
Abstract
Stair walking relies on concentric contraction of the ankle plantarflexor and knee extensor muscles, which are either absent or weakened in transtibial amputees. As a result the risk of falling is increased in this population. The aim of this study was to compare the gait patterns of transtibial amputee fallers and non-fallers during stair ascent. Eleven participants (fallers = 6; non-fallers = 5) walked along a 3-m walkway and ascended a three-step staircase with handrails, at their self-selected pace, while three-dimensional kinematic data were collected from the lower limbs. A force plate was embedded into the first step and kinetic data were measured for the intact lead limb only. The fallers walked significantly faster (p = 0.00) and exhibited less hip flexion (p = 0.05) and less anterior pelvic tilt (p = 0.04) compared to the non-fallers. The fallers had significantly greater first and second peak vertical ground reaction force (GRF) on the intact limb than the non-fallers (p = 0.05 and p = 0.01, respectively) contributing to the significantly larger ankle (p = 0.02) and hip moments (p = 0.04). These findings suggested the amputee non-fallers performed mechanically demanding tasks more cautiously. Two of the participants self-selected a ‘step to’ gait pattem, ascending one step at a time. This may be considered a compensatory mechanism for the lack of ankle mobility and functional muscle performance in these two transtibial amputees.
Introduction
Stairs are the most common form of obstacles encountered during everyday living. Stair walking is recognized as a more challenging daily activity than level walking 1,4 and falls often occur during this activity. 3 Stair ascent relies on concentric muscle power, particularly from the ankle plantarflexors and knee extensors of the stance limb, as kinetic energy is converted into gravitational potential energy. During stair ascent, the lead leg performs the greatest effort in the safe negotiation from one step to the next. The quadricep muscles play
an important role in maintaining the body upright, particularly during the single support mid-stance pull-up phase. 2
Young healthy persons can accomplish the rhythmic task of walking up stairs with relative ease. However, the neuromechanical characteristics of level gait in transtibial amputees suggest that this group of individuals may experience greater difficulties during stair ascent. In transtibial amputees, the ankle plantarflexors are absent and the knee musculature on the prosthetic side, especially the extensors, is weakened. 5 While the prosthetic foot may provide the necessary structural support, it does not allow active plantarflexion. Stair negotiation places greater functional demands on the prosthesis 6 and moves the lower limb joints through a greater range of motion (ROM) than level walking. 7 Difficulties with stair ascent and descent in transtibial amputees have been associated with a slower velocity and more asymmetrical gait patterns. 8 Therefore, stair walking is likely to highlight limiting impairments that affect safe locomotion, and these findings would have important implications for improving function in amputees.
Lower limb amputees are at an increased risk of falls compared to age-matched, able-bodied individuals. 9 The biomechanical differences between young and older adults and fallers and non-fallers have been well documented in able-bodied participants during level walking 10,11 and between young and older subjects in stair walking. 3, 4,12,13 However, little research has investigated differences in lower limb amputees. In a previous study, we reported that transtibial amputee fallers had significantly larger load rates on the prosthetic side and altered joint mechanics during the transition from double to single support compared to the non-fallers. 14 Given that stair walking is a more mechanically difficult task than level walking, it is likely that biomechanical differences would also exist between amputee fallers and non-fallers, although this has not yet been investigated. The aim of this study was to compare the gait patterns of fallers and non-fallers during stair ascent in transtibial amputees. Reduced joint range of motion has been linked with a risk of falling in older people. 10,11 Therefore, it was hypothesized that amputee fallers would exhibit decreased joint mobility bilaterally in the ankle, knee and hip joints compared to the non-fallers. A second hypothesis was that amputee fallers would exhibit reduced joint kinetics, especially at the knee and hip, compared to the non-fallers. This was based on the findings that the knee extensors perform much of the work during stair ascent 4 and that transtibial amputees rely on the hip extensor muscles on the prosthetic side during the weight acceptance and pull-up phases. 15
Methods
Participants
Eleven transtibial amputees were recruited from the local Artificial Limb Unit over a four-month period. Inclusion criteria stipulated participants must have worn their prosthesis on a daily basis without experiencing pain. They must have been able to ascend stairs independently without walking aids, although the use of handrails was permitted. Participants were classified into either the (n = 5) non-faller (Mean ±; SD age: 57 ± 21 yrs; height 170 ±; 16 cm; mass 74 ±; 19 kg; time since amputation 10.6 ±; 12.3 years) or (n = 6) faller (age: 56 ±; 13 yrs; height 178 ±; 12 cm; mass 78 ±; 13 kg; time since amputation 3.5 ±; 4.3 years) groups based on their falls history in the nine-month period leading up to testing. There were no significant differences between the two groups on these characteristics. All the falls occurred whilst performing daily activities: two participants reported falling during stair ascent; one person fell during stair descent; two fell when
walking on a slope; and one person fell as a result of a trip on level surface. The majority of participants (n = 4 faller and n = 3 non-faller) wore a Mulitflex Ankle (Blatchford, UK) prosthesis, one faller and one non-faller walked with a Vari-Flex (Ossur, UK) prosthesis, one faller wore a Ceterus (Ossur, UK) foot, and one non-faller used a Dynamic (Otto Bock, Germany) foot. Participants did not experience pain whilst standing or walking and reported general satisfaction with their prosthesis, suggesting that prosthetic alignment was adequate. 16,17 The study was approved by the South Humber NHS Research Ethics Committee (REC number: 05/Q1105/68). All participants gave written informed consent to take part in this study.
Staircase
A three-step wooden staircase was built for this study. The steps were 80 cm wide, with a rise of 20 cm, a tread of 25 cm, and a final tread of 80 cm. One Kistler force plate (model 9286AA Kistler GmbH, Winterthur, Switzerland) with built-in charge amplifiers was positioned flush into the bottom step, which was independent from the remainder of the structure. Wooden handrails were 50 cm high, attached to the main structure but not to the bottom step which housed the force plate (Figure 1). The staircase dimensions conformed to stair designs in public buildings and the number of steps was the same as that which has been used previously in stair biomechanics studies. 1,18,19 The structure was on wheels which could be locked securely into place.
Protocol
Three-dimensional kinematic and kinetic values were obtained using Qualisys Track Manager software (Qualisys, Gothenburg, Sweden) while the participants walked along a level walkway and proceeded to climb the staircase. Ten ProReflex MCU1000 cameras (Qualisys, Gothenburg, Sweden) captured 3D marker coordinate data at 100 Hz and were synchronized with the force plate that sampled at 500 Hz. The motion capture system was calibrated using a 300 mm calibration wand and L-frame reference object identifying the lab origin.
All participants completed the test wearing their own flat walking shoes which were securely fastened with laces. Details of the six-degrees-of-freedom marker set-up for static and dynamic trials have been explained previously. 14 Participants were asked to walk along a 3-m walkway in the laboratory and then climb the three-step staircase at their preferred walking speed. Participants completed a total of 12 walk trials and were allowed to rest when required. The ground reaction force (GRF) data were collected for the intact lead limb only. Participants were not instructed to stop on the last step, but to continue walking until they reached the handrail. The final tread of 80 cm allowed participants to take at least one level step after having climbed the three-step staircase to avoid the effects of slowing down.
Data analysis
Kinematic and kinetic data were processed and analyzed as described before 14 and normalized to the gait cycle starting with initial foot contact. The data were first examined for lead limb preference by determining if participants favoured either the prosthetic or the intact limb when stepping onto the first step of the staircase. Nine of 11 amputee participants displayed a clear intact lead limb preference (always led with this limb) while two participants
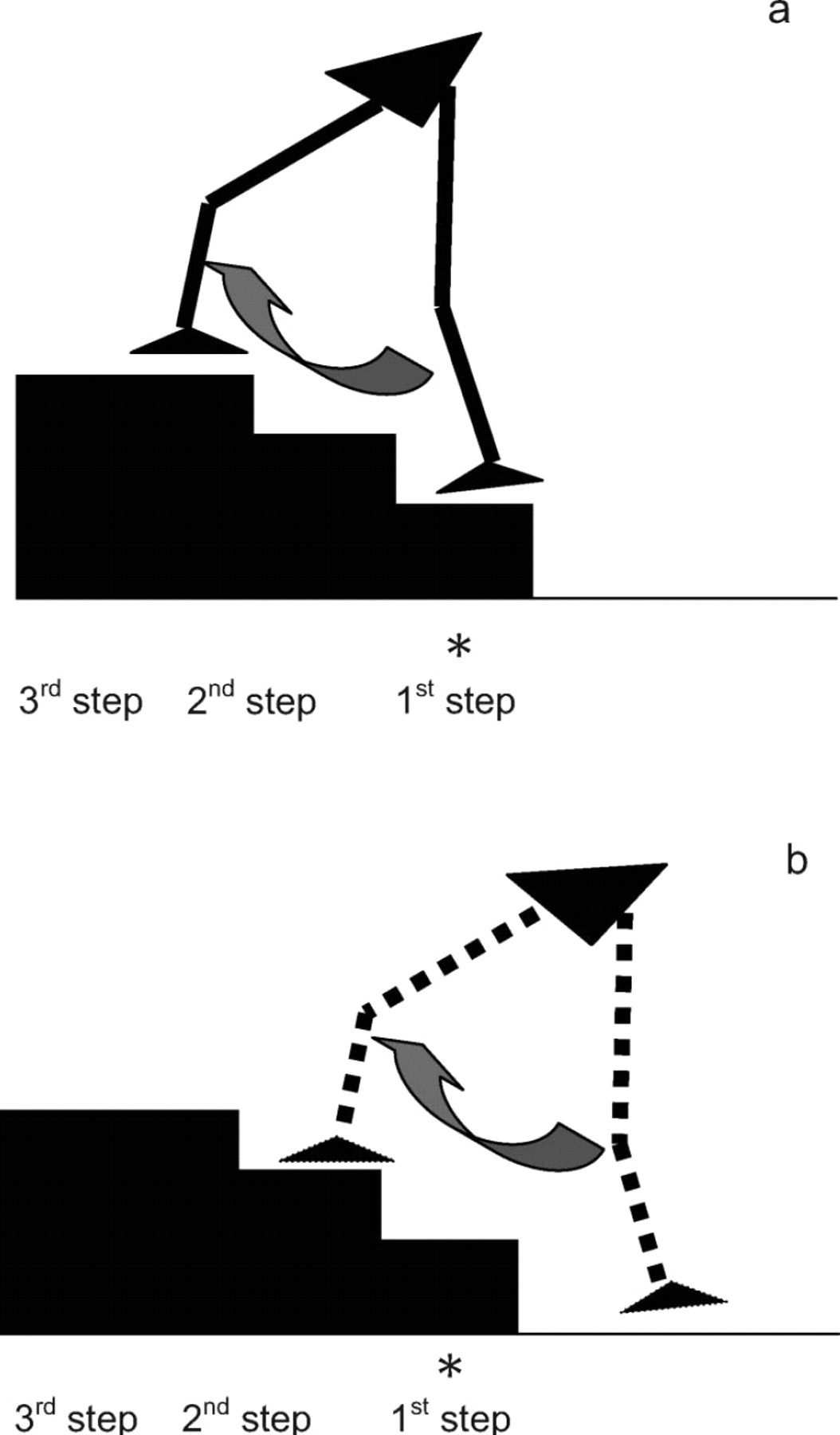
The three-step staircase used in the current study: (a) Intact lead limb (black solid line) during progression from the first to the third step; (b) Prosthetic trail limb (black dashed line) during progression from the floor to the second step. Both limbs travel the same vertical distance. Each gait cycle is initiated and terminated with foot contact. The stance phase on the first step makes up approximately 65% of the gait cycle for the intact lead limb (a); while 56% of the gait cycle is spent with the prosthetic trial limb on the floor (b). ∗Indicates the position of the force plate in the first step. The handrails are not illustrated.
did not exhibit a clear preference and lead with either the prosthetic or intact limb. However, for the purpose of this analysis, the intact limb was selected as the lead limb and the prosthetic limb as the trail limb for all subjects.
Variables
The gait variables that were selected for analysis included temporal-spatial parameters such as the average resultant walking speed (m/s) for each step and support time (stance phase %). In order to compare joint mobility in the sagittal plane, peak joint kinematics (°) and ROM for the ankle, knee and hip were analyzed bilaterally. Specifically, peak hip extension, knee flexion and ankle dorsiflexion values were examined during the stance phase; peak hip and knee flexion and ankle plantarflexion and dorsiflexion were analyzed in swing. Anterior pelvic tilt was reported during stance and swing. Kinematic data were not compared between limbs, but only across groups. Therefore, temporal-spatial and kinematic data for the intact lead limb were analyzed from initial contact on the first step to initial contact on the
third step; data for the prosthetic trail limb were analyzed from initial contact on the floor to initial contact on the second step.
Kinetic data were measured for the intact lead limb while it was in stance on the first step. The GRF variables included peak anterior-posterior braking, propulsion and vertical forces (N/kg). McFadyen and Winter (1988) identified three sub-phases during stance (weight acceptance, pull-up and forward continuance) and two sub-phases during swing (foot clearance and foot placement). 2 The Fz1 vertical force was calculated during the weight acceptance phase (loading) and the Fz3 force in the forward continuance phase (pre-swing). Fz2 represented the minimum vertical force during the pull-up phase (mid-stance). Load and decay rates (N/kg/s) were computed from the vertical force vs. time curve. Load rate represented the positive slope from initial contact until Fz1; decay rate was the negative slope from Fz3 until toe off. As it was hypothesized the joint kinetics would be reduced in the fallers, peak joint moments (Nm/kg) and power bursts (W/kg) for each mechanical joint phase were investigated in the sagittal plane. 2
Statistical analysis
Two of the amputee fallers, who had an intact lead limb preference, self-selected a ‘step to’ walking pattern by climbing one step at a time. Therefore, statistical analysis was only carried out on nine of the participants: four fallers and five non-fallers. In order to ascertain whether lower limb kinematic and kinetic differences existed between the two groups during stair ascent, an independent sample t-test was conducted on the specific variables. Levene' test for equality of variances was used to assess homogeneity. In the instance of violation of homogeneity of variance the corrected t-value was used. SPSS v 15.0 (SPSS Inc., Chicago, IL, USA) for Windows was used for statistical analysis. The alpha level for significance was set a priori at 0.05.
Results
Kinematic variables
Walking speed, stance phase (%) and peak joint kinematics are presented in Table I. The amputee fallers walked significantly faster with the lead (t= − 4.25; p = 0.00) and trail (t= −3.31; p = 0.01) limbs compared to the non-fallers. There were no differences in stance duration between the two groups.
Although the hip on the intact limb never reached full extension, the fallers displayed significantly less hip flexion (t = 2.28; p = 0.05) and less anterior pelvic tilt (t = 2.45; p = 0.04) during the forward continuance phase compared to the non-fallers. The fallers exhibited greater peak knee flexion during swing from the first to the third step with the intact limb (t= - 2.75; p = 0.03). On the prosthetic trail limb, the fallers displayed 10°; greater ROM at the knee joint and this difference was significant (t=−2.31; p = 0.05).
GRF kinetics
The GRF data for the intact lead limb are presented in Table II. There were no significant differences in either braking or propulsive forces. However, the fallers recorded significantly larger peak vertical forces Fz1 and Fz3 (t= −2.69; p = 0.05 and t=−4.94; p = 0.00,
Mean (SD) temporal-spatial, peak joint kinematic values and joint range of motion (ROM) for the non-fallers; fallers and ‘step to’ group during stair ascent. Data are presented and compared according to lead (intact) and trail (prosthetic) limbs.
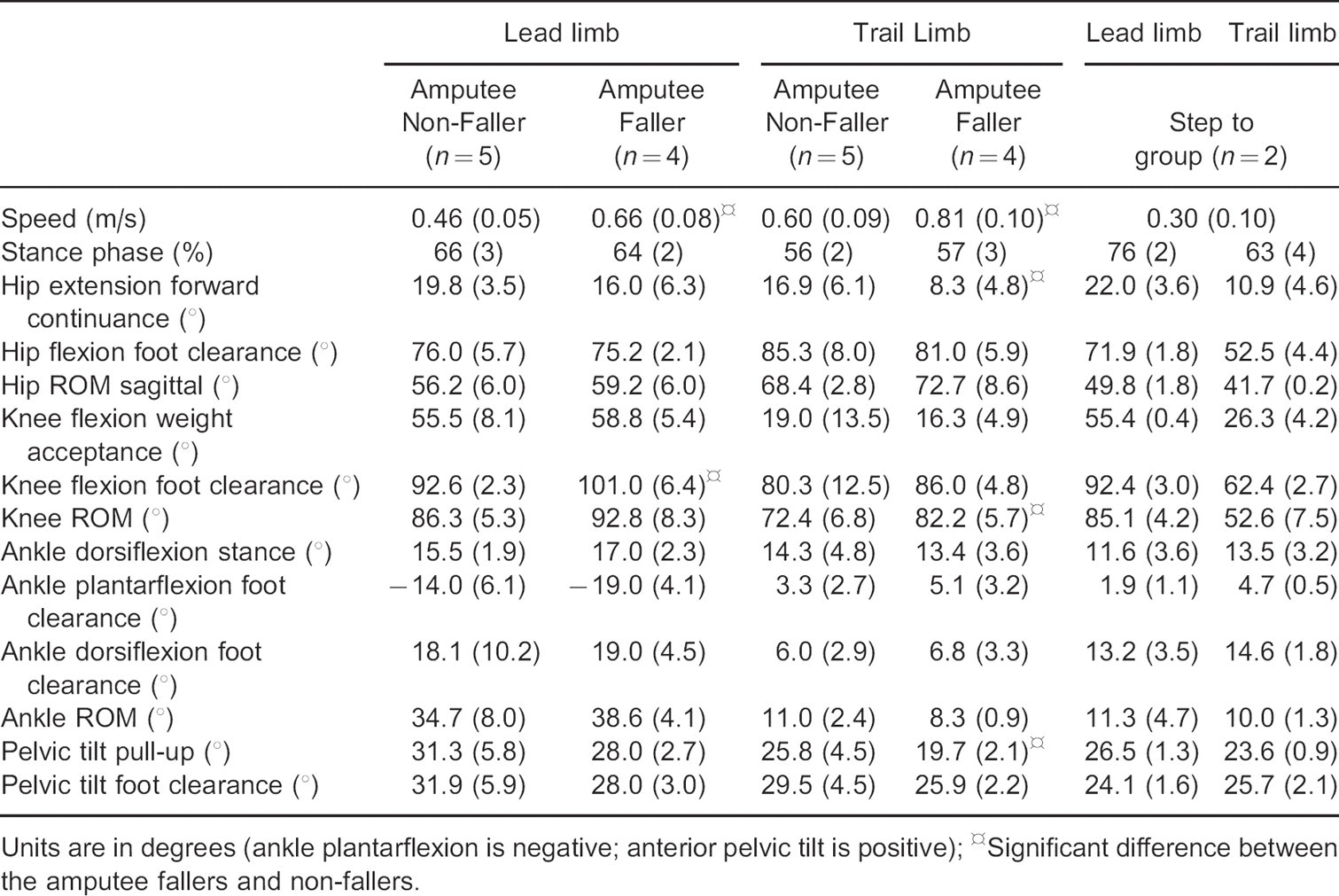
Significant difference between the amputee fallers and non-fallers.
Units are in degrees (ankle plantarflexion is negative; anterior pelvic tilt is positive)
Mean (SD) peak force (N/kg), load and decay rates (N/kg/s) and joint moments (Nm/kg) of the intact lead limb only for the non-fallers and fallers.
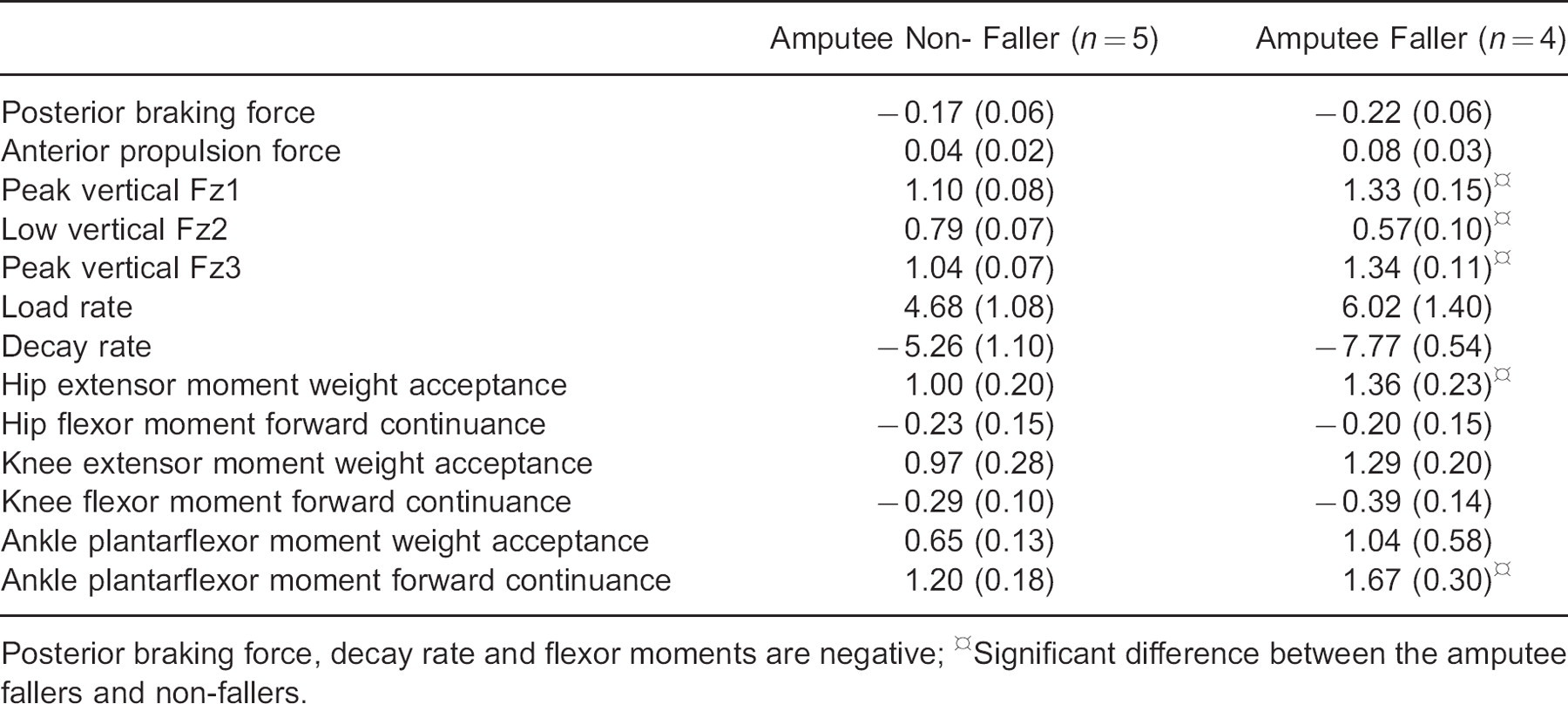
Significant difference between the amputee fallers and non-fallers.
Posterior braking force, decay rate and flexor moments are negative
respectively) and significantly lower vertical force Fz2 (t =4.07; p = 0.01) compared to the non-fallers. There were no differences in load rate, but the fallers exhibited significantly greater decay rate compared to the non-fallers (t=4.14; p=0.00)
Joint kinetics
Average joint moment profiles are shown in Figure 2 and peak values in Table II. During the weight acceptance phase, the amputee fallers had significantly larger hip moments(t=- 2.49; p = 0.04) on the intact lead limb. The fallers also exhibited a significantly larger ankle plantarflexor moment(t=- 2.94; p = 0.02) in the forward continuance phase.
Average joint power profiles are displayed in Figure 3 and peak values in Table III. There were no significant differences between the fallers and non-fallers at the hip or ankle joints. However, the amputee fallers had bigger power absorption bursts at the intact knee during the swing phase from the first to the third step. Specifically, they had a significantly larger K3 power burst (t = 4.08; p = 0.01) in the foot clearance phase and larger K4 burst in the foot placement phase probably related to speed.
Step to group
Temporal-spatial and peak kinematic values for the ‘step to’ group are displayed in Table I. Adopting a ‘step to’ stair ascent pattern was particularly reflected in the slow walking speed, which was 35–50% slower than the slowest speeds for the non-fallers and fallers, respectively. Hip ROM for the prosthetic limb was reduced by approximately 40%. Knee
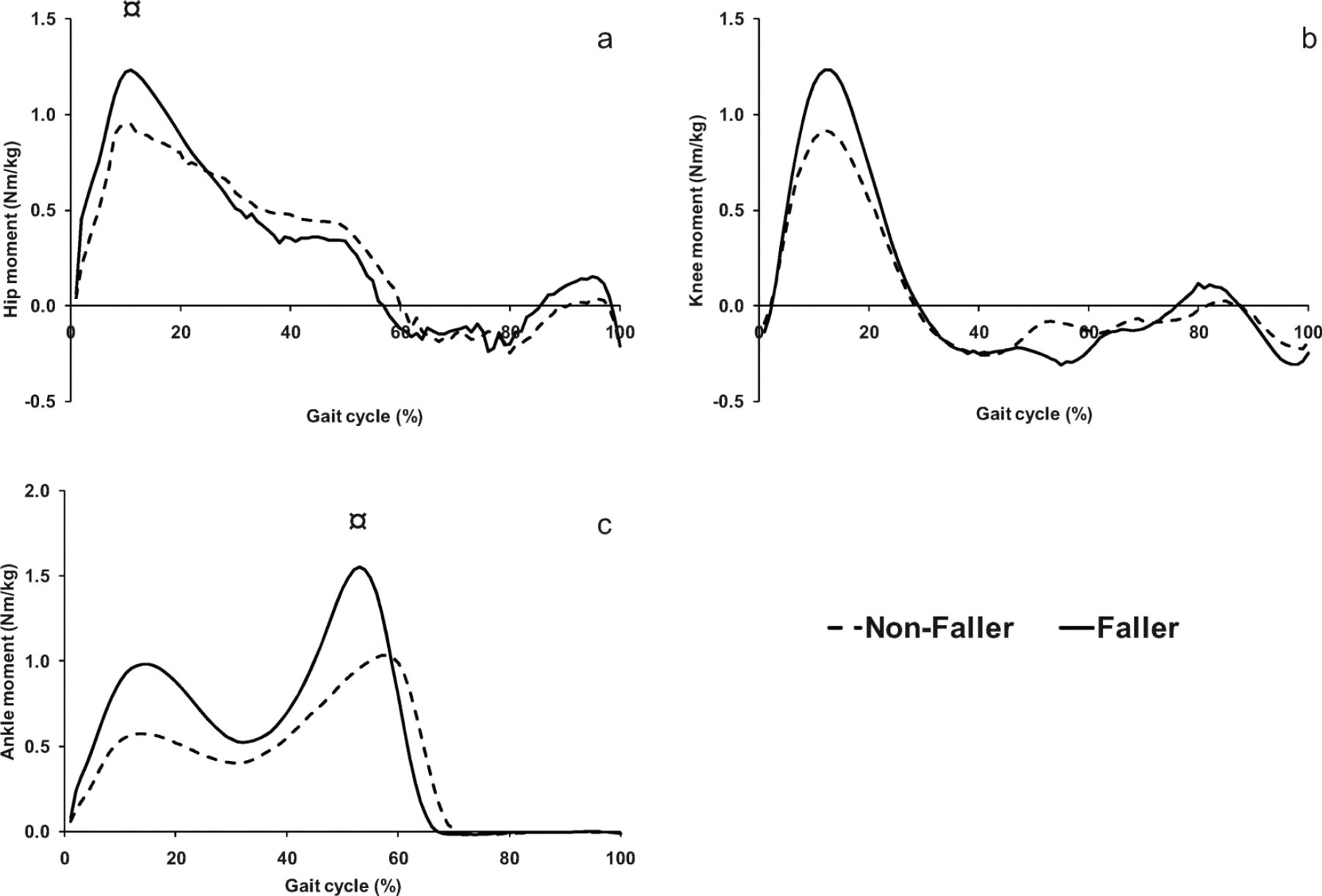
Average hip (a), knee (b) and ankle (c) internal joint moments (Nm/kg) of the intact lead limb in the non-fallers (dashed black line) and fallers (solid black line) normalized to the gait cycle starting with initial foot contact until the next foot contact. Data are presented in the sagittal plane. The stance phase on the first step makes up approximately 65% of the gait cycle. HSignificant difference between the amputee fallers and non-fallers.

Average mechanical joint power (W/kg) bursts for the hip (a), knee (b) and ankle (c) of the intact lead limb in the non-fallers (dashed black line) and fallers (solid black line) normalized to the gait cycle starting with initial foot contact. Data are presented in the sagittal plane. The stance phase on the first step makes up approximately 65% of the gait cycle. ¤Significant difference between the amputee fallers and non-fallers.
Mean (SD) peak joint powers (W/kg) of the intact lead limb only for the non-fallers and fallers.
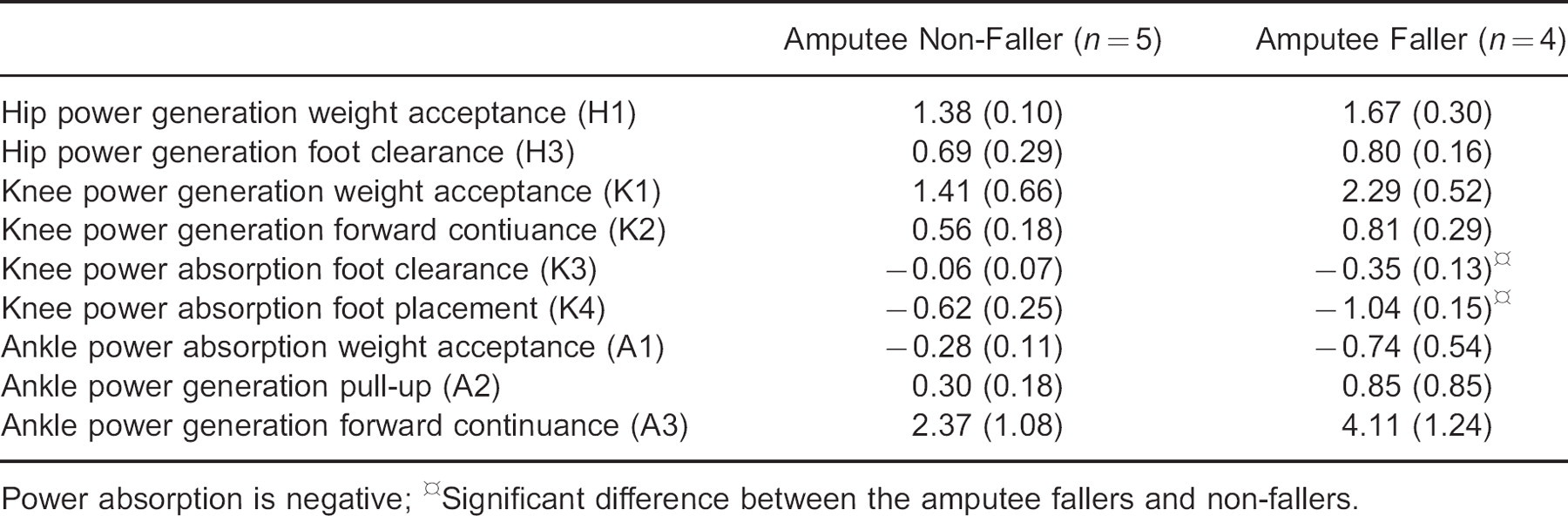
Significant difference between the amputee fallers and non-fallers.
Power absorption is negative
ROM of the prosthetic trail limb was 27% and 36% less than in the non-fallers and fallers, respectively. The ‘step to’ group did not display ankle plantarflexion on either the intact or prosthetic foot. The ankle ROM of the intact limb was 67% and 71% smaller compared to the non-fallers and fallers, respectively.
Discussion
More mechanically challenging tasks than level walking, such as stair ascent, are more likely to highlight kinematic and kinetic differences between amputee fallers and non-fallers. In a previous study, we reported no significant differences in walking speed between amputee fallers and non-fallers during level walking 14 whereas in the current study the amputee fallers were significantly faster. Another previous study reported walking speeds of 0.49 m/s on a four-step staircase in transtibial amputees. 8 The current findings demonstrate that the non-fallers walked at similar speeds to other community-dwelling transtibial amputees who were able to walk without assistive devices. The non-fallers may perform more demanding tasks more cautiously as a compensatory mechanism for the lack of ankle mobility and loss of power generation from the absent plantarflexor muscles. Conversely, the fallers walked faster and this could predispose them towards falling because they may be less likely to recover successfully from a trip or stumble on stairs when walking at markedly higher speeds. Functional muscle weakness in the single supporting limb, that might cause the limb to collapse, is another factor that may lead to a fall, particularly during the pull-up phase in stair ascent.
Joint kinematics
The ankle joint plays an integral role in stair walking, especially during the forward continuance phase when it is responsible for lifting the body. 2 It was not surprising that no differences were found between the amputee groups, as the prosthetic ankle did not move into plantarflexion and ROM is limited and disadvantaged by the prosthetic components. 8 Contrary to the first hypothesis, that anticipated reduced joint mobility in the fallers, they actually had a significantly larger knee ROM on the prosthetic trail limb than the non-fallers. Since there is no published literature to date on the kinematic differences between amputee fallers and non-fallers during stair walking, it is not clear if the greater ROM was a compensatory, more cautious strategy possibly as a result of a previous fall. However, it is not possible to differentiate the cause from the effect without a longitudinal design.
Compared to level walking, the hip did not reach full extension for either of the groups (e.g., hip extension angles remained positive). Hip flexion is influenced by anterior pelvic tilt and trunk flexion. Although trunk flexion was not measured, the results revealed significantly more anterior pelvic tilt and less hip extension in the non-fallers. Greater forward trunk lean could be related to subjects looking down at the feet. 20 Indeed, this was quite possible among the amputee groups, who have lost the proprioceptive feedback from the prosthetic ankle and foot, and may rely on visual input for controlling foot position and avoiding a trip during prosthetic swing.
All of the amputee non-fallers used the handrail to some level, whereas several amputee fallers did so only sporadically. Reeves et al. (2008) reported that the use of handrails had little effect on joint kinematics but improved dynamic postural stability. 4 This may therefore be considered a good adaptive strategy as it would provide an additional point of contact during the more vulnerable transition from weight acceptance to the pull-up (single support) phase on the prosthetic side.
GRF and joint kinetic data
In the amputee non-fallers, the Fz1 force on the intact limb was very similar to that reported by Schmalz et al. in transtibial amputees (1.16 N/kg). 6 Conversely, the amputee fallers
displayed significantly larger peak forces and reduced mid-stance force, and a larger decay rate on the intact limb compared to the non-fallers. Larger vertical forces experienced in the intact leg were related to the amputee fallers’ significantly faster walking speed and reduced loading on the handrails. This may be considered a risk for falls, especially Fz3 when the prosthetic leg was transitioning into the pull-up phase. The smaller valley peak (Fz2) suggested the prosthetic limb was moving rapidly in swing as the force plate was significantly unloaded during intact single support. 21 This finding highlights the need for strong extensor muscles in the intact limb during pull-up. A larger decay rate on the intact limb indicates the prosthetic limb would have to control larger forces when in single support.
Peak joint moments were consistently higher for the fallers, with values considerably greater than those reported for the intact limb in transtibial amputees during stair ascent. 6 In the current study, the amputee fallers had larger ankle plantarflexor and hip extensor moments most likely reflective of the significantly faster walking speed in this group and reduced handrail use. In the current study, we did not control for speed because it was unrealistic that all participants would have been able to negotiate the stairs safely and comfortably at a pre-determined speed. Further evidence for this was that some participants adopted a very slow, more careful, ‘step to’ strategy.
During stair ascent, joint power profiles showed the distinct power bursts as described previously. 2 Although there were no significant differences in peak ankle joint powers, visual inspection of the power profiles reveals distinctly larger peak values between the two groups (Figure 3c). This could be attributed to the different mechanical characteristics of the participants’ prostheses, since two of the four fallers used prosthetic feet (Vari-Flex and Ceterus, Össur, UK) which offered somewhat higher energy return than the other prosthetic feet, particularly during the forward continuance phase. The significant differences in peak knee power bursts (K3 and K4) support the second hypothesis related to joint kinetics. However, contrary to the hypothesis, the fallers exhibited significantly larger knee powers on the intact limb than the non-fallers. Evidence of the triphasic power bursts at the knee (labelled K2, K3 and K4), 2 together with hip flexor concentric activity (labelled H3), was deemed a positive mechanical characteristic in the fallers and may have implications for amputee rehabilitation.
‘Step to’ group
Transtibial amputees are typically taught to lead with their intact limb during stair ascent because of the greater joint ROM demanded by the lead limb. It is likely the ‘step to’ group adopted this gait pattern because it reduced the mechanical demands on the lower limbs and because of limitations related to the prosthetic components. Considerably less control of the prosthetic ankle was required and it performed below its functional limits. Furthermore the ankle plantarflexor muscles did not need to transport the body such a large vertical distance.
Unfortunately, we could not analyze kinetic data on those people who adopted a compensatory ‘step to’ gait pattern. However, based on the kinematic findings, factors that likely predisposed amputees to use a ‘step to’ pattern were reduced prosthetic ankle ROM, reduced functional strength of the ankle plantarflexors on the intact limb, insufficient knee extensor strength on the prosthetic limb and overall reduced ROM of the knee and hip on the prosthetic side. It is also worth noting that the ‘step to’ group was heavily reliant on handrail support, by performing considerable work with both arms. This would have reflected an effort to reduce the functional strength demands on the extensor muscle groups of the lower limbs, as well as increase the base of support. Individuals with a fear of falling or
poor balance confidence may also adopt this slower and more cautious stair walking strategy.
Some limitations to this study must be acknowledged. It is known that ‘light’ handrail use affects kinetic data to some level by redistributing the joint moments across the ankle and knee joints. 4 Therefore, some caution should be used when interpreting the kinetic results as handrail use varied across subjects. On the other hand, one could argue that the kinetic data would be a true representation of the subjects’ stair walking lower limb biomechanics. Although kinetic and joint power data were not collected for the prosthetic limb, it is anticipated that compensatory mechanisms would be evident between fallers and non-fallers. Further work collecting kinetic data from both limbs over several consecutive steps is warranted. While this study investigated functional muscle performance through the interpretation of joint moments and powers, future studies should undertake muscle strength testing and examine the relationship with falls history. Amputees vary in cause of amputation, age, confounding health comorbidities and type of prosthesis that they wear; therefore, extending these results to the wider amputee population should be approached with caution. Finally, stair descent is another activity of daily living associated with falls and future work investigating biomechanical differences in amputee fallers and non-fallers is recommended.
Conclusion
These results demonstrate that biomechanical differences exist between amputee fallers vs. non-fallers and that these are especially apparent during the transition from double support to prosthetic single support. The amputee fallers exhibited faster walking speed, which resulted in increased GRF and joint moments on the intact limb, whilst the amputee non-fallers appeared to walk more cautiously. Some subjects adopted safer stair walking strategies, such as handrail use and ‘step to’ gait patterns.
Acknowledgements
The authors would like to thank Dr Nick Jayawardhana, Consultant Physician, and Vicki Russell, Prosthetics Services Manager, from the Hull & East Yorkshire NHS Trust Artificial Limb Unit for their assistance in recruiting participants for this study.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.