
Abstract
The objective of the study was to compare the Physiological Cost Index (PCI) and walking speeds during walking in two elderly trans-femoral amputees when using knee joints which emphasized stance-phase control and Intelligent Prosthesis, and to provide some bibliographic observations on factors behind their success in improving walking ability despite their age. It was a within-subject comparison. The subjects comprised two patients, aged 75 and 81 years, with trans-femoral amputations. On admission subjects were subjected to one-leg cycling test driven by their non-amputated leg in order to evaluate their physical fitness. The PCI and speed during free level walking was measured using their original knee joints. The knee joint was then changed to IP and the subjects received prosthetic walking training programs using it. The PCI and speed measurements were taken during free level walking on completion of the training program. Both subjects showed a decreased PCI and an increased free walking speed when using the IP compared with the original knee joints. It was concluded that elderly trans-femoral amputees who are judged to be in good physical condition appear to merit the application of knee joints with superior swing phase control functions such as IP, regardless of their age.
Keywords
Introduction
In recent years there has been a trend in Japan towards an increasing number of amputations due to vascular insufficiency (Nagashima et al. 1991), as has been seen in Western countries. Elderly lower-limb amputees have complications due to generalized arteriosclerosis, and their physical fitness is commonly diminished. Furthermore, the energy consumption associated with prosthetic walking by a trans-femoral amputees is significant (Gonzalez et al. 1974; Waters et al. 1976; Traugh et al. 1975; Cammisa et al. 1990). Therefore, prosthetic walking for elderly trans-femoral amputees is, in itself, an activity that imposes a heavy physical burden. Reducing the energy requirement of prosthetic walking would be of great benefit to them. Recently, there have been some reports (Taylor et al. 1996; Buckley et al. 1997; Chin et al. 2003) of reduction in energy consumption through the use of the microprocessor-controlled pneumatic swing-phase control knee, the Intelligent Prosthesis.
The absence of any consistent definition of what constitutes successful prosthetic rehabilitation of elderly lower-limb amputees is a problem (Johnson et al. 1995; Beekman and Axtell 1987), but reports from various sources (Steinberg et al. 1985; Moore et al. 1989; Pohjolainen et al. 1990; Campbell and Ridler 1996) state high rehabilitation success rates of around 70% for elderly trans-tibial amputees, falling to approximately 50% for elderly trans-femoral amputees. Thus it is extremely difficult for elderly trans-femoral amputees to succeed in rehabilitation. Therefore, considerable difficulties are faced in devising prosthetic prescriptions for them in clinical situations. In general, knee joint selections for elderly amputees emphasize stance-phase control rather than joints with advanced swing-phase control.
This research has observed an improvement in walking ability in two subjects, who underwent trans-femoral amputation at advanced ages when the knee joints they had been using in daily life, which emphasized stance-phase control, were replaced with the microprocessor-controlled pneumatic swing-phase control knee (Intelligent Prosthesis) and renewed training. The aim of this study was to compare the Physiological Cost Index (PCI) and walking speeds during walking in two subjects, aged 75 and 81 years, with trans-femoral amputation when using a prosthesis fitted with a knee which emphasized stance-phase control and a prosthesis fitted with an Intelligent knee, and to provide some bibliographic observations on factors behind their success in improving walking ability despite their age.
Subjects
The two subjects were highly motivated to walk. They entered this study and agreed to receive prosthetic walking training in order to change from their original knee joints to Intelligent Prosthetic knee joints.
Subject 1 was male, aged 75 years, 159 cm tall, 49 kg in weight and had a stump length of 29.5 cm. He had no co-morbidity. He underwent amputation when aged 74 years as a result of trauma. He has been fitted with a prosthesis consisting of a quadrilateral suction socket, an Otto Bock 3R15 single-axis knee joint with stance-phase control and constant friction, and a single axis foot. He was able to walk with double crutches independently, and wore his prosthesis almost all day for his ordinary activities.
Subject 2 was male, aged 81 years, 164 cm tall, 50 kg in weight and had a stump length of 25 cm. His only co-morbidity was cholecystopathy. He underwent amputation when aged 80 years as a result of trauma. He has been fitted with a prosthesis consisting of a partial suction socket with suspension belt, a 3R40 (Otto Bock) semi-automatic manual release knee joint and a single axis foot. He was able to walk with one T-cane independently and wore his prosthesis almost all day for his ordinary activities.
Both amputees had superior ability to balance on the non-amputated leg, and had none of the impediments to walking indicated by Steinberg et al. (1985); dementia, advanced neurological disorders, congestive cardiac failure, advanced obstructive pulmonary disease, advanced hip flexion contracture and ulceration or infection of the remaining lower limb.
On admission, they each began by undergoing a one-leg cycling test to assess their fitness. At a later date, their Psychological Cost Index (PCI) when walking with their original prosthesis was measured. After that, the knee joints were replaced by a microprocessor-controlled prosthesis, a 4-bar linkage Intelligent Prosthesis (IP) knee joint (Nabtesco Ltd, Kobe, Japan). The fitting and alignment for the new prosthesis in both subjects were carried out by the same prosthetist. The programming of the IP was done by a physiotherapist according to the manufacturer's instructions. Following admission to this centre, both subjects received prosthetic walking training using the IP. On completion of this training program, their PCI was measured as before. Before this research began, both subjects received an internal medical checkup, blood tests, electrocardiogram and lung function test. No impediments to prosthetic walking training were found in either subject. They were aware of the purpose of the study and the possible risks, and informed consent was obtained from each.
Methods
PCI measurement
The subjects were each allowed to use any walking aids they found necessary and walked at their free walking speed over level ground during which their walking speed was measured. They were asked to walk at their free walking speed for five minutes over level ground. Their pulse rates in beats per minute (bpm) were measured at rest before walking and on completion of walking. The PCI was calculated as PCI = (pulse rate at end of walk – pulse rate at rest) (bpm)/walking speed (m/min).
Evaluation of physical fitness
The subjects were subjected to a one-leg cycling test driven by their non-amputated leg. This method has already been reported (Chin et al. 1997). A cycle ergometer (Lode Angio WLP-300ST, Holland), which can be cycled from a supine position was used. The tests were conducted with the subjects seated with their upper bodies reclining at an angle of approximately 45°. This incremental exercise test was begun with three minutes of unloaded pedaling and then with the increments of 10 W per min until the subject's self-assessed maximum load. The test subjects were directed to turn the pedals 60 times per min. During exercise, the respiratory gas was monitored with a respiromonitor (Minato RM-300 system, Osaka, Japan); the oxygen uptake was then measured. At the same time the ECG and heart rate (HR) were monitored during exercise by Stress Test system (ML-5000, Fukuda Denshi, Tokyo, Japan), and cuff blood pressure was determined every minute with autoelectrocardiometer (Colin STPB-780, Japan).
The maximum oxygen uptake during exercise as a proportion of predicted maximum oxygen uptake (%VO2max) was used as an indicator of physical fitness.
Prosthetic walking training program
Since the program using the IP knee was intended to raise walking speed, it can only be applied to amputees who have completed the basic prosthetic training program. This consists of bearing an adequate amount of body weight on the prosthetic side and being able to walk with a knee joint which emphasizes swing-phase control. If the amputees were not able to overcome these tasks, they are asked to complete the basic training program before receiving a training program using the IP. Therefore, the training programs varied with the subject. The standard program using the IP in The Hyogo Rehabilitation Center is as follows. The step length and cadence must be increased in a suitable balance to improve walking speed. Targets are set at this centre for stride length and cadence corresponding with each walking speed. Specifically, a step length of approximately 60 cm and cadence of 80∼100 are set for a walking speed of 50∼70 m/min, and 70 cm and 100∼120 for walking speed of 70∼90 m/min. The walk-path was marked in order to assist in making the step length more uniform, so that each subject could check for himself. Each subject used a portable metronome to walk to a fixed rhythm, in order to achieve uniform cadence. In that way, walking speed was gradually increased, with training continuing until the amputee could walk for five minutes at each speed. The IP was reset when the swing phase became unable to keep pace with the walking speed in the course of training. The training program continued for 12 weeks.
Results
Table I shows the subjects' PCI results, walking parameters and use of walking aids, indicating whether there was a change due to the change from the previous knee joints to the IP. For both subjects, step length had been made more even by the end of the training program with the IP, and there were improvements in cadence for Subject 1 and stride length for both subjects. Free walking speeds were increased and PCI levels were decreased.
Comparison of walking parameters and PCI.
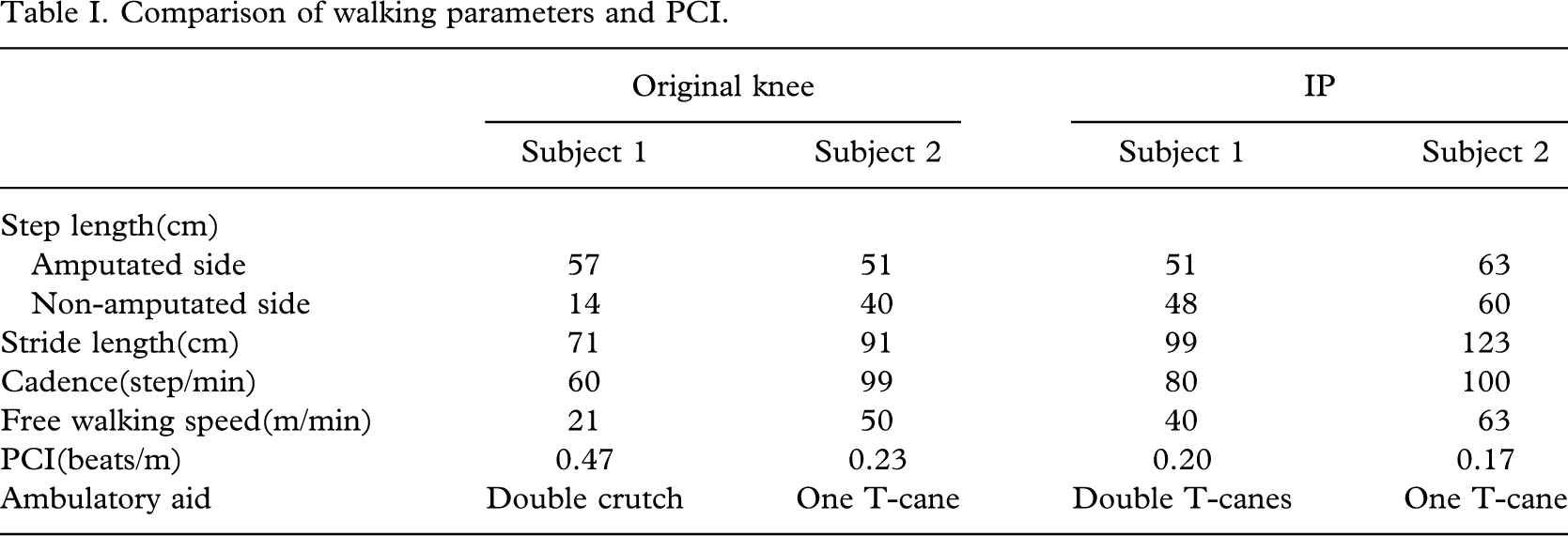
For walking aids, Subject 1 changed from two crutches to two T canes, and Subject 2 stayed with one T cane. The %VO2max values on admission to this centre were 87.8 for Subject 1 and 75.0 for Subject 2.
Discussion
PCI is one of the cardiopulmonary system measurement factors proposed by MacGregor (1979, 1981), having heart rate and walking speed as its parameters. Chin et al. (1999) have reported a significant correlation between PCI and energy consumption when walking with an IP. The IP has a microprocessor-controlled pneumatic swing-phase control knee which dynamically regulates the opening of the needle valve of a pneumatic damping cylinder in a way which allows adjustment to the desired walking speed. In these cases, use of an IP was observed to raise free walking speed and reduce PCI, compared to use of the original knee joints. This indicates that training in walking with an IP was effective in improving the swing phase dynamics.
The improvements in cadence, PCI and free walking speed were significant in Subject 1. Subject 1 had already completed the basic prosthetic training program before entering this study. Subject 2, on the other hand, could not complete this program. This may be a possible reason for the difference between the two subjects.
However, elderly trans-femoral amputees commonly struggle with rehabilitation. In contrast to this fact, both subjects in this study have acquired improved walking ability. If the factors involved are considered many elderly amputees are already in a deconditioned state, and furthermore, if they are trans-femoral amputees, prosthetic walking requires high energy consumption (Gonzalez et al. 1974; Waters et al. 1976; Traugh et al. 1975; Cammisa et al. 1990). Prosthetic walking in itself imposes a heavy burden on elderly trans-femoral amputees. Therefore, if they are to succeed in prosthetic walking, they must have sufficient fitness to withstand these physical burdens (Crouse et al. 1990; Kurdibaylo 1994). However, very few reports have examined what level of fitness is required (Chin et al. 2002). Chin et al. (2002) has reported that at least 50%VO2max is required as a level of fitness for successful prosthetic walking in elderly trans-femoral amputees. Both of these subjects had considerable levels of fitness, equivalent to 70∼80%VO2max, so they had maintained excellent fitness levels. The number of co-morbidities is another important factor impacting on successful prosthetic walking, with the functional prognosis worsening as the number increases (Johnson et al. 1995; Steinberg et al. 1985; Chin et al. 2002; Leung et al. 1996). Here, both amputations were due to trauma and Subject 1 had no co-morbidities, while Subject 2 had only one minor co-morbidity.
Furthermore, both subjects had superior balance when standing on the non-amputated leg. That appears to have been another factor contributing to their success. Several authors (Chin et al. 2002; Schoppen et al. 2003) have reported the importance of balance on the non-amputated leg for elderly trans-femoral amputees. In general, the functional progress is held to worsen with age (Dove et al. 1982; Munin et al. 2001). The subjects were aged 75 and 81 years, which was certainly not a condition in their favour, but their prosthetic walking ability was observed to improve. Harris et al. (1991) have stated that elderly amputees should not be excluded from prosthetic training on grounds of age alone. Furthermore, neither of the two subjects had any of the impediments to walking proposed by Steinberg et al. (1985), and their high levels of motivation to walk appear to have been an important factor.
In the past it has been common practice to select knee joints for elderly trans-femoral amputees that emphasize stance phase control (including fixed knees). Of course, it is difficult to draw any definitive conclusion from the limited experience of these two cases. Nevertheless, changing these two cases to highly functional knee joints and re-training them enabled efficient walking and reduced their physical burden. Elderly trans-femoral amputees who are judged to be in good physical condition, on the basis of careful assessment from various perspectives, appear to merit the application of knee joints with superior swing phase control functions, regardless of their age.
Conclusion
It is hard to draw a firm conclusion from only two case experiences. However, this study suggests the possibility that elderly trans-femoral amputees who are judged to be in good physical condition appear to merit the application of knee joints with superior swing phase control functions such as IP, regardless of their age.