
Abstract
Background:
This article describes a total surface bearing prosthetic socket for a patient (25-year-old female) with a bulbous stump.
Case Description and Methods:
The subject had unstable excessive soft tissue at the distal end of the residuum. After 2 years of prosthetic use, she experienced several problems, including pain in the residual limb and knee joint. Pressure distribution was evaluated during ambulation. We also designed a total surface bearing socket with Velcro as suspension system to distribute the load evenly on the residual limb, and to facilitate donning procedure.
Findings and Outcomes:
The main site of weight bearing in the old prosthesis (patellar tendon bearing) was anterior proximal region of the residual limb, especially the patellar tendon. The pressure was almost 10 times higher than the distal region during level walking. Pressures were distributed more evenly with the total surface bearing socket design, and the donning was much easier.
Conclusion:
Pressure distribution within the socket could be affected by socket design and suspension system. Using the total surface bearing socket and Velcro as suspension system might facilitate donning of prosthesis and reduce traction at the end of residual limb during the swing phase of gait.
Clinical relevance
Proper socket design and suspension system based on the amputees’ need can facilitate rehabilitation process and lead to the amputee’s satisfaction. The pressure is distributed more uniformly over the residual limb by the total surface bearing socket compared to the patellar tendon bearing socket for lower limb amputees with unusual stump shape.
Background
The incidence of transtibial amputations is very high. This level of amputation has been considered important in training and education for surgery, rehabilitation, and prosthetics in the past several decades. Some individuals with transtibial amputation never recover completely. 1 Surgical techniques for limb amputation generally emphasize on the tissue design or padding of muscle to cover the distal flap. The outcome is expected to be a residual limb with cylindrical shape, good padding of distal tibia and stable muscles. Prosthetic fit for areas with poor soft tissue is very challenging. 1
Successful rehabilitation of an amputee is pertinent to the design and fit of the socket because the weight-bearing capabilities of the residual limb and the foot are not identical.2,3 Distribution of interface pressure between the socket and the tissues of residual limb may alter the user’s comfort, and thus is important for the socket design.2,4 Residual limb is exposed to shear stresses and pressures at the interface of prosthetic socket and residual limb during ambulation.5,6 Various suspension systems have different effects on the interface pressure during ambulation.7–9 Pressures at the socket/skin interface vary considerably among individuals, sites, and clinical conditions.
Suspension system and prosthetic socket shape have significant roles in function of lower limb prosthesis. Proper suspension system should eliminate piston movement (vertical movement) and unwarranted translation between the socket and residual limb. 10 The suspension systems fix residual limb inside the socket through a single distal pin/lock, suction, lanyard, or magnetic coupling.9,11 Pin/lock systems apply tension distally to the residual limb and compression proximally during the swing phase of gait.9,12 Amputees with contracture may have difficulty to use pin/lock systems. In comparison to other systems, suction systems offer improved fit and reduce the quantity of pistoning within the socket. However, donning and doffing the prosthesis is a concern. 13
Lanyard suspension system comprises a lanyard cord that is attached to the distal part of the silicone liner, similar to the pin/lock system. Dietzen et al. 14 mentioned the use of Velcro as suspension system for transfemoral amputees.
Variations of the patellar tendon bearing (PTB) socket designs for transtibial prosthesis are available since 1957. 15 In this design, the sensitive areas are given relief, while the load is mainly taken by the load-tolerant areas,1,15 which can cause extra piston motion within the socket.10,16 Previous literature shows that pressure was not distributed uniformly in PTB socket.5,17–19 Convery and Buis 18 found higher pressure concentration near the proximal brim of the PTB socket (patellar bar areas), while Zhang et al. 19 observed higher pressure at the popliteal area compared to the patellar tendon.
By the development of elastomeric liners (such as silicone and gel liners) and the total surface bearing (TSB) socket, pressure could be distributed uniformly over the residual limb.20–22 Dumbleton et al. found higher pressures in the TSB socket compared to the PTB socket. Never-theless, the level of satisfaction with both sockets was similar. 23 Yigiter et al. 16 stated that weight acceptance, gait symmetry, and balance could improve with the TSB socket compared to the PTB. Narita et al. 24 also found superiority of the TSB over the PTB socket in terms of amputee satisfaction and stability.
This study aimed to examine pressure distribution over a residual limb with unusual shape (bulbous) during ambulation with two different prosthetic socket designs (PTB and TSB). Furthermore, we used Velcro as suspension system to enhance fit and facilitate donning procedure.
Case report
Ethical approval was obtained from the University of Malaya Medical Centre (UMMC) Ethics Committee. The subject was a young transtibial amputee (25-year-old female) whose lower limb was amputated 2 years ago. She consented to participate in the study.
The subject had excessive, unstable soft tissue at the end of the bulbous residual limb (Figure 1). She was referred to the Brace and Limb Laboratory, University of Malaya, because of pain at the end of the tibia and patellofemoral arthritis. She had used the transtibial prosthesis (PTB socket) with silicone liner (6 mm thickness), pin/lock, and energy storing foot for 2 years. She experienced a severe crackling sensation when moving the knee, which was loud enough to be heard by others. Furthermore, it was difficult for her to align the distal pin due to the residual limb shape.

Stump in different views (knee is in full extension).
We evaluated the interface pressure between the socket and stump during walking (level ground, and stair and ramp ascent and descent). Also, a TSB prosthesis was designed with the intension to distribute the load evenly on the stump and facilitate prosthetic donning. Velcro was used to suspend the prosthesis. Two small openings were created on the medial and lateral socket walls (Figure 2). We fixed the Velcro (hook fastener) to the socket wall (strap) and the loop fastener to the soft silicone liner (Figure 2).
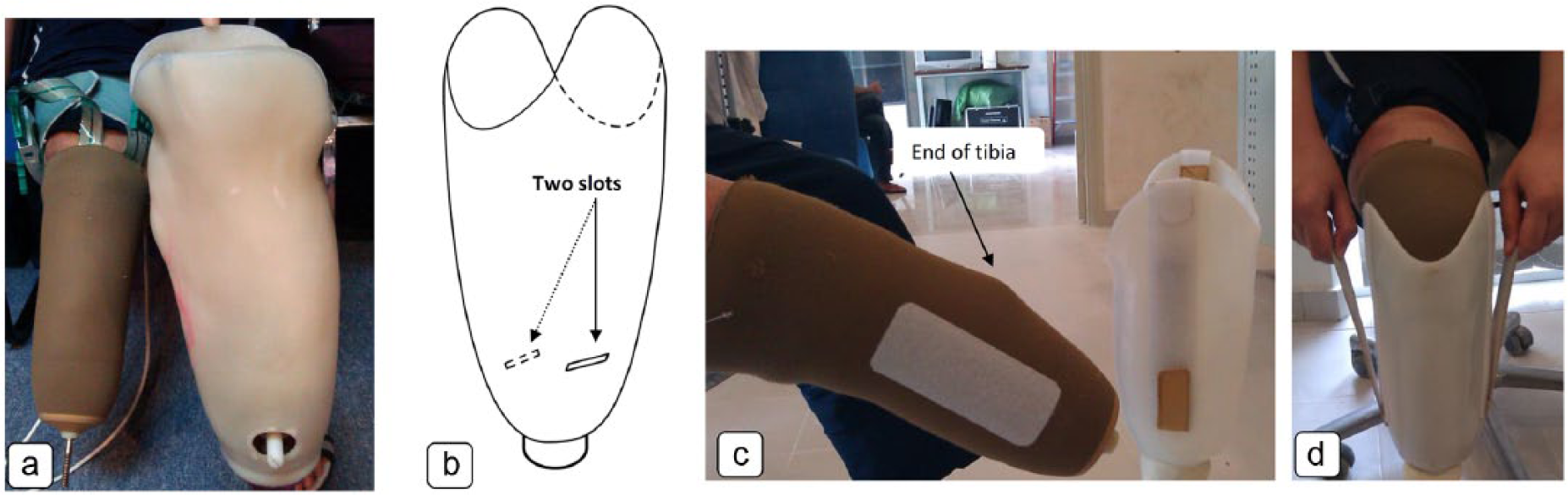
(a) Old prosthesis (PTB with silicone liner), (b) TSB socket design with two slots, (c) Velcro (loop fabric) attached to the liner, and (d) donning process.
The subject was fitted with transparent (12 mm, Northplex®, North Sea Plastics Ltd, UK) check socket to ensure TSB. Following the evaluation of fit and gait, she was asked to use new prosthesis for one month to adapt to the TSB socket. The subject had adapted to the large differences in pressure magnitudes in the former prosthesis; consequently, at first, it was difficult for her to use the new socket with the even distribution of the load on the residual limb. Thus, she was asked to increase the time of prosthesis wear and weight bearing on the prosthetic socket gradually. The subject achieved 12 h of prosthetic use after about 3 weeks when she was comfortable with the socket during walking.
The interface pressure between the stump and socket was mapped and compared during walking on level ground, and ascending and descending the stair and ramp. In order to become familiar with the environment, we asked our subject to walk in the motion analysis laboratory at a self-selected speed on the level ground, stairs, and slope prior to the experiment. To measure the pressure, four F-Socket sensors (9811, Tekscan Inc., USA) were placed on the residual limb over the medial, lateral, anterior, and posterior surfaces. The pressure profile was mapped using the Tekscan software version 6.51.
Prior to the experiment, the sensor arrays were equilibrated and calibrated using the Tekscan pressure bladder to eliminate the variation among the load cells. The patient body weight was used to calibrate the sensors in the pneumatic bladder before use. Three separate experiments were conducted for the level walking, stair, and ramp negotiations. The subject was required to ascend and descend a 4-m custom-made ramp. She was also asked to ascend and descend a custom-made staircase 82 cm wide with four steps 14 cm high. The steps were 32 cm apart. The subject completed five trials of each condition. Linear interpolation was applied to the data points to make equal lengths of data sets. The data were averaged across strides within trials and across the five trials by expressing time as a proportion of the gait cycle.
We also inquired her feedback on each system. The questions (some parts of the Prosthesis Evaluation Questionnaire (PEQ)) were related to the ability of walking with prosthesis, prosthetic fit, ability to don and doff the prosthesis, distal skin traction, residual limb pain, and overall satisfaction. 25
Findings and outcomes
Pressure measurements were logged over 12 sites of the residual limb. The findings showed that with the old prosthesis, the proximal residual limb, particularly the patellar ligament (anterior proximal) tolerated most of the load during level walking (115 ± 5.2 kPa). It was almost 10 times higher than the mean peak pressure applied to the anterior distal residual limb (12 ± 3.4 kPa). Furthermore, the pressure applied to the posterior distal (110 ± 4.5 kPa) was higher than the posterior proximal (57 ± 2.7 kPa) with the old prosthesis. Besides, the subject experienced more pressure over the proximal and distal residual limb during swing phase of gait with the old prosthesis. Figure 3 depicts mean pressures in different areas of the socket over the gait cycle during normal walking. With the new socket, the pressure was distributed more evenly over the residual limb (anterior, posterior, medial, and lateral) during walking, and extra load was successfully relieved from the anterior proximal (patellar bar).
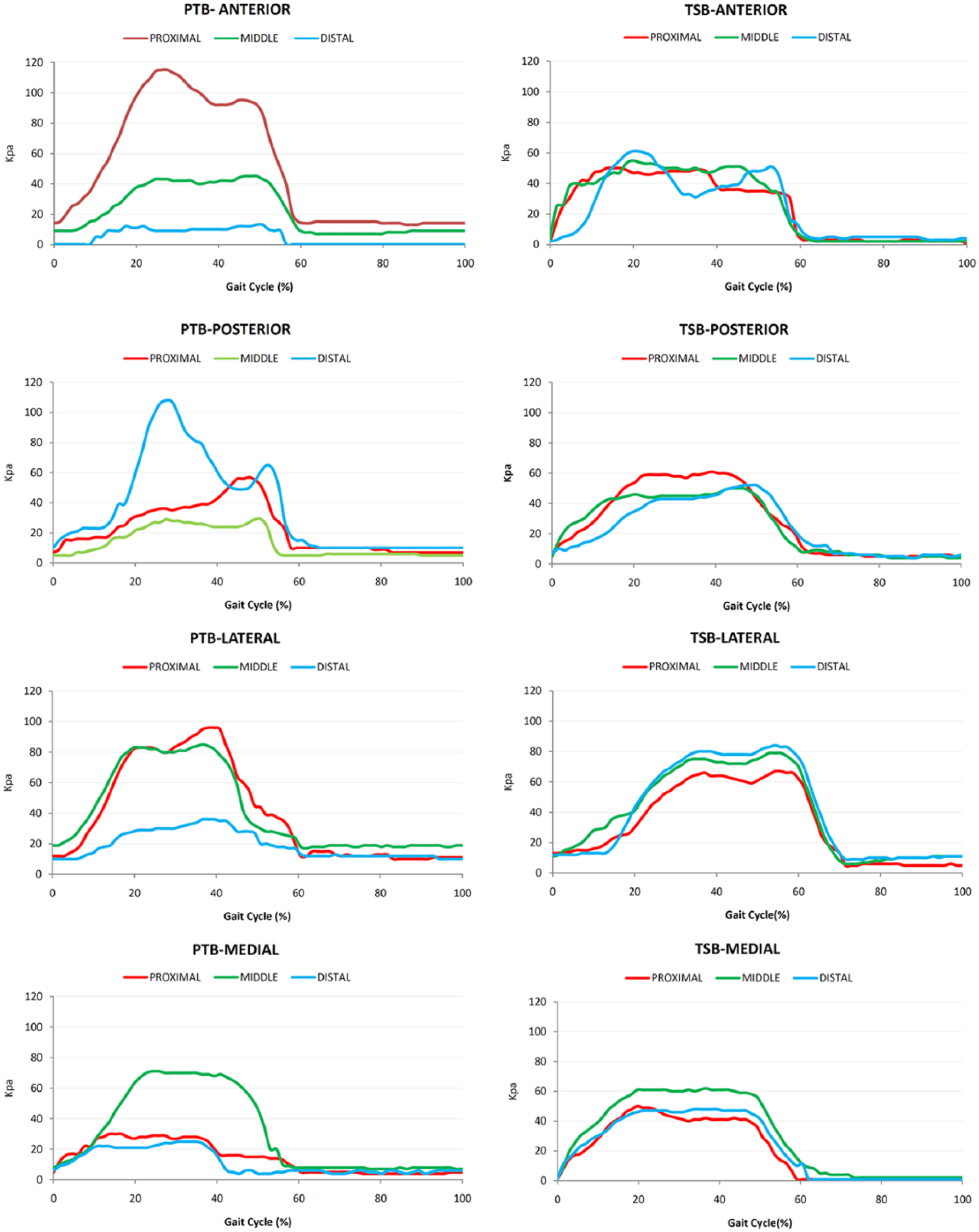
Interface pressure during normal walking (self-selected speed).
From the findings, the subject also experienced higher pressure over the anterior proximal aspect of the stump (patellar ligament) during ramp and stairs negotiation with the old prosthesis. It was as high as 132 ± 6.1 kPa and 117 ± 4.1 kPa when the subject walked down the slope and stairs, respectively. Figure 4 depicts peak pressures in different areas and compares the incline and stairs negotiation (up and down).
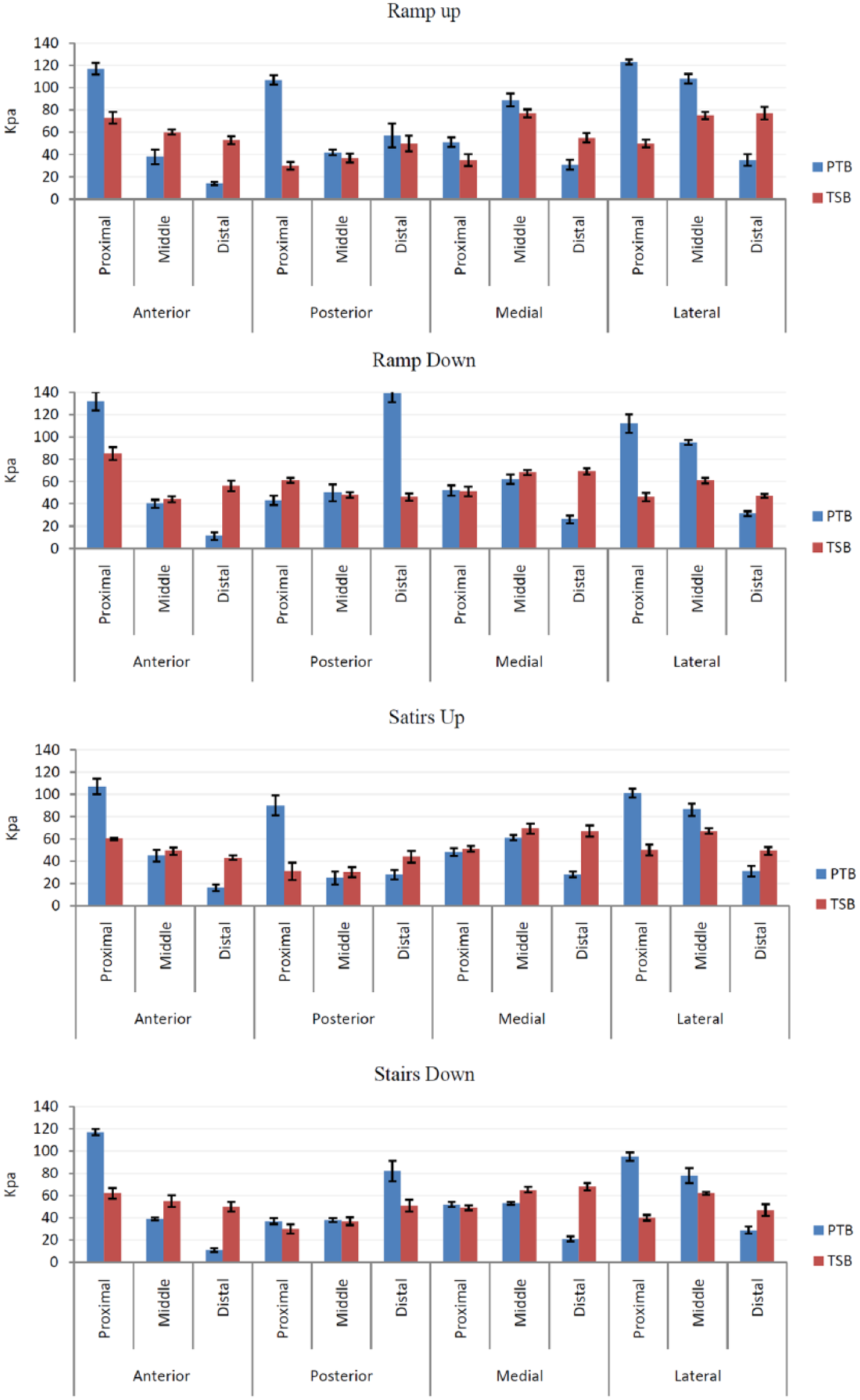
The average peak pressure (kPa) based on the socket type and sensor site during ramp (up and down) and stairs (up and down).
Subjective feedback showed improved contact between the liner and socket and decreased traction and rotation inside the socket with the TSB prosthesis. Our subject also reported a stretch at the distal tissue of the residual limb during the swing phase using the PTB socket with pin/lock suspension system. The subject stated that she was satisfied with the new socket. She could not feel any difference between the systems during sitting. Even though we did not measure the walking velocity, subjective feedback revealed faster walking with the new prosthesis and less traction and pain at the end of the stump.
The subject was also more satisfied with the donning and doffing procedures of the new prosthesis because there was no pin to align. Furthermore, she was more confident during walking without any rotation inside the socket compared to the old prosthesis. Interestingly, she could not walk with her old prosthesis after 2 months because it caused excessive pressure over the anterior proximal aspect of the socket (patellar ligament).
Discussion
Proper amputation surgery and fitting of the prosthetic socket for persons with lower limb amputation play significant roles in the rehabilitation outcome. 1 Furthermore, biomechanical understanding of the interface pressure between the socket and residual limb can improve the outcome of amputee rehabilitation. This case study compared two different socket and suspension designs on a transtibial amputee with unusual residual limb in terms of interface pressure and satisfaction.
Different suspension systems distribute the pressure differently over the residual limb. 8 Based on the literature, pressure was not distributed evenly in the PTB socket,5,17–19 and high values of interface pressure have been reported at the anterior proximal socket (PTB bar) with the PTB design.4,18 We also found that the patellar tendon was the main site of weight bearing within the PTB socket with the silicone liner during ambulation. The magnitude of pressure applied to the anterior proximal region of the PTB prosthesis with 6 mm silicone liner was 10, 8, and 12 times higher than the distal region during level walking, slope up, and slope down, respectively. Additionally, the pressure was 7 and 11 times higher than the distal region during stairs ascent and descent, respectively.
This study shows that the pressure was distributed more uniformly over the residual limb in the TSB socket, which was similar to the previous findings.20,26 The average magnitudes of pressure within the new socket was less than 80 kPa that mirrored the findings of previous studies on the TSB systems23,26 (Figures 3 and 4).
Although able-bodied individuals can easily negotiate ramps and stairs, these tasks become challenging when the motor functions are altered due to limb loss. The anterior proximal socket area exhibited higher mean peak pressure during the stair and ramp ascent and descent, which is consistent with the findings of Dou et al. 27 However, Wolf et al. 28 reported high pressure at the anterior distal region during the stair ascent, which is contrary to our findings. Dou et al. 27 observed increased pressure at the anterior proximal and posterior proximal (popliteal area) regions during the ramp ascent, which is consistent with our observations (Figure 4).
Research has shown that the pin/lock liners exert compression on the residual limb proximally and tension distally during the swing phase of gait (milking). 9 This milking phenomenon is probably the cause of short- (edema and redness) and long-term (discoloration and thickening) transformations, particularly at the distal end of the residuum.9,12 Similarly, we found that the pressure was higher with the amputee’s former prosthesis (the pin/lock system) during the swing phase of gait (Figure 3). Even though Dietzen et al. 14 mentioned the use of Velcro as suspension system for transfemoral amputees, it was a kind of lanyard system. The only difference is using the Velcro instead of the rope, and milking is still a concern. In this study, two pieces of Velcro (medial and lateral sides of the liner) fixed the liner inside the socket (not the distal part) and could decrease the rotation and milking problems.
Using the TSB socket and Velcro (as a suspension) can be a better option for lower limb amputees with unusual stump shape and could distribute the pressure more uniformly over the residual limb compared to the PTB socket. Furthermore, it might reduce the traction at the end of the residual limb during the swing phase of gait.
Footnotes
Acknowledgements
The authors would like to thank Dr Nader Ale Ebrahim and Mr Knut Lechler and Mr Mohd Firdaus Jamil for their help and encouragement.
Author contribution
H.G.H. designed the system and the protocol, fabricated the prosthesis, conducted the experiments, collected and analyzed the data, discussed the results, and drafted the manuscript. N.A.A.O. and C.T.Y. supervised the overall project, and helped in revising the manuscript. A.E. and N.A.A. analyzed the data, discussed the results, and prepared some parts of the manuscript.
Declaration of conflicting interests
The authors have no conflict of interest.
Funding
This research was supported by the Malaysia UM/MOHE/HIR (project number: D000014-16001), (grant/award number: “project number: D000014-16001”).