
Abstract
Background:
Prosthetic alignment is usually unchanged once optimized. However, a previous study indicated that long-distance walking significantly altered gait patterns, suggesting some alignment adjustments after walking are required. This study investigated the effects of alignment changes (by inserting a heel lift) on gait of a transtibial amputee before and after treadmill walking.
Case Description and Methods:
The subject walked, without heel lifts, on a treadmill until perception of fatigue. Gait changes upon heel lifting at the prosthetic side were studied before and after the treadmill walking
Findings and Outcomes:
For this subject before the treadmill walking, heel lifting induced drop-off with increased prosthetic-side knee flexion at mid-stance and pre-swing. The sound limb outreached to stabilize the gait. After the treadmill walking, the same heel lift did not induce drop-off. It reduced the plantar flexor power generation, potentially delaying its fatigue.
Conclusion:
After walking prosthetic-side heel lifting could be beneficial.
Clinical relevance
Many lower-limb amputees have difficulties in long-distance walking due to muscle fatigue. This case study proposes that appropriate alignment changes after some walking potentially relieve fatigue and encourage them to walk longer distances.
Background
Long-distance walking (LDW) is the simplest mode of physical exercises, which benefits the health of lower-limb amputees. 1 However, many lower-limb amputees could not tolerate LDW because they experienced fatigue easily. 2 Muscle fatigue inhibits force generation and shock absorption, 3 alters gait pattern, 4 and reduces the willingness to continue walking. Plantar flexors are more susceptible to fatigue than other muscles in the lower limb,4,5 and their fatigue was suggested to be the main difficulty faced by transtibial amputees when performing LDW. 6
Our previous research (n = 6) indicated that LDW induced significant changes in unilateral transtibial amputees’ gait. 7 After LDW, muscle fatigue that developed in the sound-side plantar flexors reduced the ankle motions. The fatigue could be the result of asymmetric gait patterns, which involved longer stance time and greater ground reaction force at the sound limb.7,8 The reduced sound-side ankle motions were compensated by greater prosthetic-side knee flexion, which facilitated anterior rotation of the prosthetic shank. 7 In current practice, the prosthetic alignment, which refers to spatial relationships between the socket and the prosthetic foot/shoe, would be fixed once optimized by clinicians. However, changes in gait patterns after LDW suggested that some appropriate alignment adjustments after fatigue are required.
Heel lifting alters the alignment of a prosthesis, which rotates the prosthesis with a solid-ankle-cushioned-heel (SACH) foot forward during the stance phase.9,10 This increases prosthetic-side knee flexion, and may have the effects of (1) undesirably excessive knee flexion during late stance, commonly known as drop-off, and (2) favorable reduction of the push-off power of the sound side due to the greater forward momentum of the prosthetic side. The effects could be different at different levels of fatigue. In this study, we investigated the effects of heel lifting on the gait of a transtibial amputee before and after some treadmill walking that induced fatigue.
Case Description and Methods
Subject
A male right-sided transtibial amputee participated in this study with informed consent. He was 47 years old (height = 1.7 m, weight = 74.6 kg), and had 10-years of experience using prostheses with a SACH prosthetic foot. Throughout the experiment, he used his own prosthesis, which was prescribed by a certified prosthetist about 1 year before the experiment. Ethical approval was obtained from the Human Subject Ethic Subcommittee of The Hong Kong Polytechnic University.
Testing protocol
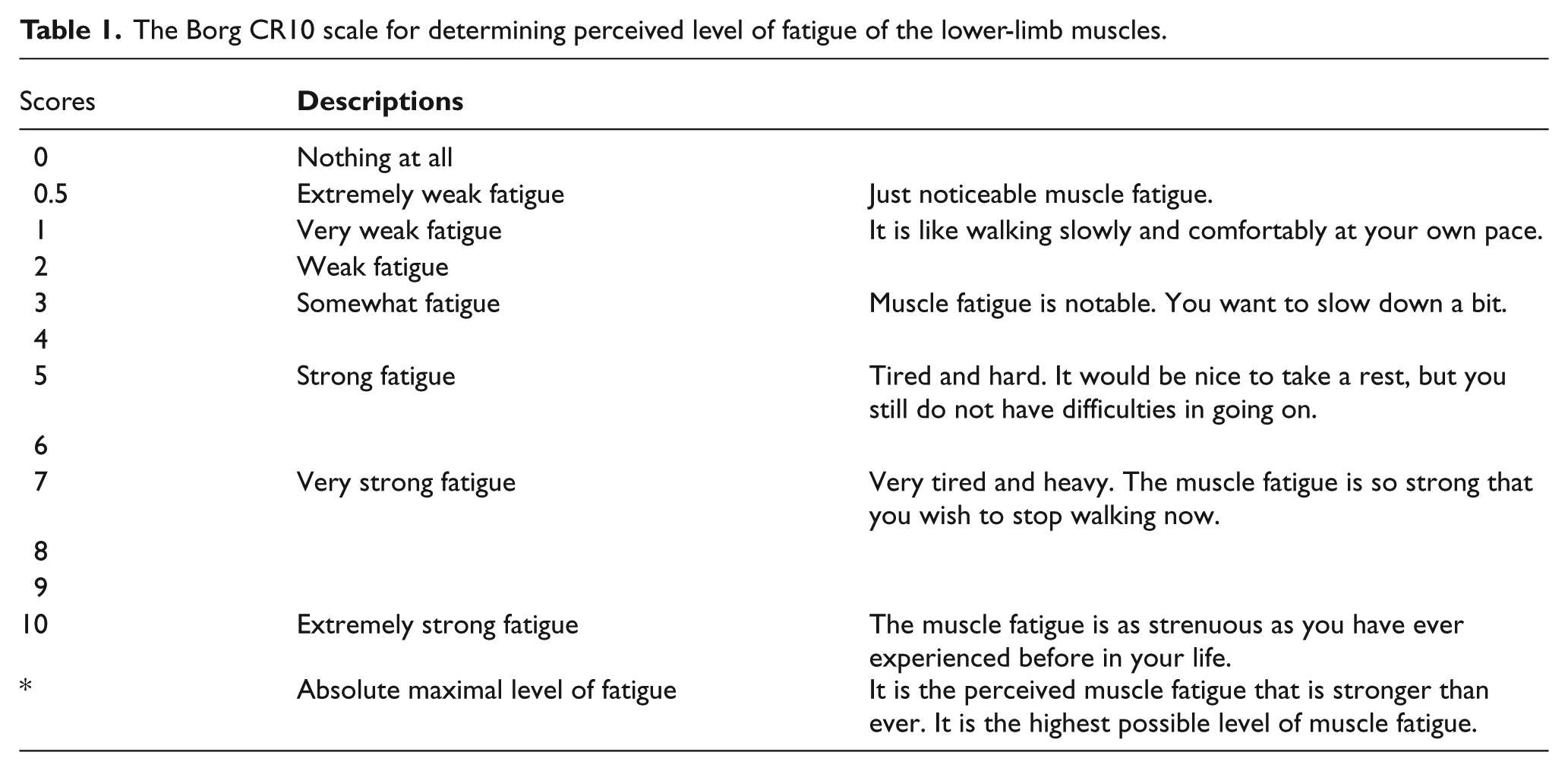
Heel lifting was achieved by inserting a wedge-shaped (peak height: 10 mm) silicon under the heel of the prosthetic foot. It rotated the prosthesis forward by roughly 2.5°. The subject was instructed to walk at a comfortable walking speed continuously with the heel lift for 5 min to get accustomed to this shoe-insert modification, followed by a short break of 2 min. This arrangement was referenced to a previous study. 10 The subject then walked, without heel lifting, at a constant comfortable speed of 1.12 m/s on a level treadmill without using handrails. During the treadmill walking, the subject reported his level of lower-limb muscle fatigue every 2 min by reporting a score based on the Borg CR10 scale 11 (Table 1). A score with decimals and a score below 0.5 were allowed. 11 When the score exceeded 3, which corresponded to “ Somewhat fatigue - need to slow down a bit,” the treadmill walking stopped. The self-reporting of fatigue was instructed before the test, and the subject did not know the treadmill walking would terminate once a score of 3 was reported. The subject walked for 16 min with a total distance of 1075 m.
The Borg CR10 scale for determining perceived level of fatigue of the lower-limb muscles.
The following gait data were collected when the subject walked overground: (1) Just before the treadmill walking (Baseline) without heel lifting, (2) baseline with heel lifting, (3) after the treadmill walking (Fatigued) without heel lifting, and (4) fatigued with heel lifting. Trials were repeated until five samples of successful walking steps, in which the whole foot completely landed within the force plate, were collected. All successful trials were used in analysis.
Apparatus
An eight-camera motion capture system (Vicon, Oxford Metrics) was used with eight MX-F40 cameras (resolution of 4-million pixel and image errors of less than 0.5 mm). Infrared reflective markers were placed bilaterally at the third metatarsal head, heel, lateral and medial malleoli, lateral and medial femoral condyles, greater trochanter, iliac crest, posterior superior iliac spine, and mid-shank and mid-thigh. The markers were attached before the 5-min acclimatization period, and remained attached throughout the experiment. Ground reaction force was measured using two force plates (Advanced Mechanical Technology, Inc.) embedded midway on an 8-m walkway. The kinematic and kinetic data were collected at 200 and 1000 Hz, respectively.
Data analysis
The gait data were analyzed using Visual3D (C-motion, Inc.). The kinematic and kinetic data were low-pass filtered using a fourth-order Butterworth filter with a cutoff frequency of 6 Hz. 12 Walking speed, stance time, step length, ground reaction forces in the anterior (GRFx, propulsive force), posterior (GRFx, braking force), medial-lateral (GRFy), and vertical (GRFz) directions, joint angles, moments and powers of the ankle, knee and hip joints, were obtained. Local peaks and points of interest in kinematic and kinetic data were determined within each gait cycle. All spatial-temporal, kinematic and kinetic quantities were averaged for each successful walking trial. Percentage differences in each gait parameter that compared the presence and absence of heel lifting were calculated at the Baseline and the Fatigued conditions.
Findings and Outcomes
Figures 1 and 2 show the kinematic and kinetic data along the gait cycle. Table 2 lists the changes in all measured gait parameters which were greater than 5% when comparing the absence and presence of heel lifting. The percentage changes in stance time, step length, GRFy, and GRFz were lower than 5%.
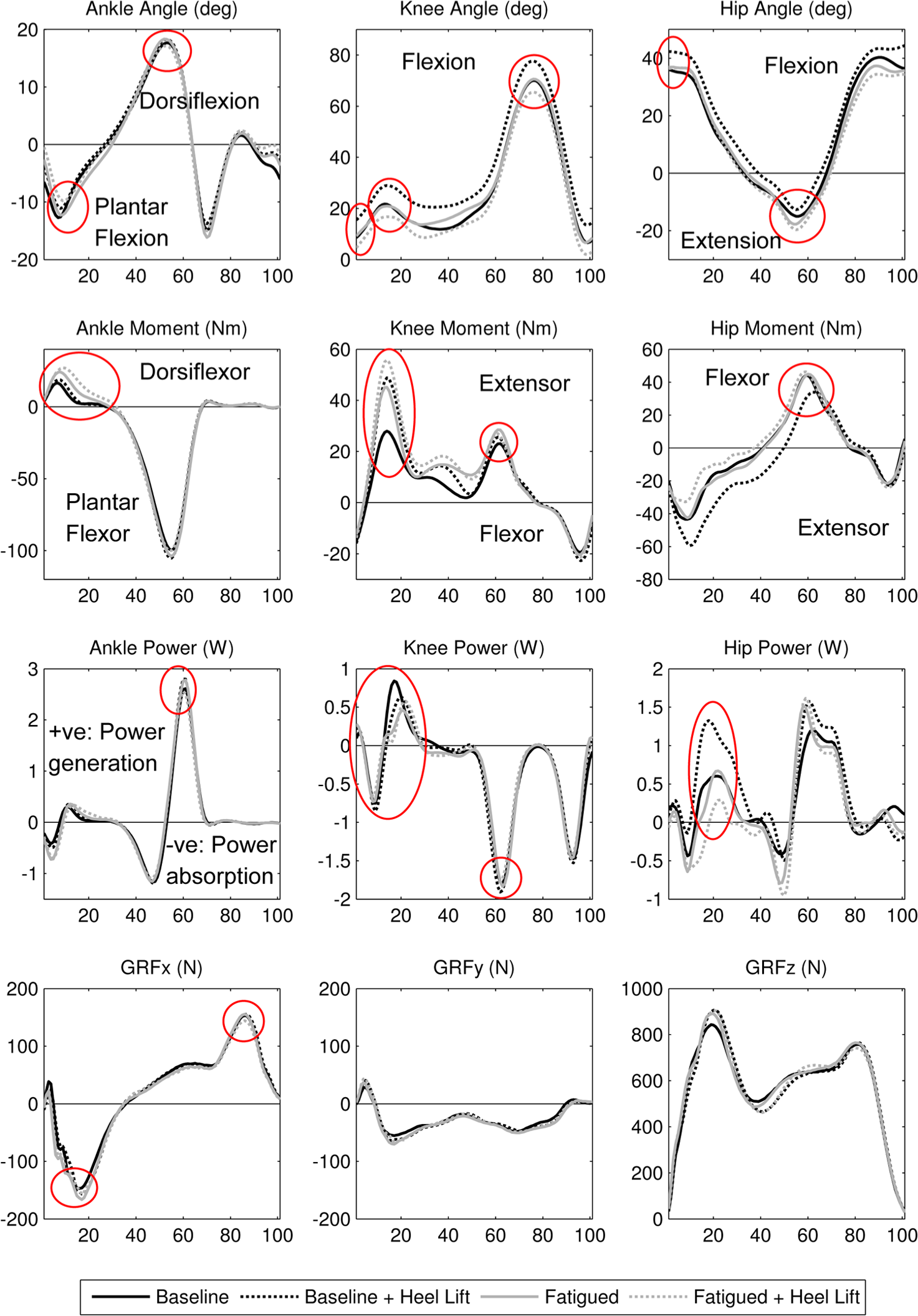
Sound-side joint angles, moments and powers of the ankle, knee, and hip joints in percentage of gait cycle. GRF in percentage of stance phase. A circle indicates that the difference is greater than 5% when comparing with and without a heel lift.
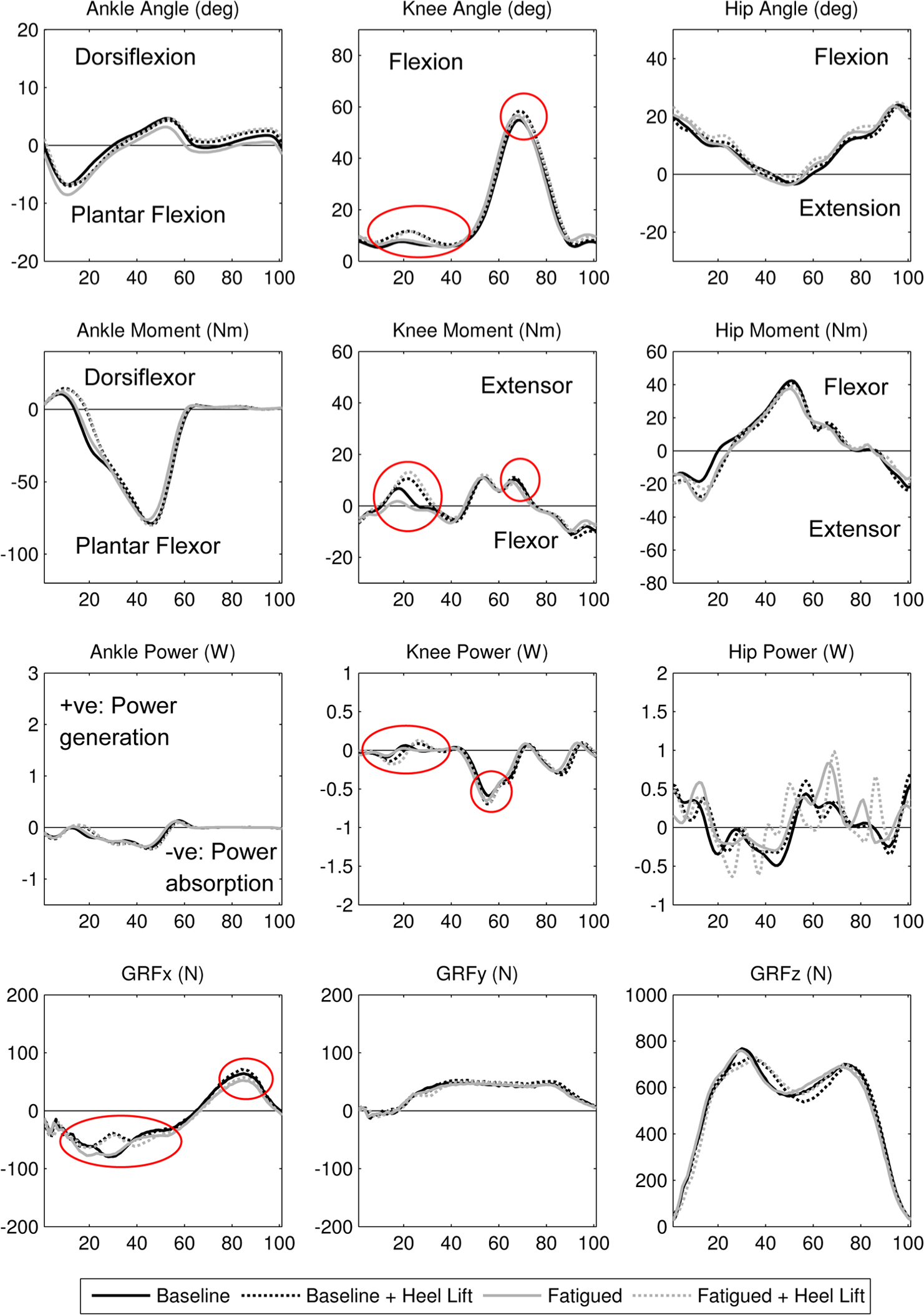
Prosthetic-side joint angles, moments and powers of the ankle, knee, and hip joints in a gait cycle. GRF in percentage of stance phase. A circle indicates that the difference is greater than 5% when comparing with and without a heel lift.
Percentage changes of walking speeds, and kinematic and kinetic gait parameters at peak values.
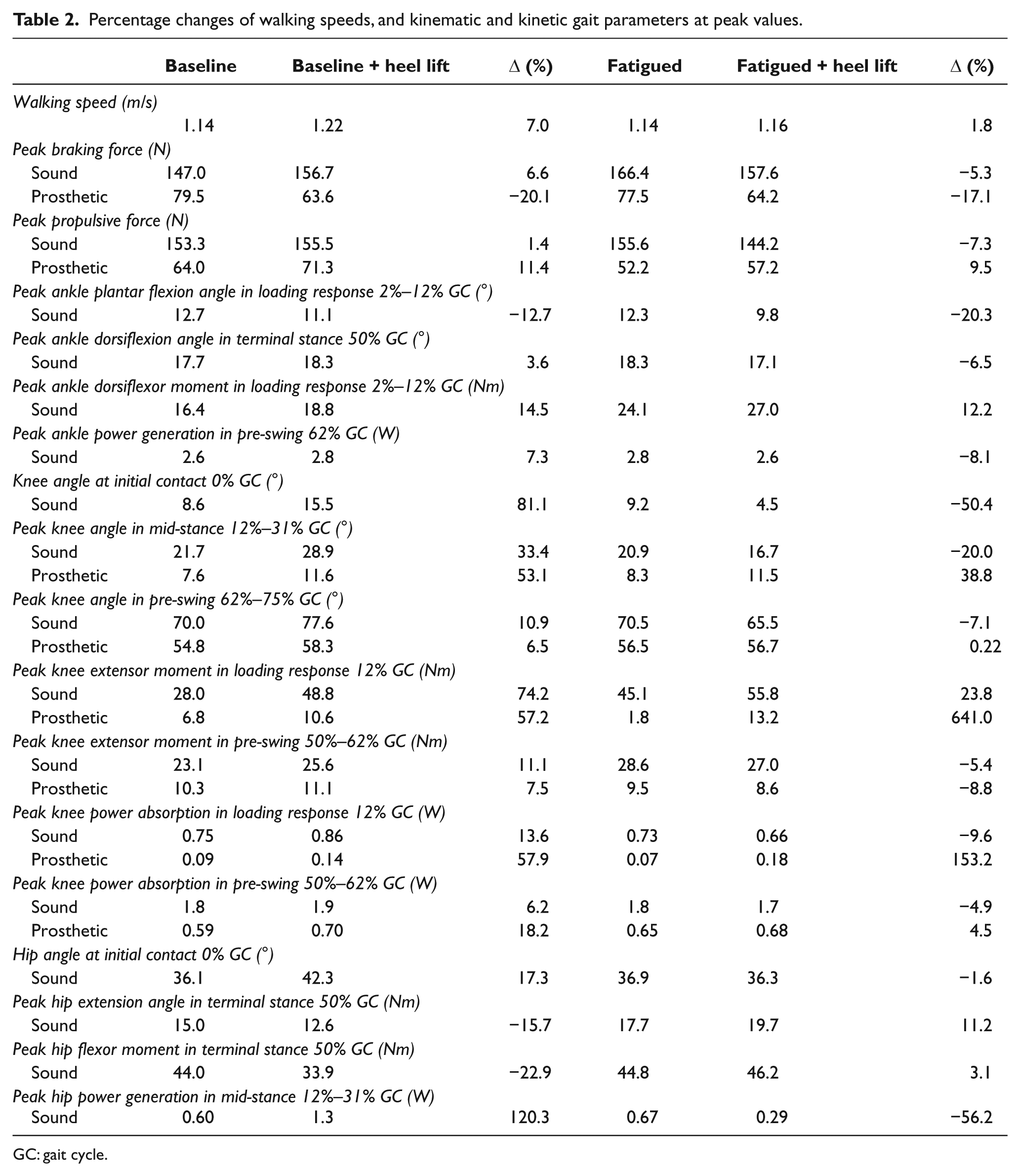
GC: gait cycle.
At the Baseline condition, heel lifting increased the prosthetic-side knee flexion in mid-stance (+53.1%) and pre-swing (+6.5%). There were also increases in peak knee extensor moment in loading response (+57.2%), peak knee power absorption in both loading response (+57.9%), and pre-swing (+18.2%). Walking speed increased (+7%), with a reduction of prosthetic-side peak braking force (−20.1%) and an increase in peak propulsive force (+11.4%). On the sound side, there were greater knee flexion (+81.1%) and hip flexion (+17.3%) at initial contact. Sound-side peak knee extensor moment increased in loading response (+74.2%) and pre-swing (+11.1%), and peak knee power absorption increased in loading response (+13.6%) and pre-swing (+6.2%). In addition, the sound-side ankle (+7.3%) and hip (+120.3%) power generation also increased.
At the Fatigued condition, adding heel lifting increased the prosthetic-side knee flexion during mid-stance (+38.8%), but the degree of the increase was lower than that at the baseline condition (+57.2%). At pre-swing, heel lifting did not produce any obvious changes in prosthetic-side knee flexion (+0.22%). Heel lifting dramatically increased the prosthetic-side knee extensor moment (+641%) and peak knee power absorption (+153.2) in loading response. Walking speed did not have obvious changes (+1.8%). There was a reduction in prosthetic-side peak braking force (−17.1%) and an increase in peak propulsive force (+9.5%). On the sound side, heel lifting did not increase the knee flexion and hip flexion at initial contact. There were reductions in sound-side ankle peak dorsiflexion angle (−6.5%), peak ankle power generation in pre-swing (−8.1%), peak knee extensor moment in pre-swing (−5.4%), peak knee power absorption in loading response (−9.6%), peak braking (−5.3%), and propulsive (−7.3%) forces.
Discussion
Although the percentage differences in some parameters are large, it should be noted that this is an one-subject research making it impossible to test whether the difference is statistically significant. For this subject heel lifting at the Baseline condition induced undesirable drop-off at the prosthetic side. With a rigid prosthetic ankle, the heel lift increased prosthetic-side knee flexion from mid-stance to pre-swing (drop-off), enhancing anterior rotation of the prosthetic shank. This reduced peak braking force and increased peak propulsive force. The subject walked faster with heel lifting, and to keep up with the increased walking speed, the sound-side hip and ankle joints generated more power. To compensate for the drop-off, the sound limb outreached to stabilize the gait by increasing knee flexion and hip flexion at initial contact. The sound-side peak braking force, knee extensor moment, and power absorption then increased. The drop-off gait was in line with the prosthetics theory about the consequence of excessive prosthetic socket flexion. 13
Heel lifting at the Fatigued condition did not give rise to drop-off. Treadmill walking increased the prosthetic-side knee flexion angle in stance phase and knee power absorption in pre-swing even without any heel lifting. This agreed with the findings in a previous research. 7 This stretched the knee extensors allowing them to readily exert higher forces in response to drop-off at late stance phase of the gait. This explained why adding the heel lift at the Fatigued condition dramatically increased the prosthetic-side peak knee extensor moment and power absorption. Nevertheless, the moment and power were still lower than the sound side, which might imply that the likelihood of developing osteoarthritis of the knee at the prosthetic side due to the increased joint moment and power was not high.8,14 Under these circumstances, heel lifting did not increase the prosthetic-side knee flexion at pre-swing as the knee was stabilized by the knee extensor muscles. The outreach of the sound limb as a means of stabilization of drop-off gait was not observed in the gait data.
For this subject, heel lifting at the state of “Somewhat fatigue - need to slow down a bit” could be favorable. It facilitated anterior rotation of the prosthetic shank in mid-stance, which brought about the reduction in prosthetic-side peak braking force and increase in peak propulsive force. The increased forward momentum of the prosthetic side reduced the power generation of the sound-side plantar flexors and knee extensors. The reductions in sound-side ankle motions and power generation might delay the plantar flexors from developing higher level fatigue. This could be the strategy to encourage LDW in transtibial amputees. Future attempts should investigate the exact timing when a heel lift should be added.
It is believed that the wedge-shaped (peak height 10 mm) heel lift does not affect the socket-limb interface stress much, as a previous research indicated that a prosthesis misaligned by 6° socket flexion did not lead to noticeable changes in the mean peak interface pressure. 15 The heel lifts could induce a small degree of leg-length discrepancy. However, they are unlikely to induce low-back pain as the pain is usually associated with leg-length discrepancy of more than 15 mm. 14
This study involved one subject, which could limit the generalizability of the information presented in this report. Given its potential in improving LDW of transtibial amputees, further research should increase the sample size, meanwhile investigating the optimal height and timing of the addition and removal of the heel lifting, the longer-term effects of heel lifts, any possible adverse effects when performing different activities, and whether the same beneficial effects could be generalized to amputees with different gait patterns and using different prosthetic components. In addition to the gait parameters, prosthetic socket-residual limb interface pressure, energy consumptions of the amputees, and electromyography signal of the lower-limb muscles could be other outcome measures.
Conclusion
Before the treadmill walking, heel lifting led to undesirable drop-off. However, after the treadmill walking which induced some fatigue, some limited evidence suggested that drop-off was not observed. At the Fatigue condition, heel lifting facilitated forward propulsion of the prosthesis and reduced the power generation of the sound-side plantar flexor. This potentially delayed the fatigue of plantar flexors, which was previously suggested to be one major difficulty faced by transtibial amputees performing LDW. This article inspires further research in prosthetic alignment, and potentially changes the paradigm of prosthetic prescription.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This study was supported by an internal grant of The Hong Kong Polytechnic University.