
Abstract
Background and aim:
The most commonly prescribed external shoe modification is the use of rocker soles. The aim of this study was to evaluate the effect of a heel-to-toe rocker sole profile on specific temporal–spatial parameters and the kinematics of walking when added to footwear.
Method:
Seventeen healthy adult volunteers participated in this study. For each subject, gait analysis was performed under two conditions that were tested in a random order: walking with either a baseline shoe with a flat sole or a modified shoe adapted with a heel-to-toe rocker sole.
Results:
Significant differences were observed between rocker sole conditions during initial double-limb support and second double-limb support during stance phase. In frontal plane movement, significant differences were observed between the rocker sole conditions but only during second double-limb support phase.
Conclusions:
This heel-to-toe rocker sole may be useful for patients with conditions such as ankle arthrodesis or for use with ankle–foot orthoses where limited ankle motion is required.
Clinical relevance
The heel-to-toe rocker sole may be useful for conditions including ankle arthrodesis and for use with solid ankle–foot orthoses but may not be suitable for patients with reduced balance or an unstable posture.
Introduction
One of the most frequent external shoe modifications used in the treatment of foot and ankle problems is the addition of rocker soles to footwear. Rocker soles have been traditionally used to provide limitation of sagittal plane motion in the forefoot. They have therefore proven efficacy for treatment of conditions such as hallux limitus and hallux rigidus, first metatarsal head dorsal exostoses, sesamoiditis, metatarsal head fractures, midtarsal joint osteoarthritis, and rheumatoid metatarsal head pain.1–3 However, their effects on other gait parameters such as ankle joint sagittal plane motion and cadence, step length, and walking speed when treating pathologies or injuries affecting ankle range of motion (ROM) have not been extensively investigated.4,5
Rocker soles have also been shown to facilitate a decrease in plantar foot pressures in targeted areas of the foot during ambulation, which has proved a useful orthotic intervention for patients with peripheral neuropathy resulting from conditions such as diabetes mellitus and rheumatoid arthritis.6–9 Biomechanically, the decrease in pressure is caused by a decrease in moment arm, which is dependent on the localization of the apex of the rocker and the size of the rocker. 10
One area of interest in the literature has centered on the effect of so-called unstable footwear, which utilize rocker soles to affect lower limb electromyographic (EMG) muscle activity and alter sagittal plane ankle motion and ankle power. This type of footwear utilizes multisegmental rocker designs. A less plantar flexed ankle position during loading response and an increase in ankle moments has been noted with this type of footwear compared to unadapted footwear. 11 However, the toe rocker shape incorporated in these designs has been shown to produce minimal alterations during late stance. The long-term effects of wearing “unstable” footwear require further investigation to enable a more enhanced understanding of the long-term implications of wearing unstable-type shoes.11,12–14
Previous studies have therefore demonstrated that clinically significant alterations to sagittal plane ankle kinematics may be expected when healthy subjects walk with shoes adapted with conventional rocker sole designs. A negative heel rocker sole has been defined as one that places the height of the anatomical heel at the same level or below that of the metatarsal heads during static stance. 15 Myers et al. demonstrated that when healthy subjects walked with a negative heel shoe, a mean reduction in ankle dorsiflexion after mid stance of 4° and an increase in maximal plantar flexion at initial swing of 4° may be expected. However, the rocker angles used, apex positions, and alterations to the heel sole differential heights 16 were not accurately defined. In addition, a previous study by Li and Hong 17 demonstrated that a negative rocker that placed the ankle in 10° of dorsiflexion during static stance produced the opposite effect in that it produced a 6° more dorsiflexed position at initial contact and a mean dorsiflexion shift during stance and swing of approximately 5°. There is therefore variance in the literature. Long et al. 18 demonstrated that a double-rocker sole shoe had minimal effects on ankle kinematics except for a mean increase in plantar flexion during pre-swing of less than 2°. Van Bogart et al. 19 when investigating the effects of a toe-only rocker sole compared to a baseline shoe demonstrated that a small increase in plantar flexion at initial contact (less than 2°), but again a mean reduction in ankle dorsiflexion after mid stance, and an increase in maximal plantar flexion at initial swing may be expected; but limited to less than 2°.
Rocker soles have been shown to produce positive effects such as forefoot plantar pressure reduction. However, it may also be possible to design a rocker sole with its profile comprising more than one curve in an attempt to reduce sagittal plane ankle motion for patients with midfoot osteoarthritis and midfoot fusions. This could feasibly be achieved by designing rocker soles comprising curves with differing radii along the base of a shoe. A posterior curve with a relatively small radius (assuming circular) would theoretically attempt to reduce ankle plantar flexion during loading response by acting as a surrogate shape and to roll the foot toward a central apex with a curve of larger radius that would gently roll the foot forward during mid stance before utilizing an anterior rocker to provide heel lift prior to swing. This could prove effective in reducing symptoms in subjects with ankle, rearfoot, and midfoot osteoarthritis who experience pain during ambulation or for the postoperative protection of subjects who have undergone subtalar or rearfoot surgical fusion.
A literature review in this field has demonstrated that the effects of rocker profiles on gait parameters differ based on the rocker sole design. 4 Myers et al. 15 reported no change of speed of walking and an increase in cadence when using a negative heel rocker sole compared to baseline. Other studies in this field have demonstrated no differences in cadence, step length, and speed of walking when using a rocker sole.20,21
Studies have also investigated the effect of different single-curve rocker sole radii on ankle–foot roll-over shapes based during gait laboratory testing 22 in able-bodied subjects. Roll-over shapes have been shown to not change appreciably while subjects walk at different speeds, or when wearing shoes of different heel heights, nor indeed those with different rocker sole radii added. In fact, results suggest that able-bodied humans actively alter their ankle movements to maintain the same resultant roll-over shapes during stance phase when walking with shoes that utilize different rocker sole radii.22–24
It has been demonstrated that a rocker profile with its apex at 40% of shoe length (based on the distance from the back of the heel relative to the total shoe length) and a single circular rocker profile radius equivalent to 25% of leg length can significantly reduce ankle joint sagittal plane ROM during stance phase to approximately 15° and that smaller radii produce more reductions in sagittal plane ankle motion than those with larger radii. 24 A rocker profile may therefore theoretically aid forward progression of the tibia where sagittal plane ankle motion is already restricted and therefore facilitate shank advancement over a stationary foot. 25
Some authors have recommended the use of a curved rocker sole shoe or one with a rocker profile in tandem with a cushioned heel in the treatment of patients with restricted ankle motion following surgical fusion or arthritic changes to the ankle or midfoot structures.18,25–29 The cushioned heel is designed to simulate plantar flexion and cause an early transition to second rocker of gait. 27 This led to the hypothesis for this study that a specifically designed rocker sole profile could induce restriction to sagittal plane ankle motion in healthy individuals during ambulation without the need for a cushioned heel. Specifically, it was thought that a multicurved rocker sole may prove effective in reducing ankle sagittal plane ROM by offering a surrogate shape to the base of the shoe, which could also be of benefit for subjects requiring the use of a fixed ankle–foot orthosis (AFO). The aim of this study was therefore to evaluate the differences in gait kinematics and kinetics plus temporal–spatial parameters caused by the use of footwear to which bilateral heel-to-toe rocker soles had been added.
Methods
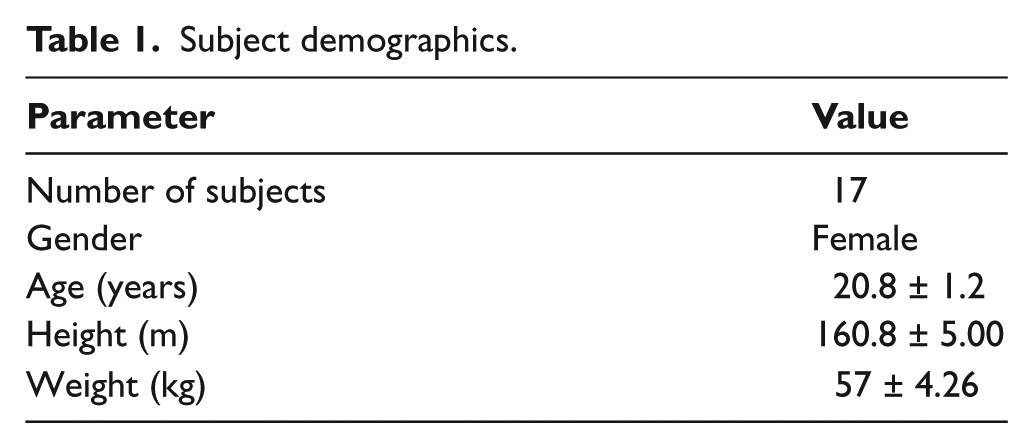
Seventeen healthy adult volunteers (females; age = 20.8 ± 1.2 years) were invited for participation in this study (Table 1). An analysis of 25 previously published studies was performed, and based on the number of male or female subjects utilized in these studies, a patient number (n = 17) was deemed to be appropriate to produce meaningful data for this study.
Subject demographics.
A complete physical evaluation was utilized to assess the presence of any neurological or musculoskeletal dysfunction. Subjects with a history of orthopedic abnormalities in the trunk, back, or lower extremities were excluded from this study.
Data collection was performed at the Motion Analysis Laboratory in the Department of Ergonomy at the University of Social Welfare and Rehabilitation Sciences. Each person walked with two pairs of shoes. One pair had a flat sole, which was used as a baseline condition (Figure 1). The toe spring on the baseline shoe equated to a 7° rocker angle at the toe end of the baseline shoe. The other pair was adapted with a heel-to-toe-type rocker sole to serve as an intervention shoe (Figures 2 and 3). The rocker sole was designed with a rear rocker curve at the heel with a relatively small radius and an anterior curve with a larger radius. The central portion was virtually flat. The rocker profile chosen was one that comprised three components in order to facilitate a reduction in ankle sagittal plane ROM. The center point of the central portion between the two main curves was positioned at 50% of shoe length (measured from the back of the heel) in order for the shoe to be able to gently rock using the anterior and posterior curves to potentially facilitate a reduction in rearfoot and forefoot motion and to make the sole unit stiffer as compared to the baseline shoe. In this way, the rocker profile would potentially act as a surrogate shape to reduce the need for the foot and ankle complex to dorsiflex and plantar flex and also to reduce metatarsal head rotation during late stance.

The baseline shoe used in this study.

The heel-to-toe rocker sole used in this study.
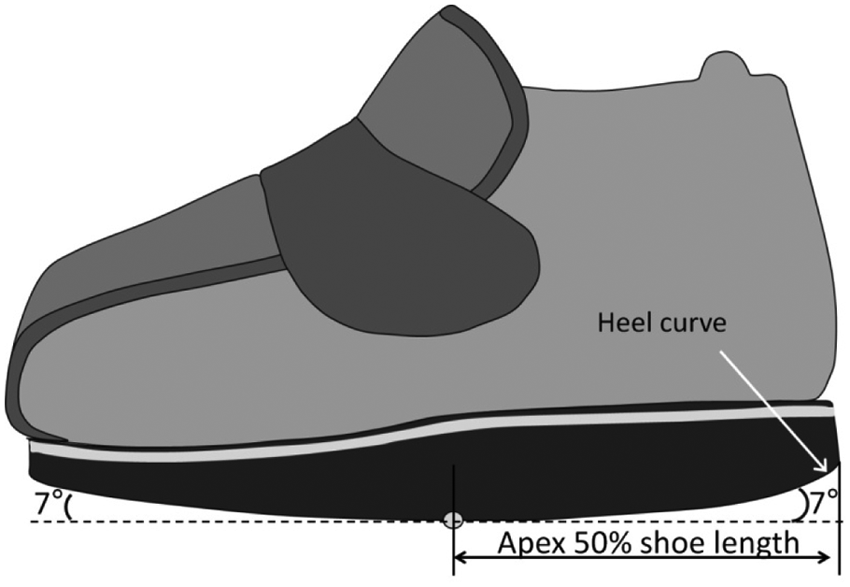
Representation of the heel-to-toe rocker sole used in this study.
Each pair of modified footwear was individually prepared by the orthotist according to the subject’s measured shoe size using a standardized pattern with the profile of the heel-to-toe rocker sole designed, so that the heel rocker finished at a point 25% of shoe length and the toe rocker began at a point equivalent to 65% of shoe length relative to the back of the heel with a short central flatter section between these points. The curve immediately posterior to center line created a rocker angle equivalent to 7° to the horizontal, and the anterior curve created a similar profile. The heel curve was based on a radius from ankle joint center. The sole and heel units were altered using the same microcellular rubber with a Shore value of 35–40 (Shore A durometer), and a sole strip was added to ensure minimal bending during walking trials.
For each subject, gait analysis was performed under the two test conditions (the baseline shoe with a flat sole and the modified shoe with the heel-to-toe rocker sole added) in a randomized order. Previous studies have demonstrated no carryover effects of different rocker soles when analyzing and comparing their effects on gait kinetics and kinematics during same-session testing.15,18,19 Five walking trials were conducted for each test for each subject. Subjects walked at their own comfortable self-selected walking speed. A short period of acclimatization was allowed prior to each walking trial when wearing either of the tested footwear conditions. A Vicon digital motion capture system (Vicon 640; Oxford Metrics, UK) using six cameras (Vicon, Infrared) at a frequency of 100 Hz and two force platforms (Kistler 9286BA, Switzerland) were used for data capturing from markers. Kinematic analysis was performed in this study using the three-segment rigid model technique described by Su et al. 30 A total of 24 markers (3 markers each) were used bilaterally positioned on the tibia, gastrocnemius, Achilles tendon, calcaneus, medial and lateral malleolus, and the base and head of fifth and first metatarsals. Subjects walked with their self-selected speed, and rest times were considered if subjects needed them between trials. Static and dynamic calibrations were performed before each assessment. This study was approved by the ethical committee of University of Social Welfare and Rehabilitation Sciences; all participants provided informed consent before being evaluated.
The data were averaged for the right lower limb once confirmation was obtained demonstrating no significant differences when comparing the data of right and left limbs for the outcome measures analyzed. Data were analyzed during the following points in the gait cycle: initial double-limb support (0%–10% of gait cycle), single-limb support (10%–50% of gait cycle), second double-limb support (50%–60% of gait cycle), initial swing (60%–73% of gait cycle), mid swing (73%–87% of gait cycle), and terminal swing (87%–100% of gait cycle). 31 The normality of data was approved by using the Kolmogorov–Smirnov test, and a paired t-test was used for comparing the efficacy between the two types of rocker soles. SPSS statistical software was used for analysis of data. The level of significance was set at 0.05.
Results
Temporal and spatial parameters
The mean of the temporal–spatial data (walking speed, stride length, and cadence) when using the two test conditions is shown in the Table 2. No significant differences were demonstrated for any of these parameters.
Mean ± SD of the spatial and temporal parameters.
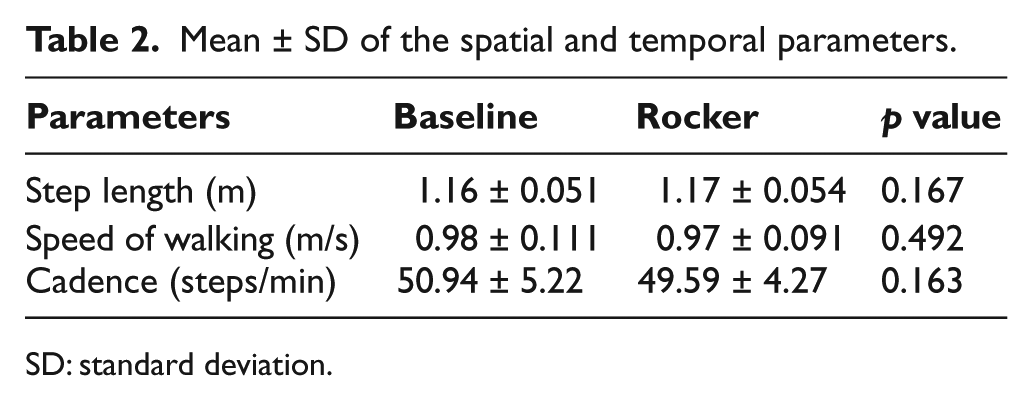
SD: standard deviation.
Joint kinematics
Table 3 shows the mean ankle dorsiflexion and plantar flexion movement measured when walking with the test conditions during specific points in the gait cycle. During initial double-limb support and second double-limb support, significant differences were observed between the rocker sole conditions (p = 0.024 and 0.010, respectively). Figure 4 shows that the maximum plantar flexion during loading response when walking with the rocker sole condition and the baseline condition was 7.8° and 13.4°, respectively. The maximum dorsiflexion during terminal stance in walking with the rocker test condition was 9.2° and in walking with baseline shoe was 13.2°, and the total maximum sagittal plane ROM of the ankle joint for the rocker condition was 17.0°, and in baseline condition, it was 26.6°.
Mean ± SD of the sagittal plane ankle motion during specific points in the gait cycle.
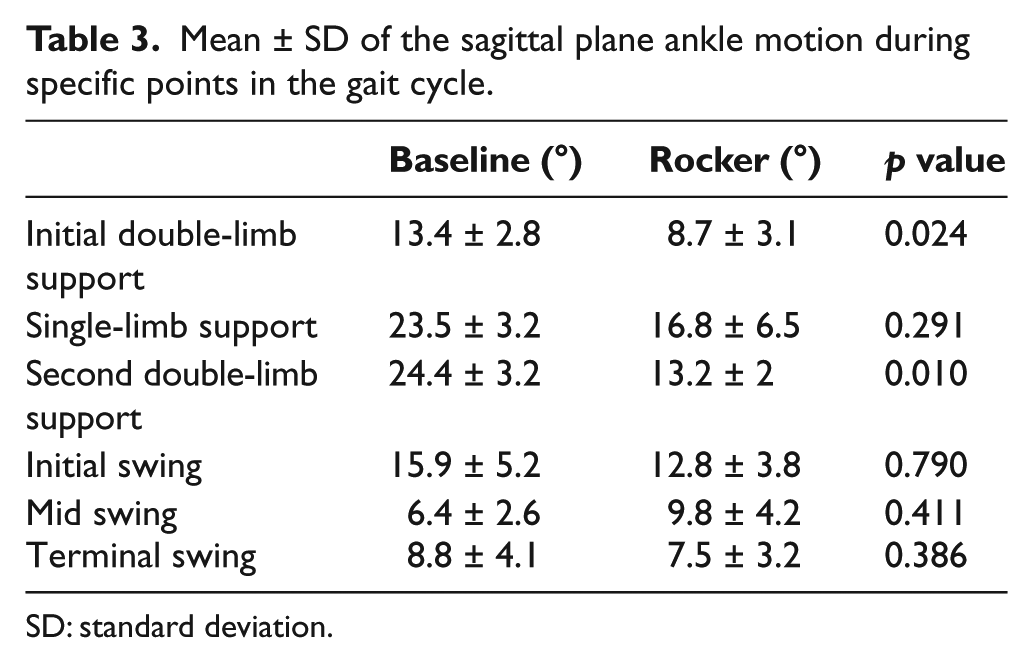
SD: standard deviation.
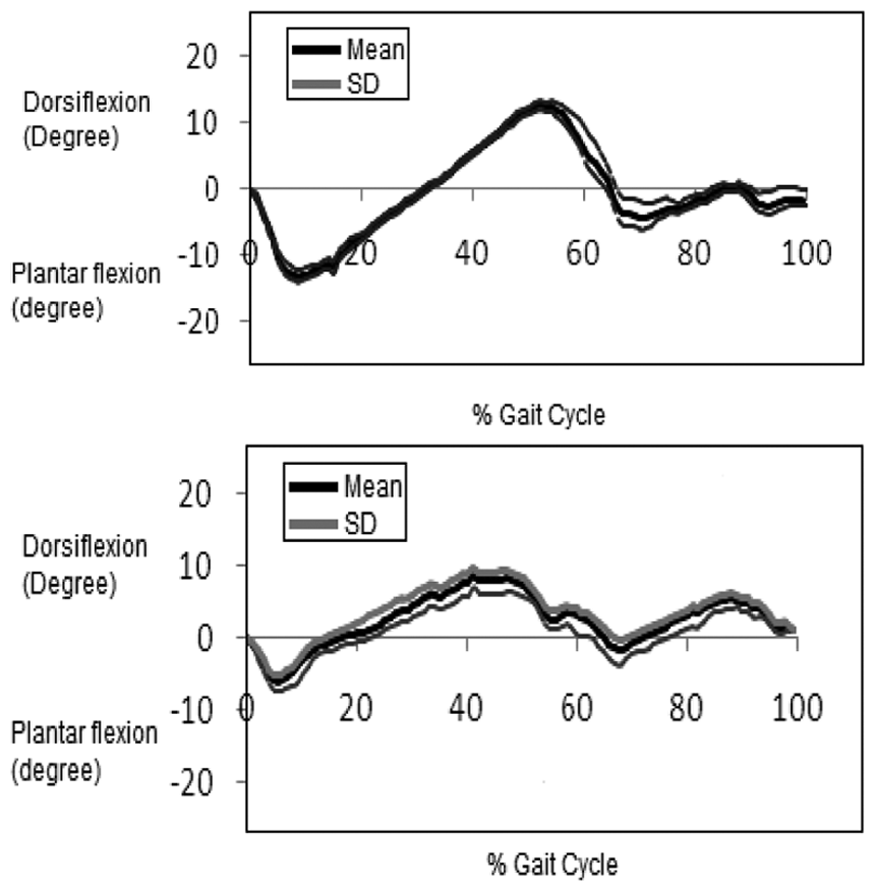
Mean ankle joint movements in the sagittal plane with the baseline shoe and the heel-to-toe rocker sole shoe for all subjects.
Table 4 and Figure 5 show inversion and eversion movements and data of shoe inversion and eversion, respectively, during the walking trials. Significant differences were only observed between test conditions during the second double-limb support phase of gait.
Mean ± SD of the inversion and eversion movements.
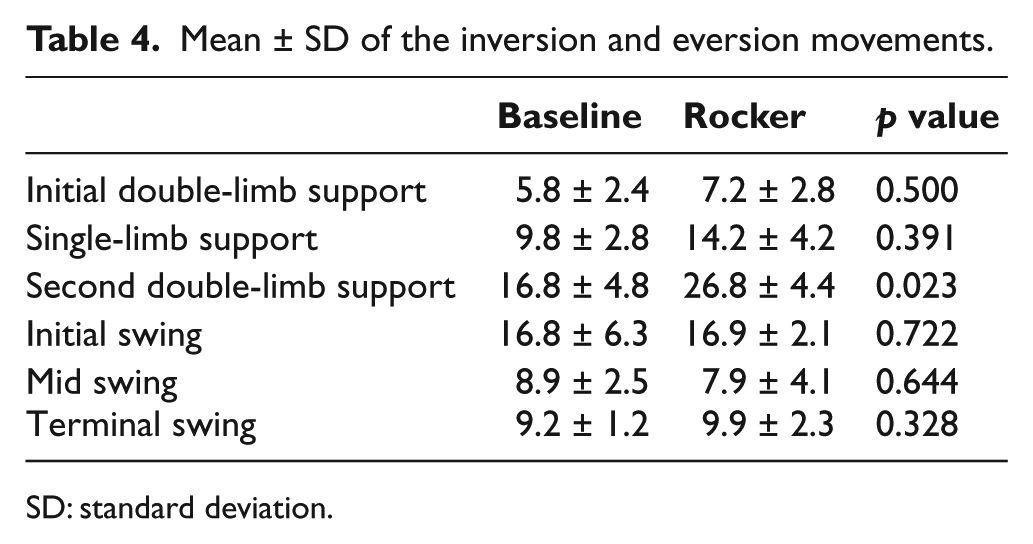
SD: standard deviation.
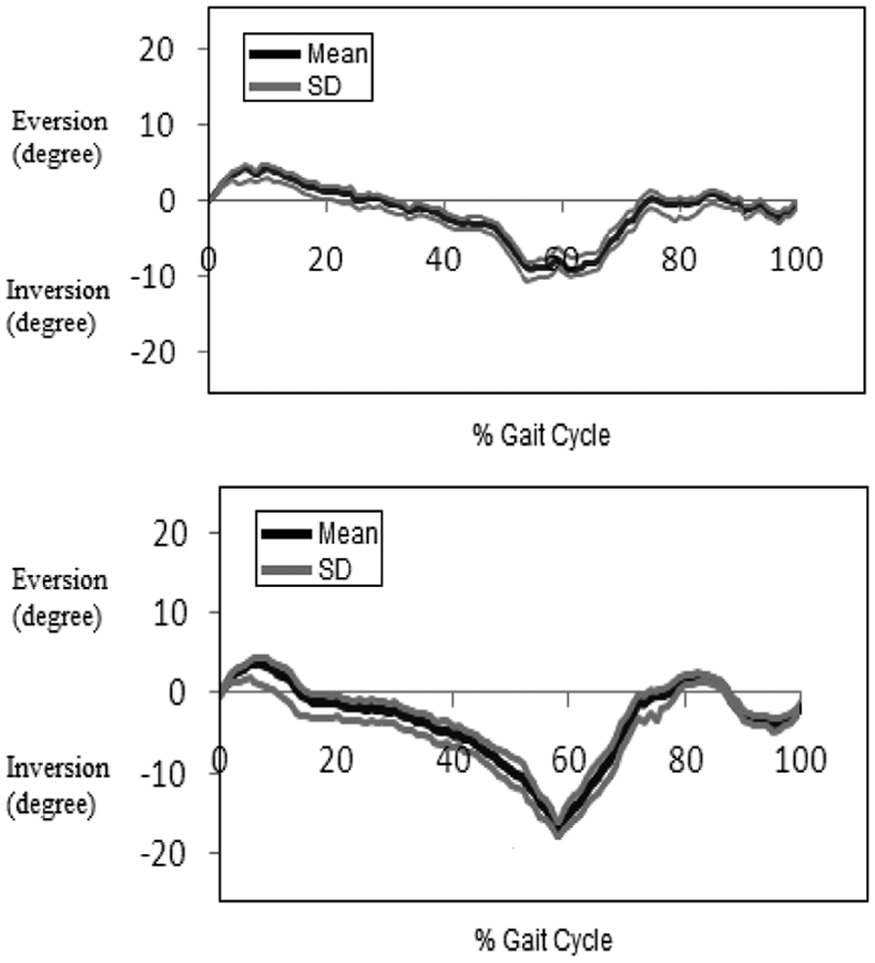
Mean ankle joint movements in the frontal plane with the baseline shoe and the heel-to-toe rocker sole shoe for all subjects.
Discussion
The most encouraging aspect of the results was that while the heel-to-toe rocker sole when compared to baseline footwear during ambulation did not significantly alter the specific temporal–spatial parameters tested (i.e. speed of walking, step length, and cadence), it did significantly reduce the sagittal plane kinematics of the ankle joint which the authors regard as clinically significant. This therefore means that it could potentially be suitable for the treatment of subjects with foot and ankle pathologies who have restriction of motion in the rearfoot or midfoot.
There is variance in the literature regarding the effect of different rocker soles on cadence, step length, and walking speed, depending on the design of rocker profile studied. Myers et al. 15 demonstrated that speed of walking was not significantly altered when subjects walked with a negative heel rocker shoe comparing to baseline, but an increase in cadence was reported. However, various other studies have demonstrated no difference in these parameters when walking with rocker sole footwear,17,18 but these investigations compared the effect of different designs of rocker sole profiles to the one included in this study and may not be directly applicable. Van Bogart et al. 19 reported a reduction in stride length and an increase in cadence with an unaltered speed of walking when using the toe-only curved rocker sole compared to baseline.
Studies investigating the effect of shoes with so-called unstable shoes, which comprise a multicurve rocker profile in the sole and heel unit, have demonstrated that they are effective in reducing pain levels in subjects with osteoarthritic changes in the foot, but they also place the ankle into a less plantar flexed position during loading response compared to normal, and this relatively dorsiflexed position continues toward mid stance.32,33 This would not be suitable where a decrease in sagittal plane ROM is required. However, the results of this study demonstrate that the heel-to-toe rocker sole may be indicated for patients who have undergone an ankle arthrodesis due to its effectiveness in reducing ankle joint ROM while maintaining a typical ankle kinematic trajectory pattern and timing. In addition, this type of rocker sole may also be suitable for use in combination with AFO where restriction in ankle sagittal plane motion is required. Future evaluation of this type of rocker sole when used with different AFO designs is therefore warranted. In this study, significant differences were noted in sagittal plane kinematics during double-limb support phases of gait compared to baseline.
Another important finding of this study was the significant differences demonstrated in eversion and inversion during second double-limb support. This demonstrated that during this phase of gait, ankle eversion and inversion was approximately twice that compared to baseline when walking with the heel-to-toe rocker sole in healthy subjects. This may have been due to the flexible upper included in the footwear used for this study and requires further investigation. Based on this finding, the heel-to-toe rocker sole may not be suitable for patients with reduced balance because walking in this rocker produced a shorter mid stance compared to baseline.
In this study, we evaluated a heel-to-toe rocker sole on healthy female subjects. This is a limitation of this study, and the results cannot be assumed to be valid for male adults. The footwear chosen for testing while appearing to be effective in preventing forward and backward motions due to the touch and close instep fastening and the fact that they were a bootee were not substantial enough to control inversion and eversion effects. In addition, the testing method was designed for subjects to be instructed to walk at their self-selected walking speed for both conditions. In order to isolate the effect of the rocker sole addition to the footwear, it would have been necessary to also perform walking tests while maintaining the similar walking speeds during both test conditions. This is also a limitation in this study. However, the overall aim was to determine the effect that the rocker sole would have in healthy individuals while walking at the speed they would actually walk when using the rocker sole shoe by taking account of any alteration to walking speed.
The evaluation of this type of rocker sole should be assessed in a further study in persons with diabetes and/or peripheral neuropathy, as it may reduce plantar pressures. However, due to its multicurve construction, investigations into its stability in all planes when added to footwear with more substantial uppers and worn by subjects with peripheral neuropathy would initially be needed. Only the immediate effect of the heel-to-toe rocker sole was assessed in this study. Its effects during an extended episode of period of treatment in this patient population compared to a control group may therefore be warranted. The important effect of the heel-to-toe rocker sole modification appears to be a beneficial limitation of ankle joint ROM. Further assessment is required to evaluate alterations in kinetics and kinematics at the knee and hip joints and their relationship to the previously measured ankle joint movement pattern in order to ascertain any proximal joint effects that may affect balance. Future work in the field utilizing this type of rocker sole may also include evaluations of postural stability and energy consumption changes.
Conclusion
The positive findings from this study were the reduction in sagittal plane ankle motion demonstrated during stance without any significant alterations to temporal–spatial parameters. The main purposes of a heel-to-toe rocker sole prescription are to facilitate forward progression of the tibia when used with AFO or to facilitate easier walking for those subjects who have undergone an ankle arthrodesis. With regard to kinematics of ankle joint, significant differences were observed during initial and second double-limb support phases in reducing dorsiflexion and plantar flexion ROM of the ankle joint. However, significant differences were also observed during second double-limb support in the frontal plane rotation of ankle joint, meaning it may prove unstable laterally for some patients. Further investigations into the effect of this type of footwear adaptation are therefore warranted.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.