
Abstract
Background:
Mechanical orthoses are used for standing and walking after neurological injury. Most orthoses such as the advanced reciprocating gait orthosis typically use solid ankle–foot orthoses.
Objectives:
The goal of this study was to test the effects of ankle dorsiflexion assistance in patients with spinal cord injury when ambulating with an advanced reciprocating gait orthosis compared to walking with fixed ankles.
Study Design:
Quasi-experimental.
Methods:
Four patients with spinal cord injury were fitted with an advanced reciprocating gait orthosis equipped with solid and dorsiflexion assist-type ankle–foot orthoses and walked at their self-selected speed. Joint angles and spatial–temporal parameters were measured and analyzed.
Results:
The mean walking speed and stride length were both significantly increased along with cadence by the volunteer subjects when ambulating using the advanced reciprocating gait orthosis fitted with dorsiflexion assist ankle–foot orthoses compared to the advanced reciprocating gait orthosis with solid ankle–foot orthoses. The mean ankle joint ranges of motion were significantly increased when walking with the advanced reciprocating gait orthosis with dorsiflexion assist ankle–foot orthoses compared to when using the advanced reciprocating gait orthosis with the solid ankle–foot orthoses. Knee joint ranges of motion were reduced, and hip joint ranges of motion were increased but not significantly.
Conclusion:
The advanced reciprocating gait orthosis fitted with the dorsiflexion assist ankle–foot orthoses had the effect of improving gait parameters when compared to the advanced reciprocating gait orthosis with solid ankle–foot orthoses.
Clinical relevance
The advanced reciprocating gait orthosis with dorsiflexion assist ankle–foot orthoses has the potential to improve hip and ankle joint kinematics and the temporal–spatial parameters of gait in spinal cord injury patients’ walking.
Keywords
Background
Spinal cord injury (SCI) is one of the injuries of the nervous system that can cause dysfunction, as well as loss of both sensation and motor performance.1,2 SCI usually occurs in young healthy adults (aged between 16 and 30 years) due to trauma.3,4 Approximately 253,000 patients with SCI existed in 2006 in the United States, and there are an additional 11,000 new cases each year. 4 In addition, approximately 300–400 new cases of SCI are added annually to the total SCI population of about 10,000 cases in Australia. 3
The ability to walk is the ultimate goal of rehabilitation in SCI patients. 5 However, walking is usually affected in patients with SCI according to the lesion level and the resulting different levels of muscle paralysis, sensory impairment, spasticity, and the lack of trunk control.6,7 The lack of active flexion and extension in the hip and knee joints, excessive ankle plantarflexion during swing phase, and an inability to properly position the lower limb for initial foot contact and the existence of so-called “foot slap” based on paralysis of ankle dorsiflexor muscles are commonly seen gait anomalies in patients with SCI.8,9 SCI patients typically exhibit slow, asymmetrical walking patterns due to lack of coordination over a wide base of support.8,10 The use of mechanical orthoses is therefore a prescribed approach for patients with SCI for standing and walking purposes.11–16
The advanced reciprocating gait orthosis (ARGO) 15 and the isocentric reciprocating gait orthosis (IRGO) 14 are both examples of orthoses that are used for walking purposes by this group of patients. The positive effects of these orthoses have been reported in previous studies.11,12 Each of these orthoses can passively assist the patient’s lower limbs by guiding them with a straight leg walking pattern while allowing the hip joints to move. However, since both knee joints are locked in extension and the ankles are usually supported in solid ankle–foot orthoses (AFOs), which also blocks ankle motion, the gait is inefficient.
Some advancements have been recently made in an attempt to provide sagittal plane ankle motion within reciprocating gait orthoses (RGOs). Genda et al. 17 developed the hip–ankle-linked orthosis (HALO), which connected the orthotic ankle joints to the orthotic hip joints to swing the limbs during walking. Evaluation of this orthosis demonstrated that ankle joint motion provided a stable gait pattern by utilizing a dorsiflexion movement to swing the contralateral lower limb. However, use of this orthosis showed no significant differences in stride length when compared to an alternative design (the Primewalk orthosis), but the HALO was more effective than the Primewalk orthosis in improving cadence and the speed of walking. 17 Yano et al. 18 developed a weight-bearing control orthosis (WBCO) that utilized reciprocal guide assistance and movable foot plates. This new orthosis provided swing of the lower leg and prepared a clearance between the sole of the shoes and the floor for more effective ambulation. 18 Evaluation of the WBCO demonstrated that paraplegic patients using WBCO could walk with a higher speed when compared with those using conventional orthoses, with similar energy expenditure. 19 Sawicki et al. 20 developed a powered AFO, which demonstrated that SCI patients experienced improved muscle activation patterns and more effective kinematics when ambulating.
Although these new versions of mechanical orthoses have been developed to improve paraplegic patient gait by inducing ankle motion, these orthosis are not available commercially and their use has been limited to the laboratory setting. A more thorough understanding of how mechanical movement of ankle joints by orthoses could alter the spatial–temporal parameters and the kinematics of walking by patients with SCI is therefore important for development of more effective orthoses.
The ankle joint has a critical role in facilitating effective propulsion during ambulation. In parallel with muscles crossing the hip or knee joints, the plantarflexor muscles acting at the ankle joint provide a high percentage of the work done during gait.21,22 The muscles around the ankle joint move the center of mass forward during push-off23,24 and decrease energy loss at heel strike by positioning the ankle effectively prior to ground contact. 25 In addition, afferent feedback from the ankle joint is critical to the control of walking and changes the motor output of spinal motor neurons by rhythmic limb loading.26–28 Based on these important effects, control of walking while also providing movement in the ankle joint during walking with mechanical RGOs may also be important.
To the authors’ knowledge, evaluation of the effect of AFOs with articulating ankle joints in association with RGOs during walking on lower limb kinematics and spatial–temporal patterns of patients with SCI has not been performed. The aim of this study was therefore to evaluate the effect of an ARGO utilizing the usual bilateral solid AFO versus the same orthosis fitted with AFOs offering a dorsiflexion assist function on the spatial–temporal parameters and the sagittal plane kinematic patterns of walking in patients with SCI.
Methods
Subjects
Four paraplegic patients with injuries at the thoracic level participated in this study (Table 1). The patients were evaluated and referred by physicians who also confirmed that the patients were physically fit for gait training with an orthosis. Each patient was then fitted with an ARGO with two types of AFO. Patients either had complete (grade A) or incomplete motor paralysis (grade B) in the lower limb muscles based on the American Spinal Injury Association (ASIA) score. 29 Inclusion criteria for participation in this study were as follows: patients with no history of cardiovascular or pulmonary diseases, contractures, severe spasticity, obesity, or asymmetric hip positions and who were at least at 6 months post injury. Patient information is reported in Table 1. All patients had undergone at least 6 weeks of orthotic gait training using the ARGO with two types of AFO as the basic rehabilitation process. Each patient gave written informed consent for the experimental procedure, which was approved by the ethics committee of the University of Social Welfare and Rehabilitation Science (USWR).
Subjects’ characteristics.
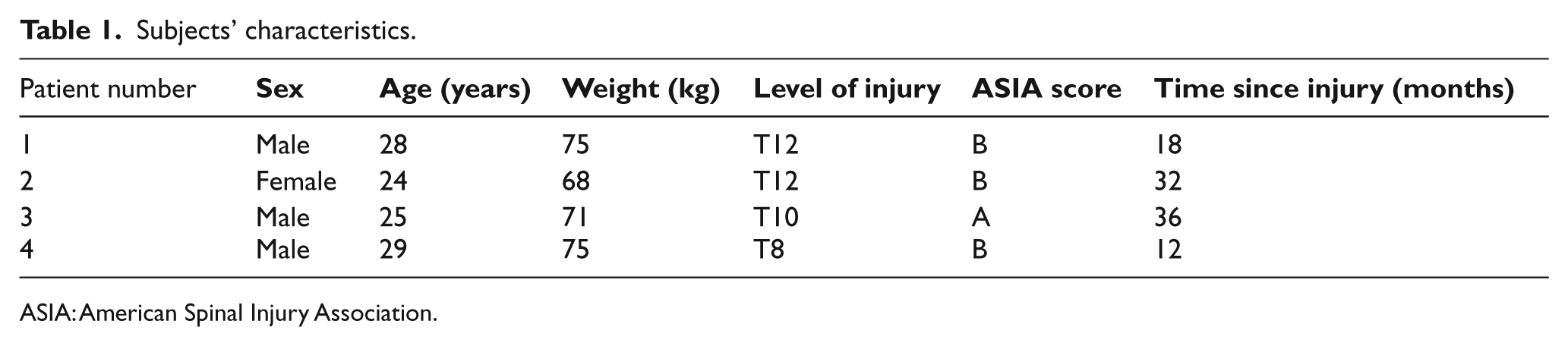
ASIA: American Spinal Injury Association.
Orthotic gait training
Figure 1 shows the advanced reciprocal gait orthosis used in this study. The ARGO has a single cable, which connects both sides of the lower leg frame. With this device, a torque exerted by one hip joint is mechanically translated to the other hip joint, which applies torque in the direction opposite to it. Gait training with the orthoses was variable (between 6 and 10 weeks) according to the level of injury in these patients. The gait training program included strengthening of the upper body muscle; transferring, donning, and doffing of the orthosis; balancing in a standing position; and walking training on regular surfaces. On completion of the gait training with the orthoses, each patient could walk with either orthosis independently without falling. All patients participated in a same-day walking trial using three-dimensional motion analysis using the Vicon system when walking with the orthoses.
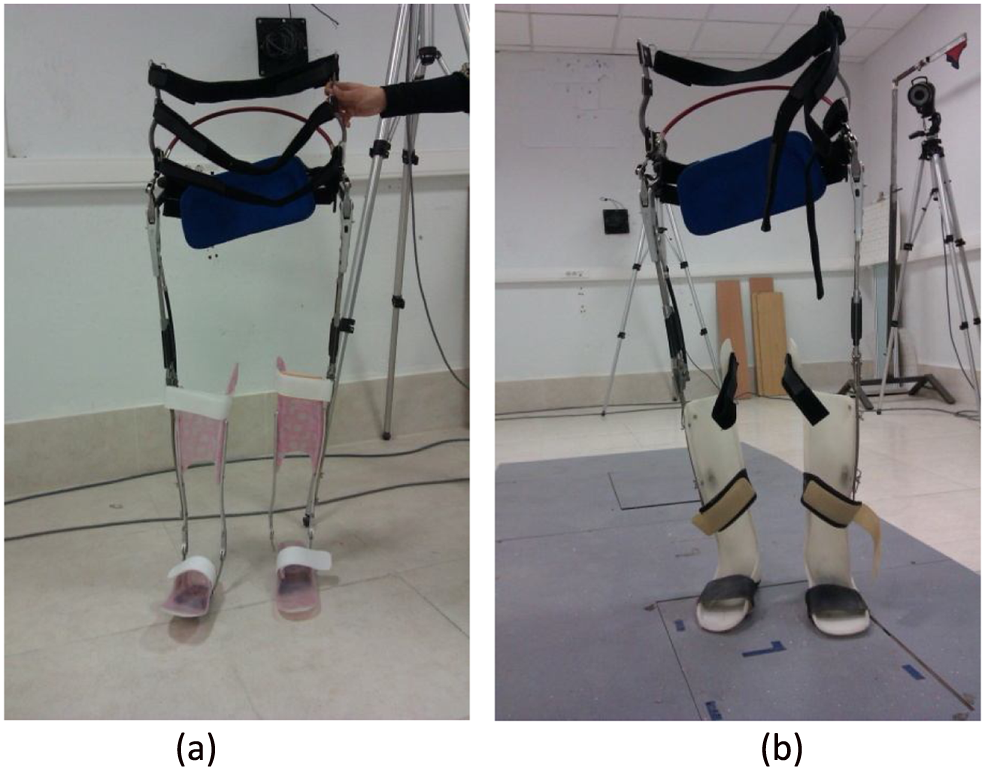
The advanced reciprocal gait orthoses used in this study. (a) ARGO with dorsiflexion assist AFO and (b) ARGO with solid AFO.
Motion analysis
The patients walked with the orthoses along a 6-m walkway in a biomechanics laboratory at least five times at a self-selected walking speed in two test conditions, that is, when wearing each of the two mechanical orthoses (the ARGO with solid AFOs, or the ARGO with AFOs incorporating dorsiflexion assist ankle joints) while using a walking frame (walker) with the wheels anteriorly positioned. The patients walked with the orthoses without shoes. A 1-inch heel lift with a nonslip finish was added to heel area of all the AFOs to replicate the pitch of a shoe with a 1-inch heel. There were no problems experienced with slippage during the walking trials.
Gait was evaluated by a Vicon digital motion capture system (Oxford Metrics, UK, 640 pixels), using six cameras (Vicon, Infrared) at a frequency of 100 Hz and two force platforms set apart and positioned to capture a left and right heel strike (Kistler 9286BA, Switzerland). A total of 18 markers were used at the following positions: bilaterally over the position of the greater trochanter, the lateral condyle of the femur, the head and lateral malleolus of the fibula, the second metatarsal, anterior superior iliac spine (ASIS), calcaneus, and over the jugular notch, the spinous process of the seventh cervical vertebrae, and the acromioclavicular joints. The markers were put on the trunk of the patients and on the orthosis as close as possible to the positions where they would be located on the patient’s skin. The marker set used was intended to measure sagittal plane movements only, and the acquired data were analyzed using MATLAB (MathWorks, Natick, MA) to compute joint angles and spatial–temporal parameters.
Ten-step cycles were selected for analysis. The cadence, stride length, speed of walking, and hip, knee, and ankle joint ranges of motion (ROMs) were analyzed from the motion analysis data. Data were averaged for both sides.
Data analysis
Normality of the data was confirmed by using the Kolmogorov–Smirnov technique. According to the normality of the data, a paired t-test was used to analyze the effects and differences in the selected outcome measures between the two orthoses. SPSS statistical software was used for analysis of the data. The level of significance was set at 0.05.
Results
Spatial–temporal gait parameters
As shown in Table 2, the mean of speed of walking with the ARGO fitted with the dorsiflexion assist AFOs (0.35 ± 0.01 m/s) was significantly higher (p = 0.012) than that with the ARGO with solid AFOs (0.32 ± 0.02 m/s). The mean cadence was also increased with the ARGO with dorsiflexion assist AFOs, but this did not reach significance (p = 0.058). The stride length was significantly longer (p = 0.002) with ARGO with dorsiflexion assist AFOs (100 ± 9.48 cm) as compared to the ARGO with solid AFOs (94.50 ± 9.25 cm).
Mean ± SD of hip, knee, and ankle joints ROM and spatial–temporal gait parameters in walking with two types of ARGO.
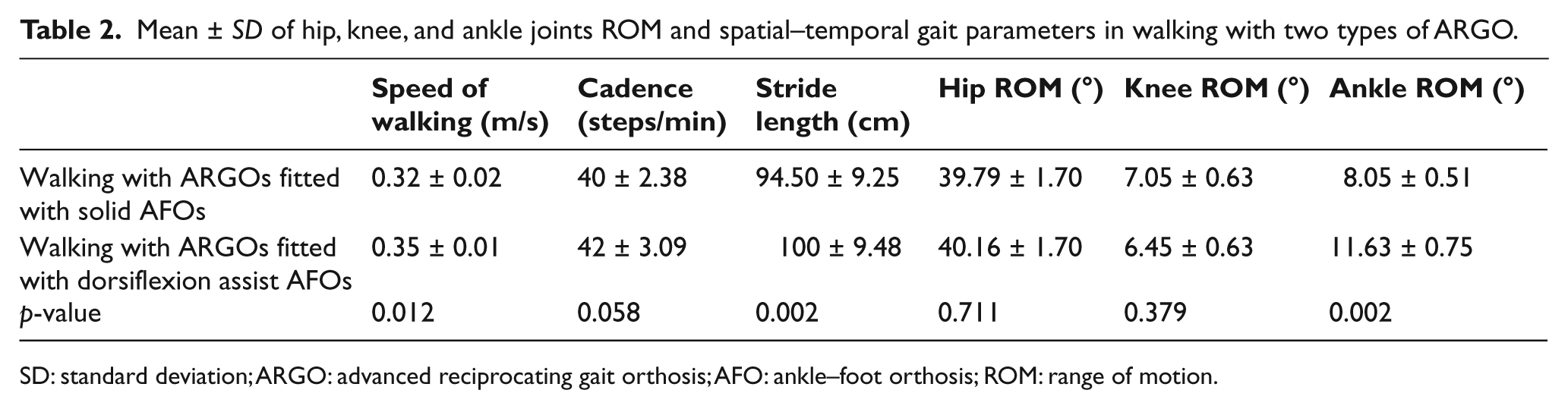
SD: standard deviation; ARGO: advanced reciprocating gait orthosis; AFO: ankle–foot orthosis; ROM: range of motion.
Joint ROMs
Table 2 shows the mean ± SD of hip, knee, and ankle joint ROMs when walking with the two types of ARGO. The mean hip joint ROM when the ARGO fitted with dorsiflexion assist AFOs was used (40.16° ± 1.70°) was larger than that when the ARGO with solid AFOs was used (39.79° ± 1.70°); however, there was no statistically significant difference noted between them (p = 0.711). The mean knee joint sagittal plane ROMs in walking with ARGO with dorsiflexion assist AFOs were reduced compared to the other test condition but again not significantly. The knee joint ROMs were not significantly affected (p = 0.379). However, as expected, the mean ankle ROM was significantly increased when walking with the ARGO fitted with dorsiflexion assist AFOs as compared to the other type of ARGO (p = 0.002).
When walking with the solid AFOs, sagittal plane motion at the ankle joint was blocked for the participants, but when using the AFO with dorsiflexion assist, the ankle joint of the orthosis participated in providing dorsiflexion and returned to a neutral position from dorsiflexion due to it incorporating a plantarflexion stop. This meant that the ankle was kept at 90° (the neutral position) at initial contact and mid stance but was allowed to dorsiflex during terminal stance. During swing phase of gait, the joint provided foot clearance by placing the ankle in dorsiflexion. Movement of the ankle joint in the AFOs with dorsiflexion assist was designed to provide sagittal motion only. Due to them having medial and lateral uprights, they were also designed to provide mediolateral stability.
Drop-locked knee joints and a reciprocating link were used at the knee and hip joints, respectively. When comparing the use of solid AFOs and AFOs with dorsiflexion assist, there was no significant difference noted between the two conditions in either hip or knee sagittal plane motion. The motion of the dorsiflexion assist AFOs was not synchronized with the other lower limb joints. The knee joints were always locked in extension and the hip joints were synchronized between themselves via the reciprocal link.
Comparison of injury level regarding gait parameters
The results of this study demonstrated that patients with a higher level of SCI have lower speeds of walking and shorter step lengths as compared to patients with a lower level of SCI. Table 3 demonstrates the alteration to walking parameters of an SCI patient with T12 level of injury compared to a patient with a T8 level of injury in this study. Kawashima et al. reported that performance of the orthotic gait depended on the level of spinal cord lesion. A limited hip ROM can result in the lower mean of gait parameters when using orthosis in the higher thoracic level of SCI patients.
Mean of spatial–temporal gait parameters in walking with two types of ARGO in SCI patients with T12 and T8 injury level.
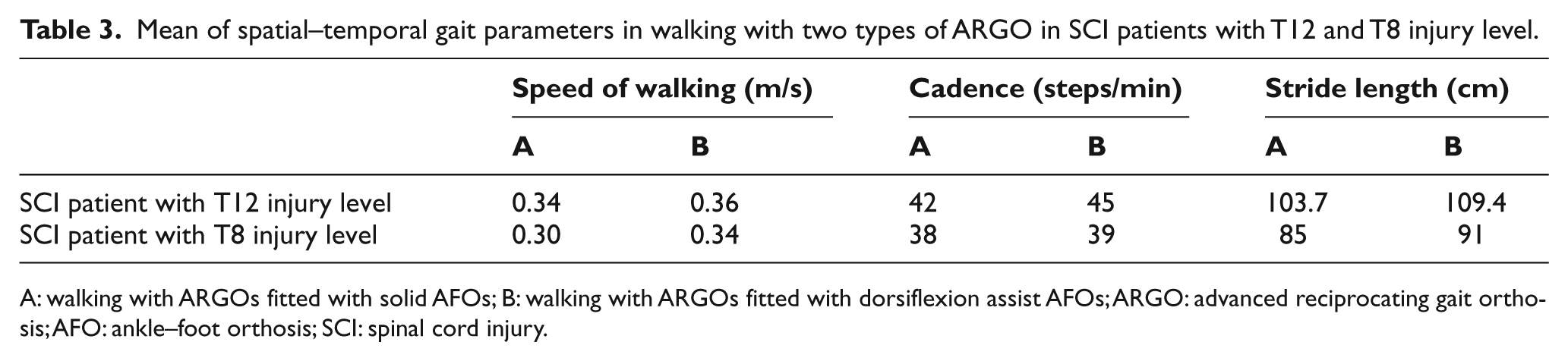
A: walking with ARGOs fitted with solid AFOs; B: walking with ARGOs fitted with dorsiflexion assist AFOs; ARGO: advanced reciprocating gait orthosis; AFO: ankle–foot orthosis; SCI: spinal cord injury.
Discussion
Improvements in the standing and walking ability of patients with paraplegia is valuable because of the effects of standing and walking in the prevention of osteoporosis, contractures of the lower limb joints, and cardiovascular as well as psychological problems.30–32 However, mechanical orthoses for use as rehabilitation devices in paraplegic patients are rarely used because of the high loads experienced on upper limb joints and the high energy consumption rates experienced when compared to wheelchair locomotion.12,33
A number of orthoses have recently been designed in order to restore the functions of standing and walking in this patient group. The ARGO has demonstrated positive effects on gait parameters in patients with SCI as compared to those afforded by hip–knee–ankle–foot orthoses (HKAFOs) and other types of RGOs.12,34 The ARGO offers a reciprocating pattern of motion in the hip joints via connection between the two hip joints and easy donning/doffing.12,34 However, this type of mechanical orthosis normally offers ambulation with fixed ankle and knee joints.
Rasmussen et al. 35 proposed a solution to this problem by adapting an IRGO with bilateral stance control knee joints for walking by SCI patients. Although this mechanism improved the kinematics of the knee and also temporal–spatial parameters in SCI walking, it did not adopt ankle joint motion because it still used solid AFOs in its design.
The results of this study showed that patients with SCI demonstrated improved gait parameters when the ARGOs utilizing dorsiflexion assist AFOs were used compared to when the ARGOs with solid AFOs were used. The movable ankle joints with dorsiflexion assist were responsible for the improvements demonstrated in the speed of walking and increased stride length. Kawashima et al. 19 evaluated temporal gait parameters with the WBCO in patients with SCI. The WBCO was constructed according to the concept of preparing a more dynamic reciprocal gait pattern for paraplegic patients using a movable foot portion. Kawashima et al. demonstrated that walking speed was significantly faster (0.31 m/s) when the WBCO was used in paraplegic patients as compared to a previous study in this field. The speed of walking in this study was 0.35 m/s and 0.32 m/s with the ARGO with dorsiflexion assist AFOs and solid AFOs, respectively. This suggests that even with a heavier system such as the IRGO, fitting a movable ankle joint with a dorsiflexion assist function in an appropriate orthosis at a position adjacent to the anatomical ankle joint of the SCI patients will improve gait parameters in SCI patients. Genda et al. 17 analyzed the efficacy of the HALO on spatial–temporal gait parameters in patients with SCI. The HALO has a mechanical linking system that connects ankle joints to the hip joint. The stride length was not significantly different between the HALO and the Primewalk orthosis, but the HALO did improve the cadence and the speed of walking as compared to the Primewalk.
The clinical observations of the paraplegic patients’ walking when the ARGO was fitted with dorsiflexion assist AFOs in this study demonstrated that ROMs of the hip joints and backward tilting of the pelvis improved when the paraplegic patients swung the lower limbs forward. The backward pelvic tilt motion of the pelvis would be improved due to the dorsiflexion movement in the ankle joints and the stable knee joints. Although the mean of this tilting and hip motion would vary between patients, it was noted that the gait parameters would depend on the level of injury in SCI patients. The lower the level of lesion, better the motions of the lower limb, and improvement in spatial–temporal and kinematic parameters may be expected. 36 ROMs in the hip joints affected the step lengths. When the step length was considered by the angle of the hip joint, the mean value for the ARGO with dorsiflexion assist AFOs was significantly improved when compared to that for the walking with ARGO with solid AFOs.
Both types of orthoses demonstrated adequate stability in standing and walking because no falls occurred during the gait training and gait evaluation sessions. Increases in the ankle joint movement would decrease trunk and shoulder girdle movement. Therefore, in walking using the ARGO with dorsiflexion assist AFOs, patients with SCI accommodated for the position using upper limb movements and had the best standing posture.
In this study, the effect of altering the AFO design in an orthosis on the gait parameters of SCI patients was evaluated, but we did not evaluate their effect on energy consumption by the patients. Evaluation of ARGOs incorporating AFOs with a dorsiflexion assist function may prove to be beneficial by improving this function and needs to be investigated in a future study. In addition, this study did not evaluate the alterations to compensatory motions or the loads applied to the upper limb joints, and these also need to be evaluated.
Kawashima et al. 19 demonstrated that energy costs reduced when the WBCO was used during walking in SCI patients, which could have meant that the gait efficiency would also be improved because of the movable ankle portion and reciprocal motion of the hip joint in WBCO. However, this is as yet unproven for other devices and further evidence of this effect is required.
In this study, the ARGO with dorsiflexion assist AFOs offered potential advantages to patients with paraplegia, such as its movable AFO structures and assisted motion in ankle joint. Problems still exist in gait efficiency when this type of orthosis is used, as a much slower speed of walking and shorter step length and lower cadence is expected when compared to normal walking. Using a motor mechanism as external power source in assisting the motion in hip and knee joints may offer a proposed solution to these problems. Arazpour et al.37,38 demonstrated the effects of a powered hip orthosis and powered gait orthosis in patients with SCI. In their study, they reported successful experiences of standing and walking with two types of powered orthosis and also demonstrated that the powered orthosis produced a higher speed of walking than an IRGO.
For patients with paraplegia, development of powered orthoses using a controlled actuator to move the hip and knee joints in association with dorsiflexion-assisted ankle joints may therefore offer a more beneficial solution for this patient group. It could enable patients with paraplegia to obtain walking ability in both a clinical environment and at home.
Conclusion
The ARGO fitted with dorsiflexion assist AFOs had the effect of improving gait parameters by facilitating movement of the orthotic ankle joints when compared to walking with an ARGO fitted with solid AFOs.
Footnotes
Acknowledgements
This article was a part of PhD thesis in department of orthotics and prosthetics in the University of Social Welfare and Rehabilitation Sciences. Hereby, we would like to thank the members of O&P department and patient contribution in all stages of study.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.