
Abstract
Background:
Spinal cord injury patients walk with a flexed trunk when using reciprocating gait orthoses. Reduction of trunk flexion during ambulation may produce an improvement in gait parameters for reciprocating gait orthosis users.
Objectives:
To investigate the effect on kinematics and temporal–spatial parameters when spinal cord injury patients ambulate with an advanced reciprocating gait orthosis while wearing a thoracolumbosacral orthosis to provide trunk extension.
Study design:
Comparative study between before and after use o thoracolumbosacral orthosis with the advanced reciprocating gait orthoses.
Methods:
Four patients with spinal cord injury were fitted with an advanced reciprocating gait orthosis and also wore a thoracolumbosacral orthosis. Patients walked along a flat walkway either with or without the thoracolumbosacral orthosis at their self-selected walking speed. Temporal–spatial parameters and lower limb kinematics were analyzed.
Results:
Mean walking speed, step length, and cadence all improved when walking with the thoracolumbosacral orthosis donned compared to the trunk support offered by the advanced reciprocating gait orthosis. Hip and ankle joint ranges of motion were significantly increased when wearing the thoracolumbosacral orthosis during ambulation.
Conclusion:
Using an advanced reciprocating gait orthosis when wearing a thoracolumbosacral orthosis can improve walking speed and the step length of walking as compared with walking with an advanced reciprocating gait orthosis, probably due to the extended position of the trunk.
Clinical relevance
Donning the thoracolumbosacral orthosis produced a relatively extended trunk position in the advanced reciprocating gait orthosis for all the patients included in the study, which resulted in improved gait parameters.
Background
Reciprocating gait orthoses (RGOs) are one type of mechanical orthosis used by spinal cord injury (SCI) patients to provide walking and standing activities. 1 The benefits of walking and standing with RGOs include improvements in both physiological and psychological aspects. 2 Physiologically, reduction in the incidence of osteoporosis, fractures, spasticity, contractures, and reduced atrophy of lower limb muscles plus improvements in blood circulation are all achieved by this patient group when utilizing RGOs. 3 In addition, improvements in self-esteem and personal relationships plus reduced rates of depression are all evidence of the advantages of being able to ambulate. 4
The positive effects of walking with RGOs have been reported in the literature. Harvey et al. 5 demonstrated an improvement when walking with an isocentric reciprocating gait orthosis (IRGO) on walking speed and energy consumption compared to that achieved when using a Walkabout orthosis. Arazpour et al. 6 and Leung et al. 7 both reported the positive effects of walking with the IRGO on both walking speed and the physiological cost index (PCI) of walking compared to a hip–knee–ankle–foot orthosis (HKAFO). Winchester et al. 8 reported that the energy costs of walking at comfortable self-selected speeds were lower with the IRGO compared to a standard RGO. Even so, walking with RGOs still results in a high energy expenditure being experienced by the patient and can therefore be exhaustive for SCI patients.9,10 Rejection rates of this type of orthosis have been shown to be between 61% and 90% in children with myelomeningocele and 46% and 54% in adult SCI patients.11–13 This is thought to be due to the high energy expenditure and high loads transmitted through the upper limbs via crutches and other walking aids which may be exasperated by walking with a flexed trunk position leading to compromised gait parameters when using RGOs.
During walking with RGOs, the users routinely shift the majority of their weight onto the stance side and elevate the pelvis to initiate hip flexion on the imminent swing leg side. This is accompanied by extension of the hip joint on the stance side leg in conjunction with reaction forces through the upper limb via a walking aid to produce this motion. However, excessive trunk flexion due to having to use a walking aid positioned in front of the RGO can hinder these motions during ambulation and may cause insufficient motion within the reciprocal mechanism of such orthoses. This may be a cause of the reported elevation in energy consumption and loads on upper limbs which has been demonstrated by SCI patients.10,14–17
In evaluation of walking mechanism of paraplegic patients in using RGO, Johnson et al. 18 demonstrated that paraplegic patients adopt a flexed trunk position and pass a large proportion of their body weight through the arms during single support when using an RGO during walking. Moments acting at the hip also cause trunk flexion, and providing an extension moment on the hip joint at the beginning of swing hinders advancement of the swing leg and contradicts the intent of the reciprocal link. Therefore, the relationship between trunk posture and the action of the reciprocal link in the RGO should be explored.
Reduction of trunk flexion during ambulation may cause an extension moment on hip joint that is needed for RGO function and produce an improvement in gait parameters for RGO users. The aim of this study was therefore to evaluate the effect of a relatively extended trunk position in SCI patients. This was achieved by wearing a thoracolumbosacral orthosis (TLSO) when ambulating with an advanced reciprocating gait orthosis (ARGO)-type RGO compared to when walking without a TLSO but utilizing an ARGO.
Methods
Patients
Four SCI patients, all with thoracic-level injury and with either grade A or B American Spinal Injury Association Impairment Scale (AIS), 19 participated in this study. Table 1 shows the demographic data of patients included in this pilot study. Inclusion criteria included no evidence of cardiovascular problems, spasticity, contracture, obesity, or asymmetry in hip joint positions in the sagittal plane and were required to be at least 6 months post injury 20 to allow psychological improvement to occur prior to being included. Informed consent was obtained from volunteer patients prior to being included in the study, and the Human Ethics Committee of the University of Social Welfare and Rehabilitation Sciences gave approval to perform the study.
SCI patients who participated in this study.
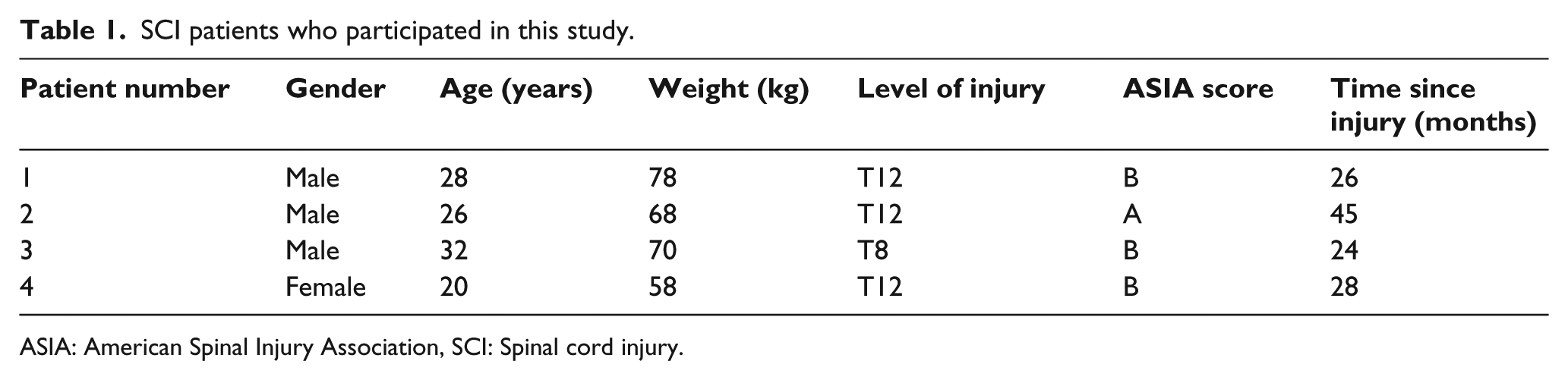
ASIA: American Spinal Injury Association, SCI: Spinal cord injury.
All patients were experienced in using an ARGO fitted with ankle–foot orthoses (AFOs) incorporating dorsiflexion assist ankle joints. 21 They all had received between 6 and 8 weeks experience of gait training (dependent on the level of injury) while walking with the help of an ARGO and also with the additional help of a TLSO. The orthotic gait training program included donning and doffing of the orthoses, balancing in a standing position and walking training on regular flat surfaces. The patients performed orthotic gait training with the ARGO and the ARGO while also wearing a TLSO prior to the walking trials. After the prescribed training programs with the orthoses, each patient could walk independently and continuously with the orthoses and walking frame. The TLSO was a Taylor-type off-the-shelf orthosis (Tynor Orthotics Pvt Ltd, India) manufactured from aluminum with 4-mm-thick uprights and soft neoprene lining with an anterior abdominal pad. The ARGO was measured to fit over the top of the brace. The brace had limited bulk, which meant that the ARGO was also suitable to be worn without the TLSO by adjusting the straps, and the patients were still able to bend forward enough to move the walking frame forward when wearing the TLSO encapsulated by the ARGO. Trunk orientation also changes the moment arm between the trunk center of mass (COM) and the hip and shoulder joints. 18 If the trunk was changed from flexion position to an extended position, the moment arm would alter so that an upward force from the hip joint could lead to initiation of trunk extension motion. This orientation may provide prevention or reduction of upper thoracic flexion. For this aim, using a Taylor-type TLSO with shoulder straps could encourage extension of upper thoracic vertebral segments rather than using a hyperextension orthosis (e.g. a Jewett brace).
The two test conditions were randomly selected to evaluate the effect of relative trunk extension on selected gait parameters when either walking with an ARGO as a control condition or walking with ARGO while also wearing a TLSO. Figure 1 shows the ARGO used in this study. Figure 2 shows the TLSO design.

SCI patient standing with the ARGO used in this study.

The TLSO used in this study.
Patients walked at their self-selected speed in a gait laboratory which incorporated a 6 m walkway and performed five walks over the force plates during the same gait analysis session. A Vicon digital motion capture system with a frequency of 100 Hz (Oxford Metrics, UK) with six infrared cameras and two force platforms (Kistler 9286BA, Switzerland) was used to capture data from passive reflective markers which were strategically placed on the lower limbs and trunk. We analyzed motion of the body segments using passive reflective markers that were located to the body and the orthosis. Lower extremity markers were placed on the uprights of the orthosis or the thermoplastic superstructure directly over the anatomical points. For dynamic trials, markers were located over the dorsum of the foot on the second metatarsal immediately proximal to the metatarsal head; on the posterior calcaneus at the same height as the toe marker, lateral ankle joint, shank, lateral knee joint, thigh, hip joint, and right and left anterior superior iliac spines; and on the sacrum. Four markers were used over the jugular notch, spinous process of the seventh cervical vertebrae, and the acromio-clavicular joints. Marker placement on the pelvis was particularly difficult for the patients who used an ARGO because the pelvic section prevented direct placement of a sacrum marker on the sacrum. The sacral marker was placed on the pelvic section, therefore separating the sacral marker from the sacrum by about 3 cm. However, as demonstrated by Johnson et al., 18 the difference of motion between the sacral marker on the pelvic section of the orthosis and the normal condition when the pelvic markers on the patients was ignored because previously, it was considered that the introduced error by the marker placement used in this study is no greater than that demonstrated in gait analyses which use the normal marker set.
The force platform was used to determine stance and swing phases. The markers placed on the sacrum and the seventh cervical vertebra were used to determine the sagittal plane angle of the trunk. We used custom programs (MATLAB; The MathWorks, Inc, Natick, MA, USA) to calculate the joints kinematics. These calculations were based on a link segment model where each body segment (thigh, foot, shank, etc.) was represented as a rigid link between two adjacent joints. All the patients used a walking frame, as shown in Figures 1 and 2, during the walking trials.
Data analysis
Normality of data in speed of walking (0.427), step length (0.567), cadence (0.611), trunk flexion (0.314), and kinematic of hip (0.383), knee (0.567), and ankle joint (0.310) was confirmed by using the Kolmogorov–Smirnov technique. According to the normality of data, a paired t-test was used for analyzing the effects and differences in the selected outcome measures between the two orthoses. SPSS statistical software version 16.0 (SPSS Inc., Chicago, IL, USA) was used for the analysis of data. The level of significance was set at 0.05.
Results
Temporal–spatial parameters
Table 2 demonstrates the effect on the speed of walking, step length, cadence, trunk flexion, and kinematic of hip, knee, and ankle joints when SCI patients walked with an ARGO while wearing a TLSO compared to being without one. The effect of wearing the TLSO during ambulation produced a statistically significant difference in the mean walking speeds between the two test conditions (p = 0.014). The mean walking speed when walking with the ARGO was 0.33 ± 0.02 m/s, while this parameter was 0.35 ± 0.02 m/s with the addition of wearing the TLSO. The cadence and step length both increased when wearing the TLSO, but not significantly (cadence p = 0.638, step length p = 0.080).
Mean and SD of temporal–spatial parameters and joints kinematic in walking with ARGO and the ARGO plus TLSO.
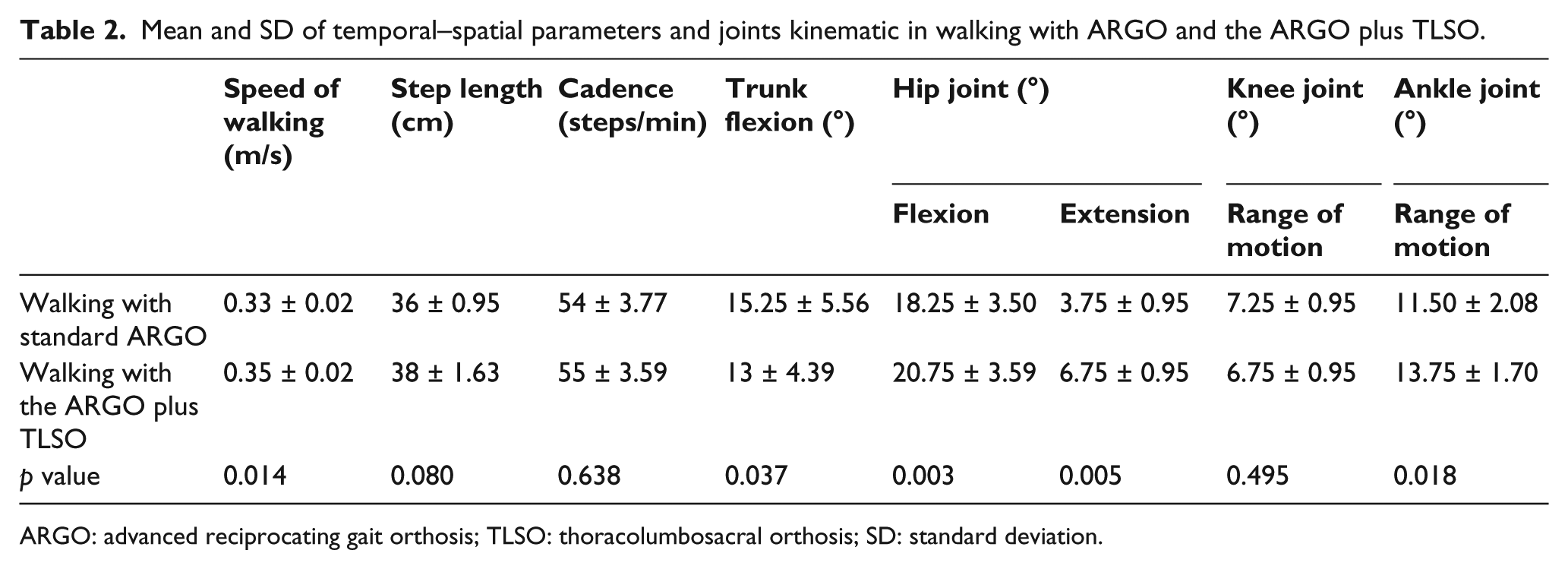
ARGO: advanced reciprocating gait orthosis; TLSO: thoracolumbosacral orthosis; SD: standard deviation.
Trunk flexion
There were significant differences in the mean trunk flexion angle between the two test conditions (p = 0.037). The mean of this parameter in walking without the TLSO was 15.25° ± 5.56°, which was reduced to 13° ± 4.39° when wearing the TLSO.
Joint kinematics
Mean and standard deviations for lower limb joint kinematics are demonstrated in Table 2. The knee joint range of motion (ROM) of 7.25° ± 0.95° was attained in using standard ARGO, while during walking with the ARGO and wearing the TLSO, this parameter was reduced to 6.75 ° ± 0.95 °. The overall knee joint ROM remained relatively constant in using two types of interventions due to the locked orthotic knee joints. Given that the knee joint was ring lock (thus movement must be restricted), the knee joint have 6 °–7 ° movement due to deformation of orthosis. However, when wearing the TLSO, the mean ankle ROM was significantly increased by 2.25 ° between the two test conditions (p = 0.018). When walking at their self-selected walking speed with the TLSO donned, hip flexion and extension for all four SCI patients also increased significantly compared to walking without it donned (Table 2). Mean hip flexion increased by 2.5° and mean extension by 3° (p = 0.003 and p = 0.005, respectively). Summarized data for sagittal plane kinematics for the trunk, hip, knee, and ankles are shown in Figure 3. Sagittal plane movement of the trunk closely followed a sinusoidal pelvic motion equating to the step cycle (i.e. half a gait cycle). The RGO users walked with a continuously larger flexed trunk position compared to when wearing the TLSO.
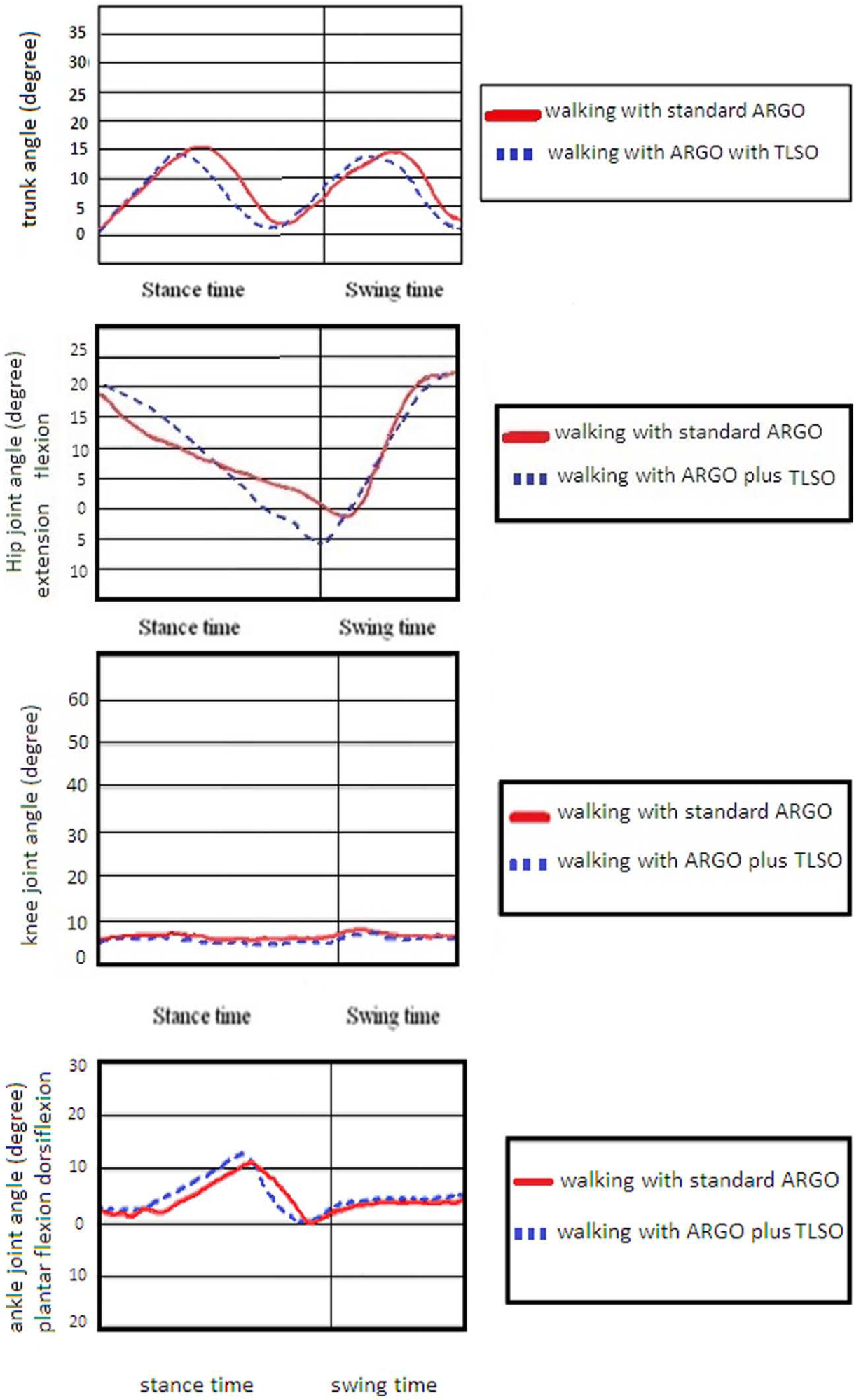
Sagittal plane kinematics for the trunk, hip, knee, and ankle joints in walking with standard ARGO and walking with ARGO plus TLSO.
Discussion
In this study, SCI patients walked with the help of an ARGO with and without the additional support of a TLSO to enable a comparison to be made between the two test conditions. The TLSO was designed to stabilize the trunk and reduce trunk motion, particularly in the upper thoracic and lumbar spine. However, the patient still needed to adopt a forward inclination of the trunk to walk with the ARGO. Indeed, patients are unable to walk with an RGO with their trunk constantly in an extension position in the full upright position during the whole of the gait cycle, but do need an extended trunk position for propulsion and commencement of flexion and swing in the lower limbs. The requirement to add load to the upper limbs via a walking aid to provide extension of the trunk and extension of the hip joints may explain the fatigue experienced in the upper limbs and high energy consumption when SCI patients use an ARGO to ambulate. The use of a walker placed in an anterior position in front of the torso also induces trunk flexion when walking with an ARGO. Nevertheless, in this study, there were significant differences noted between walking with and without spinal orthosis by the SCI patients.
Kinematics and temporal–spatial parameters were altered during the walking trials when using the TLSO, and with the trunk relatively extended. However, although the TLSO provided trunk extension in this study, patients also reported some discomfort with this orthosis. To resolve this problem, it may be prudent to replace the frame-type walking aid with elbow crutches placed adjacent to the torso during ambulation in order to provide a “C-shaped” posture within the RGO to position the ground reaction force (GRF) line of action posterior to the hip joint. The design and evaluation of a chest band may therefore also prove useful in reducing trunk flexion of patients during walking with RGOs, and a further study using this technique would be beneficial.
The mean of speed of walking and step length in this study are comparable with previous studies in this field. The mean walking speeds achieved by SCI patients have been shown to range between 0.34 and 0.17 m/s with mechanical orthoses 4 and between 0.4 and 0.31 m/s with powered orthoses.22,23 When using the ARGO plus TLSO test condition, the mean walking speed attained in this study was 0.35 m/s, which compares favorably with previous studies.
Flexion or extension of the trunk can change the moment arm between the COM of the trunk and the hip and shoulder joints. 18 Therefore, an extended trunk position may encourage weight-bearing through the stance leg rather than the walking aid utilized. Walking with RGO in this position can reduce loads on upper limb joints, ambulation effort, and energy consumption due to weight-bearing on the stance lower leg.
SCI patients experience high loads through the upper extremity when walking with RGOs, which is dependent on the amount of flexion and the resultant position of the trunk. 18 This is one of the main problems which results in high energy consumption when using orthoses. During walking, able-bodied patients have exhibited increased knee flexion, ankle dorsiflexion, and hip flexion during stance phase with the trunk in a flexion position. 20 These alternations may have occurred in order to maintain dynamic balance by shifting the body’s COM to a position and to facilitate patterns of vertical displacement similar to that of upright walking. Walking speed, step length, and cadence were all also decreased with the trunk in a flexion position compared to upright posture during walking. Indeed, the function of reciprocal link in the RGO was positively affected by the extended trunk position, as evidenced by the kinematic data. Increased trunk and hip joint extension on the stance side produced increased flexion of the swing side. Conversely, flexion of the trunk provides hip flexion in stance lower leg, which in turn encourages swing hip extension of the swing leg in forward ambulation. 18 Therefore, if trunk extension could be provided by an RGO mechanism and superstructure, improvement of gait parameters in temporal–spatial parameters may be expected.
As with other previous studies on evaluation of walking with RGO, a limitation of this study relates to the small sample population. Including SCI patients with different level of injury introduces a multitude of parameters such as the different level of motor and sensation, different passive ROMs of the joints, and varying degrees of spasticity. It has been demonstrated that RGO users with T12, T11, L3, and C7 levels of injury walk with a flexed trunk position. 18 Even though SCI patients with a T12 injury level may have the capacity to control trunk and pelvic positioning to some extent, using a TLSO to prevent trunk flexion in these patients can provide information about the influence of trunk extension when using an ARGO for walking in SCI patients. The main aim of this study was therefore the influence of using the ARGO with the trunk in a relatively extended position on the walking parameters exhibited by SCI patients. The information gained following this type of evaluation can potentially help researchers involved in gait rehabilitation of SCI patients when using an ARGO. Further research is needed regarding evaluation of the effect of trunk position in walking with RGOs simultaneously on loading levels of the upper limbs and energy consumption. If trunk extension can be assisted in a novel way when ambulating with RGOs, it will prove beneficial for the rehabilitation of SCI patients.
Conclusion
Analyses of walking with an ARGO while wearing a TLSO demonstrated increased temporal–spatial parameters and improved gait patterns when trunk flexion was reduced. The results of this study propose that improvements in the design of RGOs to provide trunk extension should be explored further because walking with current RGOs causes high loading to the upper limbs and high energy consumption.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This material was based on work supported by the Deputy of Research and Technology of Mazandaran University of Medical Sciences (grant number: 677).