
Abstract
Background:
Amputation is a life-changing event accompanied by challenges for the affected person with time-dependent depression often used to quantify its level of impact on their psychological well-being. There are varied factors that contribute to this and its persistence. The aim of this study was to explore the experiences over time of people with diabetes and/or peripheral vascular disease following an amputation and the impact on their psychological well-being.
Objectives:
To develop an understanding of the experience of living with an amputation and a chronic condition in order to help clinicians identify those in need of counselling support.
Study design:
A qualitative study utilising an iterative approach in line with the philosophy of interpretive phenomenology.
Methods:
Six participants who had experienced a lower limb amputation associated with peripheral vascular disease/diabetes were interviewed on two occasions (baseline and 4 months). An interpretative phenomenological approach was utilised for both data collection and analysis.
Results:
For these participants, amputation was part of the chronology of their chronic disease. It was the individual’s variable experience of health which impacted their psychological well-being rather than the length of time since amputation.
Conclusions:
The multivariable experience of amputation means that individually tailored counselling/psychological support is recommended.
Clinical relevance
An understanding of how the experience of living with an amputation and a chronic condition may change over time will help clinicians to identify the ongoing need for counselling support.
Keywords
Background
Amputation is a dramatic, life-changing event usually accompanied by a multitude of challenges for the affected person1–6 with time-dependent depression often used to quantify its level of impact on psychological well-being.4–11 Studies suggest a higher incidence of depression among amputees compared to the general population.5,6,8,10 Additionally, Singh et al. 11 found a reoccurrence of depressive symptoms 2–3 years post-amputation. These studies5,6,8,10,11 also identify that age, the cause of amputation, the person’s level of general health, and the level and intensity of phantom pain influence the occurrence and impact of depression over time. In their review, Horgan and MacLachlan 12 concluded that depression is a normal reaction immediately post-amputation and can remain for an average of 2 years, decreasing over a period of 8 years.
As various factors contribute to the occurrence of depression5,6,8,10–12 and its persistence over time, establishing support for people who have undergone amputation is challenging. In the United Kingdom, it is customary that people receive introductory counselling at their rehabilitation centre soon after a lower limb amputation. However, the onus is then on them to request counselling again if their needs remain or change. This is problematic given that depression can remain for up to 3 years11,12 and that older people who have undergone amputation are unlikely to seek counselling. 13 Furthermore, for those with diabetes and/or peripheral vascular disease, depression may already exist before the amputation.14,15 This may add to the complexity of the factors that lead to it persisting over time. It is important that clinicians are able to understand the complexity of physical and psychological well-being so that appropriate support can be provided. Depression can be measured with existing tools, 16 but these may not capture the persons overall feelings of well-being and there is no quantifiable tool to measure this.
Therefore, the aim of this study is to explore the experiences of people with diabetes and/or peripheral vascular disease following an amputation and the impact of this on their psychological well-being. The study is based on the underpinning philosophy of interpretivistic phenomenology 17 which acknowledges the researchers prior experience and knowledge of the subject area through a process of reflexivity while recognising both the uniqueness and similarities of the participant’s personal experiences. 17
Methods
Study design
In order to explore the personal experience of living with an amputation and its impact on their psychological well-being over time, a qualitative study based on the philosophy of interpretivistic phenomenology was designed. An iterative approach to data collection and analysis was employed in line with the requirements for the process of interpretive phenomenological analysis. 17
Participants
Ethical approval was obtained from the University of Bolton and the North Manchester Research and Ethics Committee. Potential participants were identified at the Manchester Disablement Services Centre. A purposive sampling criterion was used with the participants having undergone a unilateral lower limb amputation due to peripheral vascular disease and/or diabetes during the previous 14 months and could demonstrate a suitable level of English and cognitive ability in order to be interviewed. Six patients consented to be interviewed twice at baseline and month 4.
Data collection
Data were collected via audio digital recording of semi-structured interviews. Both interviews lasted approximately 1 h and were carried out at the Manchester Disablement Services Centre at Withington Hospital Manchester. The first interview incorporated elements identified from a literature review as well as allowing for new areas and personal experiences to be explored. For example, Has undergoing an amputation changed the way you see yourself? Has undergoing an amputation affected your everyday life?
The second interview incorporated areas and experiences identified in the first interview in order to allow reflection and explore any changes that may have occurred. Field notes were made immediately after the completion of individual interviews to supplement the data.
Data analysis
The digital recordings were transcribed verbatim and then an iterative approach to data analysis was carried out. The transcripts from the interviews at baseline and at 4 months were annotated closely, ‘coding’ for insights into the participants’ experiences through analysis of their words, phrases and interpretation of their meaning. This was followed by cataloguing of the codes into ‘themes’ which were then organised into clusters and subordinate themes and further categorised into the final super-ordinate themes. 17 Continuous re-examining of the transcripts was carried out to ensure the analysis retained ‘what’ the participant said and remained grounded in the data.
Results
There were four male participants with a mean age 64.8 years (standard deviation (SD) = 7.95) and two female with a mean age 69 years (SD = 10.32). (Participants details can be viewed in Table 1).
Participant details.
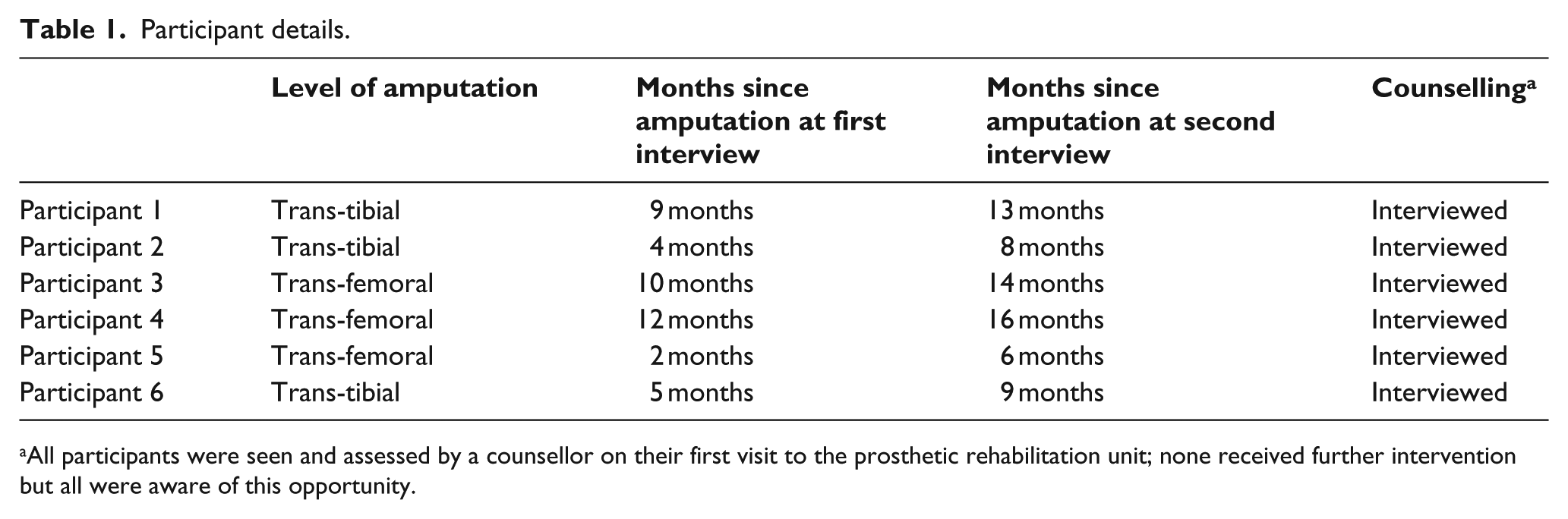
All participants were seen and assessed by a counsellor on their first visit to the prosthetic rehabilitation unit; none received further intervention but all were aware of this opportunity.
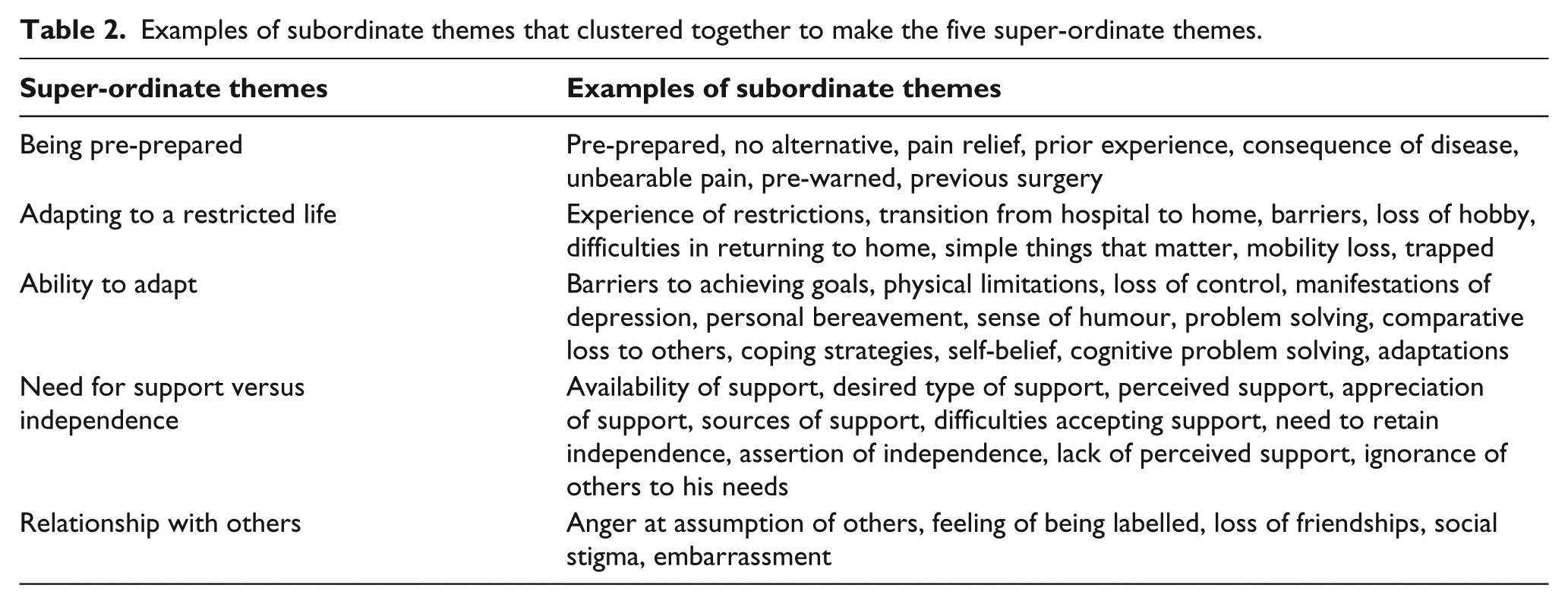
For half the participants, there appeared to be a steady or improving picture in terms of their general psychological well-being between interviews. However, half of the participants did reveal significant negative changes in this well-being over this short time frame in relation to complications. It was clear from the second interview that undergoing amputation is a very personal experience. Those individuals with serious complications such as an unhealed residuum (Participant 1), the threat of further amputations (Participant 4) and diabetic complications (Participant 6) are most at risk of poor psychological well-being and need more ongoing counselling. This demonstrates the complex interplay of living with a chronic disease, the amputation itself and the associated complications. Five themes (Table 2) emerged from the data which illuminate the participants overall experiences. These experiences may relate to the onset and persistence of depression.
Examples of subordinate themes that clustered together to make the five super-ordinate themes.
The first interview revealed the participants’ reflections of events leading up to the amputation as this clearly had an influence on outcome.
Theme 1: being ‘Pre-conditioned’
The participants expressed the feeling that the disease process and pre-amputation preparation can assist eventual acceptance of the process. All of the participants had undergone limb salvage operations. Five of the participants knew that amputation was a possible consequence, using words such as ‘semi-conditioned’, ‘pre-conditioned’ (Participant 3), ‘no shock’ (Participants 3 and 4), and ‘on the cards’, ‘accustomed to’, and ‘natural course’ (Participant 2). Pain relief from the effects of vascular insufficiency and infection was the foremost priority for this group and they therefore considered the risks associated with amputation as justifiable: Even if I … didn’t survive it wouldn’t have mattered. The pain and illness was that bad. (Participant 1)
Others noted that having an amputation was a ‘… no brainer …’ (Participant 5) and rationalising it in relation to a more negative outcome ‘… as it is, you live …’ (Participant 4). They felt that amputation was effectively a choice of life over death.
Theme 2: ‘Adapting to a restricted life’
At the first interview, all participants described limitations or mobility restrictions brought about by amputation which affected a wide range of activities. The realisation of these limitations came in waves as they moved through the post-amputation stage.
Initial period – post-amputation
Most reported a concern initially following amputation with regard to their changing lives and how they would cope: How am I going to cope now …?. (Participant 6)
But acceptance of amputation came with the realisation that they had no choice and they had to get on with life: … put that part of my life behind me. Just go on from there …’ (Participant 5)
However, one participant struggled to accept her unexpected amputation. She feared the limitations and she felt she was to blame due to her diabetes: I didn’t realise I would have an amputation’ I didn’t realise the restrictions … It is sad that it happened because of the diabetes because you kind of blame yourself. (Participant 6)
Despite the feeling of acceptance in hospital, most found the initial transition between hospital and home difficult: I didn’t realise how much it does affect you … Till I got home and I realise now I have got to get about in the wheelchair and it is not in a straight ward. (Participant 6)
However, in most cases, these restrictions subsided as they lived in supportive environments with appropriate adaptations and/or where they could rely on the assistance of others.
Ongoing restrictions
Limitations were still evident in the second interview but had changed over time. Participant 5 was doing extremely well in terms of his mobility, and his focus had changed from residuum concerns to anticipating the advantages of new prosthetic components: Each month I find I can do something different. (Participant 5)
Participants 2 and 3 continued to improve their general mobility, although their prosthesis usage was still low: I acquired a 3 wheeled scooter … I can now get up to the bowling green … (Participant 2)
Participant 1 had limited mobility caused by his unhealed residuum which prevented his return to work, causing distress. One participant required a bypass on her remaining leg with the possibility of a further amputation. This led to doubt about whether she would ever walk again: If this one is above the knee. I won’t be able to walk. (Participant 4)
Participant 6 had been bed bound for some time, causing a knee contracture to develop that prevented her from walking at all. She stated that it was … a bit of a shock … . I have to accept that I am not as good as I thought I would be.
Her amputation and the complication associated with this compounded the effects of living with a chronic condition. The restrictions reported appear to be related to whether the amputation was expected or not, and whether the participant had rationalised the need for the amputation. Ongoing complications and poor health are the main reasons for an apparent negative psychological impact. Those who did not have complications were able to accept their restricted mobility.
Theme 3: ‘Ability to adapt’
Most of the participants revealed that positive thinking, problem solving and a sense of humour were central to adapting to life after amputation: There is always a solution to most things (Participant 1)
and A sense of humour is a necessity … (Participant 3)
There were other differences in the participants’ ability to adapt. Participant 1’s return to work was halted by his unhealed residuum which left him feeling that he had hit a ‘stalemate’ situation.
He felt less valued; his own view of ‘self’ and worth was linked to being useful and productive: If I could get back to work everything would be normal … I don’t want to be stuck on the scrap heap … Once I am up and going I won’t see it has an issue. (Participant 1)
His inability to return to work was made worse by his apparent lack of control over his residuum healing. He alternated between positive thoughts and doubts which showed a conflict between his cognitive assessment of the situation and his desires: … I am positive about it and I don’t foresee any sort of problems, but I am also quite a practical person thinking maybe I will or won’t … (Participant 1)
He knew that he would eventually have to make a decision regarding work but wanted it to be his choice, not dictated by his residuum: … it’s annoying me because I don’t want it (residuum) to win … I don’t want my left leg or lack of leg to rule me. (Participant 1)
It is clear that these participants faced varying restrictions in their lives compared to pre-amputation. However, it is also evident that the level to which these restrictions affected the individual was not based purely on the level of those restrictions but on their aspirations for mobility. Those with higher aspirations and lower mobility tended to be more affected by limited mobility than those with moderate, lower aspirations where limitations were accepted.
Theme 4: ‘Need for support versus independence’
With the exception of one participant, all reported that they had strong support networks which they valued: Knowing the children are always there, that helps a lot. That gives a lot of confidence. (Participant 4)
However, some needed to negotiate the level of support required, with many families being over-supportive or protective and taking over tasks that individuals felt capable of doing. One participant reported having to be very proactive in moderating the level of support offered: Whoa, whoa, whoa, stop. I can sort things out. (Participant 1)
And Participant 5 talked about being over-protected: ‘… finally got her head round it; she can leave me alone for 3 or 4 hours and I am not going to disintegrate.
There was also an element of not wanting to be a burden and maintaining their own self-esteem: ‘They have lives of their own’ (Participant 4) and, ‘Without your leg it is difficult to get to the toilet … they provided me with a water bottle and it was seeing him come in and just empty it for me, it just uurrrhh, it just felt wrong. (Participant 1)
There were many examples of support from families and loved ones that show the importance of this to the individuals’ adjustment and recovery. This is clearly an importance adjunct to professional support through counselling. However, the families clearly needed support in relation to the level of physical care they offered as this could impact on psychological well-being. When this support is absent is clearly causes distress and adds to the participant’s negative experience as articulated by participant 6: I’ve only seen my son once, once in six weeks … but she (daughter) hasn’t been once and she’s not even given an excuse.
Theme 5: ‘Relationships with others’
Only one of the participants revealed that they felt socially isolated. However, a number noted that undergoing an amputation had affected friendships: … You find out who your real friends are … since I was in the hospital I have hardly heard from him at all. (Participant 2)
Some put this down to social embarrassment with participant 5 revealing that the amputation seemed like the ‘Elephant in the room’. In contrast, for those able to re-enter normal social activities, this supported adjustment to the amputation. There were some variances between the ways in which the participants felt others viewed them: … people stare at you … That’s because I have lost my leg. I don’t feel like a proper person … May be it will be different when friends do start coming round but at the moment I feel such a burden. (Participant 6)
This further emphasises the potential for friends to have a positive role in helping with the adjustment to living with an amputation.
In contrast, others’ opinions and advice may have a negative effect: They say … ‘Why don’t you stay on the sick?’ … that sort of devalues you. (Participant 1)
Although this group stated that they would not let the views of others impact them or stop them engaging in activities, it is apparent that this has a negative impact on these participants.
The factors identified within these themes clearly show that there are influences on their experience of having an amputation and their adjustment to it. These factors could be associated with depression. However, what has been found is that post-amputation experience is dependent on pre-amputation adjustment, having an ability to retain some control, appropriate support from family and friends, readjustment in relationships, the incident of complications and fear of further amputation.
Discussion
This study has provided insight into these participants’ experiences of living with an amputation and has revealed factors that may influence whether people experience post-amputation poor psychological well-being which may lead to depression. Previous literature5,6,8,10,11 has identified that age, the cause of amputation, general health, and the level and intensity of phantom pain influence the occurrence and impact of depression over time. In addition to these factors, this study paints a complex picture of the interactions between their chronic disease, the expectation of the amputation, adjustment pre-amputation, the appropriate support of family and friends after the amputation, readjustment in relationships and the fear generated by complications. The impact of the amputation in those with long-term chronic disease is compounded as these are already linked to levels of depression.14,15,18 Indeed, the participants reported the difficulties of their underlying health in addition to the impact of the amputation. Consequently, it is important to recognise that individuals that have undergone amputation with related chronic diseases may need different support and counselling from those who undergo amputation due to trauma.
Most participants in this study felt prepared for the amputation as they were pre-warned about this possibility. This notion is supported by Rybarczyk et al., 19 who stated that those who have amputation due to vascular disease may have time to prepare themselves. However, they still reported anxiety about the future which indicates a need for early counselling and support which has been recommended as being beneficial at 6 months post-amputation. 7
As previously identified, 20 the transition from hospital to home also proved difficult for the participants in this study as the reality of their new ‘self’ in terms of their physical abilities became more apparent as they returned to their normal home environment. Physical restriction was related to perception of ‘self’ and may have had an effect on psychological health. Also, those who lived alone experienced higher levels of anxiety following discharge from hospital, aligning with the work of Singh et al. 21 Coping with anxiety needs to be addressed within the period of transition and adaptation to their home environment. Where there are issues of poor health and low levels of support, a gradual transition to home from hospital may be desirable.
This study has revealed the benefits of social support from family and friends, as long as it was considered appropriate and focussed on the needs of the person. It is known that this has a protective benefit 22 and that it is beneficial in terms of general adjustment to amputation 23 with greater life satisfaction, mobility and more engagement in meaningful activity. 24 Social support is clearly crucial to the process of adjustment in the social context, but in the persons work environment, there may have to be additional adjustments.
The experience of one participant in this study aligns with Burger and Marinček 25 in that individuals who undergo amputation are found to have less employment opportunities with many finding it difficult to return to their present occupation, especially if it is a physically demanding job. Productive work and maintenance of status are important to amputees in relation to their identitiy. 1
A further perspective on identity in addition to occupational role is that of a changed body. There is evidence that those who undergo amputation may feel that their body is strange, unfamiliar and mutilated. 20 Interestingly, this self-image was not obviously evident in this study, more the perception of ‘others’ view of them as being ‘disabled’ or other negative views. Social stigma is linked to increased rates of depression and that these cause activity restriction due to social discomfort and feelings of vulnerability.12,26
For these participants, amputation was one of the stepping stones to be crossed in their experience of living with a chronic disease. Therefore, we recommend that people with chronic disease who require a planned amputation have counselling which includes family and close friends from an early stage. This has the potential to aid adjustment after the amputation through ensuring that family and social support is appropriate, allows for the development of independence and maintains identity as much as possible. Dependent on the persons underlying disease and the potential physical complications, associated post-amputation counselling and support should be tailored to the persons needs as recommended by Rybarczyk et al. 8 It is apparent from this study that ‘counselling’ role and the support of family members and friends have for these participants is crucial in their longer term recovery and adjustment over time. It is also important that longer term counselling should be available according to the persons changing needs over time and in relation to both their amputation and their chronic disease.
Further work is recommended in order to evaluate the long-term effects of a tailored approach to professional counselling which is aligned with the social support from families and friends.
Limitations of the study
This study aimed to explore the experience of undergoing amputation due to diabetes/peripheral vascular disease in those over 55 years of age and therefore further research is required to look at other distinct groups. Ideally, the participants would have been followed for the entire 18 months of their post-amputation period but time restrictions for the research made this impossible. Some of the questions utilised in the interview were closed which may be perceived to be a weakness in the study design. However, the participants did not respond in a ‘closed’ way, rather they expanded on their response of ‘yes’ or ‘no’ in order to justify and explain their responses. In this way, the questions can be viewed as ‘triggers’ which the participants used to reveal their thoughts and experiences. A perceived limitation could be seen to be the sample size. However, it was not the intention to survey a large and diverse population in order to be generalisable with the results but to gain in-depth insight into the participants experiences which is in line with the philosophy of interpretive phenomenology and which cannot be examined using other methods. 27
Conclusion
In this group of participants, their experience of a long-term chronic disease plus an amputation illuminates the complexity of factors that may contribute to poor psychological well-being which may in turn lead to depression and also those factors that may positively influence their overall experience. There is a need for tailored and timely professional counselling which links with the social support that families and friends provide.
Footnotes
Acknowledgements
We would like to thank the research participants who gave their time and expertise and the staff at the Manchester Disablement Services Centre and the Directorate of Prosthetics, Orthotics and Podiatry at the University of Salford.
Author contribution
The original research was carried out by Elaine Washington as part of an MSc in Psychology at the University of Bolton. Dr. Anita Williams contributed to the preparation of data and the writing of this article.
Declaration of conflicting interests
The authors declare no conflict of interest.
Funding
This research was carried out as part of an MSc in Psychology funded by the University of Salford.