
Abstract
Background:
People with spinal cord injury walk with a flexed trunk when using reciprocating gait orthoses for walking. Reduction in trunk flexion during ambulation has been shown to improve gait parameters for reciprocating gait orthosis users.
Objective:
The aim of this study was to investigate the effect on energy expenditure when spinal cord injury patients ambulate with an advanced reciprocating gait orthosis while wearing a thoracolumbosacral orthosis to provide trunk extension.
Study design:
Quasi experimental study.
Methods:
Four patients with spinal cord injury were fitted with an advanced reciprocating gait orthosis after completing a specific gait training program. Patients walked along a flat walkway using the advanced reciprocating gait orthosis as a control condition and also while additionally wearing a thoracolumbosacral orthosis at their self-selected walking speed. A stopwatch and a polar heart rate monitor were used to measure walking speed and heart rate.
Results:
Walking speed, the distance walked, and the physiological cost index all improved when walking with the advanced reciprocating gait orthosis/thoracolumbosacral orthosis test condition compared to walking with no thoracolumbosacral orthosis in situ.
Conclusion:
Spinal cord injury patients can improve their walking speed, walking distance, and physiological cost index when wearing a thoracolumbosacral orthosis in conjunction with an advanced reciprocating gait orthosis, which may be attributed to the trunk extension provided by the thoracolumbosacral orthosis.
Clinical relevance
It is concluded that wearing thoracolumbosacral orthosis in association with an advanced reciprocating gait orthosis could be an effective alternative in rehabilitation for thoracic level of paraplegic patients to promote their health and well-being.
Keywords
Background
Reciprocating gait orthoses (RGOs) such as the advanced reciprocating gait orthosis (ARGO) and the isocentric reciprocating gait orthosis (IRGO) are utilized to enable people with spinal cord injury (SCI) to ambulate for therapeutic purposes. The main concept of walking with RGOs is that hip flexion of one lower limb causes extension of the contralateral lower limb via a reciprocal link. Propulsive forces are provided by the trunk and upper limb muscles due to paralysis of lower limb muscles. 1
This type of orthosis therefore has an effective role in walking by SCI patients, but rejection rates have been reported as being between 46% and 54% in adults and 61% and 90% in children with myelomeningocele.2,3 This has also been attributed to high loading on the upper limb joints and excessive energy expenditure 4 due to the need to also use walking aids such as crutches and specifically designed walkers. 5
Previous studies in this field have demonstrated the positive effects of walking with RGOs. Harvey et al. 6 in a comparison between an IRGO and the Walkabout orthosis (WO) reported an improvement in walking speed and energy consumption when walking with the IRGO. The positive effects of walking with an IRGO on both walking speed and the physiological cost index (PCI) of walking have also been demonstrated when compared to a hip–knee–ankle–foot orthosis (HKAFO).7,8 Winchester et al., 9 in comparison between two types of IRGO, demonstrated that the energy costs of walking at self-selected speeds were lower with the IRGO compared to a standard RGO. With regard to postural effects, Johnson et al. 10 showed that all RGO users walk with a flexed trunk and pass a large proportion of body weight through the arms during single support. They also demonstrated that shoulder moments create trunk extension. Also Bernardi et al. 3 announced that the mechanical power required for walking causes high metabolic energy expenditure. Saha et al. 11 demonstrated that a flexed trunk position increases metabolic energy expenditure in normal subjects.
In an evaluation of the effect of a relatively extended trunk position in SCI subjects achieved by wearing a thoracolumbosacral orthosis (TLSO) when ambulating with an ARGO, Arazpour et al. 12 demonstrated that wearing an ARGO when wearing a TLSO improved walking speed and the step length of walking as compared with walking with an ARGO alone, which was attributed to the extended position of the trunk.
The main goals of using assistive devices such as crutches or walkers in conjunction with RGOs are to provide propulsion as well as increased maneuverability, independence, and providing safety and stability during ambulation. 4 However, one consequence of this is that SCI patients walk with increased trunk flexion when using RGOs and walking aids. They therefore need the height of the walking aid to be increased to a higher position than would normally be supplied to provide trunk extension if it is designed to be positioned anteriorly to their base of support. 10 Kang et al. demonstrated an improvement in walking parameters by SCI patients when using a powered gait orthosis (PGO) within parallel bars compared to ambulating with a walking aid alone. This was attributed to the fact that subjects had less trunk flexion using the parallel bars compared to using a walker with the PGO. 13
Excessive energy consumption during ambulation has been reported as an important factor in producing the high rejection rates of orthosis use documented in SCI patients. Using PGOs, which provide power to mechanical orthoses, the use of functional electrical simulation in so-called hybrid orthoses and improvement in the structure of the mechanical orthoses have been stated as being three recommended approaches in resolving this problem for people with SCI. 14 Although the improvement of energy expenditure in using a PGO 7 and hybrid orthoses has been demonstrated in the literature, 15 this study using a TLSO and an ARGO was designed to provide additional information for the development of new mechanical orthoses for people with SCI.
Changes in trunk orientation also change the moment arm between the trunk’s center of mass (COM) and the hip and shoulder joints. 10 If the trunk were to be placed in a relatively extended position, the moment arm would alter so that an upward force from the hip joint could lead to initiation of trunk extension motion. This orientation may provide prevention or reduction in upper thoracic flexion. For this aim, using a Taylor-type TLSO with shoulder straps could encourage extension of upper thoracic vertebral segments rather than when using a hyperextension orthosis (e.g. a Jewett brace). Reduction in trunk flexion during ambulation in this patient group may decrease energy consumption for RGO users. Therefore, the aim of this pilot study was to evaluate the effect of a relatively extended trunk position in SCI subjects on energy consumption and speed of walking when using an RGO.
Methods
The two test conditions were randomly selected to evaluate the effect of relative trunk extension on speed, distance of walking, and PCI when either walking with an ARGO as a control condition or walking with an ARGO/TLSO configuration. Figure 1 shows the ARGO and the TLSO designs used in this study.

SCI patient standing with the ARGO and the TLSO designs used in this study.
Subjects
Four SCI patients, all with thoracic-level injury and with either grade A or B American Spinal Injury Association (ASIA) score, participated in this study. 16 Table 1 shows information regarding the subjects who volunteered for this pilot study. Inclusion criteria included no evidence of cardiovascular problems, spasticity, contracture, obesity, or asymmetry in hip joint positions in the sagittal plane, and all participants were required to be at least 6 months post-injury to allow psychological improvement to occur prior to being included in the study. Informed consent was also obtained from volunteer patients prior to being included in the study, and the Human Ethics Committee of the University of Social Welfare and Rehabilitation Sciences gave approval to perform the study.
SCI subjects who participated in this study.
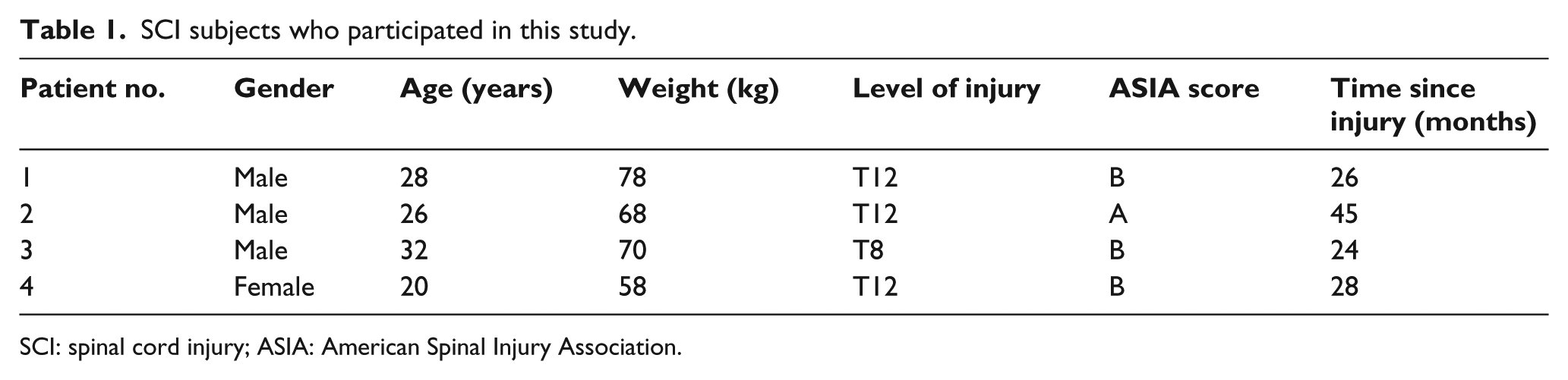
SCI: spinal cord injury; ASIA: American Spinal Injury Association.
Orthotic intervention
An ARGO (RSL Steeper, UK) was used in this study. The ARGO consisted of two knee–ankle–foot orthoses, which were connected together with a pelvic band and superstructure with right- and left-side hip joints connected together via a cable-type reciprocal link. The function of the reciprocal link is to provide flexion of the orthotic hip joint on one side with simultaneous extension of the contralateral hip joint. In this study, the ankle–foot orthoses (AFOs) incorporated in the ARGO were custom molded using plaster of Paris casts of the lower limbs for each volunteer subject, and the superstructure was adjusted and adapted to fit each patient. The AFOs incorporated dorsiflexion assist ankle joints, and a pair of drop lock knee joints connected the AFOs to the ipsilateral thigh section. 17 All patients walked without shoes. A 25-cm heel lift with nonslip finish was added to heel area of all AFOs to replicate the pitch of a shoe with a 25-mm heel.
The TLSO used in this study was a Taylor-type off-the-shelf orthosis (Tynor Orthotics Pvt Ltd, India) manufactured from aluminum with 4-mm-thick uprights and soft neoprene lining with an anterior abdominal pad. The ARGO was measured to fit over the top of the brace. The brace had limited bulk, which meant that the ARGO was also suitable to be worn without the TLSO by adjusting the straps. The patients were all able to bend forward enough to move the walking frame forward when wearing the TLSO encapsulated by the ARGO.
Orthotic gait training
Depending on the level of injury all subjects received between 6 and 8 weeks experience of gait training prior to gait analysis. This comprised five 2-h sessions per week with the orthosis. They walked with the ARGO for half of the time in each session and with the ARGO/TLSO during the rest of the time. The orthotic gait training program consisted of donning and doffing of the orthoses, passive stretching of the lower extremities, upper limb strengthening, balancing in a standing position, and walking training on regular flat surfaces. All gait training was done by an expert physiotherapist experienced in training walking and standing in paraplegic patients. Orthotic gait training with the orthosis was completed prior to performing the trials for this study to ensure that each SCI subject could walk with the ARGO and the ARGO/TLSO independently without falling when walking with the aid of a walking frame.
Experimental approach
To provide information to evaluate PCI, a Polar Heart Rate monitor was used.7,8 To calculate the PCI using this approach, the heart rate at steady-state walking (HRss) and the heart rate at rest (HRar) were measured. The following formula was used to measure the PCI

To obtain a baseline level of PCI, subjects sat for 10 min prior to any measurement. The approach used for PCI measurement consisted of 5 min of complete rest in a sitting position, 5 min in a standing position, walking with the orthosis for 6 min at their self-selected walking speed, and a final 2 min of rest in the seated position. During resting, standing, and walking, the heart rate was calculated every 15 s. After 10 min of rest in the sitting position with the alternative test condition donned, the next evaluation and measurement was started. The mean heart rate during the final 2 min of rest in the sitting position was considered as HRar and average heart rate after 6 min of walking with the orthosis was considered as the HRss.
Subjects were asked to walk using two types of orthosis condition (walking with an ARGO as a control condition or walking with ARGO/TLSO in a randomized order, along a pre-determined 40-m rectangular walkway at their self-selected speed). To calculate the velocity, the interval between the starting and stopping time was used. Velocity (V) was calculated by measuring walking distance and time using a 6-min walking test (6MWT), using a stopwatch, and the distance walked being measured by a meter. All participants with SCI had same conditions during the walking tests, and the positive and negative accelerations at the start and end of the tests were not considered. Three trials were used for each condition and subject. The two test conditions were randomly selected (A = wearing ARGO, B = wearing ARGO/TLSO).
Data analysis
Considering small sample size, nonparametric statistical method was used for analysis. According to this point, a Wilcoxon signed-rank test was used for analyzing the effects and differences in the selected outcome measures between the two conditions. SPSS statistical software version 16.0 (SPSS Inc., USA) was used for analysis of data. The level of significance was set at 0.05.
Results
The mean ± standard deviation (SD) of PCI, distance, time, HRss, and HRar during the two conditions (walking with an ARGO as a control condition or walking with ARGO/TLSO) is demonstrated in Table 2.
Comparison of speed of walking, distance walked, and PCI during the two conditions.
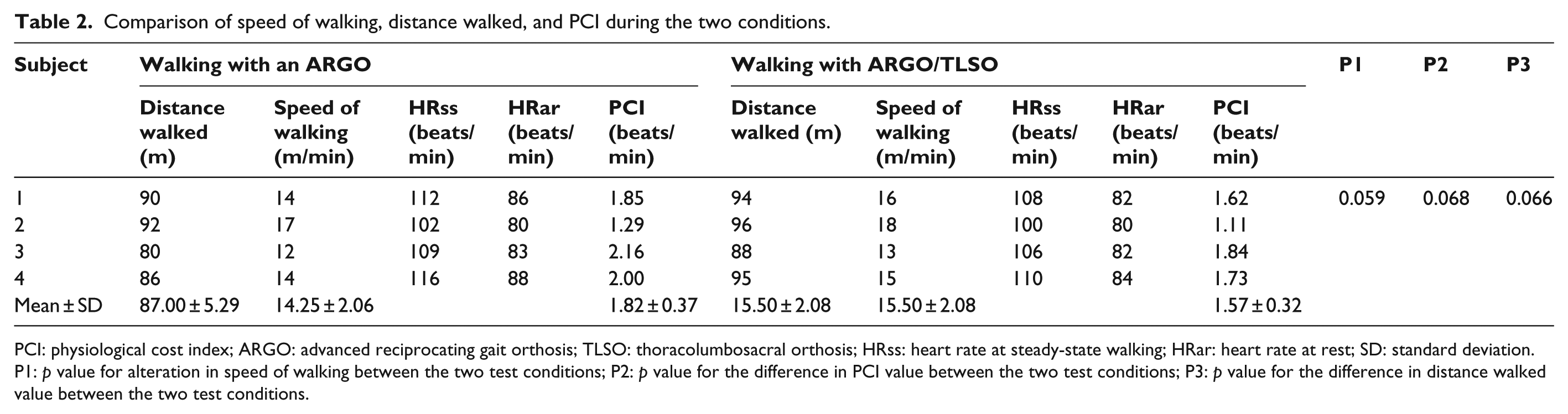
PCI: physiological cost index; ARGO: advanced reciprocating gait orthosis; TLSO: thoracolumbosacral orthosis; HRss: heart rate at steady-state walking; HRar: heart rate at rest; SD: standard deviation.
P1: p value for alteration in speed of walking between the two test conditions; P2: p value for the difference in PCI value between the two test conditions; P3: p value for the difference in distance walked value between the two test conditions.
There was no statistically significant difference between orthotic walking conditions (p = 0.059) in speed of walking, but walking with the ARGO/TLSO improved the speed of walking as compared to walking with an ARGO as a control condition (Table 2). Similar to speed of walking, there was no statistically significant difference in the total distance walked between the orthotic test conditions (p = 0.066), but wearing the ARGO/TLSO improved the distance walked as compared to an ARGO (Table 2). Table 2 shows that here was also no statistically significant difference between orthotic walking conditions in PCI values (p = 0.068).
Discussion
This study provides the first comparison of the effect of relative trunk extension on walking speed, maximum distance walked during a 6MWT, and energy consumption during ambulation with lower extremity orthotic intervention in a SCI patient population. It has previously been shown that SCI subjects walk with trunk flexion with assistive devices during ambulation, and that an extended trunk position as evidenced by the kinematic data positively influences the function of the reciprocal link in an RGO. 10 This study has shown that trunk extension can be provided by an RGO mechanism and extension of the proximal superstructure via a TLSO, which improved temporal spatial parameters of gait.
Speed of walking, high-energy consumption, and high loads on upper limb joints (e.g. shoulder and wrist) have been demonstrated as being the main reasons for orthotic rejection in SCI patients.1,4 This type of intervention was originally used as a means of providing exercise and rehabilitation. 18 Any means of providing an improvement in walking speed or reduction in the energy expenditure and loads on upper limb joints could theoretically provide increased orthosis usage rates by SCI patients.
The rate of energy expenditure in this study when using the TLSO was improved when compared to the ARGO in isolation as the control orthosis. When walking with the ARGO, the SCI patients used additional energy in extending the trunk to bring the center of gravity of the trunk over the base of support for stability. This undesirable standing posture may cause undesirable effect on the joints in the long term. With the ARGO/TLSO, the SCI patients achieved a more upright posture through trunk support. When comparing the results of this study with previous studies which have evaluated only mechanical orthoses (e.g. the IRGO and hip guidance orthosis (HGO)), the mean of the energy consumption demonstrated in this study was comparable with other previous studies on SCI patients. 4
Both the speed and distance walked with the ARGO was low as compared to walking with the ARGO/TLSO test condition. A flexed trunk position when also associated with paralysis of lower limb muscles may be the cause of low walking speeds demonstrated when using an ARGO without an extended trunk position. 12 The average gait velocity and energy consumption have been demonstrated as being 1.28 m/s and 0.176 mL/kg/m, respectively, in healthy subjects, 19 while the mean of these parameters were reported between 0.2 and 0.3 m/s with an energy consumption of 1.0 mL/kg/m with RGOs in SCI patients.2,3
The sagittal plane position and orientation of the lumbar and thoracic portions of the spine within an orthosis are the important factors in providing improvement in walking speed and reduction in energy consumption in SCI patients. Harvey et al. 6 in a comparison between the WO (which does not have a rigid structure at lumbar level) and the IRGO demonstrated lower walking speeds and increased PCI in SCI patients when walking with the WO. Arazpour et al. in using ARGO/TLSO reported improvement in gait parameters compared to walking with ARGO as control condition. They did not evaluate energy consumption but demonstrated an improvement in gait parameters when also wearing a TLSO. 12
Improvement in the mechanical design of orthoses has been recommended to provide the optimal orthoses for walking by SCI patients. 4 Since extension of the trunk provided improvement in gait parameters and energy consumption in SCI patients in this study, the design and construction of an ARGO incorporating an adjustable and movable trunk supporter will be beneficial in this field. It has been shown that advanced mechanical orthoses such as the IRGO can improve the speed and distance of walking when compared to HKAFOs. 8 The use of powered orthoses has also been shown to improve gait parameters and energy consumption of walking in SCI patients compared to mechanical orthoses. 20 The results of this pilot study gave the research team confidence to extend this research in a future study by designing and constructing a new orthosis for SCI patients based on the results of this study and a previous study by Arazpour et al., 12 by fabrication of an ARGO with an adjustable and removable lumbar section that provides trunk extension and limits flexion of the spine.
Johnson et al. 10 reported that trunk flexion increases energy expenditure and that an extended posture could increase the hip flexion moment during swing through action of reciprocal link, but they did not evaluate energy expenditure with the trunk in an extended position. Dall et al. 21 demonstrated that patients who use RGOs do not use its mechanism to its full potential because they should extend the trunk to effectively activate the reciprocating mechanism, but most of them walk with the trunk in flexion. Bernardi et al. 3 announced that because the mechanism does not activate with the trunk in a flexed posture, some new mechanism should be designed.
The PCI is a measure of alteration of heart rate (beats/min) during exercise. 22 It has a good linear relationship between the heart rate and oxygen uptake 23 and has been used as a reliable measure of the energy cost during ambulation among healthy and SCI patients.24,25
Energy expenditure has historically been measured by different methods: energy consumption (the amount of oxygen consumed per time traveled), energy cost (the amount of oxygen consumed per distance traveled), and PCI (the difference between walking and resting pulse per gait speed). Previous studies have stated that in patients with slow walking and high-energy expenditure, energy cost and energy consumption are not clinically significant. 4 However, PCI has been introduced as a sensitive tool for detecting small but significant differences. PCI was introduced as a proxy index for oxygen cost, so the results of studies which use PCI for SCI patients are more valid in energy expenditure. Previous studies in this field have demonstrated that SCI patients walk with their trunk in a flexed position during orthosis use.10,12 They proposed that trunk extension may improve energy consumption in these patients. Wearing a TLSO with an ARGO to provide trunk extension improved energy consumption compared to wearing an ARGO alone in SCI patients in this study.
Depending on the amount of flexion and the resultant position of the trunk, SCI subjects experience high loads through the upper extremity when walking with RGOs. 10 The shoulder joint force was not evaluated in this study. Evaluation of this parameter and shoulder joints muscle activity and latissimus dorsi muscle activity will be beneficial in a future study.
One limitation of this study relates to the small sample population. Another limitation of this study was the actual patient population. Participants in this study presented different levels of injury. These levels of injury provided different levels of motor power and sensation, different passive range of motions (ROMs) of the joints, and varying degrees of spasticity. Further research is needed regarding a simultaneous evaluation of the effect of trunk position in walking with RGOs on loading levels of the upper limbs, especially the shoulder joints, in the anterior–posterior and vertical directions. If trunk extension can be assisted in a novel way when ambulating with RGOs, it will prove beneficial for the rehabilitation of SCI patients.
Conclusion
In this study, we investigated the PCI during orthotic walking with an ARGO and TLSO in a small-sample-sized study and showed that paraplegic patients could walk at relatively higher speed and lower energy consumption compared with the ARGO alone.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material was based on the work supported by the Deputy of Research and Technology of Mazandaran University of Medical Sciences (grant no. 677).