
Abstract
Background:
Lower limb amputation sometimes predisposes to degenerative secondary disorders.
Objectives:
To evaluate the distal femoral cartilage thicknesses of patients with unilateral transtibial amputations using ultrasound and to investigate the relationship between cartilage thickness and disease-related parameters.
Study Design:
Cross-sectional study.
Methods:
Twenty-four unilateral transtibial amputees (mean age: 46.4 ± 8.5 years, range: 28–60 years) were evaluated. Duration of prosthesis use (years) and daily walking time with prosthesis (hours) were recorded. Functional status was assessed by gate velocity (m/s), and 6-min walking distance (m) with prosthesis. Ultrasound was used to measure distal femoral cartilage thicknesses bilaterally at medial/lateral condyles and the intercondylar areas. The percentages of cartilage loss (of the amputee-side in comparison with the nonamputee-side) were calculated.
Results:
Compared to the nonamputee-sides, distal femoral cartilage was significantly thinner at lateral condyles and the intercondylar areas on the amputee-sides (p < 0.05). Significant positive correlations were detected between the percentage of cartilage loss (at all three sites of measurement) and gate velocity, 6-min walking distance, and daily walking time with prosthesis (all p < 0.05).
Conclusions:
Future prospective controlled studies are warranted to determine the principles of optimum prosthetic use regarding its possible effects on the femoral cartilage of amputee patients.
Clinical relevance
The correlations between the cartilage loss in the amputee extremity with faster gait and longer daily prosthetic use suggest that abnormal gait patterns might increase the loading on the amputated extremity.
Background
Lower extremity amputation not only limits mobility, but also predisposes to painful secondary disorders that result in additional disabilities. 1 For instance, increased risk of osteoarthritis in the intact knee is one of those secondary disorders. It was reported that in patients with unilateral lower extremity amputations, the prevalence of knee pain is twofold and that the prevalence of knee osteoarthritis is 17 times greater than their age-matched nonamputees.2,3 These problems were attributed to the biomechanical changes secondary to the increased loading on the intact extremity, and also to the extremity loss and/or prosthesis use. 4 While some studies reported increased risk of postamputation degenerative changes in the joints of the intact extremity,2,3 others showed cartilage loss in the hip joint of the amputee-side.5,6
In addition to the studies investigating the biomechanical and clinical changes in the intact extremity,2,3 several imaging modalities have been studied to show the degenerative changes in the intact and amputee-sides of these patients.4 –6 Among them, direct radiographs have been commonly used to assess the degenerative articular changes in lower extremity amputees.5 –8 However, direct radiographs are inadequate for the assessment of the cartilage and have some limitations due to the positioning of the knee.9,10 Magnetic resonance imaging (MRI) can also be used for the assessment of the cartilage, but it has the disadvantage of being expensive. 9
Ultrasonography (US) is a relatively inexpensive imaging modality (when compared with MRI) and is adequate for the assessment of cartilage than direct radiographs, that is, patient acceptability of the US examination is high, with no radiation exposure. The validity of US in the measurement of distal femoral cartilage thickness was previously reported.9,11 –15 On the other hand, there are no studies on the sonographic evaluation of the distal femoral cartilage thickness in patients with unilateral transtibial amputation. Therefore, the present study aimed to investigate the effect of amputation on the distal femoral cartilage thicknesses by using US and to determine the correlations between cartilage thicknesses and certain disease-related parameters such as stump length, time elapsed after the amputation, duration of prosthesis use, and functional status.
Methods
All lower extremity amputee patients who were admitted to our Orthopedic Rehabilitation Unit were evaluated. Among them, patients with acquired transtibial lower extremity amputation and sufficient cognitive functions to answer the questions were recruited. The study was approved by the Local Ethical Committee, and written informed consent forms were obtained from the participants.
The inclusion criteria were as follows: patients having an unilateral transtibial amputation, and using a silicone liner, pin-locked, solid action cushioned heel (SACH) foot prosthesis for at least 3 months. The exclusion criteria were as follows: patients having a bilateral amputation, a diagnosis of rheumatologic disease, previous surgery in the lower extremities (other than amputation), intra-articular knee joint injections performed within the past 6 months, glycosaminoglycan preparation use within the past 6 months, presence of a contracture that limits the knee hyperflexion, or having a congenital amputation. Among 58 lower extremity transtibial amputee patients, 22 were not eligible to participate in the study. Thirty-six patients fulfilling the inclusion criteria were called by phone. Four of them were not accessible; the remaining patients were informed about the study. Among them, four patients did not accept to participate and two were excluded from the study because of a trauma history in the intact knee at the time of injury preceding the unilateral amputation, and two of them were excluded because of use of a different type of prosthesis (carbon foot). The remaining 24 patients were enrolled in the study.
Data, including age, gender, body height (cm), body weight (kg), education, occupation, coexisting systemic diseases, dominant extremity, amputee extremity (left/right), amputation indication (vascular or traumatic), stump length (measured between the medial side of the knee joint and the stump edge), time elapsed since amputation (months), and the duration of prosthesis use (months) were recorded. All patients were asked about their daily hours of prosthesis use and walking.
All patients marked the knee and stump pain severity on a Visual Analogue Scale (VAS; from 0 (no pain) to 10 (worst pain)).
Functional status was assessed by gate velocity and 6-min walking distance with the prosthesis. For calculation of the gate velocity, patients were asked to walk a 10-m distance as fast as possible; the walking time was recorded and walking speed was calculated in meter per seconds. The 6-min walking distance (in meter) was measured as the distance each patient walked with the prosthesis within 6 min. 16 In addition, functional level of the patients was determined by the K classification system. 17
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was used for the assessment of knee-related functional status for both amputee and nonamputee-sides. 18 The WOMAC consists of 24 items divided into three subscales: WOMAC-A (pain, 5 items), WOMAC-B (stiffness, 2 items), and WOMAC-C (physical function, 17 items). The items are scored on a 5-point Likert scale, and the global score is taken as the sum of all item scores for each subscale.
All sonographic examinations were performed with a 5–13 MHz linear probe (General Electric, Logiq P5). In an attempt to blind the ultrasonographer (N.A.), patients were prepared for US by another physiatrist (S.K.). She took off the liner of the prosthesis distal to the knee joint. Patients did not take off their prosthesis and prosthetic foots. While patients were lying in supine position on the examination table, knees were flexed as much as possible, and their feet were on the examination table (the flexion angles were similar between the normal vs amputee-sides; 134.6° ± 1.4°, 133.8° ± 2.7°, respectively; p > .05). The distal parts of the knees were covered by a sheet. The US probe was placed transversely on the horizontal line drawn at the superior edge of the patella, perpendicular to the knee articular surface. 9 The angle between ultrasound transducer and articulating surface was recorded for each knee, and these values ranged from 0° to 10° as described by Naredo et al. 12 Imaging parameters were same for both knees of each patient. Sonographic measurement of the distal femoral cartilage thickness was performed by N.A. by drawing a straight line on midpoints of the lateral condyle, intercondylar notch, and medial condyle from the cartilage–bone interface to the synovial space–cartilage interface. 12 The measurements (at three reference points perpendicular to bone–cartilage interface) were repeated thrice for each knee joint. The averages of the three measurements were used to calculate the cartilage thicknesses at medial/lateral condyles and the intercondylar area. All images were evaluated by another physiatrist (L.Ö.) (an expert ultrasonographer with more than 10 years of background in musculoskeletal US) to increase the accuracy of measurements (Figure 1).
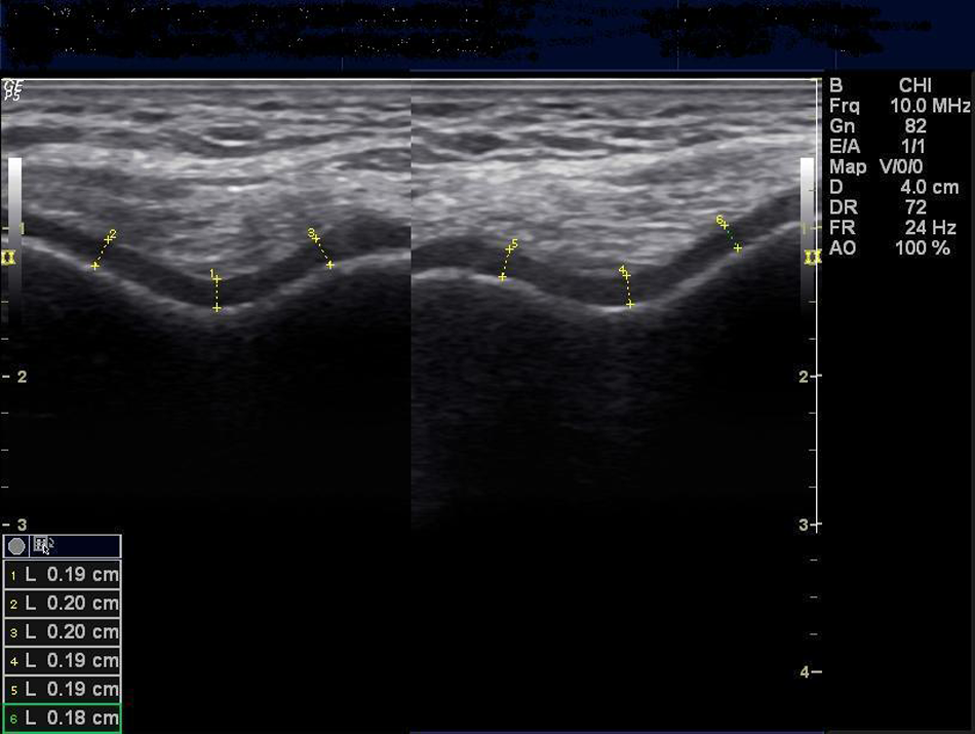
Ultrasound image (suprapatellar axial view) demonstrating the bilateral cartilage measurements in one patient: (1) right knee intercondylar area, (2) right knee lateral condyle, (3) right knee medial condyle, (4) left knee intercondylar area, (5) left knee medial condyle, and (6) left knee lateral condyle.
The percentage of distal femoral cartilage thickness (DFCT) loss of the amputee-side (in comparison to the intact side) was calculated for the three sites of measurement as follows: 100 × (DFCTintact − DFCTamputee)/DFCT intact.
Statistical analyses were performed using SPSS 17.0 software. Descriptive statistics were used for numeric demographical data and frequency analysis was used for categorical data. Wilcoxon signed-rank test was used for the comparison of the distal femoral cartilage thickness of the intact and amputee-sides. Spearman correlation coefficient was used to examine the relationship between cartilage thickness/loss of the amputee-sides with other variables and p-values less than 0.05 were considered significant.
Results
Twenty-four unilateral transtibial amputee patients with a mean age of 46.4 ± 8.5 years (range: 28–60 years) were analyzed. Table 1 represents the demographical and clinical features of the patients. The indication for amputation was peripheral vascular insufficiency in 15 (62.5%) and trauma in 9 (37.5%) patients.
Demographic and clinical features of the patients.
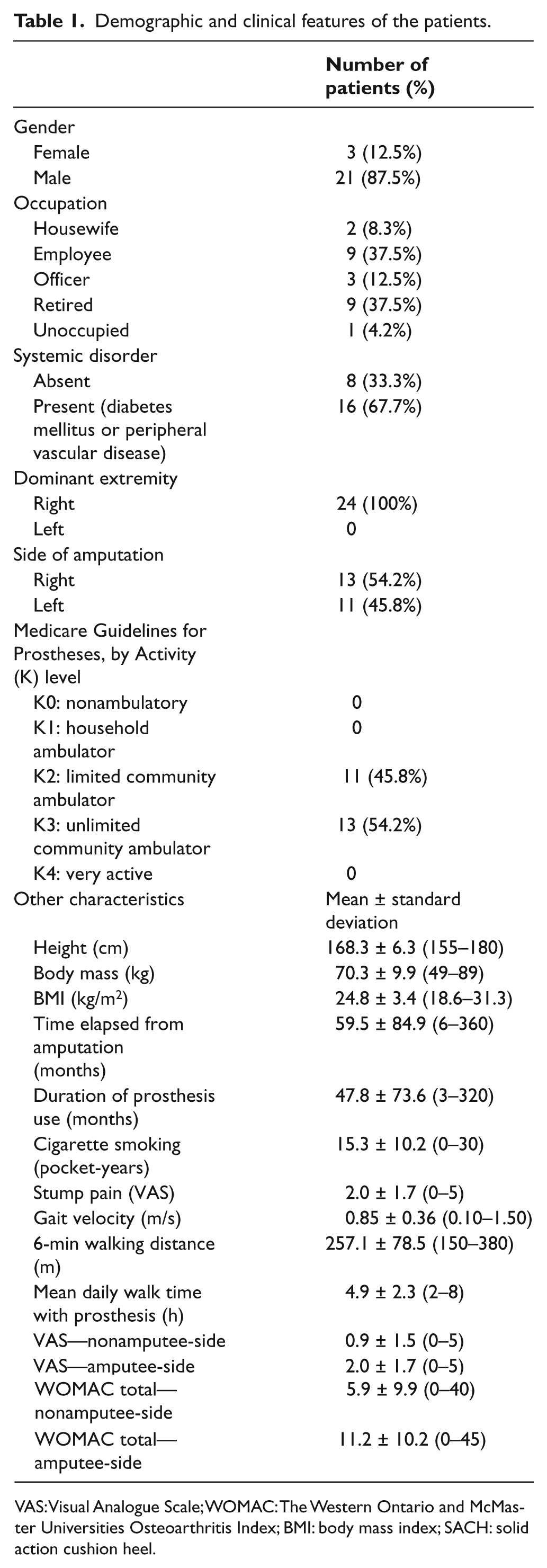
VAS: Visual Analogue Scale; WOMAC: The Western Ontario and McMaster Universities Osteoarthritis Index; BMI: body mass index; SACH: solid action cushion heel.
When compared with the intact side, distal femoral cartilage thickness was significantly decreased at the lateral condyle and the intercondylar area, but not at the medial condyle of the amputee-side (Table 2).
Comparison of cartilage thicknesses (amputee vs nonamputee-sides).
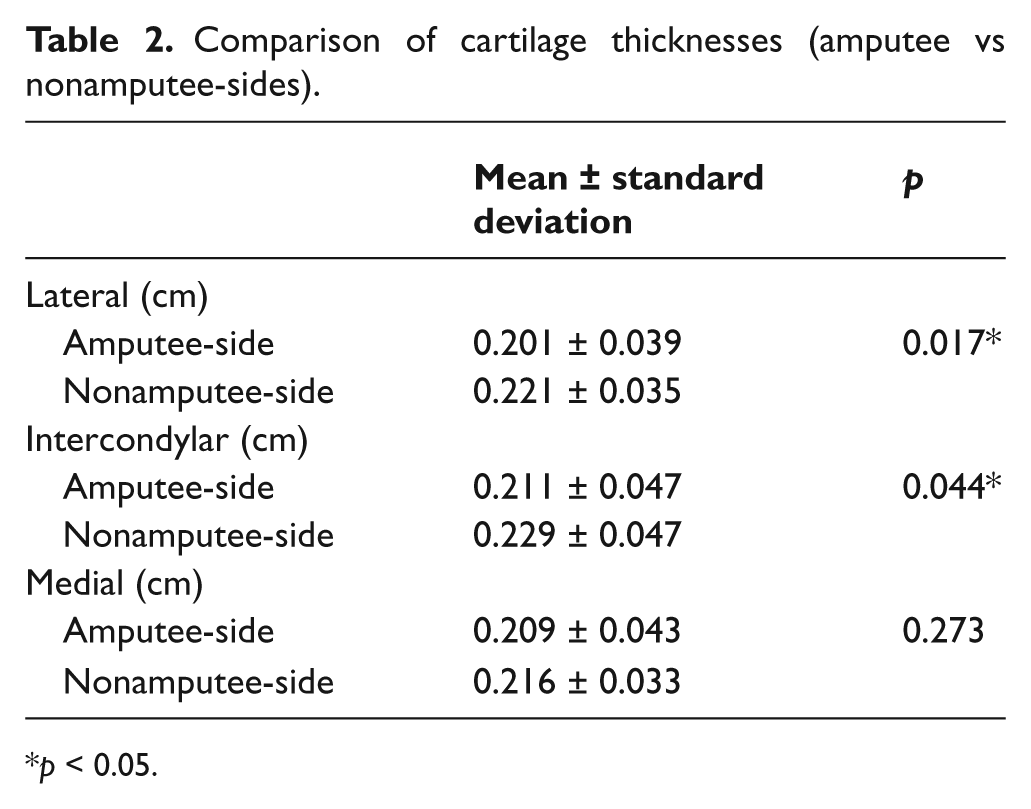
p < 0.05.
Lateral condyle cartilage thicknesses (amputee-sides) were positively correlated with time elapsed since amputation, duration of prosthesis use (months), velocity of walking, 6-min walking distance, and daily walking time with prosthesis (Table 3).
Correlations between cartilage thicknesses and clinical features of the patients.
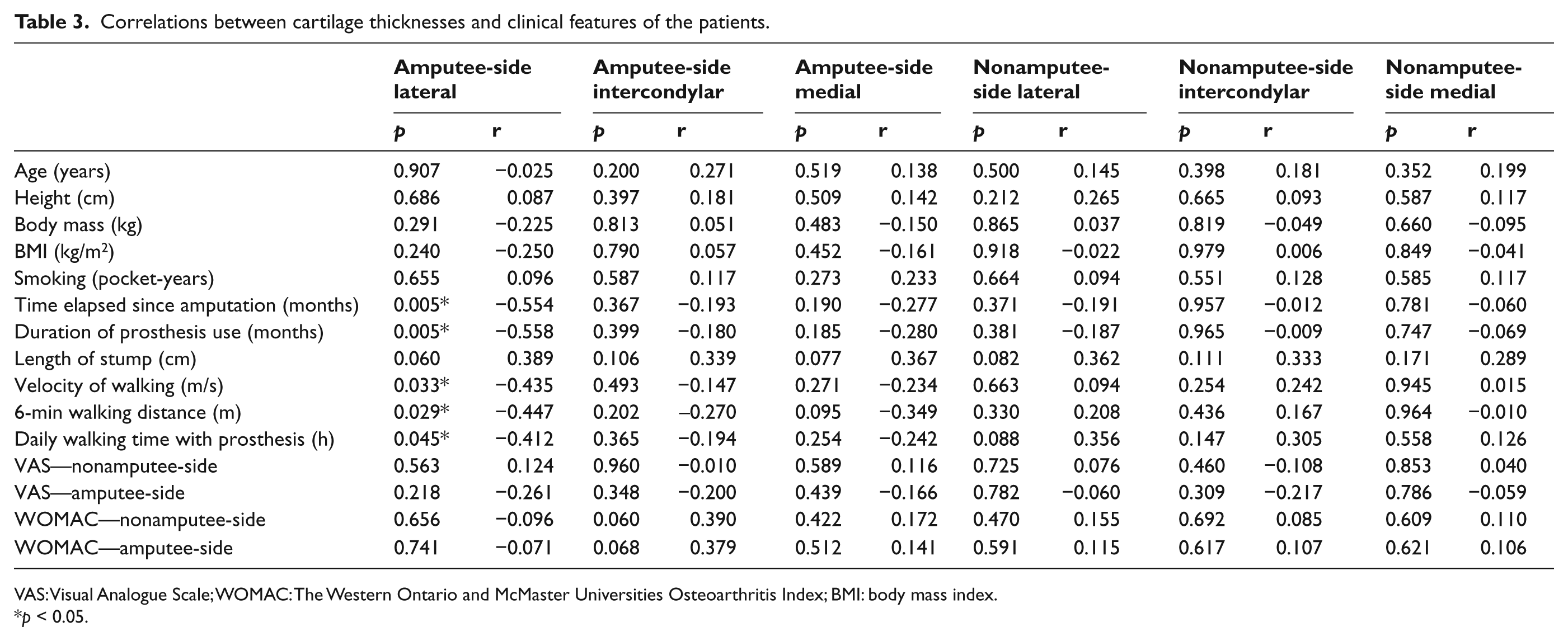
VAS: Visual Analogue Scale; WOMAC: The Western Ontario and McMaster Universities Osteoarthritis Index; BMI: body mass index.
p < 0.05.
The percentages of cartilage loss (at all three sites) on the amputee limbs were positively correlated with velocity of walking, 6-min walking distance, and daily walking time with prosthesis (Table 4; all p < 0.05) but not with other parameters.
Correlations between the cartilage loss and the clinical features of the patients.
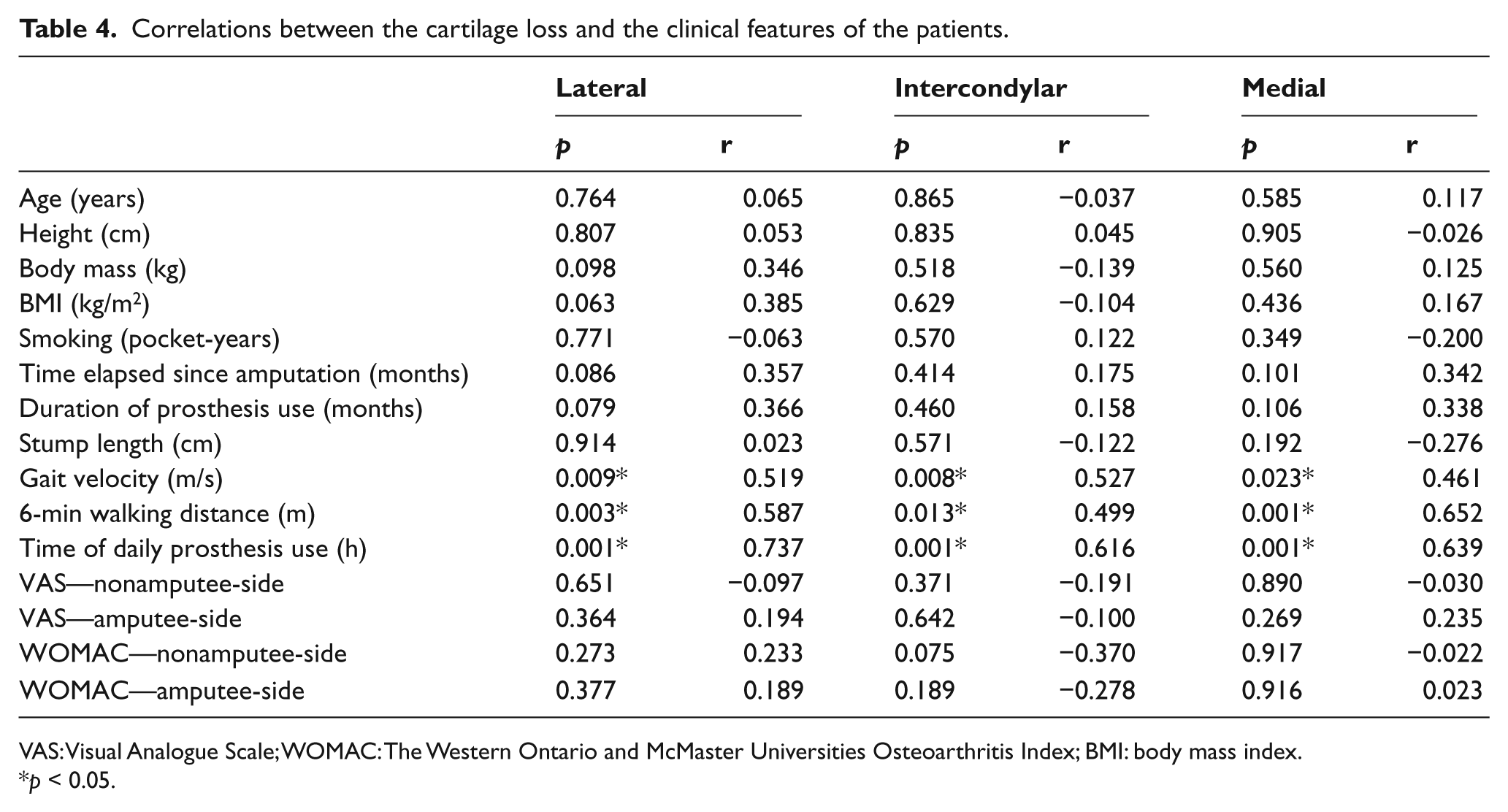
VAS: Visual Analogue Scale; WOMAC: The Western Ontario and McMaster Universities Osteoarthritis Index; BMI: body mass index.
p < 0.05.
Discussion
In this study, femoral lateral condyle and intercondylar area cartilage thicknesses were found to be significantly decreased on the amputated extremity of unilateral transtibial amputee patients. The percentage of cartilage loss on the amputee-side was positively correlated with gate velocity, 6-min walking distance, and duration of daily prosthetic use.
In one study where the authors assessed the development of hip osteoarthritis using direct radiographs, they reported the prevalence of osteoarthritis as 55% and 18% for the amputated and intact extremities, respectively (with a cut-off point of 2.5 mm articular space width and a Kellgren Lawrence grade of II). 5 In a similar study, Benichou and Wirotius 6 reported decreased hip cartilage thickness at the amputee-sides of 27 out of 53 patients with above-knee amputations. In our study, we have measured the femoral cartilage thicknesses and also found a decrease on the amputee-sides.
Despite the studies reporting increased degeneration risk and decreased cartilage thickness in the hip joint of the amputee extremity,5,6 there are also some studies reporting an increased degeneration risk in the intact extremity. 2 In a group of 78 patients with unilateral transtibial knee disarticulation or transfemoral traumatic amputation (with more than 5 years after surgery), the prevalence of hip and knee osteoarthritis in the intact extremity was 14%, and 27%, respectively. This was significantly higher compared to the general population. 2 However, the prevalence of osteoarthritis was not correlated with age, level of amputation, and time after surgery; and without identifying specific risk factors, the authors concluded in general that it would be beneficial to apply strategies for preventing osteoarthritis in that specific population. 2 Because the clinical symptoms do not always correlate with the radiographic findings, the authors used the American College of Rheumatology criteria for the diagnosis of osteoarthritis in that study. Although we could not estimate the prevalence of osteoarthritis in a similar way, we have shown that the amputee extremity is at risk of distal femoral cartilage thinning in our study. In the study reporting hip cartilage thinning in the amputated extremities of the above-knee amputee patients, a negative correlation was found between the cartilage thickness and stump length. 6 Although a significant correlation was not observed between the cartilage thickness and stump length in our study, the percentage of the cartilage loss on the amputee limb was positively correlated with gate velocity, 6-min walking distance, and daily walking time with prosthesis.
In the studies where higher risk of degenerative changes in the intact extremities were reported, the risk was attributed to the increased loading that could result from relevant biomechanical changes, for example, bouncing gait pattern with the intact extremity when the prosthesis is not in use (especially at night while urgently going to the toilet).1 –4 All the patients in the present study had prostheses, but because they had never received prompt training for walking with prosthesis before they were admitted to our center, the increased loading on the amputee extremity due to defective gait patterns might have caused cartilage thinning on the amputee-sides. The correlations between the cartilage loss in the amputee extremity with faster gait and longer prosthetic use suggest that abnormal gait patterns might increase the loading on the amputated extremity. Accordingly, despite the studies reporting a high risk of degenerative changes in the joints of the intact limbs, the femoral cartilage thinning on the amputee limbs of our patients might be attributed to the aforementioned mechanisms. 4 Although the daily hours of walking with prosthesis was asked to the patients, the gait patterns without the use of prosthesis (especially at night) were not examined in our study.
Morgenroth et al. 1 investigated the effect of prosthetic foot type on external adduction momentum in the intact knee and concluded that prosthetic feet designed to store the energy provide more foot-ankle push-off. They have mentioned that energy-storing prosthetic feet, which result in less external adduction momentum in the intact knee compared to the conventional feet, could potentially reduce the risk of knee osteoarthritis. Since feet type may affect the degeneration of the cartilage surfaces, and we have a few patients using an energy-storing prosthetic foot, only patients using SACH foot were included in our study.
There are some limitations of the present study related to US; US is a user-dependent technique, and evaluation of proximal tibial and patellar cartilage are unavailable with US. Other limitations would be as follows: first, our sample size was small mainly because of the strict exclusion criteria and enrollment of only transtibial amputees. Second, computerized gait analysis could have also been used to elucidate/quantify the association between different gait patterns and the cartilage loss of our patients. Third, daily hours of walking with prosthesis depended on self-reporting of the patients.
Conclusion
The present study revealed important results for the follow-up of unilateral transtibial amputee patients by determining the correlation of distal femoral cartilage loss with gate velocity, walking distance, and daily hours of walking with prosthesis. Moreover, although US has been previously used for the assessment of the sciatic nerves and patellar tendons of unilateral lower limb amputees,19,20 to our best knowledge, this is the first study that has evaluated the distal femoral cartilage thickness of amputee patients with this convenient imaging modality. Last but not least, future prospective and controlled studies are needed to determine the optimum gait velocity and duration of daily prosthesis use that would be most appropriate for the maintenance of knee joint cartilage in lower limb amputee patients.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.