
Abstract
Background:
Knee–ankle–foot orthoses are utilized for walking by patients with lower limb weakness. However, they may be rejected by patients due to the lack of knee flexion available when using them for walking activities.
Aim:
The aim of this study was to perform a pilot study investigating the effect of a new powered knee–ankle–foot orthosis on walking in healthy persons before testing with patients with lower limb weakness.
Methods:
Walking evaluation was performed on five healthy subjects (mean age: 26 ± 5.6 years). Walking trials were randomly performed in three test conditions: normal walking without an orthosis, walking with a conventional knee–ankle–foot orthosis unilaterally, and also with a new powered knee–ankle–foot orthosis applied to the same leg.
Results:
The means of walking speed, cadence, and knee flexion during swing and step length were all decreased. Compensatory motions were increased by both orthoses compared to normal walking. More knee flexion was observed in both swing and stance phases when walking with the powered knee–ankle–foot orthosis compared to the conventional knee–ankle–foot orthosis.
Conclusion:
The results demonstrated the potential of a powered orthosis in providing improvements in gait parameters compared to a conventional device in healthy subjects but are yet untested in subjects with lower limb weakness.
Clinical relevance
The results of this study demonstrated that a powered knee–ankle–foot orthosis could lock the knee during stance and provide active knee flexion during swing to potentially reduce the tripping during ambulation.
Introduction
Patients with poliomyelitis, stroke, or incomplete spinal cord injury usually use knee–ankle–foot orthoses (KAFOs) to ambulate. This type of orthosis has lockable knee joints that prevent knee joint flexion during walking, 1 which can cause abnormal gait patterns such as hip hiking, leg circumduction, and vaulting when patients use KAFOs. 2
Dysfunction of lower limb joints and their associated soft tissues in such patients, along with experience of low back pain, can result in a reduction in gait efficacy, increased center of mass (COM) displacement in the vertical direction, increased energy consumption, and early fatigue, which are all complications when walking, and can result in abnormal and un-cosmetic gait patterns in these patients.1,3,4
Recently, so-called stance control KAFOs (SCKAFOs) have been developed to provide free knee flexion during swing and prevent knee flexion during stance phase of gait by incorporating innovative orthotic knee joints. The Otto Bock Free Walk/Becker UTX, Horton’s Stance Control Orthosis, Fillauer Swing Phase Lock, Becker Orthopedic 9001 E-Knee, Ottawalk Belt-Clamping Knee Joint, Dynamic Knee Brace System, and the Dual Stiffness Knee Joint are all examples of such orthoses. 5
Previous studies have evaluated the effect of a variety of SCKAFOs. The positive effects of this type of orthosis demonstrated in literature have included increased walking speeds and stride lengths; reduction of compensatory motions such as plantar flexion of the contralateral ankle in stance (vaulting), dynamic pelvic obliquity (hip hike), leg circumduction, and upper body lateral sway during walking; and a more symmetric walking pattern compared to other orthoses.6 –9 This has been evidenced when utilized by healthy subjects, those with poliomyelitis and also spinal trauma, 3 plus those with neuropathies, incomplete spinal cord injuries, spina bifida, multiple sclerosis, and muscular dystrophy. 5 Some SCKAFOs need knee extension to obtain accurate locking of the knee joint, and, in addition, many operate by utilizing ankle motion (e.g. some degree of passive ankle dorsiflexion range) or knee joint movements. Lack of controlled knee flexion during stance phase, attainment of knee extension, and easy switching between stance and swing modes have been quoted as being limitations of mechanical SCKAFO designs. 5 The powered lowered limb orthosis described in this study is able to provide powered motion to the knee joint, via torque provided by the joint actuators to actively move the orthotic knee joint through all phases of gait. 10
Current advances in technology may therefore improve the limited knee control options available from current SCKAFOs. 5 Using electronic actuators in the joints of lower limb orthoses could provide better control of lower limb motion during walking.11 –13 The control of knee flexion and extension motion during swing and stance phases also remains a limitation of currently developed SCKAFOs. 5 Use of powered SCKAFOs could reduce orthosis rejection and increase cosmesis and confidence during ambulation in users with lower limb muscle weakness. 5 Current issues that have been shown to promote rejection of SCKAFOs include the incidence of pain and a reduction in knee joint movement due to walking with a fixed knee position during stance phase.1,3 In addition, increased vertical displacement of the COM, 14 the high muscular effort needed to walk, 4 early fatigue during walking, 1 and high energy consumption during walking could all contribute to high rejection rates when using KAFOs. 4
A new powered SCKAFO was therefore developed to reduce the functional limitations of current SCKAFOs. The rationale for this study was to assess a new orthosis that provided powered knee flexion and extension during swing phase; accepting the fact that the ankle–foot orthosis (AFO) section of the orthosis would also provide adequate ankle stability and reduce ankle plantar flexion during swing to a minimum to prevent tripping and falls. The orthotic knee joint was developed to provide resistance to knee flexion during stance phase and active knee flexion followed by extension assistance during swing phase to potentially provide a smoother and more natural gait. The software and hardware used for the knee joint in this study were previously tested in a powered gait orthosis and performed as predicted by simulations. 15
While this new powered SCKAFO has potential advantages over currently available SCKAFOs, a pilot study utilizing gait evaluation with healthy subjects was required to confirm that the orthosis provided a safe, repeatable range of sagittal plane knee rotation to obviate the shortcomings of current nonpowered devices and to essentially determine whether the unit would work as planned. While the issue of stance control could not be addressed due to the inclusion of only normal subjects in this study, the issue of knee flexion range and tripping was thought to be a real one given the reduction to knee flexion with power KAFOs even with normal subjects. Therefore, the aim of this study was to perform a pilot study investigating the effect of a new powered KAFO on walking in healthy persons before testing with patients with lower limb weakness.
Methods
The new powered KAFO prototype
The newly designed powered KAFO utilized a lateral upright manufactured in aluminum incorporating a single-axis free knee joint (ORTHO SYSTEMS in motion, Kirchheim, Germany), connected to a 40W electric actuator (“Maxon Motor EC max30”; Maxon, Sachseln, Switzerland) with a planetary gearbox providing a reduction ratio of 111. It was designed to restrict knee flexion in stance phase of gait, and when the foot went into swing phase after push off, the actuator flexed the knee joint actively. Control of the actuator was provided manually by the volunteer subjects using a switch and was pushed by them when they unloaded the desired leg. One rechargeable 24-V battery (LiPo battery, Thunder Power RC G6 Pro Lite 25C 5400 mAh 6-Cell/6S) with 2 h of available continual working was used to provide power for the actuator. The battery and electronic unit of the new orthosis were suspended on a waist belt by the subjects and weighed 0.7 kg. The additional components of the new powered KAFO added 0.8 kg of extra weight compared to the unadapted orthosis.
Subjects
Five healthy subjects of mean age of 26 ± 5.6 years, weight of 66 ± 3.8 kg, and height of 176 ± 4.6 cm participated in this study. Exclusion criteria included any known history of orthopedic disease or any other ailment that would affect their ambulation. Each of the subjects was casted and fitted with a KAFO with a drop-locked knee joint and a new powered KAFO by an orthotist in Department of Orthotics and Prosthetics. The set of new powered orthosis was used in all subjects. The AFO portion of the drop-locked KAFOs and new powered KAFO was provided by casting the lower limb of each subject with their ankle joint positioned at approximately 5° of plantar flexion. The KAFO was not designed to be ischial bearing and used a thigh corset in its design. Lining material with durable-density polyfoam was added to the footplates of the AFOs. The uprights were made from aluminum, and the upright material was the same for both orthoses (Figure 1).

The new powered SCKAFO and the conventional KAFO used in this study.
The subjects performed orthotic gait training with the powered KAFO for accommodation purposes and to become conversant in how to control the orthosis during ambulation for five consecutive half-day sessions immediately prior to the walking trials. The subjects did not receive any walking acclimatization with the conventional KAFO due to its more simplistic structure. At commencement of stance phase, the knee joint was locked in an extended position. This position continued until to toe off phase (pre-swing), when the subjects, according to their detection, pushed the switch button, and the actuator began to provide active knee flexion until mid-swing, when active knee extension was provided in order to return the knee to full knee extension to position the lower limb for heel strike according to the programmable controller. The powered KAFO did not allow commencement of stance phase with the knee slightly flexed for safety reasons and therefore did not replicate the normal loading response evidenced during normal walking.
Subjects walked independently, without falling during data collection in the gait analysis laboratory. The University of Social Welfare and Rehabilitation sciences (USWR) gave approval for performing the study, and consent was obtained from each subject before they took part.
Gait analysis
Gait data were acquired in a motion analysis laboratory using a calibrated six-camera video-based motion analysis system (Oxford Metrics, Inc., Oxford, UK) with a capture frequency of 100 Hz. Reflective markers were put on the orthosis and the skin of the subjects at the following positions: bilaterally over the position of the greater trochanter, the lateral condyle of the femur, the head and lateral malleolus of the fibula, the second metatarsal, anterior superior iliac spine (ASIS), calcaneus, over the jugular notch, the spinous process of the seventh cervical vertebrae, and the acromioclavicular joints. Horizontal and vertical excursions of the hips were analyzed from the trajectory of the markers put on each ASIS.
The average of three walking trials was used for each subject while walking along a 6m walkway at their self-selected speed of walking in three test conditions during clinical testing. Two step cycles (i.e. one right and one left to provide a complete stride) were selected for the walking analysis. There were no significant differences between left and right. There was a resting period (1 h) between the walking conditions while the orthoses were changed. All subjects wore the KAFO with drop-locked knee joint first, which was then converted to a powered SCKAFO using the same thermoplastic thigh and AFO sections. This was done so that the effect of the orthosis on gait was isolated as far as possible to alteration to the orthotic knee joint. It was not therefore possible to randomize the procedure for testing using this method. The data were processed at 100 Hz with the VICON BodyBuilder model (Oxford Metrics). The data derived were then analyzed using MATLAB (MathWorks, Natick, MA, USA). The speed of walking was determined based on the marker data obtained from the marker attached to the calcaneus.
The mean speed of walking, step length, cadence, maximum knee flexion angle during swing, and compensatory motions were all calculated for each subject. The mean of these variables was computed for each of the three conditions (i.e. normal walking, KAFO, and new powered KAFO). Safety of walking with powered KAFO was evaluated by restriction of knee joint flexion in stance phase without falling. Knee flexion in swing phase was analyzed by actuator activity during ambulation in providing knee flexion. Works of powered KAFO were detected by providing more knee flexion than conventional orthosis during gait analysis in healthy subjects.
According to the small sample size (i.e. the number of subjects < 10), a normal distribution could not be assumed. The Friedman test as a nonparametric test was used to evaluate differences in parameters for all five subjects (JMP IN software; SAS Institute, Inc. Cary, NC). SPSS 16 was used for data analysis. The significant level considered was α ≤ 0.05.
Results
Kinematics
The mean maximum knee flexion angle (K1) and the maximum knee extension (K2) during loading response and the maximum flexion angle during swing phase (denoted K2) versus percentage of gait cycle for all the subjects for all three test conditions are shown in. At mid-swing, the new powered KAFO flexed the knee joint to a maximum of 40.2° ± 1.30° compared to 6.6° ± 0.89° when walking with the conventional KAFO. During stance, very little flexion was achieved. However, at pre-swing, knee flexion provided by the actuator was similar to the angle demonstrated during normal walking (Figure 2).
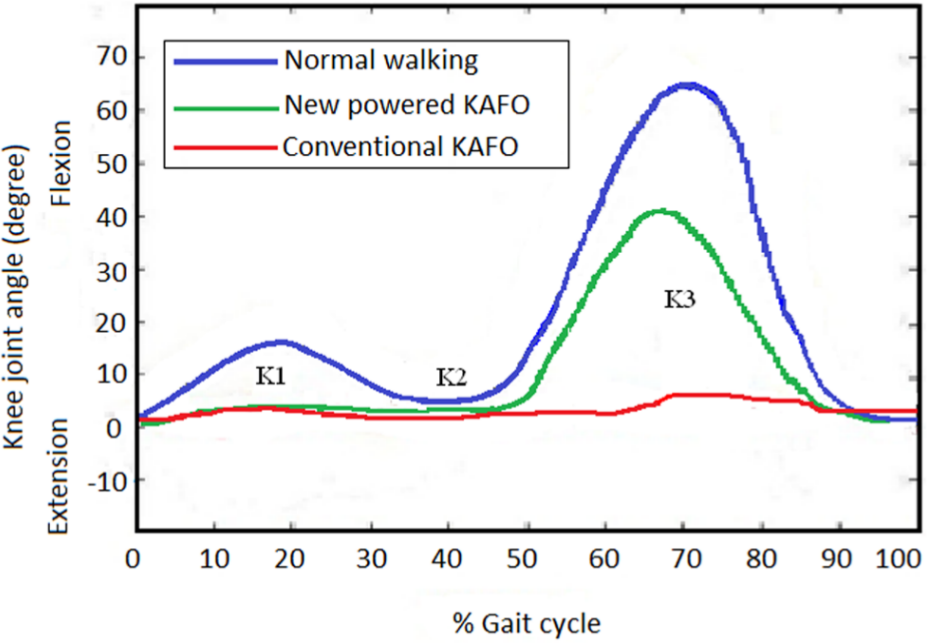
Sagittal plane kinematics of the knee joint in healthy subjects when walking with a powered or conventional KAFO compared to normal walking.
Spatiotemporal parameters
Mean spatiotemporal parameters of the subjects when wearing the conventional KAFO and the new SCKAFO compared to normal walking without orthosis are summarized in Table 1.
Mean (SD) of maximum knee flexion angle during swing and spatial–temporal gait parameters in walking with two types of KAFO and normal walking without orthosis.
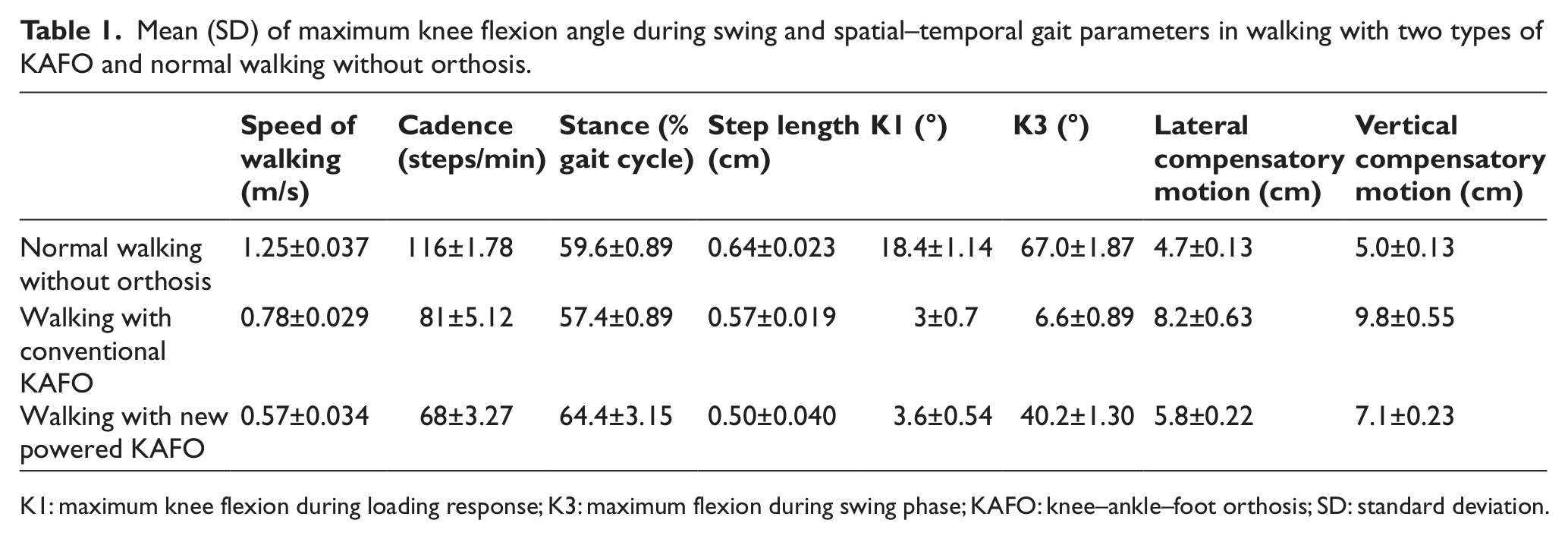
K1: maximum knee flexion during loading response; K3: maximum flexion during swing phase; KAFO: knee–ankle–foot orthosis; SD: standard deviation.
The mean speed of walking over all subjects with the new powered KAFO and with conventional KAFO were 54% and 37%, respectively, slower compared to normal walking without using an orthosis (Table 2). Walking with the powered KAFO and conventional KAFO also resulted in a mean of 21% and 10%, respectively, shorter step length compared to normal walking (Table 2). The cadence of walking was decreased using the two types of orthoses compared to normal walking. There were therefore significant differences in comparison between normal walking and walking with orthoses in temporal–spatial parameters and also between the two types of orthoses (Table 3). The conventional KAFO demonstrated greater speed of walking, cadence, and step length compared to the new powered KAFO.
Percentage change for each primary outcome measure compared to normal walking.
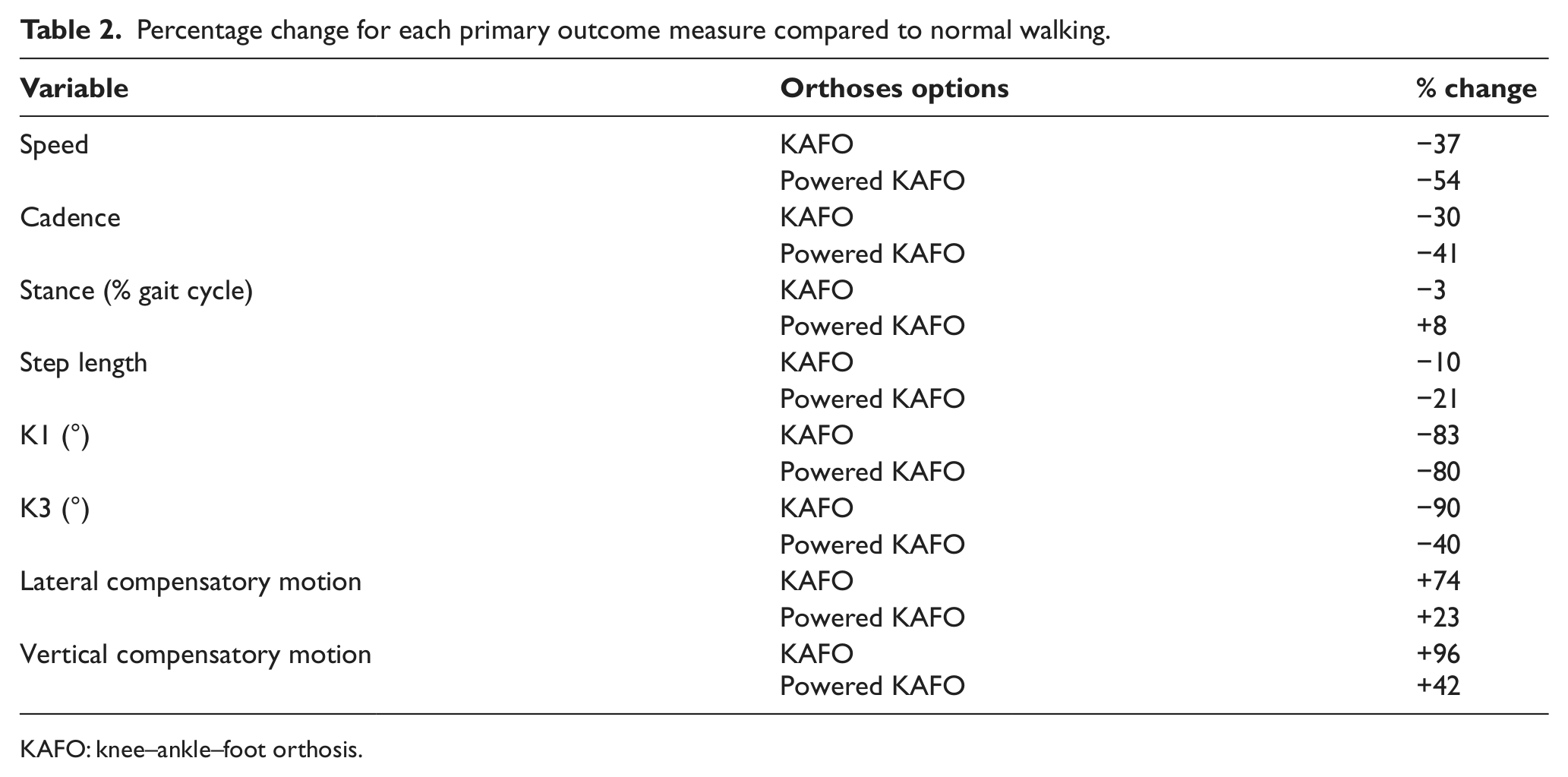
KAFO: knee–ankle–foot orthosis.
Comparison of maximum knee flexion angle during swing and spatial–temporal gait parameters in walking with two types of KAFO and normal walking without orthosis.
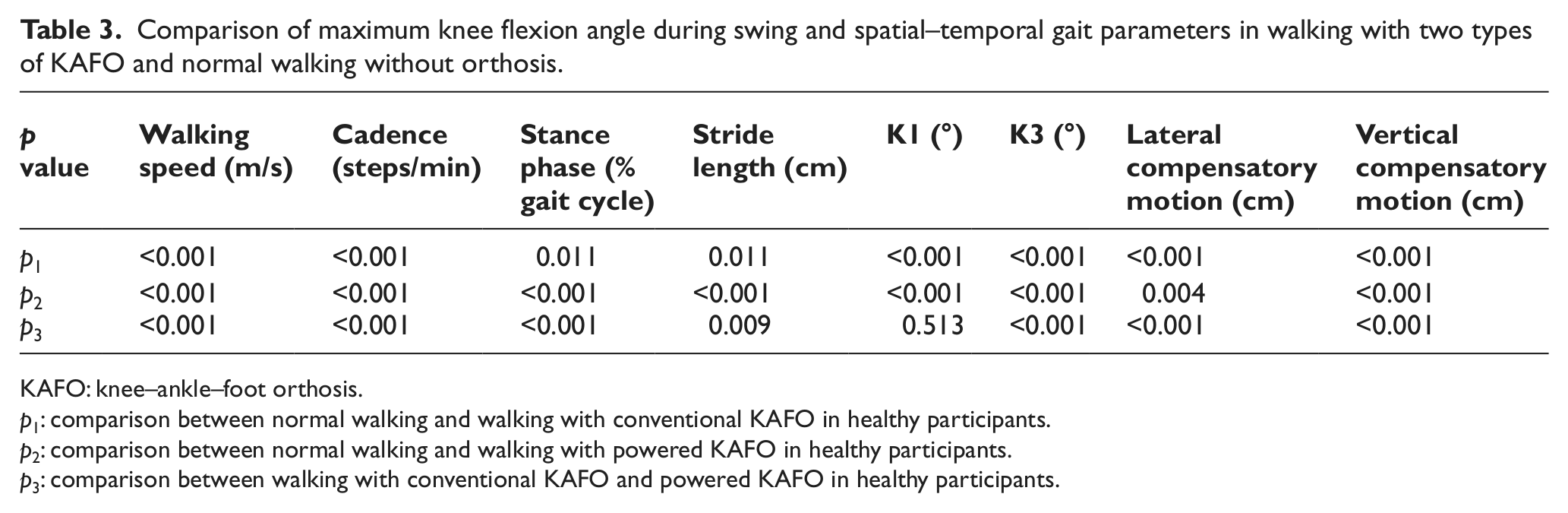
KAFO: knee–ankle–foot orthosis.
p1: comparison between normal walking and walking with conventional KAFO in healthy participants.
p2: comparison between normal walking and walking with powered KAFO in healthy participants.
p3: comparison between walking with conventional KAFO and powered KAFO in healthy participants.
Compensatory motions at the hip
Vertical hip motion during ambulation was greater than normal walking when using both the KAFO (96%) and powered KAFO (42%). In addition, more lateral compensatory motion (74% and 23% in using the conventional KAFO and the new orthosis, respectively) was also observed compared to normal walking, which proved to be a statistically significant difference (Figure 3).
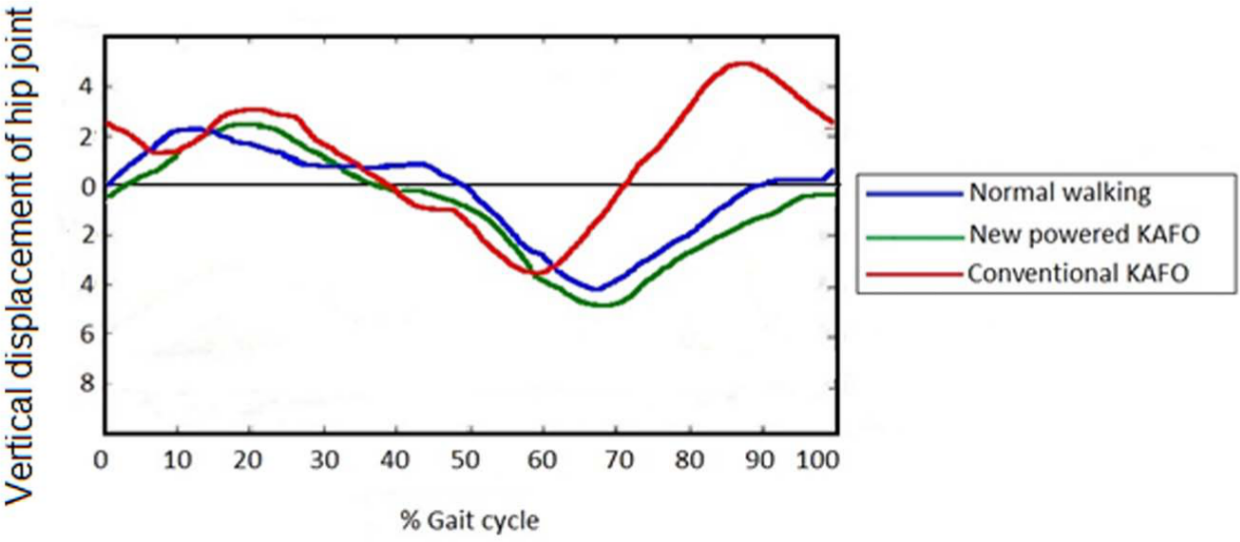
Mean vertical displacement of the hip when walking with the conventional KAFO and powered KAFO.
Discussion
This study investigated the effect of a new powered KAFO design on walking in healthy persons compared to normal walking and also a conventional KAFO. This study determined that more knee flexion was possible for healthy people during ambulation in both swing and stance phases compared to walking with a powered KAFO or conventional KAFO. Decreased knee flexion poses a problem for swing phase of gait, which inevitably occurs with increased vertical displacement as noted in this study. This may have an effect on trips and falls, but this is as yet untested. Nevertheless, it was thought necessary to design the powered orthotic knee joint to provide active knee flexion during swing phase of gait to obviate this.
Based on the knee flexion pattern in walking with the new powered KAFO, less vertical displacement of the hip joint may be expected due to the reduced vertical and lateral compensatory motions demonstrated compared to the conventional KAFO, which could lead to a more efficient gait pattern with the new orthosis. Similar results were reported by Ohta et al. 16 and Arazpour et al. 10 for spinal cord injury patients walking with a powered gait orthosis. In addition, the positive effects of SCKAFO use on pelvic movement such as smoothing of pelvic movement and pelvic obliquity have previously been demonstrated by McMillan et al. 3 and Irby et al. 8
A more natural gait pattern in knee flexion during swing was provided by the new orthosis, as has been previously demonstrated in other SCKAFO designs. The mean of this parameter was reduced using the SCKAFO in this study compared to normal walking without an orthosis. However, when compared to previous studies in this field, the mean reported range of knee motion with a SCKAFO was 44° in studies by Hebert and Liggins, 6 Irby et al., 8 and Kaufman et al. 4 This was more than achieved in this study. However, there is potential to improve this parameter by further development of this new orthotic device. The mean knee flexion in swing was 40% less when compared to normal walking, and a method of improving this parameter should therefore be considered in further development of this orthosis. Provision of knee flexion by an orthosis can reduce compensatory patterns of walking such as hip hiking, vaulting, and circumduction compared to walking with conventional KAFO. Providing a near-normal pattern of walking in the affected side could reduce the muscular effort needed for the unbraced side during ambulation.
Although the mean speed of walking was reduced significantly in both orthotic test conditions compared to normal walking, the new orthosis produced significant slower walking when compared to the conventional KAFO. A similar result was demonstrated for step length and cadence compared to normal walking. The angular velocity that the motor could provide was low, which automatically increased the swing phase duration and thereby decreased walking speed with the powered KAFO. Since walking speed is highly important for patients and is highly correlated to functional ability, this parameter should be improved with optimization of the method of knee orthotic joint actuation (e.g. by using a load cell mounted underneath the heel of the affected side to initiate motion using a controller that could be programmed to initiate knee motion when weight was fully transferred onto the affected foot). Improvement of knee joint design or longer periods of acclimatization with the powered KAFO would also be recommended for further studies in this field.
In comparison with the literature in this field, our results were similar to that demonstrated by Irby et al. 8 and Yakimovich et al. 17 However, one study has reported an improvement of speed of walking and step length with a SCKAFO. 3
Some limitations of this study should be considered. First, this study was performed with the help of healthy volunteer subjects. Further study of new orthosis should be evaluated on patients with lower limb weakness. In this study, energy consumption was not considered and the period of accommodation was short, and indeed, subjects were only acclimatized to the powered SCKAFO. The test method did not utilize randomized sampling and is a limitation of the study. However, there was an approximate hour of rest between testing sessions for the different orthoses, so carryover effects would be minimal. In addition, the new KAFO requires active hand control to operate, and it will currently only be suitable for use by a patient population with cognitive, upper extremity coordination.
Conclusion
The results of this study indicated that the new powered KAFO provided safety and knee flexion during walking. New powered KAFO decreased compensatory motions and increased knee flexion compared to conventional KAFO. Future studies with volunteer patients with lower limb paralysis on energy consumption will be beneficial in this field and should also involve patients with stroke or poliomyelitis and should enable a longer term of accommodation with a powered KAFO.
Footnotes
Conflict of interests
The authors do not have any conflicts of interest with regards to the study presented in this paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.