
Abstract
Background:
Traditionally, the anatomical knee joint is locked in extension when walking with a conventional knee–ankle–foot orthosis. A powered knee–ankle–foot orthosis was developed to provide restriction of knee flexion during stance phase and active flexion and extension of the knee during swing phase of gait.
Objective:
The purpose of this study was to determine differences of the powered knee–ankle–foot orthosis compared to a locked knee–ankle–foot orthosis in kinematic data and temporospatial parameters during ambulation.
Study design:
Quasi—experimental design.
Methods:
Subjects with poliomyelitis (n = 7) volunteered for this study and undertook gait analysis with both the powered and the conventional knee–ankle–foot orthoses. Three trials per orthosis were collected while each subject walked along a 6-m walkway using a calibrated six-camera three-dimensional video-based motion analysis system.
Results:
Walking with the powered knee–ankle–foot orthosis resulted in a significant reduction in both walking speed and step length (both 18%), but a significant increase in stance phase percentage compared to walking with the conventional knee–ankle–foot orthosis. Cadence was not significantly different between the two test conditions (p = 0.751). There was significantly higher knee flexion during swing phase and increased hip hiking when using the powered orthosis.
Conclusion:
The new powered orthosis permitted improved knee joint kinematic for knee–ankle–foot orthosis users while providing knee support in stance and active knee motion in swing in the gait cycle. Therefore, the new powered orthosis provided more natural knee flexion during swing for orthosis users compared to the locked knee–ankle–foot orthosis.
Clinical relevance
This orthosis has the potential to improve knee joint kinematics and gait pattern in poliomyelitis subjects during walking activities.
Background
Knee–ankle–foot orthoses (KAFOs) may be prescribed for individuals with conditions such as poliomyelitis, post-polio syndrome (PPS), stroke, spinal cord injury (SCI), and degenerative muscular disease. 1 Traditional KAFOs incorporate locked orthotic knee joints, which provide stability during stance phase and prevent knee motion during the swing phase. Walking with this type of KAFO produces a stiff leg with resulting difficulty in ambulation. KAFOs with free knee joint permit knee motion during swing phase and allow limited stability during stance, but can increase the risk of buckling and falling. 2 Major shortcomings of locked knee joint KAFOs include the prevalence of increased upper-body lateral sway, ankle plantar flexion of the contralateral foot (vaulting), hip elevation during swing phase (hip hiking), or leg circumduction. 3 Walking with these conditions may also initiate soft tissue and joint dysfunction in the hip and lower back leading to pain and motion loss and increased muscular effort with possible higher energy expenditure. 4
Recent developments in KAFO design have included the design of stance control orthotic knee joints which resist knee flexion during stance phase but allow free knee flexion during swing phase. Studies involving stance control knee–ankle–foot orthoses (SCKAFOs) have reported positive effects on specific gait parameters in subjects requiring lower limb support.1–4 McMillan et al. 1 evaluated the effect of the Horton’s SCKAFO on gait parameters exhibited by three subjects with poliomyelitis and compared the results when wearing a locked knee KAFO. They reported increases in walking speed, cadence, stride, and step length, with fewer compensatory motions at the hip, pelvis, and trunk, and a more symmetrical gait pattern when subjects wore the SCKAFO, as full knee extension is needed at 30% of the gait cycle. Similarly, Hebert and Liggins 5 reported that, for a single subject with PPS, when walking with a SCKAFO, there was near-normal knee flexion during swing, reduced pelvic retraction and rotational excursion, and improved hip power generation compared to a locked KAFO.
Tokuhara et al. 6 evaluated the effect on the gait of 10 able-bodied subjects when using a computer-controlled SCKAFO and demonstrated that the kinematics of walking were compatible to that of normal adult walking. Kaufman et al. 4 evaluated the alteration in energy expenditure demonstrated during walking in a subject with poliomyelitis when using a SCKAFO with an electronically controlled orthotic knee joint which had the facility to either have the joint locked in extension or when providing stance phase control. Oxygen consumption rate and energy costs were significantly reduced with the stance control test condition. Irby et al. 7 reported an increase in walking speed, cadence, and swing phase knee flexion when an able-bodied subject used the dynamic knee brace system (DKBS) SCKAFO compared to a locked knee KAFO. In a subsequent study, Irby et al. 8 compared the effect on gait of the DKBS when used by both experienced and novice KAFO users. Both novice and experienced users demonstrated increased peak knee flexion in swing and reduced compensatory motions (e.g. vaulting and hip hiking) when walking with the SCKAFO compared to a traditional locked knee KAFO. Interestingly, novice users had higher walking speeds and step lengths when using the SCKAFO compared to experienced users. Bernhardt et al. subsequently evaluated the efficacy of the DKBS on 20 subjects via a questionnaire. The respondents reported that stability in standing and walking was increased when wearing the DKBS compared to their conventional orthosis. However, donning and doffing of the DKBS were perceived to be difficult, and the large size and weight of the knee joint were thought to be disadvantages. 9
The advantages of SCKAFOs compared to conventional orthoses have therefore been shown to include the facility to provide a greater sagittal plane range of motion (ROM) of the knee and decreased compensatory motions (e.g. vaulting and hip hiking).1,4,10–12 However, disadvantages still exist in some SCKAFO designs. These include the need for full knee extension to be achieved during gait (pre-swing) in some designs and, because some provide activation by positioning the ankle or knee at specified angles, adequate ROM at these joints is required to provide locking of the orthotic knee joint during stance phase. In addition, some designs only offer a limited number of knee locking positions or need the knee to be in an extended knee position for stability reasons during gait.
Powered lower limb orthoses have been shown to be useful devices for walking in disabled subjects (e.g. SCI, stroke, or poliomyelitis). 13 These devices restore a portion of the torque that is applied normally to the lower limb joints during walking. 14 In an attempt to address the documented limitations of current SCKAFO and KAFOs designs, a new knee joint mechanism for use in KAFOs was developed to restrict knee flexion during stance phase and actively flex the knee during swing and also to provide full knee extension prior to heel strike. The feasibility of this mechanism design had previously been evaluated on healthy subjects and a single subject with poliomyelitis.15,16 This study evaluated this technology to enable it to be potentially incorporated in a new knee joint mechanism for use in KAFOs. Therefore, this study was designed to evaluate the effect of a new powered knee joint mechanism on KAFO user’s gait to determine the extent to which the new knee joint mechanism would correct KAFO-induced gait abnormalities.
Methods
Subjects
KAFO users were identified by the prosthetics and orthotics service at a rehabilitation center. In order to participate in the study, subjects were required to have previously routinely used KAFOs either unilaterally or bilaterally with lockable orthotic knee joints, be able to walk a minimum of 50 m, and to have sufficient hip flexor strength to advance the limb during swing phase. Muscle strengths were assessed manually based on the Oxford scale. 17 Muscle strengths in the hip joint were required to be at a minimum level equivalent to level 3 on the Oxford scale.
Exclusion criteria included the existence of impaired cognition, poor balance, not able to walk 50 m, or the existence of soft tissue contractures greater than 15° at the hip, 10° at the knee, or 5°at the ankle. Subjects with medical problems such as orthostatic hypotension, cardiac arrhythmias, vestibular dysfunction, and peripheral neuropathy, which could contribute to falling, or having near falls, or loss of balance, were not considered for this study. In addition, subjects who had experienced a fall or near-fall due to stance-related issues and subjects who may also be having difficulties in swing phase due to poor balance were excluded. 18 The study was approved by the university’s Human Ethical Committee and all subjects signed informed consent prior to participation in the study.
General information of subjects (e.g. age (year), weight (kg) and history of illness), use of orthoses or walking aids, and current ambulatory function was recorded. Any newly developed symptoms that reduced his or her physical function, such as fatigue, weakness, and/or pain related to PPS, was recorded. 19 All the subjects had been affected by poliomyelitis in their childhood and four of them were showing PPS symptoms. None of the participants needed or used bilateral KAFOs. All participants used a KAFO unilaterally in this study. Knee muscle strength was assessed only in the affected side.
Interventions
Each subject was fitted with two custom mold type KAFOs by a certified orthotist. The KAFOs were manufactured with molded thigh cuffs and solid ankle–foot orthoses (AFOs). The new design of a powered KAFO utilized a medial and lateral upright that was manufactured in aluminum incorporating a single-axis free knee joint (Figure 1). A 40-W electric actuator (“Maxon Motor EC max30”; Maxon, Switzerland) with a planetary gearbox providing a reduction ratio of 111 was used to provide knee joint flexion and extension power for this orthosis. It was designed to restrict knee flexion during stance phase, and when the foot progressed into the swing phase after push off, the actuator flexed the knee joint actively.

The orthoses used in this study.
Torque control over the knee joint was applied corresponding to different phases of the gait cycle. This prototype resisted knee flexion at any angle during stance phase. Actuation began at heel strike due to load transferring through the joint. Two triggers were needed to actuate the joint, and a predefined threshold of moment was assigned to trigger the actuator. At approximately 55%–60% of the gait cycle during late stance, the joint was actuated to provide flexion of the knee joint due to lower limb unloading. At the point of full flexion, a predefined delay enabled the joint to stop and prepare for stance phase by moving back to full extension gradually. The delays could be altered during the training process for fine tuning for each individual to achieve 45° of flexion and 0° of extension during swing phase and to obviate the need for sudden increases in walking speed. A rechargeable 24 V battery (Lipo Battery, Thunder Power RC G6 Pro Lite 25C 5400 mA h 6-Cell/6S) with 2 h of available continual working was used to provide power for the actuator. The battery and electronic unit of the new KAFO were placed on a waist belt by the subjects and weighed 0.7 kg. The additional components of the new powered KAFO added 0.8 kg of extra weight compared to the conventional orthosis. Figure 1 shows images of the orthosis used in this study.
After subjects were measured and fitted with the powered KAFO unilaterally, a supervised gait training programme was commenced in a rehabilitation center under controlled and supervised conditions in order for the patient to achieve confidence and experience in balance, standing, and walking with the orthosis. They were trained to ambulate on level ground for 4 weeks, 3 days in a week, for 2 h each day, so that they could walk independently prior to commencement of experimental testing. Three trials per orthosis were collected while each subject walked along a 6-m walkway at their comfortable self-selected speed. Subjects were given a 1 h rest between testing of each orthosis. All participants used the KAFO with drop lock knee joint and then the powered SCKAFO. The patients also get 30 min accommodation time to the new powered KAFO prior data gathering.
Gait analysis
Following orthotic gait training, subjects participated in a two-part data collection session which consisted of gait evaluation initially with the locked knee KAFO and then the powered KAFO. The same thermoplastic sections were utilized for each KAFO for each subject. A calibrated six-camera three-dimensional (3D) video-based motion analysis system (Oxford Metrics, Inc, Oxford, UK) with a capture frequency of 100 Hz and two force platforms (Kistler 9286BA, Switzerland) were used to gather data while walking with the orthoses in the motion analysis laboratory. Reflective markers were placed on the orthosis and the skin of the subjects in the following positions: over the jugular notch, the spinous process of the seventh cervical vertebrae, bilaterally over the acromio-clavicular joints, the anterior superior iliac spine (ASIS), the greater trochanter, the lateral condyle of the femur, the head and lateral malleolus of the fibula, calcaneus, and on the dorsum of the foot over the second metatarsal head.
Retro reflective markers were applied directly to the skin on the non-affected side in the positions described and left in place during the whole testing session. On the affected side, markers were again placed on the dorsum of the foot over the second metatarsal head, and on the calcaneus, but this time on the lateral aspect of the mechanical ankle joint axis of rotation, on the lateral bar over the position of the fibular head, and on the mechanical orthotic knee joint over its axis of rotation.
Data were processed at 100 Hz with VICON Body Builder (Oxford Metrics) using the standard lower limb model included in the software. The data were then analyzed using MATLAB (MathWorks, Natick, MA, USA). The mean walking speed, step length, cadence, maximum knee flexion angle during swing, and maximum pelvic tilt on the affected side during swing were calculated for each subject. Walking speed was measured from the marker placed on the calcaneus. Hip hiking was analyzed from the trajectory of the markers put on each ASIS.
Statistical analysis
Normality of data in speed of walking (p = 0.999), step length (p = 0.999), cadence (p = 0.447), stance phase percent (p = 0.905), maximum knee flexion in swing (p = 0.995), and pelvic obliquity (p = 0.884) was confirmed by using the Kolmogorov–Smirnov technique. A paired t-test was used to compare the two orthoses. SPSS statistical software (JMP IN software; SAS Institute, Inc., Cary, NC, USA) was used for analysis of the data. The level of significance was set at 0.05.
Results
Seven poliomyelitis subjects (all males) were enrolled in the study. Table 1 shows the demographic characteristics of participants in this study.
Subject information.
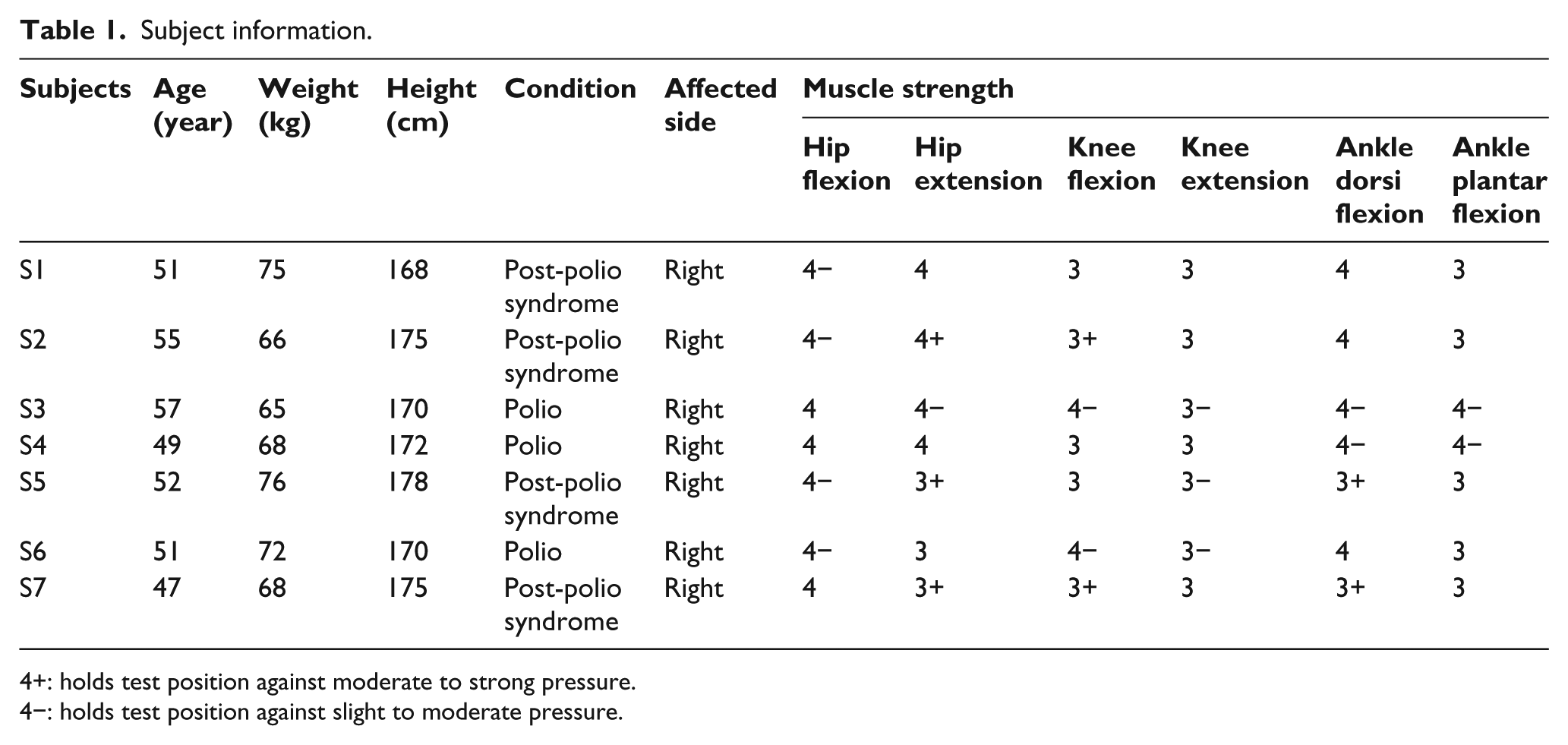
4+: holds test position against moderate to strong pressure.
4−: holds test position against slight to moderate pressure.
Temporospatial parameters
Table 2 demonstrates the temporospatial and kinematic data for the participants when ambulating using the locked knee KAFO and the powered KAFO.
Mean and standard deviation (SD) for temporospatial parameters and peak knee angle in swing (°) for subjects wearing the locked knee KAFO and the powered KAFO.
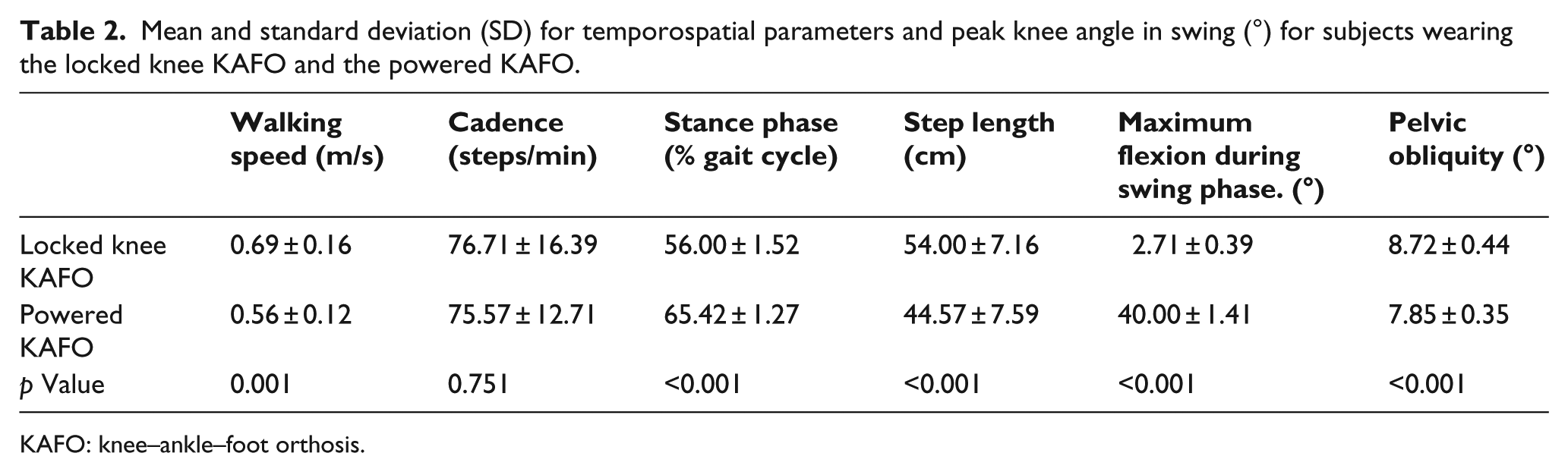
KAFO: knee–ankle–foot orthosis.
Walking speed was significantly slower (18%) (p = 0.001), with the powered KAFO compared to walking with the locked knee KAFO. Walking with the powered KAFO also resulted in a significantly shorter step length (18%) compared to walking with the locked knee KAFO (p < 0.001). There was a significant 16% increase in stance phase percentage of the gait cycle (p < 0.001) when walking with the powered KAFO, but no significant difference in cadence between the two orthoses (p = 0.751).
Kinematics
There was significantly higher knee flexion during swing phase when walking with the powered KAFO compared to the locked knee KAFO (p < 0.001) (Figure 2) (Table 2). The maximum pelvic tilt on the affected side during swing was significantly increased when subjects walked in the powered KAFO compared to the locked knee joint KAFO (p < 0.001) (Figure 3).
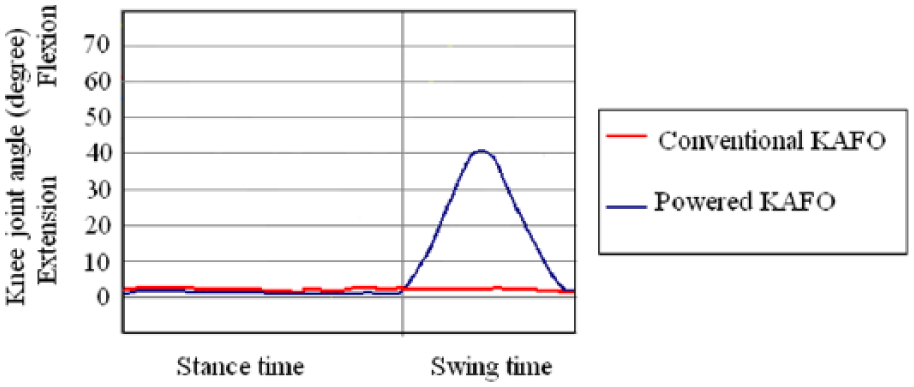
Mean sagittal plane knee kinematic for each orthosis.
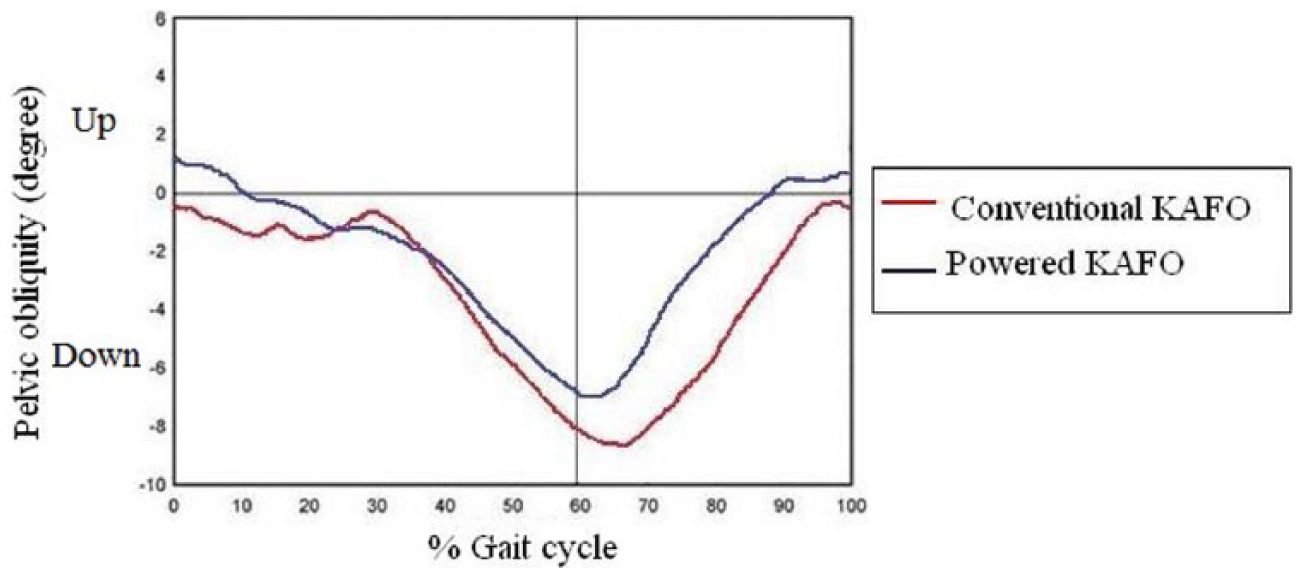
Mean pelvic obliquity for each orthosis.
Discussion
This study evaluated the effect on walking of using a KAFO which incorporated a powered knee joint compared to a locked knee KAFO in subjects with poliomyelitis and PPS. The main functional purpose of the powered KAFO was to provide active knee flexion in swing phase and provide resistance to knee flexion during stance phase. This study demonstrated that the newly powered KAFO could achieve this function.
The KAFO with drop locked knee joints affected the walking patterns of the subjects with poliomyelitis by creating a functionally longer lower limb by restricting flexion of the knee joint during swing phase. However, when walking with the powered KAFO compared to KAFO with drop locked knee joints in this study, hip hiking (i.e. pelvic obliquity) was significantly increased, even though it was expected that provision of active knee flexion when using the powered KAFO would actually reduce hip hiking during ambulation. Arazpour et al.,20,21 when using a powered hip orthosis and an isocentric reciprocating gait orthosis (IRGO) incorporating an active knee joint in spinal cord–injured subjects, reported that lateral and vertical compensatory motions were reduced compared to when using a mechanical IRGO. Using a mechanical SCKAFO has also demonstrated a reduction in pelvic obliquity when compared to a KAFO with drop locked knee joints.1,5,22,23
The maximum knee flexion was 2.71° ± 0.39° when using the KAFO with locked knee joints and was significantly increased when using the powered KAFO (40° ± 1.41°). Normal maximum knee flexion during swing phase has been reported as being 67°. 16 The mean range of knee flexion with a SCKAFO has been demonstrated to be 44°.4,5,8 Yakimovich et al. 23 in an evaluation of a new SCKAFO reported a 32° average range of knee motion during swing. Arazpour et al. 15 in evaluating the powered KAFO in a single poliomyelitis subject demonstrated a 42.5° range of knee motion. Active flexion and extension of the knee joint during the whole of the gait cycle, and particularly during stance phase, are not provided by all current SCKAFO designs. This point is a potential advantage of a powered KAFO over a SCKAFO. This device also has the capability of resisting knee flexion during loading response with maximum flexion during stance being dictated by the software and potentially matching that of the sound limb.
Previous studies have demonstrated that increased knee motion in swing phase can lead to reduced energy consumption during walking with a SCKAFO.1,4 Based on the increased knee flexion during swing in using the powered KAFO, reduction in energy consumption when compared to devices with locked knees may be expected.
Improved knee joint kinematics and increased stability during walking with a KAFO by poliomyelitis subjects is important, because these factors can potentially decrease energy expenditure in such subjects. Due to lower limb muscle paralysis, poliomyelitis subjects have difficulty in achieving foot clearance, and walking with a KAFO with locked knee joints may also induce increased quadriceps weakness due to the knee being locked during the whole gait cycle. 24 Use of a powered KAFO may help this problem by providing active knee flexion during swing phase.
The mean walking speed was significantly reduced when walking with the powered KAFO even though a specific gait training programme was completed by each participant. More extensive experience in using a powered KAFO is therefore required to enable subjects to become more proficient in ambulating with it donned to produce faster walking speeds and is in agreement with the findings by Irby et al. 8 who reported improvement in walking speed by using walking training with a SCKAFO. Hebert and Liggins 5 reported no change in temporospatial parameters between the locked and auto modes for a single post-polio subject. Zissimopoulos et al., 22 using the Horton SCKAFO in the locked, unlocked, and auto position in nine healthy subjects, demonstrated no significant difference in freely selected walking speed between the auto- and locked modes. However, McMillan et al. 1 reported that speed and cadence were increased in using the automatic mode in a SCKAFO compared to wearing the locked mode KAFO in their three subjects. In other studies, increased walking speed, cadence, and flexion of knee joint when using SCKAFO have been demonstrated.7,8 However, those studies had longer times of accommodation with the orthosis compared to this study.
Subjects with weakness of the lower limb muscles who need a KAFO to walk may not be readily able to change their step length compared to healthy subjects. 22 Therefore, using a powered KAFO may be more reliable device to achieve this desired outcome. Nevertheless, step length was decreased by 18% in this study when using the powered KAFO compared to a KAFO with locked knee joints. Subjects using the conventional KAFO had a long lever arm in providing step length, while in wearing powered KAFO the lever arm was shorter. Experienced KAFO users who participated in this study only had 2 weeks of accommodation time in learning to walk with the powered KAFO. Since speed of walking is related to step length, decreased step length provided a reduction in speed of walking in this study.
The powered KAFO resisted knee flexion during stance phase. Due to the fact that knee flexion in stance phase plays a shock absorbing role in walking, using a soft ankle cushion heel (SACH) in combination with the powered KAFO is proposed. Future studies must also include the development of a power unit which can offer knee flexion and extension during loading response as well as swing phase control.
A lightweight KAFO has been shown to improve the gait efficiency of polio subjects. Heim et al. 25 demonstrated that carbon KAFOs were 30% lighter in weight compared to metal KAFO and 70% of the post-polio subjects were satisfied when wearing this type of orthosis. Steinfeldt et al. 26 announced that the maximum walking distance of polio subjects significantly increased when using a carbon KAFO which had a 40% reduction in weight. The weight of the new orthosis in this study was more than the conventional KAFO. This factor may have influenced walking speed and step length.
The limited acclimatization time, evaluation of the powered KAFO by experienced locked knee KAFO users instead of SCKAFO users, subjective control of the powered orthosis, lack of evaluation of the effect of the powered KAFO on energy consumption, and the low sample size are all limitations of this study. Further studies which resolve these limitations on subjects with poliomyelitis would be beneficial. Ankle angles (vaulting) or hip rotation (circumduction) was not analyzed in this study. Investigation of these parameters in this field will be beneficial. Since the powered KAFO in this study also weighed significantly more than conventional orthoses, one may expect to find that users also report this as a disadvantage. Optimizing powered KAFOs in terms of weight is proposed as a future plan of study in this field. Patient satisfaction is important to assess, since dissatisfaction may result in non-use, even if the orthosis has biomechanical advantages, and an investigation of this point will be beneficial in a future study.
Conclusion
This study evaluated the effects of a KAFO which incorporated a powered knee joint on gait in subjects with poliomyelitis. The involvement of disabled subjects with lower limb muscle weakness in this study permitted an analysis of the kinematic and temporospatial effects of a powered KAFO on walking in a user population. The feasibility of this new powered KAFO in a further group of subjects (n = 7) suffering from poliomyelitis was demonstrated in this study.
The new powered KAFO provided controlled active knee flexion and extension during walking for a volunteer poliomyelitis subject compared to existing KAFOs and also demonstrated a slower speed of walking and shorter step length, increase in stance phase percentage, and increased peak knee flexion during swing as compared to the conventional KAFO in this study. Longer training times and also an amended gait training regime may be necessary for subjects to fully adapt to using the powered KAFO. Further studies are needed to measure the effects of powered KAFO on energy consumption in subjects with poliomyelitis.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the Iranian National Science Foundation (INSF) for financial support (grant No. 93018293) for this research.