
Abstract
Background:
Lower limb amputation leads to impaired balance, ambulation, and transfers. Proper fit of the prosthesis is a determining factor for successful ambulation. Vacuum-assisted socket systems extract air from the socket, which decreases pistoning and probability of soft-tissue injuries and increases proprioception and socket comfort.
Objectives:
To investigate the effect of vacuum-assisted socket system on transtibial amputees’ performance-based and perceived balance, transfers, and gait.
Study design:
Quasi-experimental before-and-after study.
Methods:
Subjects were initially assessed using their prosthesis with the regular socket and re-evaluated 4 weeks after fitting including the vacuum-assisted socket system. We evaluated the mobility grade using Medicare Functional Classification Level, Berg Balance Scale, Four Square Step Test, Timed Up and Go Test, the 6-Min Walk Test, the Locomotor Capabilities Index, Satisfaction with Prosthesis (SAT-PRO questionnaire), and Houghton Scale.
Results:
A total of 16 unilateral transtibial dysvascular amputees, mean age 65.12 (standard deviation = 10.15) years. Using the vacuum-assisted socket system, the patients significantly improved in balance, gait, and transfers: scores of the Berg Balance Scale increased from 45.75 (standard deviation = 6.91) to 49.06 (standard deviation = 5.62) (p < 0.01), Four Square Step Test decreased from 18.18 (standard deviation = 3.84) s to 14.97 (3.9) s (p < 0.01), Timed Up and Go Test decreased from 14.3 (standard deviation = 3.29) s to 11.56 (2.46) s (p < 0.01). The distance walked in the 6-Min Walk Test increased from 288.53 (standard deviation = 59.57) m to 321.38 (standard deviation = 72.81) m (p < 0.01).
Conclusion:
Vacuum-assisted socket systems are useful for improving balance, gait, and transfers in over-50-year-old dysvascular transtibial amputees.
Clinical relevance
This study gives more insight into the use of vacuum-assisted socket systems to improve elderly transtibial dysvascular amputees’ functionality and decrease their risk of falls. The use of an additional distal valve in the socket should be considered in patients with a lower activity level.
Background
It is estimated that 115,000 individuals require an amputation of a lower limb due to peripheral vascular disease in the United States each year. Of those, 30% are transfemoral and 70% are transtibial amputations. 1
Lower limb amputation leads to a series of physical consequences that are associated with functional limitations that may affect the patient in different ways. The most common ones are impaired balance, ambulation, and ability to transfer.1 –3 These changes are also related to the amputation level; higher amputation levels are associated with more severe consequences than lower levels. Factors such as the age of the patient, comorbidities, and motivation also influence the outcome of prosthesis fittings. The success rate of prosthesis fitting in elderly dysvascular patients is low and also related to the level of amputation. Fletcher et al. 4 found that only 36% of all older amputees received proper prostheses (64% in transtibial, 31% in transfemoral).
One of the factors that impede adaptation to the prosthesis is change in the volume of the residual limb as a result of the forces acting on the residual limb especially during weight-bearing activities (like transfers and ambulation). These volume fluctuations promote pistoning (axial relative movement between the residual limb and the socket), cutaneous irritations or injuries, discomfort, and, occasionally, reductions in activity. 5 Therefore, proper fit of the prosthesis to the residual limb is a determining factor for obtaining successful ambulation in amputee patients. 5
Various studies have shown the impact of prosthetic devices on amputee patients’ mobility to the point that some patients are even able to modify and reduce some of the limitations brought about by amputation.3,5
Vacuum-assisted socket systems (VASSs) are devices which employ a pump to actively extract air from the socket through a unidirectional valve, generating a negative pressure between the socket and the liner that covers the residual limb. 3 There are various studies which show the usefulness of these devices for keeping the residual limb volume stable2,3 and facilitating contact between the socket and the residual limb. The clinical benefits of this effect are as follows: decreased pistoning and probability of soft-tissue injuries as well as increased proprioception, control of the prosthesis, walking capabilities, and socket comfort.2,3,6
Elevated vacuum socket systems have been marketed for the prevention and/or treatment of skin injuries of the residual limb that result from the friction created between the skin and the socket.
The primary objective of this study was to investigate the effect of a VASS on balance, transfer ability, and ambulation in dysvascular transtibial amputees over 50 years of age. Other objectives were to study the patients’ perception of prosthesis use, satisfaction, and functional capabilities, and to assess the relationship between the benefits of using a VASS and the patients’ mobility grade, which may have to be considered when fitting the prosthesis.
Methods
This research received approval from the center’s research ethics committee. It’s design was based on a quasi-experimental before-and-after intervention study in which the intervention being studied was performed according to the approved indications. The study sample comprised 16 amputees who were 50 years of age or older with the following inclusion criteria:
Unilateral transtibial amputation;
Prosthesis use for at least 6 months prior to enrollment;
Ability to walk indoors with or without supervision and with or without ambulation aids;
Informed consent to participate in the study.
Criteria for exclusion were the existence of cognitive impairments hindering the ability to follow instructions and/or perform the tests. The patients were recruited at routine follow-up outpatient visits carried out in the Amputee Unit of our hospital’s Rehabilitation and Physical Medicine Department. Those who met the selection criteria and gave their informed consent were enrolled as participants.
Study and intervention method: VASS
The VASS studied was the Ottobock Harmony® P2 & HD (Otto Bock HealthCare GmbH, Duderstadt, Germany). The mechanical pump of the VASS is placed under the socket and activated by the body weight at each step, thus maintaining a defined range of negative pressure between the inner wall of the socket and the polyurethane liner.
Patients were initially assessed using their usual prosthesis. Since installing the VASS requires a substantial modification of the socket, a copy of their usual socket was made for each patient, and the VASS was adapted following the manufacturer’s instructions. The use of the VASS does not require specific training. Patients were given an explanation of its function and were recommended to use it for 4 weeks prior to re-evaluation to ensure proper adaptation to the new socket.
The patients’ overall mobility grade was evaluated based on the Medicare Functional Classification Levels (MFCLs). 7 This classification describes mobility levels with MFCL-0 being non-ambulatory and without the potential to ambulate with a prosthesis, MFCL-1 being restricted only to household ambulation, MFCL-2 having limited abilities to ambulate in the community, MFCL-3 demonstrating unlimited community ambulation, and MFCL-4 being a very active user whose mobility exceeds basic ambulation skills.
To evaluate the effects of the two different socket designs, the following scales and tests were used.
Evaluation of balance
Berg Balance Scale
The Berg Balance Scale (BBS) is a 14-item scale designed to evaluate balance. Scores vary between 0 and 56 points, with higher scores reflecting a greater ability to balance. It is a validated test, and the minimum detectable changes in elderly populations have been described.8,9
Four Square Step Test
The Four Square Step Test (FSST) is a test that assesses the risk of falling among amputees. It records the time in seconds that the patient takes to step into four squares that are formed by two crutches, starting in clockwise direction and then stepping back in counter-clockwise direction. In transtibial amputees, a time of 24 s or more is considered a predictive value of falling. The FSST has high consistency, sensitivity, and specificity and has shown excellent inter-observer and test–retest reliabilities. 10
Functional evaluation of gait and transfers
Timed Up and Go Test
The Timed Up and Go Test (TUG) is considered a measure of basic mobility including ambulation and ability to transfer and turn. The time (in seconds) that the patient takes to stand up from a seated position in a chair, walk 3 m forward, turn 180°, and return to the initial position is measured. The test is finished when the patient is once again seated. This test has been proven reliable and valid for evaluating physical mobility and risk of falling in transtibial amputees.11,12
6-Min Walk Test
The patient must walk between two points that are 24 m apart for 6 min. The total number of meters walked during those 6 min is recorded. This test has been previously used for evaluating walking capacity and overall function of transtibial amputees. 13
Subjective evaluation of the prosthesis
Assessment of the locomotor capability: Locomotor Capabilities Index
The Locomotor Capabilities Index (LCI) is a self-administered questionnaire specifically for patients with amputation of a lower limb which evaluates overall locomotor ability and patient independence. It consists of 14 questions on different locomotor activities performed in the last 4 weeks. The final score varies between 0 and 42 points, with a higher score implying greater mobility.14 –16
Evaluation of the patient’s satisfaction with the prosthesis: SAT-PRO questionnaire
This is a self-administered questionnaire for determining the patients’ satisfaction with the use of the prosthesis. It consists of 15 categories. Lower scores indicate higher satisfaction. 16
Evaluation of the use of the prosthesis: Houghton Scale
This is a self-administered scale used to determine the use of the prosthesis. It consists of four categories. Its use is recommended for routine clinical practice.8,17
Statistical analysis
Averages and standard deviation (SD) were used for the descriptive statistics of quantitative variables. Percentages were used for qualitative variables. The non-parametric Mann–Whitney U-test was used to analyze the differences between dependent quantitative variables, and the Wilcoxon test was used to evaluate the differences between independent quantitative variables. Subgroup analyses of the results were performed for the two MFCLs in the study sample. Results with p < 0.05 were considered statistically significant.
Results
The total number of participants was 16, 87.5% men and 12.5% women. The average age was 65.12 (SD = 10.15) years. The etiology of amputation was peripheral vascular disease in all cases, and all patients had also been diagnosed with diabetes mellitus.
A total of 6 patients (37.5%) were assigned to the MFCL-2 and 10 patients (62.5%) to the MFCL-3 mobility grade, creating two subgroups for further analysis. The average time since amputation was 5.2 (SD = 2.2) years.
The results of the overall evaluation of the 16 patients were the following. Evaluation of balance. On the BBS, patients obtained an average score of 45.75 (SD = 6.91) using their previous socket and 49.06 (SD = 5.62) when using the VASS. This difference was statistically significant (p < 0.01). To complete the FSST, patients took an average of 18.18 (SD = 3.84) s when using their regular socket and 14.97 (SD = 3.9) s when using the VASS. This difference was statistically significant (p < 0.01).
Results for the functional evaluation of gait and transfers were as follows: for the TUG, the patients took an average of 14.30 (SD = 3.29) s when using their previous prosthesis and 11.56 (SD = 2.46) s when using the VASS. This difference was statistically significant (p = 0.01). While performing the 6-Min Walk Test (6MWT), patients walked 288.53 (SD = 59.57) m with their regular socket VAS and 321.38 (SD = 72.81) m with the VASS. This difference was statistically significant (p < 0.01).
The results of subjective evaluation were as follows: on the LCI questionnaire, patients scored an average of 43.31 (SD = 10.32) without the VASS and 47.44 (SD = 7.97) with the VASS. This difference was not statistically significant. On the Satisfaction with Prosthesis (SAT-PRO) Scale, values of 27.50 (SD = 12.44) were obtained with the normal prosthesis and 27.69 (SD = 14.97) with the VASS. This difference was not statistically significant. On the Houghton Scale, patients scored 9.31 (SD = 1.62) without the VASS and 9.88 (SD = 1.78) with the VASS. This difference was not statistically significant.
The results for the subgroups with MFCL-2 or MFCL-3 mobility grades are given in Table 1. It is worth drawing attention to the fact that the MFCL-3 patients are the ones who experienced a statistically significant improvement in all measures of balance, transfers, and gait, as well as on the LCI. The MFCL-2 patients experienced a statistically significant and clinically relevant improvement in the risk of falling and the use of the prosthesis, and it is worth mentioning that one of them was only able to complete the 6MWT when using a VASS.
Summary of subgroup results for MFCL-2 and MFCL-3 patients.
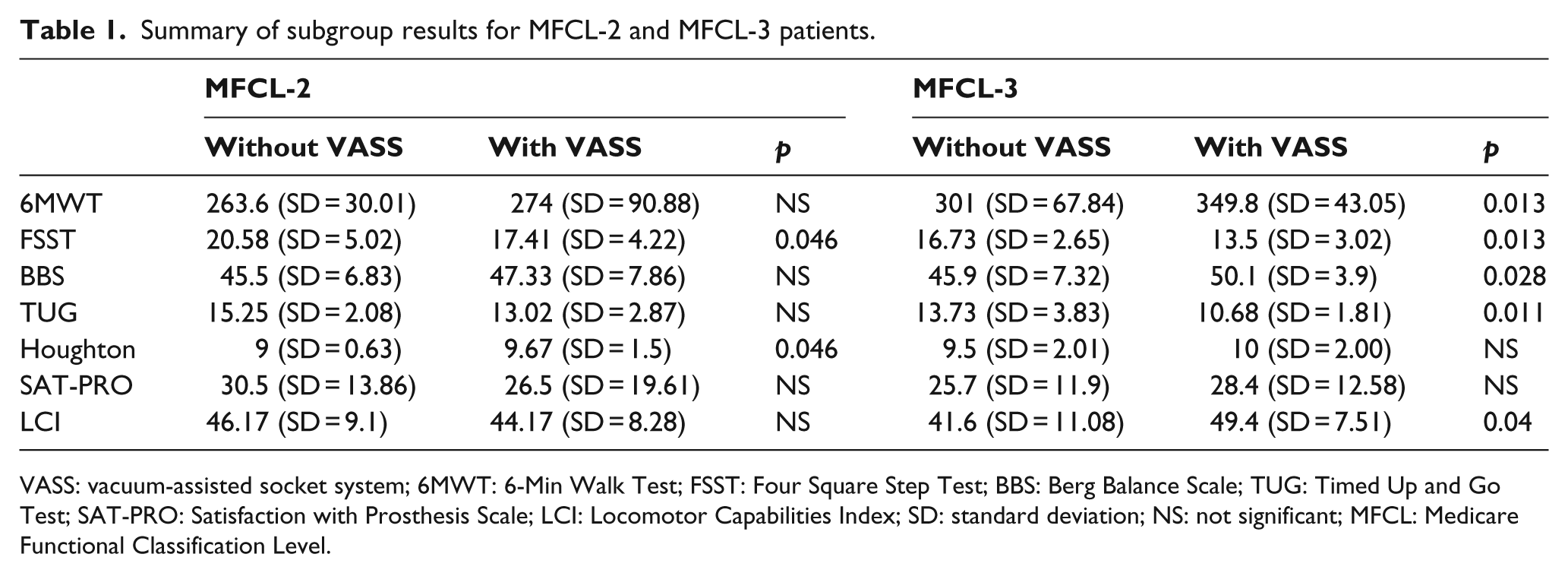
VASS: vacuum-assisted socket system; 6MWT: 6-Min Walk Test; FSST: Four Square Step Test; BBS: Berg Balance Scale; TUG: Timed Up and Go Test; SAT-PRO: Satisfaction with Prosthesis Scale; LCI: Locomotor Capabilities Index; SD: standard deviation; NS: not significant; MFCL: Medicare Functional Classification Level.
Regarding complications, the appearance of blisters was observed in three patients. All of them had a MFCL-2 mobility grade. The installation of an additional distal valve allowed the blisters to resolve. It also facilitated the use of the VASS in these patients with lower activity levels.
Discussion
Our results indicate that VASSs are useful for improving balance, gait, and transfers in patients over 50 years old with a dysvascular transtibial amputation. There are various studies on the effect of VASSs on the skin, wound healing, and residual limb volume, but the authors are not aware of the studies which have assessed the effects of these devices on balance, functionality, or patient satisfaction.
Authors such as Gerschutz et al., 18 Brunelli et al., 19 and Hoskins et al. 20 claim that these systems can not only prevent cutaneous problems but also accelerate the healing process. Others such as Klute et al. 6 and Gerschutz et al. 21 have shown that the use of a vacuum suspension as opposed to a pin-type suspension improved the adaptation to the socket, decreased pistoning, and kept residual limb volume constant. Beil et al. 22 performed a study using a vacuum system that succeeded in avoiding loss of residual limb volume in the socket during the day, increasing the negative pressure generated in the socket interior during the swing phase. These results were confirmed by Goswami et al. 23 in 2003 with no observation of the appearance of pain or cutaneous erythema secondary to the vacuum system. All of these results may indicate an increase in functional capacity, but the authors have only noted one study which evaluates the effect of a VASS on mobility. Ferraro 24 concluded that the probability of falls in the future decreased in her patients when they used a socket including a VASS. This group used the Activities-Specific and Balance Confidence (ABC) Scale which is a self-administered questionnaire considered reliable in amputees. Its results are considered to be related to patient mobility. Overall, these data are in line with those found by our group in a preliminary study. 25
Our study included objective measurements of function such as balance, transfers, and ambulation and subjective evaluations of the patients in terms of mobility, satisfaction, and the use of the prosthesis. Even though the results are based on a small sample size, the overall improvement in function is remarkable and significant for the group of patients with higher activity levels (MFCL-3).
Results obtained in the 6MWT stand out because the improvement is significant when using the VASS. The subgroup of MFCL-3 individuals presents a significant improvement with an average increase of 48.8 m when using the VASS. This result is larger than the 45 m which has been described by Resnik and Borgia. 26 as the minimal detectable change (MDC) in this test. For patients with higher activity levels, the improvement on the TUG is also significant. It took an average of 3.05 s less to perform the test when using the VASS. The size of this difference is very close to the MDC of 3.6 s as reported for transtibial amputees by Resnik and Borgia.27
Regarding the subjective evaluation of the patients’ use of the VASS, only the LCI as a functional self-reported measure demonstrated an improved score in patients with higher activity levels when using the VASS. This finding is consistent with the results of our study’s objective functional tests as well as the results of Ferraro. 25
It is also worth noting that this sample had high initial scores which reflect a previously medium to high level of use and satisfaction with the prosthesis as well as with the patients’ motor capabilities. Klute et al. 6 also found that despite obtaining a better adaptation to the socket when using a vacuum system, patients reported worsened condition of the residual limb, of ambulation, and their own frustration (as measured using the Prosthesis Evaluation Questionnaire). In concordance with these authors, it is likely that some patients need more time to adapt to the use of a new device than was provided in the study, despite the fact that the use of a VASS does not require specific training. The differences in sample size, activity level, and prior satisfaction of patients included in each study may be factors which influence the differences in these results.
In our work, the results obtained for patients with MFCL-2 mobility grade show differences which imply a trend of clinical improvement (in balance, transfers, and ambulation), but only the results of the FSST and the Houghton Scale reached statistical significance. This may be due to an insufficient sample size (six patients with MFCL-2 mobility grade). Since they are patients with less physical capabilities, they may need more time to adapt to and use the device in order to demonstrate objective and subjective changes. The activity level may also be related to the appearance of blisters due to the use of the device which were only observed in MFCL-2 patients.
The authors believe that patients with low activity levels (MFCL-2) spend more time sitting. The pull produced by the weight of the prosthesis while seated may allow air to enter the socket interior such that, upon standing and activating the VASS, friction may be produced, thus causing injury to the skin. Ferraro 25 also considered the presence of air in the socket as a possible mechanism of injury to the skin of the residual limb in patients who used a VASS. In our sample, an additional distal valve was installed that allowed the entrance of air while seated, thus avoiding axial pull. It also allowed the VASS to be activated once standing, facilitating the expulsion of air and the proper fit in the socket. The installation of an additional distal valve in the socket resolved the appearance of blisters in our sample, creating a solution to be considered for patients with lower activity levels. The VASS with the mechanical pump requires a minimum amount of activity to maintain the level of vacuum. If the patient does not walk enough, the vacuum loses power and the socket gets loose which promotes pistoning and skin irritation. This problem could be fixed by an electronic pump that does not depend on walking to produce the vacuum. That should be further studied in the future.
We believe that the results of this study are clinically meaningful since the use of a VASS in patients with characteristics comparable to those of our study sample may be sufficiently beneficial for the rehabilitation physician to consider this device when prescribing a prosthesis. The sample size is one of the limitations of this study. Since the significance level for some variables is p < 0.05, a larger sample would allow confirmation of some of this study’s results. Other limitation is that a third measurement with the previous prosthesis is missing, but all the participants except one refused to use their previous socket again because of the subjective benefit of the new socket including the VASS. We also decided to make a copy of their usual socket to adapt the VASS for the second measurement in order to keep their previous prosthesis intact, but the copy of the usual socket could have been used for the whole study. We believe that more studies should be performed in order to show the effects of a VASS in transtibial amputees with the goal of allowing recommendations to be made based on residual limb size and the patient’s overall mobility.
Conclusion
In conclusion, the Harmony® P2 & HD is a useful device in dysvascular transtibial amputees over 50 years of age. In our study, the use of VASS improved balance, gait, and transfers in patients with MFCL-3 mobility grade and balance and prosthesis use in patients with MFCL-2 activity level. In patients with a lower activity level, the use of an additional distal valve in the socket should be considered.
Footnotes
Author contributions
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.