
Abstract
Objective: The objective of this study was to compare the Physiological Cost Index of walking with a reciprocating gait orthosis to that of walking with bilateral knee-ankle-foot orthoses (KAFOs) by subjects with paraplegia resulting from T12 – L1 spinal cord lesions.
Methodology: Six chronic paraplegic subjects who had T12 – L1 spinal cord lesions and who previously wore bilateral KAFOs were recruited. Each subject was fitted with an isocentric reciprocating gait orthosis (IRGO) and received a standardized training program. Subjects were then asked to walk using the two orthotic devices along a 40 m rectangular pathway at a speed that was comfortable for them. The walking speed was measured using a stop watch, and a Polar Heart Rate Monitor was used to measure the heart rate of the subjects. The Physiological Cost Index (PCI) was calculated for comparison.
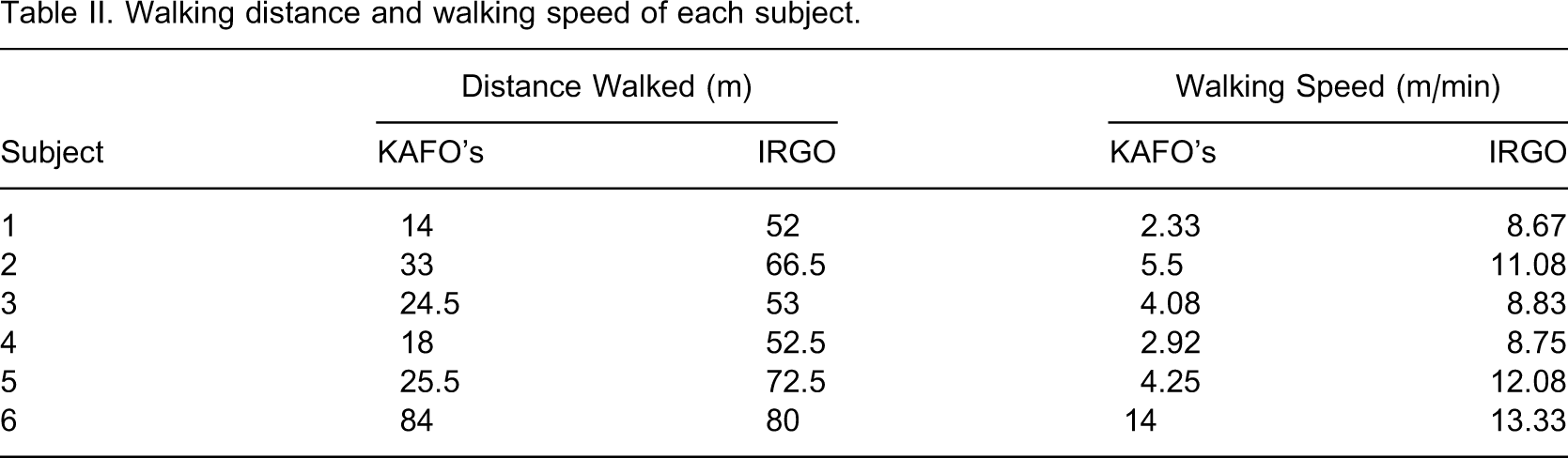
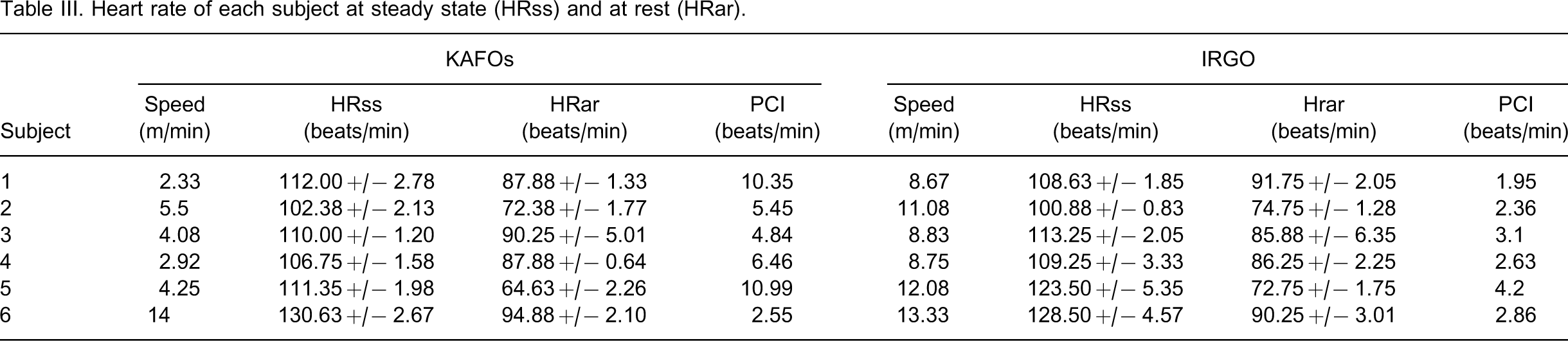
Results: Ambulation using the IRGO (10.46 +/− 2.00 m/min) was significantly faster (p = 0.009) than ambulation using the bilateral KAFOs (5.51 +/− 4.30 m/min). The PCI demonstrated when walking with the IRGO (2.85 +/− 0.77 beats/m) was significantly lower (p = 0.0306) than that of the bilateral KAFOs (6.77 +/− 3.28 beats/m).
Conclusion: Paraplegic patients with T12 – L1 spinal cord lesions walk faster and more efficiently using the isocentric reciprocating gait orthosis as compared to using the bilateral KAFOs.
Keywords
Introduction
Spinal cord injury is one of the most traumatic and disabling orthopaedic conditions. Most of the patients diagnosed with a significant spinal cord injury are confined to a wheelchair for the most part of their lives. Aside from a significant loss of sensory and motor functions below the level of lesion, paraplegic subjects may also experience medical complications such as spasticity, joint contractures, pressure sores, osteoporosis and urinary tract infections.1,2 Some 95% of these subjects usually suffer from at least one secondary complication, and 58% have three or more complications.3,4 In order to improve the physiological and psychological well-being of such patients, they are encouraged to resume their ability to stand or walk in some way.5 Physiologically, standing and walking can prevent joint contractures, improve urinary and bowel function, reduce spasticity, and decrease the incidence of pressure sores.6 Likewise, patients can generally improve psychologically. As alternatives to the tilt-table and other upright mobility devices, several orthotic devices have been developed to allow patients to stand or walk with the assistance of walking aids. The selection of appropriate devices and the physiological intensity of the corresponding orthotic gait depends on the level and severity of the spinal cord lesion.7,8 Despite the fact that orthotic ambulation is not, for the most part, a functional replacement of wheelchair mobility, regular walking exercise is encouraged among patients with paraplegia.
Patients with complete T10 – L1 lesions have paralysis of their lower extremities. There is lack of voluntary control of the hip, knee and ankle joints. The most common orthotic intervention is the bilateral knee-ankle-foot orthoses (KAFOs). A pelvic band with bilateral orthotic hip joints may also be included to alter the structure as bilateral hip-knee-ankle-foot orthoses (HKAFOs). When KAFOs or HKAFOs are worn, the knees are locked in full extension and the ankles are in neutral position. Using their trunk muscles, these patients have the options to walk with conventional orthoses and crutches using reciprocating gait pattern. Since much effort is needed to involve alternative flexion and extension of the uncontrolled hip joints, the induced reciprocating gait is slow. The patients usually walk with swing through gait for a faster speed. However, this swing-through gait still results in very high energy consumption, and the upper extremities become heavily loaded. The long-term utilization of bilateral KAFOs or HKAFOs among patients with T10 – L1 lesions is therefore rare, usually lasting for less than 6 months;9,10 thus decreasing the degree of mobility and other beneficial effects of standing and walking.
A reciprocating gait orthosis allows one leg to be placed ahead of the other during walking to simulate a reciprocal walking gait. It is more often prescribed for patients with higher lesions. The trunk muscles of these patients are severely impaired. They require the trunk section of the reciprocating orthosis to support and stabilize their trunk during walking. The reciprocal walking gait pattern requires less effort to ambulate compared to the swing through gait, which is facilitated by the conventional orthosis. The swing through gait performed with bilateral KAFOs was thus compared with the reciprocating gait orthosis in this study. Among the various designs, the Isocentric Reciprocating Gait Orthosis (IRGO) is more energy efficient.11 It consists of a trunk section and a push-pull rod (rocker bar) which extends from two KAFOs to connect the lateral hip joints. This mechanism allows the transfer of energy from one leg to the other during the weight shifting process.12 Flexion of one hip causes a reciprocal hip extension of the opposite limb. With proper bracing of the trunk and hips, and the application of additional stiffness of the lateral uprights, a reciprocating gait orthosis can provide a firm support to patients so that they can stand without the use of crutches or walkers. Their hands then become free to perform other activities while standing.13 However, a pair of elbow crutches is normally required for walking. The gait performance of various orthoses, including reciprocating gait orthoses, among patients with paraplegia has been studied. Compared with other orthotic devices, the Isocentric Reciprocating Gait Orthosis (IRGO) is more energy efficient.11
The most commonly damaged lower level spinal cord region is T12 – L1.14 Paraplegic patients with lesions at this level are commonly prescribed bilateral KAFOs. In a similar manner as subjects with higher lesions at T10 – L1 level, they do not ambulate efficiently. In order to improve their gait efficiency and thus to encourage the long-term utilization the use of an IRGO would therefore seem appropriate, However, there is limited evidence in the literature which details a comparison of gait performance of patients with spinal cord lesions at the T12 – L1 level when using either bilateral KAFOs or an IRGO.
The Physiological Cost Index (PCI)15 is a measure of change of heart rate (beats/min) during exercise. It has a good linear relationship between the heart rate and O2 uptake,16 and has been used as a reliable measure of the energy cost during walking among healthy subjects17 or those with spinal cord lesions at or below T3 level.18 It is assumed that the use of IRGO in this patient group would improve their gait efficiency and subsequently encourage the long term utilization of the walking device. The objective of this study is to compare the PCI of paraplegic patients with spinal cord lesions at the T12 – L1 level whilst ambulating either with bilateral knee-ankle-foot orthoses or an isocentric reciprocating gait orthosis.
Methodology
Subjects
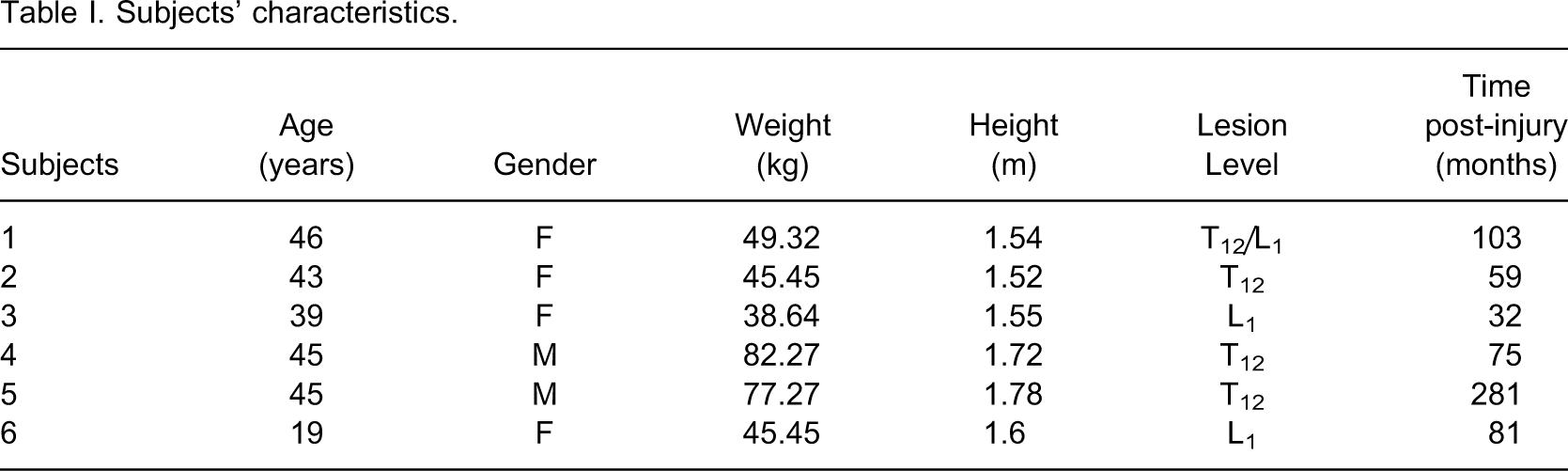
Subjects were included in the study if they were adult paraplegics as a result of complete T12 – L1 lesions. They were all experienced bilateral KAFOs users with normal upper limb strength. The subjects were assessed and referred by physicians who also confirmed that the subjects were physically fit for intensive orthotic training. Each subject was then fitted with an IRGO, which consisted of a pelvic or trunk section and a rocker bar that extended from two KAFOs to connect the lateral hip joints. Subjects with known cardiovascular or pulmonary diseases, contractures, severe spasticity, obesity, or asymmetric hip positions were excluded from the study. Written consent was obtained from each subject before testing. The study was approved by the Human Subject Ethics Committee of The Hong Kong Polytechnic University and the Research and Development Committee of the MacLehose Medical Rehabilitation Centre.
Training
All subjects were given an 8-week standardized training program after measurements for the fitting of IRGO had been taken. There were three sessions per week. Each session was 2 h long. The contents of the program included passive stretching of the lower extremities, upper limb strengthening exercises, balance training in the standing position, gait training and functional skills training (such as donning and doffing of the orthosis, sit to stand training and kerb climbing). The subjects were then fitted with the orthoses and four specific skills were taught in order to initiate an efficient locomotion whilst walking with the IRGO. These were diagonal weight transfer, hip and trunk extension, pushing down on the hands, and kick through of the legs. This second training session lasted for eight weeks and was performed three times per week.
Experimental procedures
The Polar Heart Rate Monitor, with a chest electrode attached to the subject's chest region, was used to acquire data to calculate the Physiological Cost Index (PCI). This was achieved by using the following formula:

Subjects were asked to walk using two orthotic devices in random order, bilateral KAFOs and an IRGO, along a pre-determined 40 m rectangular pathway at a speed that was comfortable for the subject. At the beginning of each walking trial, each subject was instructed to sit for 10 min for calming down to baseline levels before the PCI measurement. The PCI measurement procedure consisted of a 5-min period of quiet rest while sitting, 5 min of static standing, 6 min of walking at a speed that was comfortable to the subject, and a final 2-min period of rest in sitting position. Heart rate was recorded every 15 sec throughout the entire measurement period. A new trial was then started following a 10-min sitting period. The average heart rate during the last 2 min of: (i) sitting, and (ii) 6-min walking were calculated as (a) the heart rate at rest (HRar) and (b) heart rate at steady state (HRss), respectively, for analysis.
Statistical analysis
The data collected for the two orthotic conditions were averaged for the calculation of Physiological Cost Index (PCI). All relevant data were analyzed using two-tailed paired t-tests. A 95% level of confidence was considered statistically significant.
Results
Subjects' characteristics
Walking distance and walking speed of each subject
Heart rate of each subject at steady state (HRss) and at rest (HRar)
Discussion
The paraplegic subjects tested with low thoracic lesions were unable to maintain their hip function when walking with bilateral KAFOs, and required considerable effort to ambulate using a tiring swing-through gait. The situation was improved with faster walking speeds and lower PCIs when subjects walked using an IRGO. In this study, five out of the six subjects walked more efficiently when they used an IRGO. The remaining subject walked very quickly but with similar speeds in both the bilateral KAFO and IRGO conditions (14 m/min vs. 13.33 m/min respectively). This subject was relatively young (19 years old) and her injury occurred at around the age of 12. She had studied in a special school for five years and had been trained and encouraged to walk with bilateral KAFOs in the school environment daily. She walked with similar speed in both bilateral KAFOs and IRGO conditions after the eight-week IRGO training period. Since the patient was relative young, her walking performance might also be improved after intensive practice with the IRGO. Moreover, the intensive training at her early age might also be the reason of her outstanding walking performance comparing with other tested subjects.
Direct measurement of heart rate was used to indicate the amount of physical effort exerted when walking with the two test conditions.20 With bilateral KAFOs the subjects use additional energy in extending the trunk and hips to bring the trunk's center of gravity over the base of support for stability. This undesirable standing posture may also bring about undesirable effects on the joints in the long term. With the IRGO, the subjects achieve an upright posture through trunk support and controlled hip movement. However, no significant difference was found in the static standing heart rate among the two orthotic conditions (Table III).
In this study, the results of the PCI measurement showed that patients with T12 - L1 spinal cord lesions walk faster and more efficient using the IRGO. The IRGO gait performance of these subjects might further improve when they will have more experience with the orthosis. Besides walking, the orthotic intervention facilitated them to achieve other functional tasks as they will be able to utilize their hands when they stand with the orthosis. These will encourage the long term usage of the walking device and will bring more positive effect to the rehabilitation of these subjects.
Not only does the reciprocating gait pattern offered by the rocker bar linking the hip joints in the IRGO result in reduced energy consumption when walking; its rigid structure also supports and stabilizes the lower trunk and the lower limbs during static standing. The weight of an IRGO is approximately 6 kg whilst that for two KAFOs is 4 kg. Even though it has been claimed that the weight of a reciprocating gait orthosis has little or no influence on the patients' walking on level ground,21 an alternative design using materials with higher strength to weight ratios should be developed to enhance the utilization of the orthoses and thus improve the quality of life of the patient needing this orthotic service. In addition to experimental or laboratory measurements, information such as frequency of use and performance in the home and office environment, as well as other evaluation instruments such as the Spinal Cord Independence Measure22 should be considered in the functional evaluation process.
Conclusion
Six chronic paraplegic subjects, with T12 – L1 spinal cord lesions participated in gait evaluation whilst walking with bilateral KAFOs and IRGO interventions. The walking speed was faster and the Physiological Cost Index lower when the subjects walked with IRGO. In conclusion, patients with T12 – L1 spinal cord lesions walk faster and more efficiently using a reciprocating gait orthosis and its use should therefore be encouraged for the appropriate subjects.