
Abstract
Background:
The advanced reciprocating gait orthosis (ARGO) has a rigid structure which provides restricted movement at the hip, knee, and ankle joints and incorporates a pelvic section with an extended section in the lumbar region. Healthy subjects, when walking with an RGO in situ, could feasibly demonstrate the level of limitation in movement imposed by ARGO-assisted ambulation.
Objective:
The aim of this study was to compare the function of the advanced reciprocating gait orthosis when fitted with the dorsiflexion-assist ankle–foot orthoses on temporal–spatial parameters and kinematics of walking in both able-bodied people and those with spinal cord injury.
Study design:
Quasi experimental design.
Methods:
Data were acquired from six able-bodied and four spinal cord injury subjects who used an advanced reciprocating gait orthosis which incorporated dorsiflexion-assist ankle–foot orthoses. Kinematics and temporal–spatial parameters were calculated and compared.
Results:
All able-bodied individuals walked with speeds which were only approximately one-third that of when walking without an orthosis. The mean step length and cadence were both reduced by 48% and 6%, respectively. There were significant differences in hip, knee, and ankle joint range of motions between normal walking and walking with the advanced reciprocating gait orthosis both in able-bodied subjects and patients with spinal cord injury. There were also significant differences in the speed of walking, cadence, step length, hip range of motion, and ankle range of motion when using the advanced reciprocating gait orthosis between the two groups.
Conclusion:
Temporal–spatial parameters and lower limb sagittal plane kinematics of walking were altered compared to normal walking, especially when spinal cord injury subjects walked with the advanced reciprocating gait orthosis compared to the able-bodied subjects.
Clinical relevance
To produce an improvement in RGO function, an increase in walking performance should involve attention to improvement of hip, knee, and ankle joint kinematics, which differs significantly from normal walking.
Keywords
Background
Several types of orthoses have been designed and constructed to assist paraplegic patients in walking and standing. 1 Hip–knee–ankle–foot orthoses (HKAFOs), hip guidance orthoses (HGOs), advanced reciprocating gait orthoses (ARGOs), isocentric reciprocating gait orthoses (IRGOs), the Walkabout orthoses, and the Primewalk orthoses are all mechanical orthoses that permit walking in this patient group. 1 Studies have demonstrated that the ARGO and the IRGO produce higher walking speeds, greater stride lengths, increased cadence, and reduced energy consumption for paraplegics following analysis with other comparative designs. 2
Although reciprocating gait orthoses (RGOs) facilitate walking with reduced compensatory motions and more cosmetic gait patterns than other orthoses such as HKAFOs, rejection of these types of orthosis for ambulation in preference to wheelchair use is still common.3,4 Usage times of RGOs have been suggested as being 2 h per day, with rejection rates being reported as ranging from 46% to 54% in people with spinal cord injury (SCI).4,5 The effort required to ambulate, the high loads experienced on the upper limb joints, and high levels of energy consumption are considered as main reasons for the limited use of RGOs. 4 Typical speeds of walking are described as ranging from 0.2 to 0.3 m/s with an energy consumption of 1.0 mL/kg/m with RGOs in people with SCI.6,7 In comparison, healthy subjects have an average gait velocity and oxygen consumption of 1.28 m/s and 0.176 mL/kg/m, respectively. 8
The energy consumption of walking with RGOs is therefore high due to the large amount of power needed to ambulate with these orthoses. 6 Dall et al. 9 reported that a reciprocal link fitted to an RGO did not help in enabling the lower limb to swing. These observations were confirmed by Johnson et al. 10 who also demonstrated that RGOs only applied a small hip flexion moment. However, when using powered orthoses, it has been demonstrated that improvements in hip joint kinematics may be expected compared to non-powered devices.11,12 Furthermore, reductions in trunk and pelvic motions have been shown to be more important than the use of a reciprocal link between the hips in encouraging swing in the lower limbs in paraplegic patients.9,10
The level to which the above parameters may be improved when walking with an ARGO is at present unclear. Therefore, by analyzing the gait of able-bodied subjects when walking with an ARGO, useful information may be provided about the limitations and levels of improvement in gait parameters which may be expected for this type of orthosis. In order to determine the limitations of walking with an ARGO in situ, further research is therefore required. To the authors’ knowledge, no evidence exists using gait analysis to determine the impact of a mechanical orthosis on the temporal–spatial parameters and kinematics of walking when worn by both able-bodied participants and people with SCI. Therefore, the aim of this study was to determine the effects of ambulating with an ARGO on the temporal–spatial parameters and kinematics of walking in able-bodied subjects and people with SCI.
The ARGO has a rigid structure which provides restricted movement at the hip, knee, and ankle joints and incorporates a pelvic section with an extended section in the lumbar region. This therefore allows limited movement during ambulation. The acceptability of walking with an RGO on a level surface by paraplegic patients is not clear. Healthy subjects, when walking with an RGO in situ, could feasibly demonstrate the level of limitation in movement imposed by ARGO-assisted ambulation. Temporal–spatial and kinematic parameters can be influenced during ARGO-assisted locomotion differently by normal and SCI subjects and may provide information in the way in which ARGOs provided limitation in walking. The information obtained from this study will help both clinicians and researchers by highlighting the importance of undertaking gait analysis of RGOs for use in the clinical setting. In addition, it may also provide a better understanding of the relationship between walking with an RGO and patient outcome measures to optimize RGO prescription in various patient groups.
Methods
Subjects
Four paraplegic subjects with injuries at the thoracic level participated in this study. Their demographics are shown in Table 1. They were evaluated and referred by physicians who also confirmed that the patients were physically fit for gait training with an orthosis. Each subject was then fitted with an ARGO with dorsiflexion-assist-type AFOs. Volunteer SCI subjects with complete (grade A) or incomplete motor paralysis (grade B) in the lower limb muscles based on the American Spinal Injury Association (ASIA) score 13 participated in this study. Inclusion criteria for participation in this study were no history of cardiovascular or pulmonary diseases, contractures, severe spasticity, obesity, or asymmetric hip positions and that they were at least 6 months post-injury. Six able-bodied subjects (male, mean age range 33 ± 2.6 years (35.6–30.04 years), mean weight 68 ± 4.6 kg (72.6–63.4 kg) and mean height 178 ± 5.2 (183.2–172.8 cm)) took part in the study. They had no known history of musculoskeletal disorder/condition or any other ailment which would influence their walking pattern. A standard ARGO equipped with dorsiflexion-assist AFOs was used for the study (Figure 1). Each subject gave written informed consent for agreeing to undertake the experimental procedure, which was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Science.
Patient information for subjects who participated in this study.
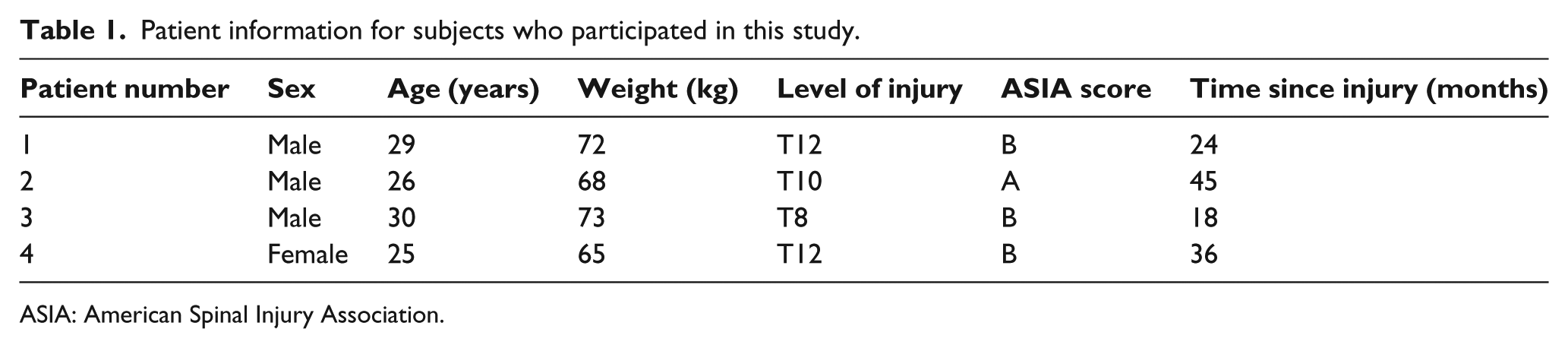
ASIA: American Spinal Injury Association.

The design of the advanced reciprocal gait orthosis with dorsiflexion-assist AFOs used in this study.
Orthotic gait training
The ARGO has a single cable which is connected bilaterally to the side members of the knee–ankle–foot orthosis sections. A flexion torque applied by the subject to one hip joint is mechanically translated to an extension torque on the contra-lateral hip joint and vice versa. The amount of gait training with the orthoses varied between subjects (between 6 and 10 weeks) according to their level of spinal injury. The gait training program included strengthening of upper body muscle, transferring, donning and doffing of the orthosis, balancing in a standing position, and walking training on regular surfaces. Each patient could walk with the orthosis independently with a walking aid without falling after completion of gait training with the orthosis. The ARGOs were manufactured from casts of the lower limbs for all subjects by an experienced orthotist.
The dorsiflexion-assist AFO sections were manufactured from 4-mm copolymer polypropylene and custom molded from plaster of Paris casts with full-length footplates, anterior trim lines at the malleoli, and incorporated dorsiflexion-assist ankle joints (manufactured by Tavan Sazan Company, Iran) with an ankle plantarflexion stop. The lining material with durable density poly foam (Ottobock, Germany) was added to the footplates and proximal aspect of the AFOs. A 2.5 cm heel lift with nonslip finish was added to the heel area of all AFOs to replicate the pitch of a shoe with a 2.5 cm heel.
Gait analysis
Gait analysis data from six healthy subjects and four SCI patients were obtained at the Department of Ergonomy, Biomechanical Research Laboratory, which is equipped with Vicon digital capture system (Oxford Metrics, UK; 640) for capturing kinematic data and two force plates at the sampling frequency of 100 Hz (Kistler 9286BA, Switzerland) embedded flush in the floor of a 6-m walkway. Kinematic data were gathered at a frequency of 100 Hz.
The volunteer subjects all walked along a 6-m walkway in a biomechanics laboratory at least five times at their self-selected walking speed when wearing the ARGO while using a walking frame (walker) with the wheels anteriorly positioned. Each patient could walk with the orthosis independently using walker assistance without falling after completion of gait training with the orthoses.
A total of 18 retro-reflective markers were used at the following positions: bilaterally over the position of the greater trochanter, the lateral condyle of the femur, the head and lateral malleolus of the fibula, the second metatarsal, anterior superior iliac spine (ASIS), calcaneus, and over the jugular notch, the spinous process of the seventh cervical vertebrae, and the acromio-clavicular joints. The markers were positioned on the trunk of the patients (over the jugular notch, the spinous process of the seventh cervical vertebrae, and the acromio-clavicular joints) and on the orthosis as close as possible to the positions where they would be located on the participant’s skin. The subjects were instructed to stand statically in the position dictated by the orthosis when it was donned, and markers were positioned on the trunk and lower limbs. The able-bodied subjects stood in their natural upright stance position during the marker setup prior to the assessment of able-bodied gait. The marker setup was the same for three groups (i.e. able-bodied, able-bodied when walking with the ARGO, and SCI subjects walking with the ARGO).
The cadence; stride length; speed of walking; and hip, knee, and ankle joint ranges of motion (ROMs) were analyzed from the motion analysis data. We used custom programs (MATLAB; The Math Works, Inc; Natick, MA, USA) to calculate the joint kinematics. These calculations were based on a link segment model where each body segment (thigh, foot, shank, etc.) was represented as a rigid link between two adjacent joints. The temporal–spatial parameters were determined based on the marker data obtained from the marker attached to the calcaneus.
Orthosis considerations
The orthoses were fabricated to be adjustable so that all individuals could use the same superstructure. The ARGO with dorsiflexion-assist AFOs had a mean weight of 6.8 kg (6.8 ± 3.9 kg). The uprights of new orthosis were constructed to be adjustable and also the straps to be adjustable so that this orthosis could be used by all the healthy and SCI volunteer participants. The proximal lateral side members were not adjustable and the straps were used to anchor the brace proximal to the hips. The lower limb side members were, however, designed to be adjustable so that the orthotic hip and knee joints could be positioned appropriately. The polypropylene ankle–foot orthoses were custom made for each participant. Sagittal plane kinematic and temporal–spatial data were measured under three conditions: (1) normal walking without wearing an orthotic device in healthy able-bodied subjects, (2) walking with the ARGO in healthy subjects, and (3) walking with the ARGO in SCI subjects.
Data collection
Each subject had multiple practice sessions for walking with the orthosis along the walkway for habituation to the device before actual trials were obtained. During data capture with or without the orthosis, each subjects walked with a pulpit-type walking frame. During each test condition, the subject walked along the walkway five times. Each individual was asked to walk at their self-selected speed for each trial. Test conditions were randomized in order, and there was a duration of rest between the tests.
Statistical analysis
Prior to analysis, the data were normally distributed as confirmed by the Kolmogorov–Smirnov. Repeated measures one-way analyses of variance (ANOVAs) tests were used to evaluate differences in speed of walking; stride length; cadence; and hip, knee, ankle joint ROMs in sagittal plane (JMP IN software; SAS Institute, Inc., Cary, NC, USA). Post hoc analysis using the Tukey honestly significant difference (THSD) was employed to identify specific differences between groups. SPSS 16 was used for all data analysis and the significant level considered was α = 0.05.
Results
Table 2 shows the means ± standard deviations (SDs) of the primary outcome measures and Table 3 shows the relevant p values when comparing the three test conditions.
Mean ± SD of hip, knee, and ankle joint ROMs in sagittal plane and spatial–temporal gait parameters in walking with ARGO in two groups and normal walking without orthosis.
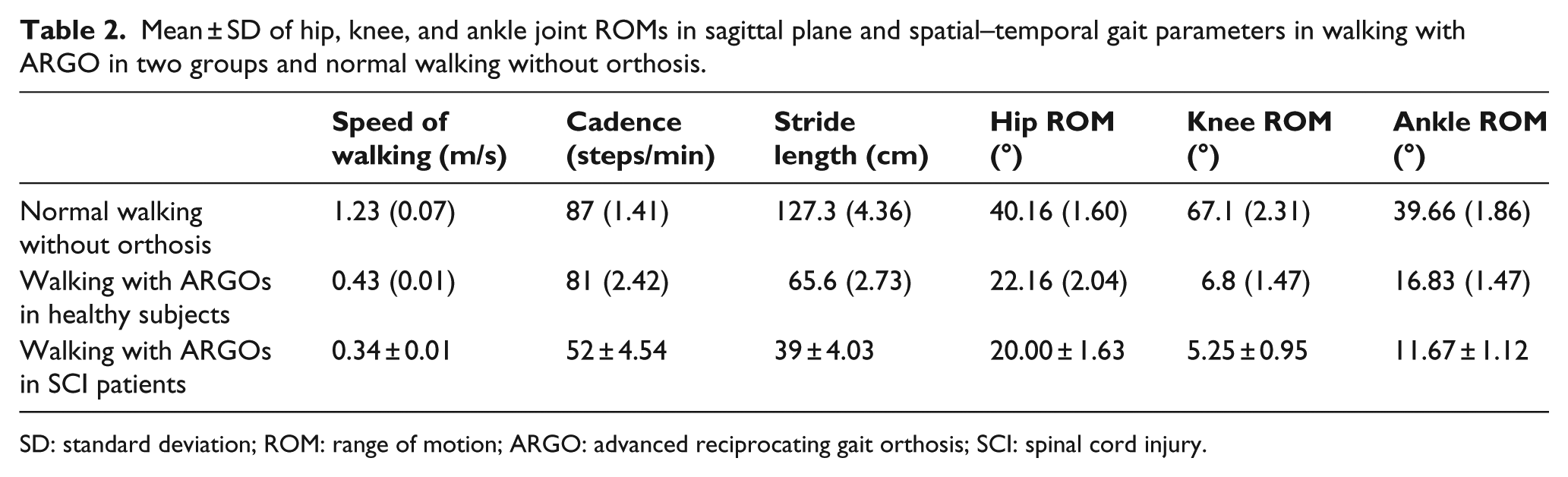
SD: standard deviation; ROM: range of motion; ARGO: advanced reciprocating gait orthosis; SCI: spinal cord injury.
p values of hip, knee, and ankle joint ROMs and spatial–temporal gait parameters between the three test conditions.
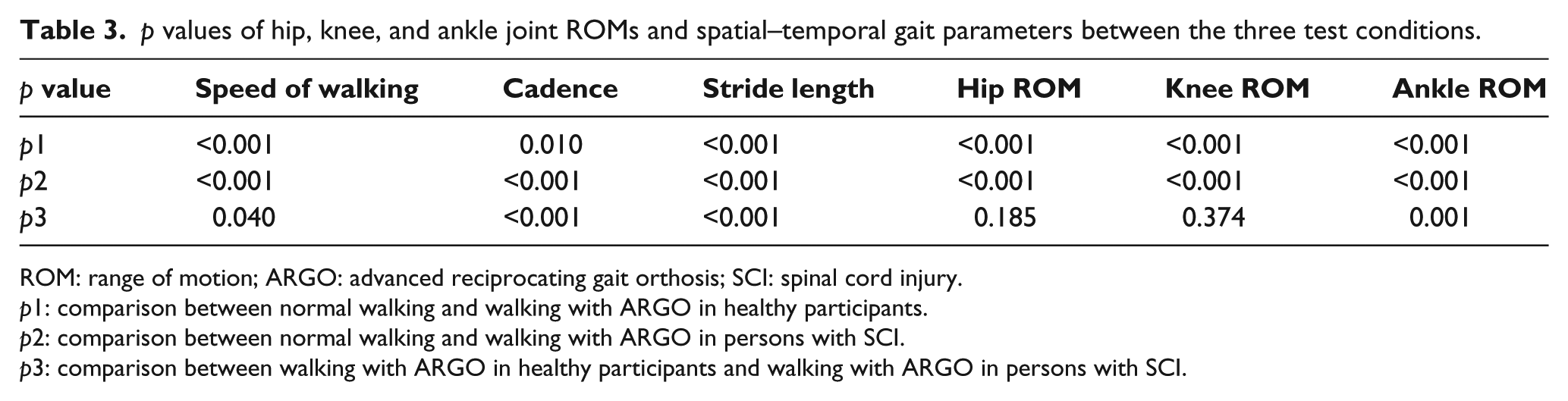
ROM: range of motion; ARGO: advanced reciprocating gait orthosis; SCI: spinal cord injury.
p1: comparison between normal walking and walking with ARGO in healthy participants.
p2: comparison between normal walking and walking with ARGO in persons with SCI.
p3: comparison between walking with ARGO in healthy participants and walking with ARGO in persons with SCI.
Temporal–spatial parameters
The self-selected walking speeds and step lengths were both significantly reduced by 65% (p < 0.001) and 48% (p < 0.001), respectively, when healthy participants walked with the ARGO compared to their normal walking, and cadence was decreased by 6%. Table 3 and Figure 2 demonstrate that walking with the ARGO in SCI patients produced a difference in speed of walking (18% decreased), cadence (51% decreased), and stride length (23% decreased) when compared to walking with this orthosis by the healthy subjects.
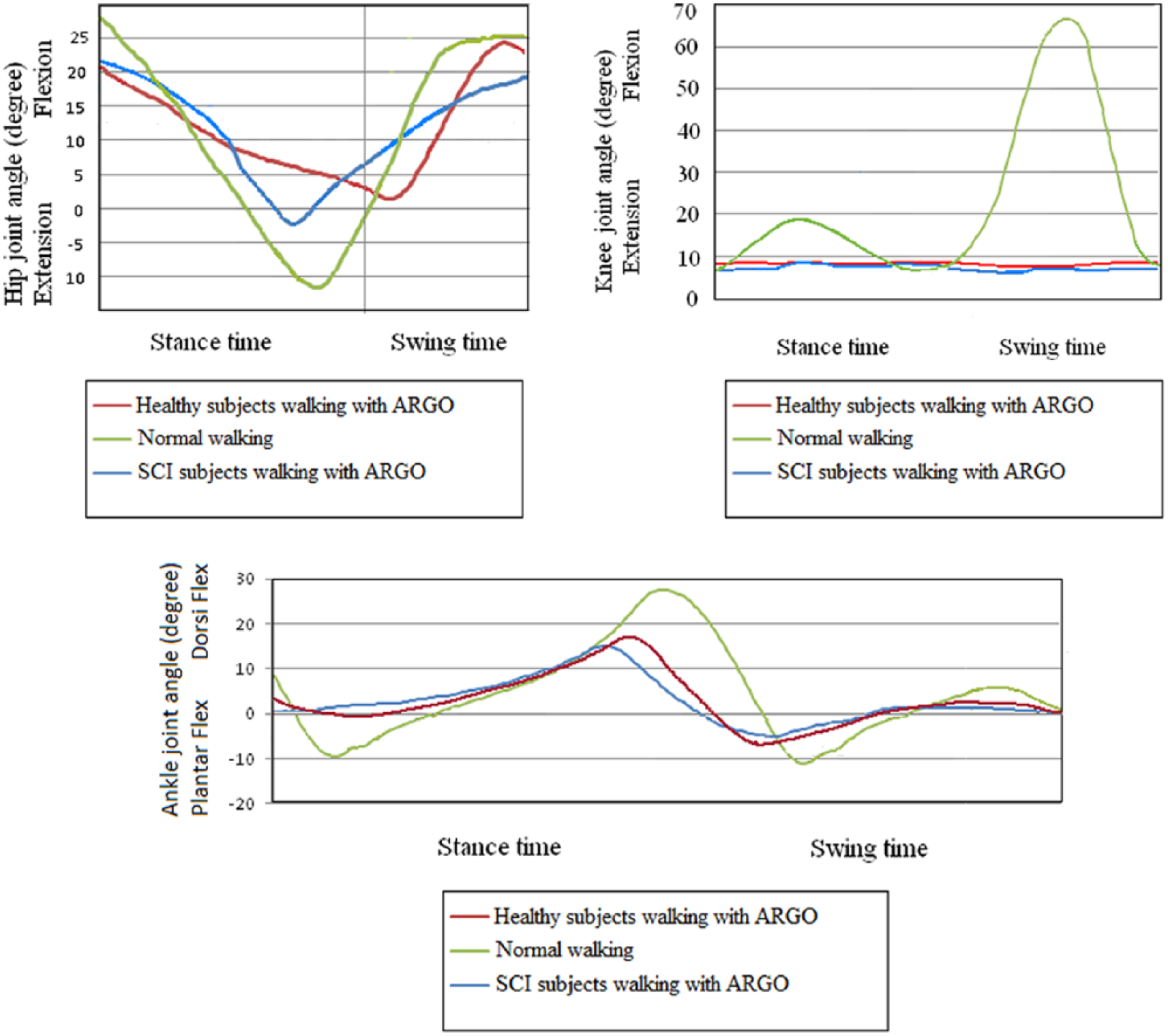
Mean sagittal plane kinematics for hip, knee, and ankle joints in normal walking, walking with ARGOs in healthy subjects, and walking with ARGOs in SCI patients.
Kinematics
These results coincided with decreased hip ROM (18°), knee ROM (61°), and ankle ROM (23°) in healthy participants walking with the ARGO compared to normal walking. There was significant difference between normal walking and walking with ARGO in healthy participants in hip, knee, and ankle joints ROM (Table 3 and Figure 2).
There was a significant difference between walking with ARGO in patients with SCI and normal walking in hip and ankle joint ROM (Table 3). Walking with ARGO in SCI patients decreased hip joint ROM (9%) and ankle joint ROM (31%) compared to walking with this orthosis in healthy subjects.
Discussion
All temporal and spatial parameters and sagittal plane joint kinematics were reduced in walking with the ARGO as compared to normal walking within the control group. These mean reductions were higher when the ARGO was used by the SCI subjects. The restrictive structure of the ARGO can cause further reduction in these parameters when worn by SCI subjects compared to able-bodied subjects due to their paralysis of the lower limb muscles. In comparison with previous studies in this field, Audu et al. 14 reported a reduction in the speed of walking and step lengths when evaluating a powered hip orthosis in healthy subjects. Arazpour et al. 15 also demonstrated similar results in the evaluation of a new powered gait orthosis on healthy subjects.
The findings of this study demonstrated that all subjects had smaller hip ROMs as compared to normal walking without an orthosis. Paraplegic users of the ARGO do not have active hip extensor and flexors to provide active ROM. The clear point in this issue is that there is limitation by the mechanical link between the orthotic hip joints which restricts movement. Perhaps one solution may be via the application of an external power source in providing active motion in the hip joint. 12
The findings of this study demonstrate that walking with the ARGO produced a lower speed of walking in both participant groups when compared to normal walking. This was less than half the speed achieved by healthy participants when the ARGO was used by SCI patients. Interestingly, cadence was reduced approximately 6% by healthy participants when walking with the orthosis compared to normal, but that for persons with SCI was significantly reduced by approximately 40% compared to normal. However, step lengths between both groups when walking with the ARGO were similar even though both were significantly smaller than normal healthy participant walking (p < 0.001) for persons with SCI and healthy participants, respectively. Decreased hip joint ROM in sagittal plane may have been the main factor in providing less step length in healthy and SCI subjects when wearing ARGO. Ankle joints in the ARGO that were used in this study had plantarflexion stop to prevent drop foot and provide foot clearance. This character may influence the step length during walking with ARGO. In addition, it would appear that the two main factors in producing the demonstrated reduction in persons with SCI walking speed with the ARGO were the reduction in hip ROM and step length when compared with that demonstrated by healthy participants walking with the orthosis.
With regard to kinematics, the main result of this study was reduction in knee ROM in walking with ARGO as compared to normal walking. Using this type of orthosis demonstrated approximately 60° of reduction in knee joint ROM in SCI and healthy subjects when walking with the ARGO. The locked knee joint that is used in ARGO during ambulation may have been the main factor for this result. This type of knee joints provided locked position in knee during stance and swing phase. Using a powered knee joint and stance-control knee designs may be beneficial in this case to increase knee joint ROM and improve knee kinematics.16,17 Similarly, there were differences noted between normal walking and walking with ARGO in healthy participants (i.e. in the control group) and also between the control group and SCI subjects at the hip. Paralysis of lower limb muscles in the SCI patients may have been the main reason for this result. When ablebodied subjects walked with the ARGO, the restrictive structure of the mechanical orthosis (ARGO) may have caused this result. Improvements to the mechanical design of the ARGO or alternatively the addition of an external actuator to the orthotic hip joint may be of benefit. 11
There are a number of limitations of this study. One limitation is that the authors did not explore the influence of the orthosis on energy consumption during walking in healthy subjects and SCI patients. Direct correlations between orthosis stiffness and energy consumption have been previously demonstrated in the literature. Walking is important goal in the rehabilitation of SCI subjects, and orthotic rehabilitation plays important role in providing this aim. Since walking parameters can also influence energy consumption and the rejection rate of wearing an orthosis, it was thought prudent to quantify the limitation in providing normal gait parameters induced when walking with an orthosis. Development of orthoses superstructures in the future may provide improvement of energy consumption in orthotic rehabilitation of SCI patients using the information available for both orthosis stiffness and their effect on gait parameters.
While it was noted that the healthy subjects had an altered trunk position in walking with the orthoses, the evaluation of flexion and extension positions of trunk in using RGOs and the effect of this position on the ROM of the hip joint is still unclear and needs further investigation. An adjustable ARGO with custom mold AFO was used in this study. The results would have been improved if each participant had a custom-made orthosis. This point is another limitation of our study.
Conclusion
The results of this study demonstrated that walking with an ARGO by healthy participants and SCI subjects produced reduced key temporal and spatial gait parameters, and further development work is therefore needed to produce a more effective device to more closely match the gait parameters of normal walking for people with SCI. To produce an improvement in RGO function, an increase in walking performance should involve attention to improvement of hip, knee, and ankle joint kinematics, which differs significantly from normal walking. For this to be achieved, the structural design of orthotic ankle, knee, and hip joints needs to be improved.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received financial support from the Iranian National Science Foundation (INSF) (grant number (91002361)).