
Abstract
Background:
A powered knee–ankle–foot orthosis was developed to provide restriction of knee flexion during stance phase and active flexion and extension of the knee during swing phase of gait.
Objective:
The purpose of this study was to determine its effect on the physiological cost index, walking speed and the distance walked in people with poliomyelitis compared to when walking with a knee–ankle–foot orthosis with drop lock knee joints.
Study design:
Quasi experimental study.
Methods:
Seven subjects with poliomyelitis volunteered for the study and undertook gait analysis with both types of knee–ankle–foot orthosis.
Results:
Walking with the powered knee–ankle–foot orthosis significantly reduced walking speed (p = 0.015) and the distance walked (p = 0.004), and also, it did not improve physiological cost index values (p = 0.009) compared to walking with the locked knee–ankle–foot orthosis.
Conclusion:
Using a powered knee–ankle–foot orthosis did not significantly improve any of the primary outcome measures during walking for poliomyelitis subjects.
Clinical relevance
This powered knee–ankle–foot orthosis design did not improve the physiological cost index of walking for people with poliomyelitis when compared to walking with a knee–ankle–foot orthosis with drop lock knee joints. This may have been due to the short training period used or the bulky design and additional weight of the powered orthosis. Further research is therefore warranted.
Keywords
Background
Knee–ankle–foot orthoses (KAFOs) are prescribed for individuals with a range of conditions such as poliomyelitis, degenerative muscle disease, stroke or incomplete spinal cord injury. Conventional KAFOs incorporating drop lock type orthotic knee joints hold the knee in extension during walking activities and are unlocked for activities such as sitting. This therefore produces an abnormal gait pattern during ambulation, which has been linked to pain and loss of motion in the hip and lower back.1,2 Increased upper-body lateral sway, increased ankle plantarflexion of the contralateral foot (vaulting), hip elevation during swing phase (hip hiking) or circumduction may also occur. 3
Walking with the knee locked in extension means there is an inability to flex the knee during loading response (LR) which causes an abrupt initial loading and also disrupts the smooth progression of the centre of mass (COM) of the body 4 as well as increasing its vertical displacement by up to 65%. 5 This can result in a high energy consumption and premature fatigue for the KAFO user,2,6 which may lead to rejection of the orthosis. 6
Stance-control knee–ankle–foot orthoses (SCKAFOs) are KAFOs which are designed to provide flexion during swing phase and stability during stance phase when ambulating. 7 Previous studies have shown that SCKAFOs provide a more symmetrical gait, improved mobility and also reduce the amount of compensatory motion which occurs when walking compared to that seen in conventional KAFOs.2,6,8,9 However, they do not routinely provide active flexion and extension of the knee throughout the gait cycle.
A powered KAFO (Figure 1) was developed to provide active knee flexion and extension during swing phase of gate while providing stability during stance in subjects with quadriceps weakness, 10 and its feasibility has been evaluated in healthy subjects in a previous study. However, the purpose of this study was to evaluate its effect on the physiological cost index (PCI) of walking (a proxy measure of energy consumption) by a group of subjects with poliomyelitis.
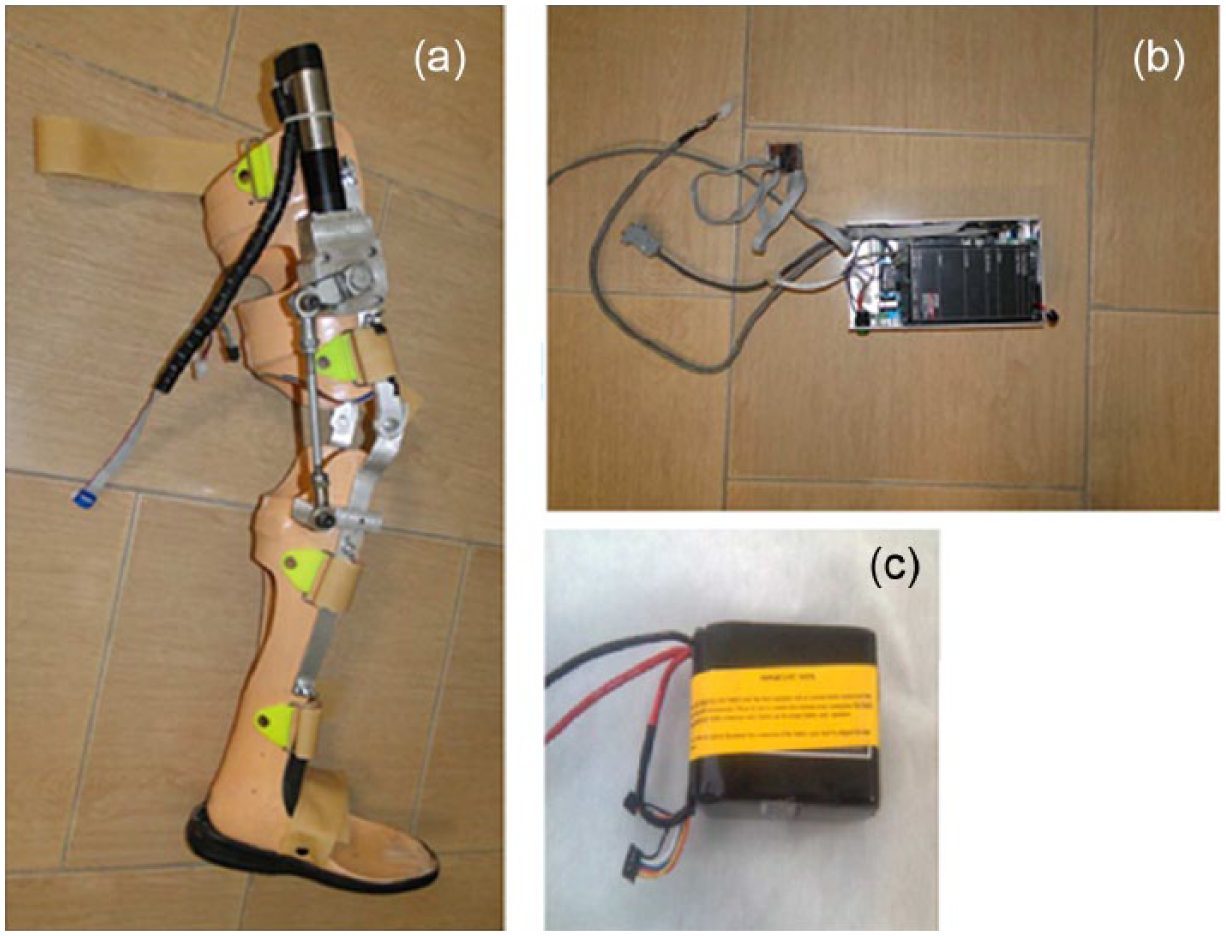
(a) Powered orthosis used in this study, (b) control unit and (c) rechargeable 24 V battery.
Methods
Subjects
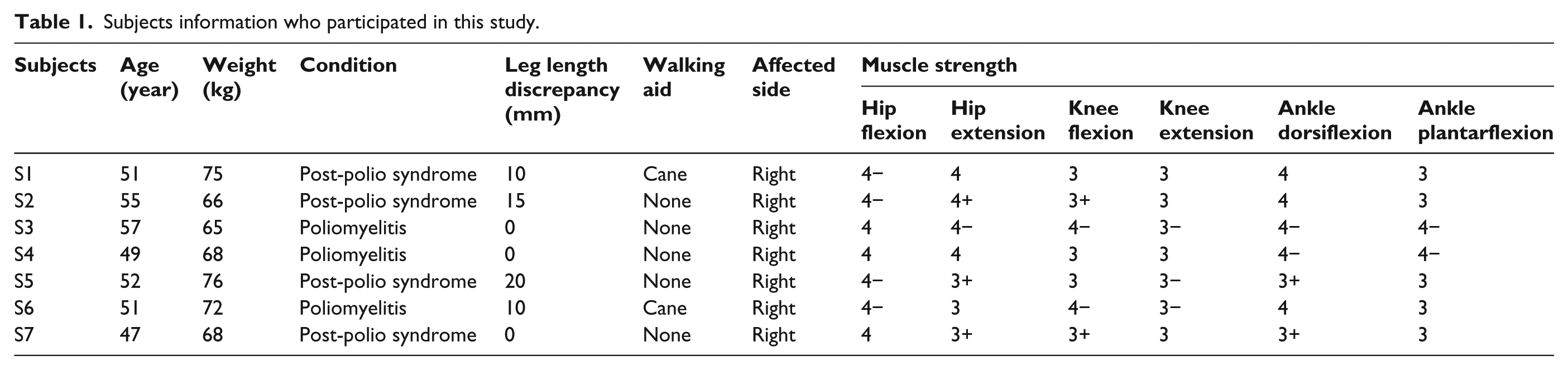
Seven subjects with poliomyelitis participated in the study. Inclusion criteria included those subjects who routinely used KAFOs either unilaterally or bilaterally with lockable orthotic knee joints, with the ability to walk a minimum of 50 m and the presence of sufficient hip flexor strength to advance the affected limb during swing phase. Exclusion criteria included the existence of impaired cognition, weak balance, a history of pain in the back or in the upper or lower limbs, or the existence of joint contractures greater than 15° at the hip, 10° at the knee or 5° at the ankle. Muscle strengths at the hip were assessed manually and were required to be at a minimum level of 3 based on the Oxford scale. The study was approved by the Human Ethics Committee of the University of Social Welfare and Rehabilitation Sciences. Informed consent was obtained from all subjects prior to participation in the study. Table 1 shows the relevant subject demographics.
Subjects information who participated in this study.
Leg length discrepancy
Four of the volunteer subjects had a fixed equinus deformity at the ankle due to leg length discrepancy on the effected lower limb; so it was necessary to add accommodative heel elevators mounted on an inlay added to the footplate of the ankle–foot orthosis (AFO) sections within the respective powered KAFOs. Heel elevators of 10, 15, 20 and 10 mm depth at the heel were constructed from crepe material and cemented onto the inlay for subjects numbered 1, 2, 5 and 6, respectively.
Gait training
After having been casted, measured and fitted with two types of bespoke cosmetic KAFO, all subjects attended a rehabilitation centre for 10 days to undergo a standardized training programme which consisted of five 2-h sessions per week which included passive stretching of the lower extremities, upper limb strengthening exercises, balance training in the standing position, gait training, donning and doffing of the orthosis and sit-to-stand training. This approach was performed under controlled and supervised conditions in order for the patient to achieve confidence and experience in balance, standing and walking with the orthosis. This ensured each subject could walk independently with the orthoses before taking part in the data collection for this study.
Interventions
Each subject was fitted with the two bespoke KAFOs by a certified orthotist. Both KAFOs were fabricated with moulded thigh cuffs and solid AFOs manufactured from copolymer polypropylene of 4 mm thickness. Both orthoses utilized medial and lateral uprights which were manufactured in aluminium. One KAFO utilized drop lock orthotic knee joints, while the powered KAFO incorporated single-axis free knee joints. A 40-W electric actuator (Maxon Motor EC-max30; Maxon, Switzerland) with a planetary gearbox providing a reduction ratio of 111 was attached to the lateral orthotic knee joint in the KAFO. The powered KAFO was designed to restrict knee flexion at any angle in the stance phase, and when the foot progressed into swing phase, the actuator flexed the knee joint actively and then actively extended it ready for heel strike. To eliminate fitting discrepancies which may have impacted the results, both orthoses were made of the same cast aluminium.
Control of the orthosis
A closed-loop position control system was used in the powered orthosis. In order to recognize heel strike, an indirect torque meter was used based on the electrical current consumption of the actuator when it passed a definable threshold under the sudden increased load on the leg. After heel strike, when a specific load had been applied on the joint, the movement cycle was triggered according to a pre-defined threshold in the software until at full unweighting the joint was driven into flexion. The end point of the flexion cycle was recognized due to closed-loop position control by a powerful controller and the software. After reaching the maximally flexed knee position (45° of knee flexion), a definable delay could be adjusted for various walking speeds and consequently joint extension would occur at the right position to return the joint to its primary position for the next stride.
A single rechargeable 24 V battery (Lipo Battery, Thunder Power RC G6 Pro Lite 25C 5400mAh 6-Cell/6S, Thunder Power RC company, USA) with 2 h of available continual power was used to provide power for the actuator. The battery and electronic unit (total weight = 0.7 kg) were placed on the subject’s waist belt. The additional componentry of the new powered KAFO meant that it weighed 0.8 kg more than the unpowered orthosis. Figure 1 shows the powered orthosis used in this study.
Experimental approach
Walking speed was measured via a stop watch and also measuring the distance walked. Subjects were asked to walk using the KAFO with drop lock knee joints or the powered KAFO in a random order along a pre-determined 40 m rectangular walkway at their self-selected speed.
A Polar Heart Rate monitor was used to evaluate the PCI. Heart rate at steady-state walking (HRss) and heart rate at rest (HRar) were measured, and the following formula was used to measure the PCI

To obtain a baseline level of the PCI, subjects sat quietly for 10 min prior to any measurement. The PCI measurement regime consisted of an initial 5 min of complete rest in a sitting position, 5 min in a standing position, walking with the orthosis for 6 min at their self-selected walking speed and a final 2 min of rest in the seated position. During resting, standing and walking, the heart rate was calculated every 15 s. After 10 min of rest in the sitting position with the next orthosis, the next evaluation and measurement were started. The mean of heart rate during the final 2 min of rest in the sitting position was considered as HRar and average heart rate during the 6-min walking test with the orthosis was considered as HRss. 11
Bailey and Ratcliffe evaluated the reliability of PCI analysis in a test–retest condition when the heart rate is measured in a non-steady-state, steady-state or 10 s post-exercise condition in normal women walking at preferred speed on a treadmill. This study demonstrated that for best repeatability, steady-state conditions should ideally be achieved for the walking heart rate measure. It was proposed that a more accurate resting heart rate may be recorded during the recovery period rather than at the beginning of the walk test. 12
The two orthosis conditions used were randomly assigned to each subject. Before data collection, the subjects were allowed 30 min to provide an accommodation time for each device. A 1-h washout period was used between each orthotic test condition before collection of data. None of the subjects required the assistance of a cane or walking aid during the testing, although two of the subjects routinely used a cane for longer distances.
Statistical analysis
Normality of the data was confirmed using the Kolmogorov–Smirnov technique. A paired t-test was used to compare the two orthoses. SPSS statistical software (JMP IN Software; SAS Institute, Inc.) was used for analysis of the data. The level of significance was set at 0.05.
Results
The mean ± standard deviation (SD) of walking speed, distance walked and PCI when walking with a locked KAFO as a control condition and a powered KAFO are shown in Tables 2 and 3. There was a statistically significant reduction in both walking speed (p = 0.015) and the distance walked (p = 0.004) when ambulating with the powered KAFO compared to a locked KAFO (Table 2). The powered KAFO also significantly increased the PCI of walking compared to the KAFO with drop lock orthotic knee joints (p < 0.009; Table 3).
Mean ± SD and comparison of speed of walking and distance walked during the two orthotic conditions.
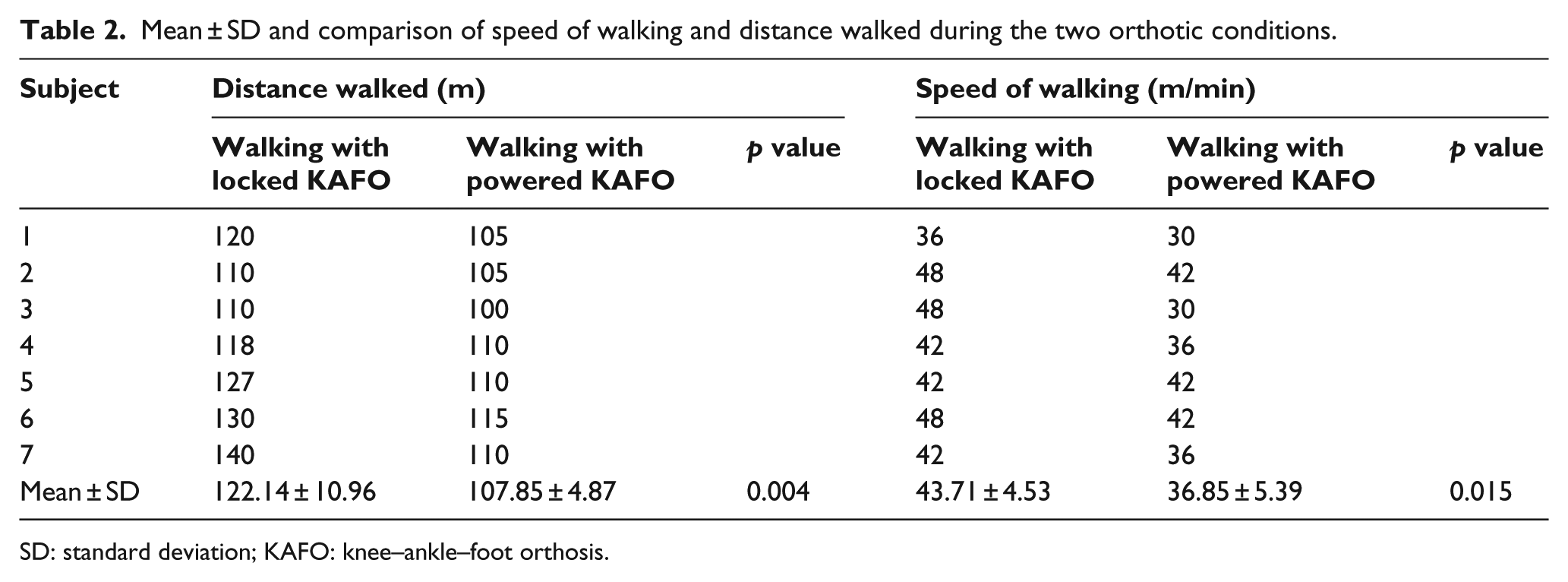
SD: standard deviation; KAFO: knee–ankle–foot orthosis.
Mean ± SD and comparison of PCI during the two orthotic conditions.
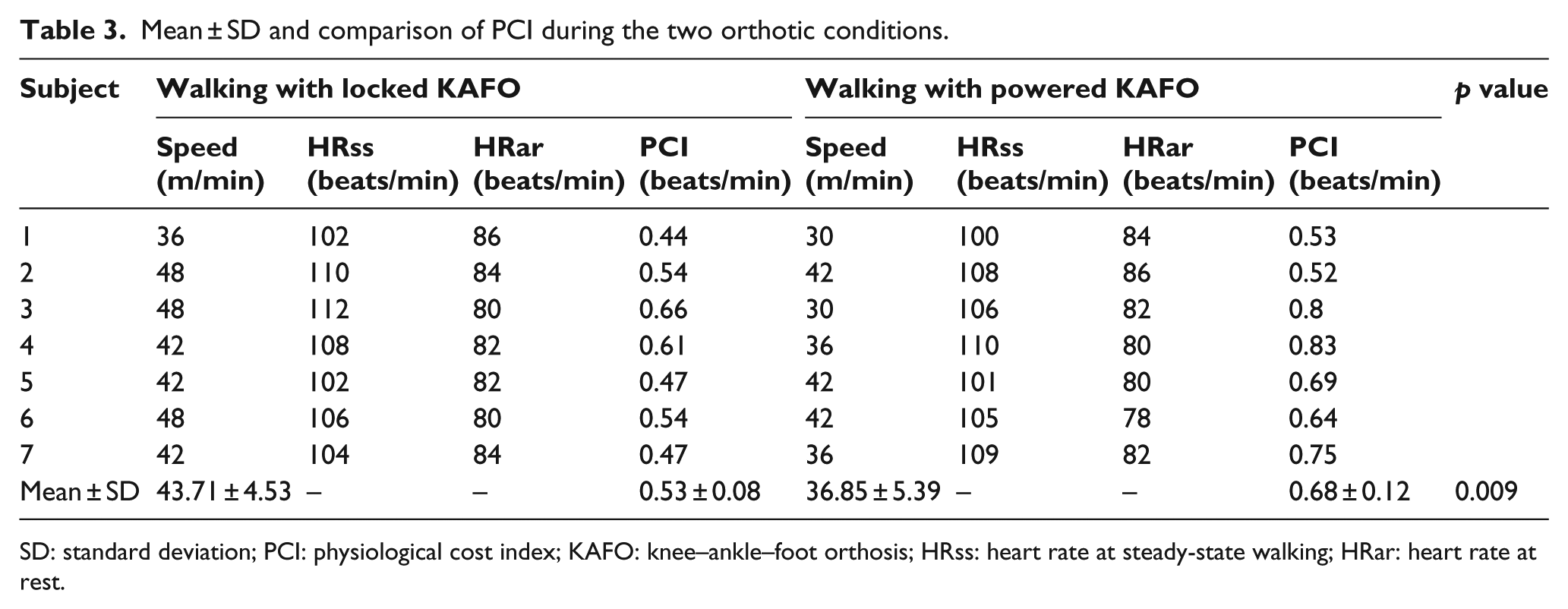
SD: standard deviation; PCI: physiological cost index; KAFO: knee–ankle–foot orthosis; HRss: heart rate at steady-state walking; HRar: heart rate at rest.
Discussion
The aim of this study was to evaluate the effect of new powered KAFO on walking speed, distance walked and the resulting PCI in poliomyelitis subjects. The results of this study demonstrated that using the powered orthosis had no beneficial effect in improving any of the primary outcome measures. All subjects experienced a reduced walking speed, a shorter walking distance and an increased PCI compared to a KAFO with more conventional orthotic knee joints as a control condition.
Direct measurement of heart rate was used to demonstrate the value of physical effort exerted when walking with the two test conditions. 11 In this study, the results of the PCI measurement showed that poliomyelitis subjects walked with increased energy consumption when using new powered KAFO. All the subjects in this study were experienced KAFO users, and the gait performance when walking with the powered KAFO may further improve with more experience of using the orthosis for long-term use.
According to our knowledge, this study is first which has evaluated the effect of walking with a powered KAFO on energy consumption in poliomyelitis subjects, and only three studies have evaluated energy consumption rates in poliomyelitis subjects when wearing SCKAFOs compared to KAFOs with the knee joint locked in position.13–15 Although SCKAFOs provide knee flexion during swing phase and prevent knee flexion in stance phase during walking, this type of orthoses has also not shown a significant improvement in reduction of energy consumption.13,14 Active flexion and extension of the knee joint during the whole of the gait cycle, and particularly during stance phase, are not provided by all current SCKAFO designs. This point is a potential advantage of a powered KAFO over a SCKAFO.
In this study, wearing the new KAFO decreased gait velocity compared to the conventional KAFO. A typical walking speed in the healthy adult population has been quoted as being 1.3 m/s (10). The mean of this parameter in studies involving poliomyelitis subjects has been shown to be 1.18 (13), 0.82 (9), 0.8 (14), 0.59 (8), 0.63 (19), 1.04 (18) or 0.61 (20) m/s when using a mechanical stance-control orthosis (SCO) for ambulation, while when wearing a powered SCO, this parameter has been reported to be 0.57 m/s (21). The average for this study was 0.61 m/s. There is variance in the literature as to the effect of SCKAFOs on walking speed.2,7,8,13,15,16–18 Irby et al. reported that using the dynamic knee brace system (DKBS) in novice KAFO users increased velocity and cadence over the traditional locked KAFO. Using the new orthosis in their study increased knee range of motion in the novice group compared to the experienced group, but peak knee extension moments tended to be greater for the experienced group. 8 In another study by Irby et al., 9 gait analysis of 14 SCKAFO users with the DKBS during 6 months of use demonstrated that all subjects significantly increased peak knee flexion, peak hip flexion, velocity, stride length and cadence over this extended period.
A limited accommodation time of 2 weeks and the increased weight afforded by the powered knee joint mechanism may be the main reasons for the non-significant findings in this study. The subjects who participated were experienced conventional KAFO users and therefore routinely walked with circumduction and hip hiking during ambulation. Although the step length of subjects was not evaluated in this study, a decreased step length may have caused the reduction in walking speed measured. A reduction in step length has previously been reported for poliomyelitis patients when walking with a SCKAFO.8,16
The number of participating subjects was small in this study, and as a result, the findings cannot be generalized to the larger population. More studies are therefore needed to analyse this effect further. Only pelvic obliquity was analysed in this study, and neither ankle angle (vaulting) nor hip rotation (circumduction) was investigated in this study, which will need to be investigated in future studies.A more comprehensive evaluation of kinematic and temporospatial parameters and electromyographic analysis may assist in understanding the underlying training or orthotic effects of KAFO wear. Evaluation of this orthosis on a further cohort of patients utilizing longer training periods for walking in subjects with quadriceps weakness will also be beneficial. It would also have been beneficial to compare the powered orthosis to a SCKAFO rather than a KAFO with drop lock orthotic knee joints. A reduction in knee joint bulk and weight, as well as development of more advanced control software, will be considered as key elements for future studies. Adequate gait training and accommodation with the orthosis with a new control mechanism will be required before wearing a powered KAFO.
Conclusion
Using the powered KAFO did not reduce the PCI of walking in subjects with poliomyelitis. Powered KAFOs have the potential to reduce energy consumption and user effort during walking, but this current design did not achieve this goal. The short training period and the increased bulk and weight afforded by the mechanism could be the reason for the limited findings in this study, and further research is needed to explore the influence of a powered KAFO in individuals with neurologically related lower limb weakness.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financially supported by the Iranian National Science Foundation (INSF; grant no. 92001422).