changes have previously been shown by direct radiographs and ultrasound (US) imaging studies.4,7,8 Although direct radiographs have some limitations for cartilage evaluation (e.g. positioning problems, indirect prediction of cartilage thickness), they have been commonly used for evaluation of degenerative joint changes of lower limb amputees.4,7,9,10 Magnetic resonance imaging (MRI) is a standard technique for assessment of cartilage changes; however, it is expensive. On the other hand, US is a convenient and cost-effective imaging modality when compared with MRI.
In a recent US study, it has been reported that distal femoral cartilage was found to be thinner on the amputee side when compared to the intact leg in patients with unilateral transtibial amputations. 8 Herewith, another problem in these patients would be muscle atrophy leading to loss of strength on the amputated side. Using US and computed tomography, this has also been documented in transtibial amputees.11,12 Previous literature has reported that amputees have quadriceps muscle atrophy and thinner distal femoral cartilage; however, to the best knowledge of the authors, previous studies did not explore the relationship between these changes and the type of prosthesis in transtibial amputees.8,11,12 Additionally, cartilage and muscle problems have also not been studied together in these patients. Therefore, the purpose of this study was to assess the effects of different prosthesis types on quadriceps muscle and distal femoral cartilage thickness. In this regard, we have used US imaging which is a convenient imaging method for prompt evaluation of these structures.11,13,14
Methods
A total of 38 transtibial amputee subjects were recruited. They were enrolled if they had been using unilateral modular system (silicone liner pin system (N = 25) and vacuum system (active vacuum system (N = 12), passive vacuum system (N = 1)) below-knee prostheses for at least 6 months. Patients were excluded if they had bilateral amputation, rheumatic disease, previous lower limb surgery (other than the amputation), and contracture (limiting knee hyperflexion). The study protocol was approved by the local ethics committee, and the patients consented to participate.
Demographic and clinical characteristics of the subjects including age, weight, height, and body mass index (BMI), smoking habit, amputation indication (vascular or traumatic), stump length (measured between the tuberosity of tibia and the stump edge), duration of amputation and prosthetic use, type of prosthesis, and daily walking time with the prosthesis were recorded. Functional use of the prosthesis was assessed by Houghton score. 15
Ultrasonographic examinations were done bilaterally using a linear probe (5–12 MHz Logiq P5, Wisconsin, USA). Distal femoral cartilage assessment was performed as patients lay in supine position with their knees in maximum flexion. The transducer was placed axially above the superior edge of patella. 14 Cartilage thickness measurements were taken from the medial femoral condyle (MFC), lateral femoral condyle (LFC), and intercondylar area (ICA) (Figure 1). Muscle thickness measurements were done bilaterally from rectus femoris (RF), vastus lateralis (VL), vastus medialis (VM), and vastus intermedius (VI) muscles while patients lay in supine position with their lower limbs extended (and relaxed). The probe was held with light touch in order not to cause any muscle deformation. Images were obtained at the most bulky area of each muscle: 11 at mid-thigh (midway between the anterior superior iliac spine and the upper pole of the patella) for VI and RF muscles and at 10 cm rostral to the knee joint for VM and VL muscles (Figure 2). The probe was held axially on each muscle. For standardization of the thickness measurements, a perpendicular line was drawn from the femoral cortex, and the distance between the inner and outer borders of each muscle was measured (automatically by the US device). 16
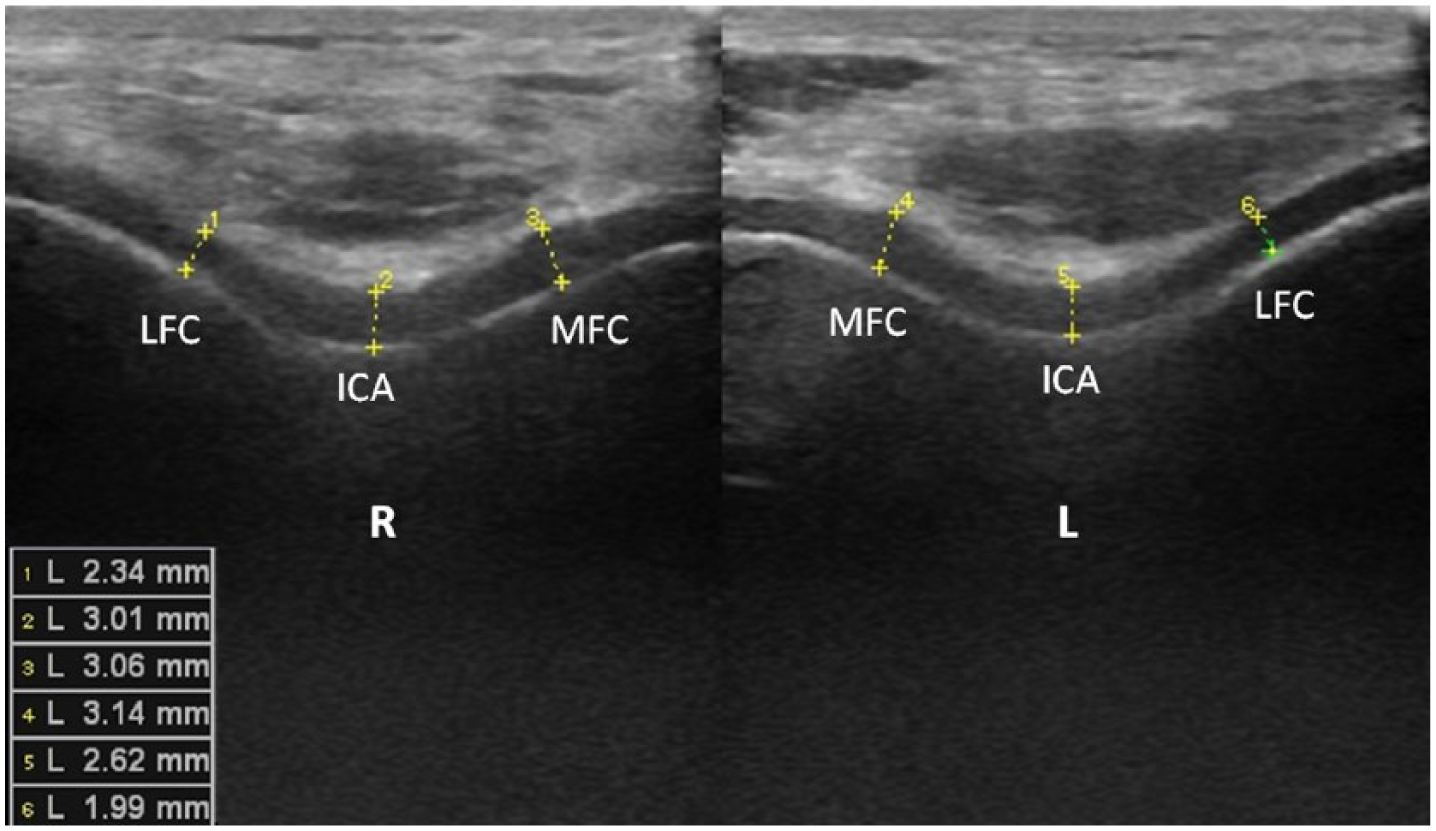
Ultrasonographic image (suprapatellar axial view) demonstrating bilateral femoral distal cartilage measurements. A perpendicular line was drawn from the mid points of the medial, intercondylar, and lateral sides of the cartilage.
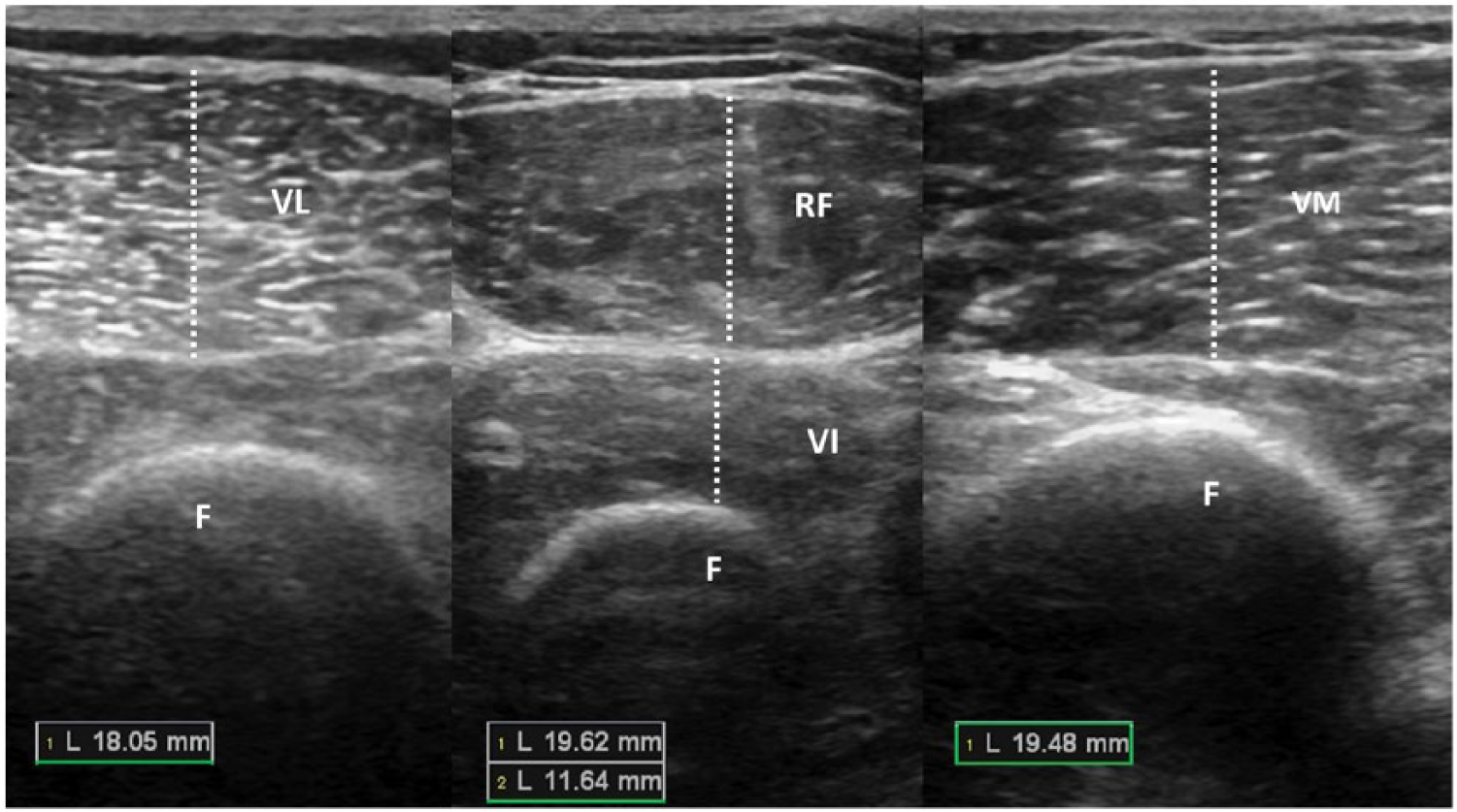
Ultrasonographic imaging (axial views) of the anterior thigh shows quadriceps muscle thickness measurements. The probe was held transversely above each muscle. A perpendicular line was drawn from the most outer edge of the femur between superficial and deep epimysium of the muscle.
Statistical analysis
Statistical analysis was performed using SPSS 17.0. Data are expressed as mean ± standard deviation. Normal distribution and homogeneity of variances were tested using Kolmogorov–Smirnov and Levene’s tests, respectively. Paired-samples t-test was used for comparison of the cartilage and quadriceps muscle thicknesses (intact vs amputee legs). Student’s t and Mann–Whitney U tests were used for comparison of the clinical/US measurements between groups. Categorical variables were compared with Chi-square or Fisher’s exact test. Correlations between subject characteristics and US measurements were evaluated by Spearman or Pearson correlation coefficients. Statistical significance was set at p < 0.05.
Results
Demographic and clinical characteristics of the subjects are given in Table 1. Distal femoral cartilage and quadriceps muscle thickness measurements of the subjects are given in Tables 2 and 3. When compared with the intact limbs, cartilage (at the LFC, MFC, and ICA) and RF, VI, and VM muscle thickness values were significantly decreased on the amputated limbs (all p < 0.05).
Clinical characteristics of the patients.
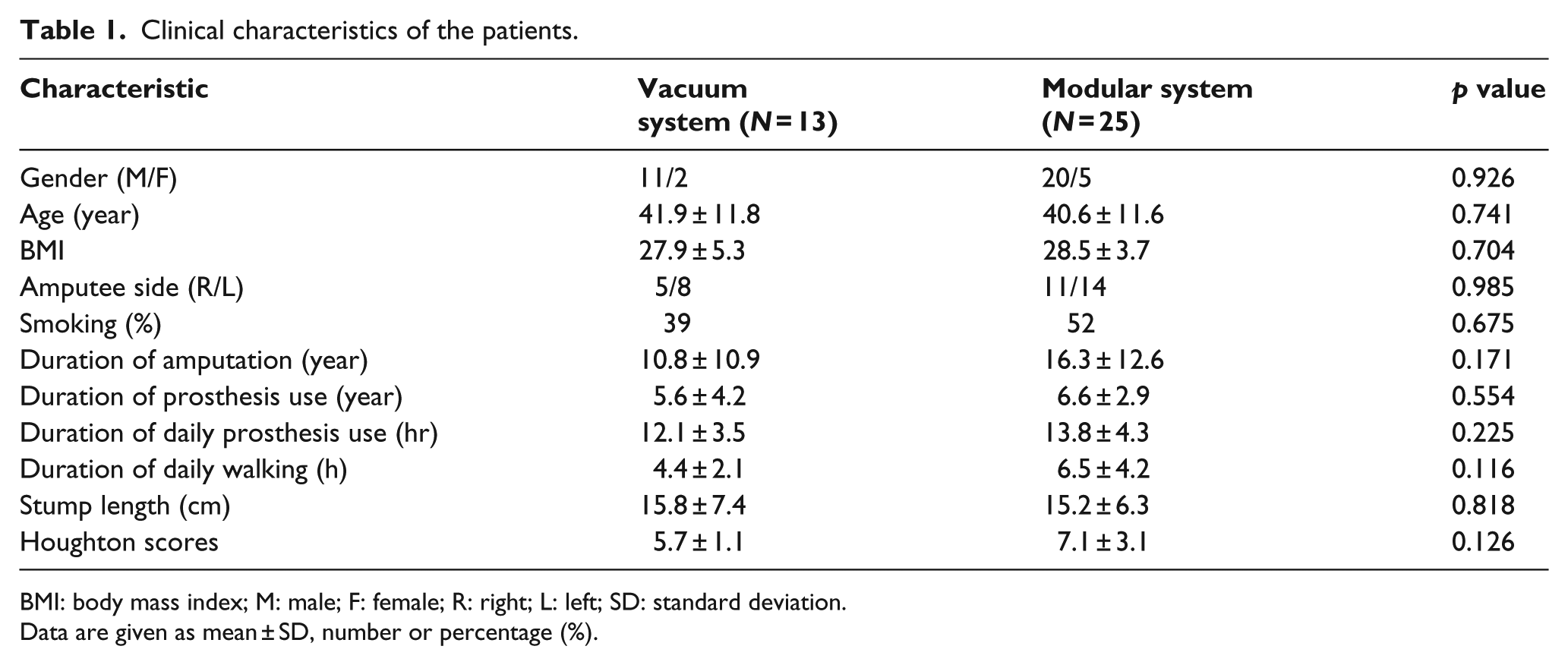
BMI: body mass index; M: male; F: female; R: right; L: left; SD: standard deviation.
Data are given as mean ± SD, number or percentage (%).
Comparison of femoral cartilage (mm) and quadriceps muscle thicknesses (mm) in amputated and intact legs.
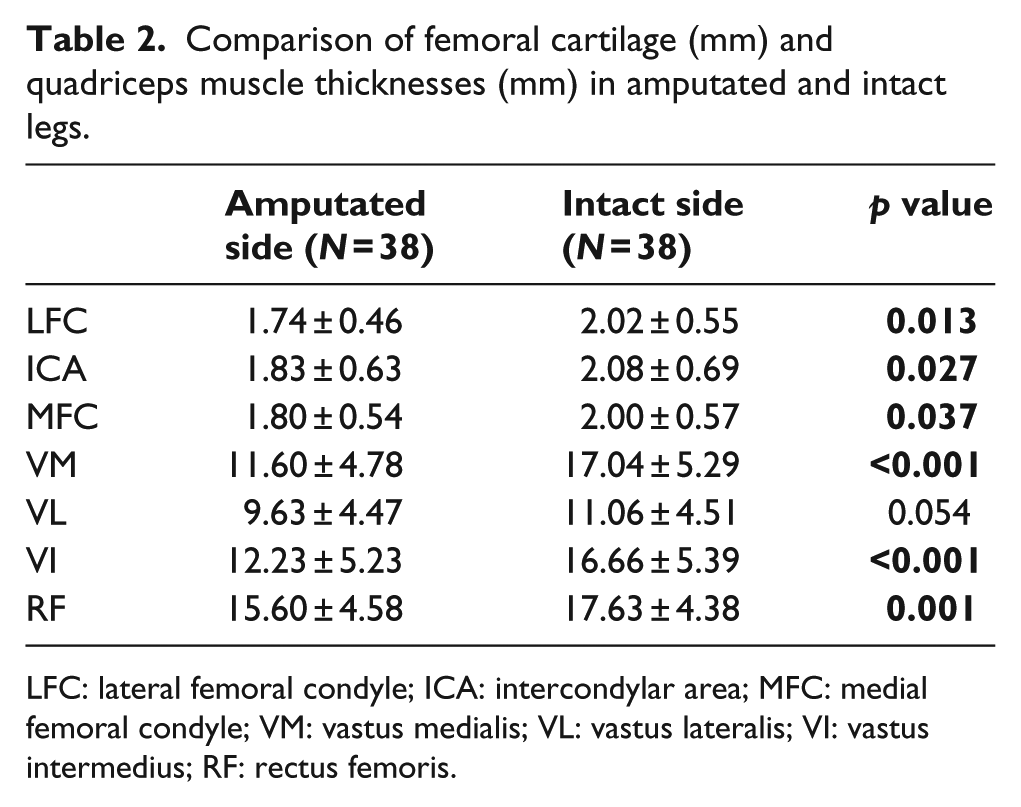
LFC: lateral femoral condyle; ICA: intercondylar area; MFC: medial femoral condyle; VM: vastus medialis; VL: vastus lateralis; VI: vastus intermedius; RF: rectus femoris.
Comparison of femoral cartilage and quadriceps muscle thicknesses (mm) in between vacuum system and silicon liner pin system groups.
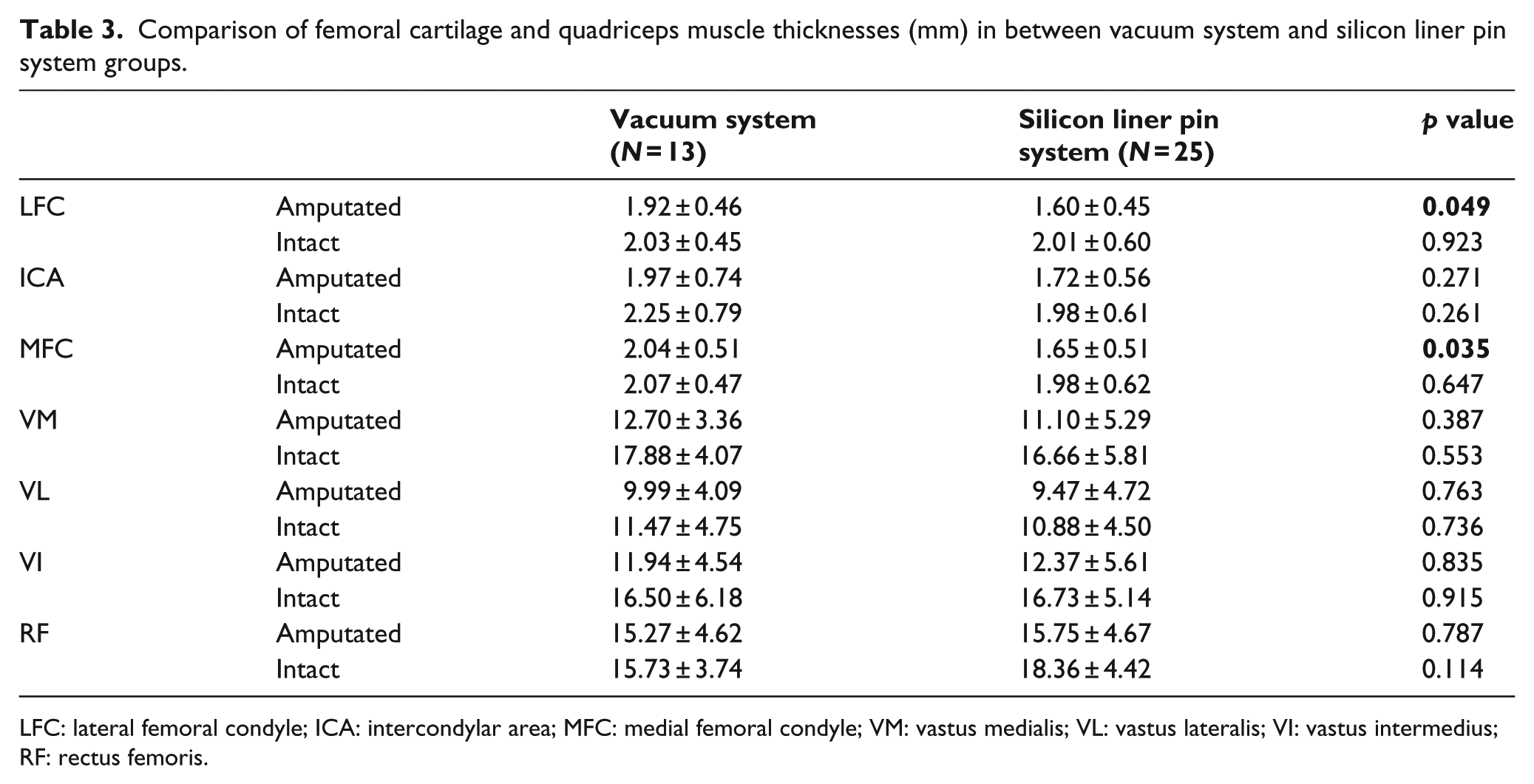
LFC: lateral femoral condyle; ICA: intercondylar area; MFC: medial femoral condyle; VM: vastus medialis; VL: vastus lateralis; VI: vastus intermedius; RF: rectus femoris.
Duration of amputation was negatively correlated with the LFC measurements (r = –0.396, p = 0.019) on the amputated sides and with the MFC measurements on both amputated (r = –0.431, p = 0.010) and intact (r = –0.410, p = 0.014) sides. BMI was positively correlated with VL (r = 0.476, p = 0.006) and VI muscle thicknesses (r = 0.454, p = 0.009) on the amputated sides.
Clinical characteristics and US measurements were similar between the two groups, except LFC and MFC thicknesses being thinner in the silicon liner pin system users (both p < 0.05) (Tables 1 and 3).
Discussion
The main objective of this study was to explore the effects of prosthesis type on muscle thickness and distal femoral cartilage in transtibial amputees. When compared with the intact sides, distal femoral cartilage and quadriceps muscle thicknesses were found to be decreased on the amputated sides. Furthermore, the decrease in cartilage thickness was worse in silicon liner pin system users.
Aside from the suggested indicators of successful prosthetic outcome, for example, patient’s age, comorbidity, and amputation level/etiology, the selection of prosthesis (according to patient’s characteristics/requirements) is also an important factor.6,17–19 Attachment of the prosthesis to the stump is provided with several suspension systems in different types of prostheses. The socket fit and the suspension system of the prostheses have important impact as regards the displacement of prosthetic limb on the stump (during walking–pistoning movement), stump skin problems, mobility, and satisfaction related to the prosthesis. 17 Several advantages of vacuum suspension systems have been reported in comparison with other conventional systems such as pin locked systems. Without inhibition of wound healing, vacuum suspension systems allow early fitting of the prosthesis and provide prompt mobilization. 6 Effects of different prostheses on residual limb and stump health have been investigated in biomechanical studies;6,15 however, the effects of prosthesis type on cartilage degeneration have not been studied. According to the results of our study, the unfavorable effects on the cartilage seemed to be worse in the silicon liner pin system users when compared to vacuum suspension users. This finding is one of the noteworthy results of this study.
On the other hand, joint degeneration and cartilage loss in the lower limbs of amputee subjects still remain to be a serious concern.1,4,7,8,20 Yet, decreased cartilage thickness either on the amputee or healthy limbs (unfavorably affecting the functionality) has been previously reported.1,4,7,8 Additionally, it has been shown that age-related muscle atrophy was seen predominantly in the anterior thigh muscles. 21 Moreover, one study has shown that (anterior) muscle atrophy developed in RF, VI, VL, VM, and sartorius muscles of the amputated limb, whereas dorsal thigh muscles (gracilis and hamstring muscles) were not significantly affected. 11 In that study, when compared with a healthy control group, atrophy was seen in the RF and VI muscles of the intact limb. In this study, we have selectively/comparatively explored the effects of two different prostheses on the distal femoral cartilage and quadriceps muscle thicknesses. Although muscle atrophy was observed on the amputated side of all subjects, it was similar between the two groups. However, LFC and MFC values were thinner in the silicon line pin system users. In a previous study, Lloyd et al. 22 reported that symmetric muscle strength had important implications to reduce the knee degeneration risk in transtibial amputees. Transtibial amputees walk with decreased knee joint flexion during the stance phase of the amputated limb, possibly due to reduced knee extensor activity.11,23 Therefore, detection of atrophy in the distal femoral cartilage and quadriceps muscle of our patients might be related to long-lasting inactivity or disuse.
There are some drawbacks in our study. Small sample size, cross-sectional design, and the lack of a healthy control group or functional assessment limit the generalization of our results.
Conclusion
In summary, we imply that distal femoral cartilage and quadriceps muscle thicknesses are decreased on the amputated sides of transtibial amputee subjects and that the unfavorable effects on the cartilage seem to be worse in the silicon liner pin system users. Future studies with larger samples and functional assessment (also including other prosthesis types) are awaited to better understand the clinical relevance of this difference and also to better guide the prosthetic prescription/use in this group of amputees.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.